Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students

 ,
,
Abstract
1. Introduction
2. Methods
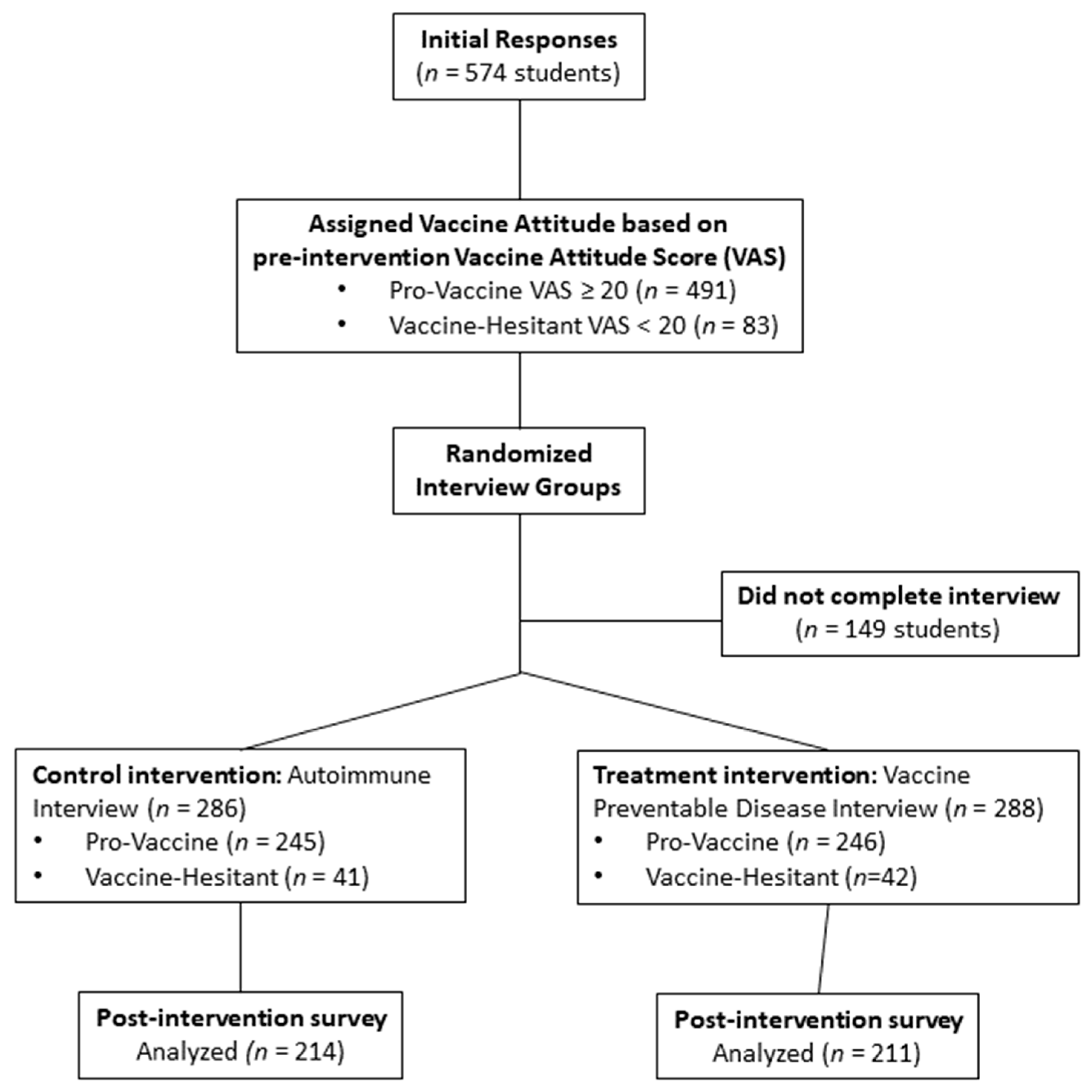
2.1. Study Population
2.2. Assigning Vaccine Attitude Groups and Randomization Process
- Vaccines are more helpful than harmful
- Treatment for autoimmune diseases is more helpful than harmful
- Medications for depression are more helpful than harmful
- Vaccines often have severe side effects
- People with autoimmune diseases suffer considerably
- Medication for depression is effective at treating depression
- There are effective treatments for autoimmune diseases
- Depression can be overcome using willpower
- Vaccines cause autism
- Exercise is the best treatment for autoimmune diseases
- Vaccines are effective at preventing disease
- Medications for depression have severe side effects
- I am likely to fully vaccinate my children/I have fully vaccinated my children
- What is your relationship to the person who had the disease?
- When did they develop the disease?
- Which disease was involved?
- What type of physical suffering did the disease cause? How bad was it?
- How did the disease limit the person’s ability to do normal activities?
- How did the disease affect the person’s interaction with other people?
- How did the disease affect the person’s friends, family, or loved ones?
- How did the disease affect the person financially?
- Were there any other effects of the disease?
- Vaccines are more helpful than harmful
- Treatment for autoimmune diseases is more helpful than harmful
- Medications for depression are more helpful than harmful
- Vaccines often have severe side effects
- People with autoimmune diseases suffer considerably
- Medication for depression is effective at treating depression
- There are effective treatments for autoimmune diseases
- Depression can be overcome using willpower
- Vaccines cause autism
- Exercise is the best treatment for autoimmune diseases
- Vaccines are effective at preventing disease
- Medications for depression have severe side effects
- I am likely to fully vaccinate my children/I have fully vaccinated my childrenComplete next section only if you interviewed a VPD-subjectCircle an answer: much more opposed, slightly more opposed, no effect, slightly more in favor, much more in favor
- How did hearing about the subject’s physical suffering affect your opinion of vaccines?
- How did hearing about how the disease limited normal activity affect your opinion of vaccines?
- How did hearing about how the disease affected the subjects’ interactions with other people affect your opinion of vaccines?
- How did hearing about how the disease affected the subject’s family, friends, or loved ones affect your opinion of vaccines?
- How did hearing about the disease’s financial impact on the subject affect your opinion of vaccines?Rank the following:
- (a)
- Physical suffering
- (b)
- Limitation of activities
- (c)
- Interactions with other people
- (d)
- Effect on family, friends, or loved ones
- (e)
- Financial impact
- Please explain briefly, what effect, if any, the project had on your attitude towards vaccination and why it has that effect.
- If this interview did NOT affect your attitude towards vaccination, why not?
2.3. Analyses
3. Results
3.1. Overview and Pre-Interview Intervention Vaccine Attitudes
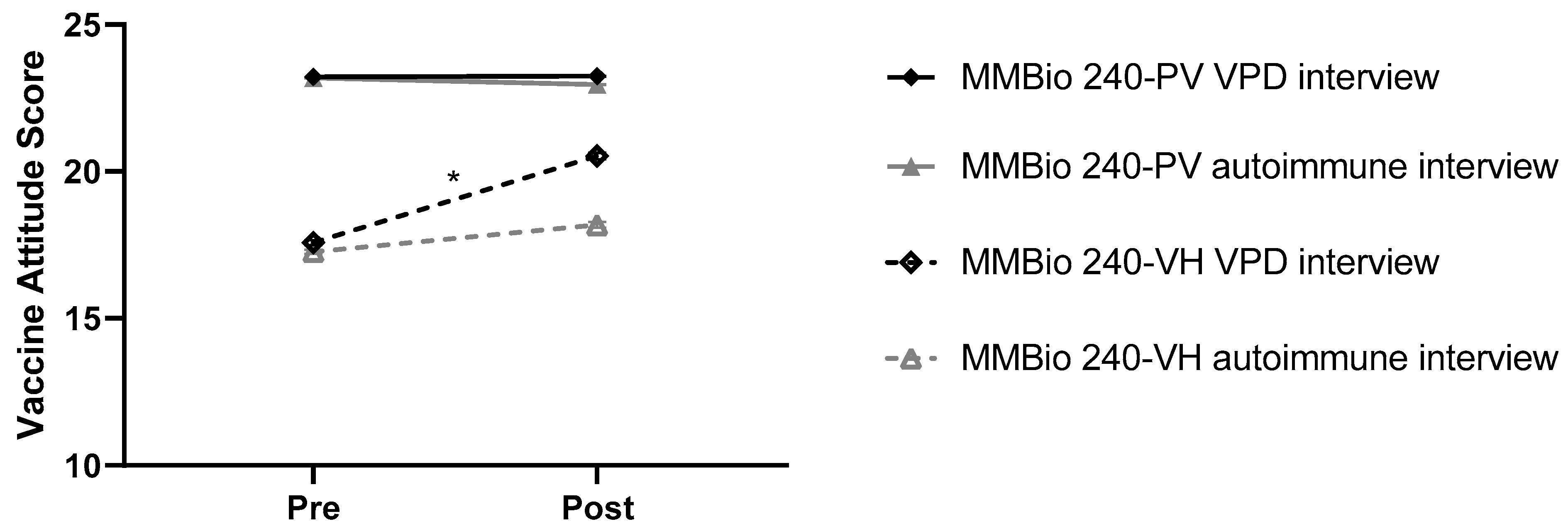
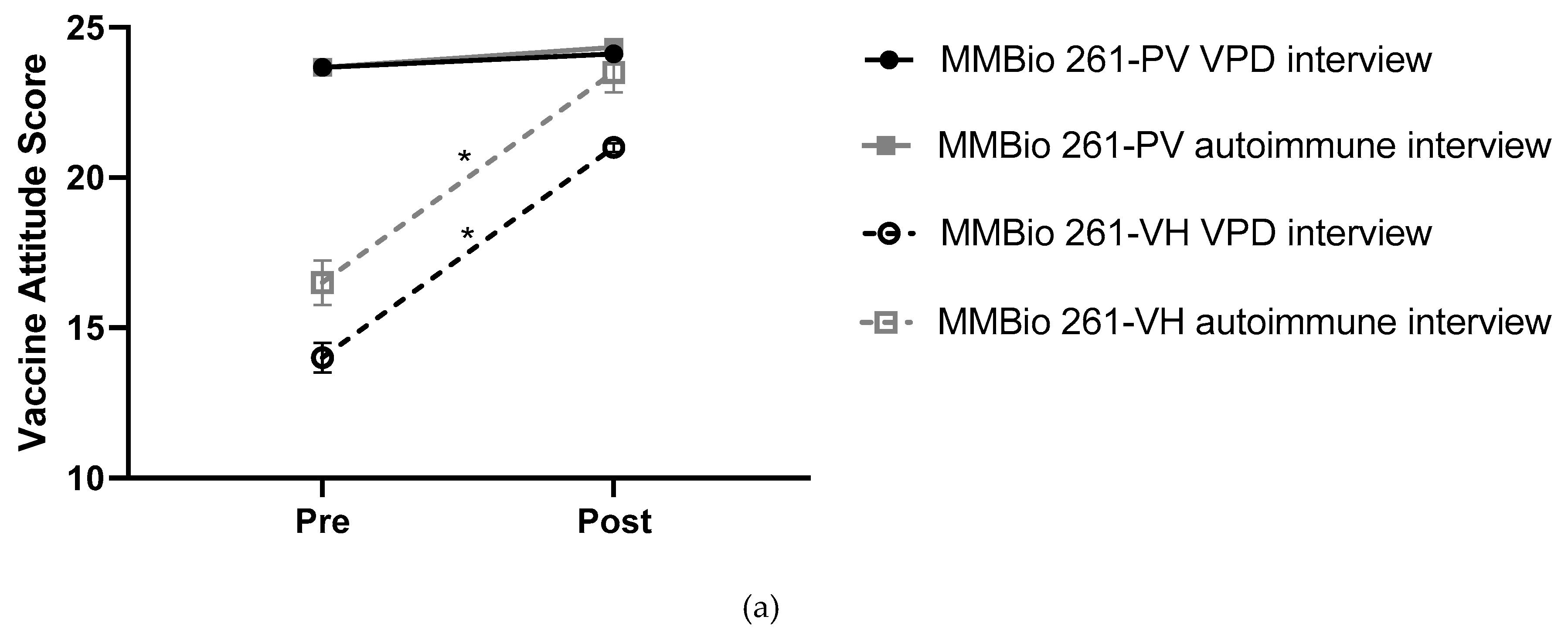
3.2. Interview Intervention Improves Student Vaccine Attitude Scores
3.3. Vaccine Education Likely Improves Student Vaccine Attitudes
3.4. Vaccine-Hesitant Students’ VAS Change Dependent on Pre-Intervention VASs and Class
3.5. Vaccine-Hesitant Student Post-Intervention VAS Increase Correlated with Perceived Physical Suffering and Physical Limitations
3.5.1. Interview Examples Correspond to Student Perceptions of Physical Suffering and Physical Limitations
3.5.2. Student Ranking of Influential Factors Does Not Match Actual Impact
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Orenstein, W.A.; Douglas, R.G.; Rodewald, L.E.; Hinman, A.R. Immunizations in the United States: Success, Structure, and Stress. Health Aff. 2005, 24, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Pan, W.K.; Halsey, N.A.; Stokley, S.; Moulton, L.H.; Navar, A.M.; Pierce, M.; Salmon, D.A. Nonmedical exemptions to school immunization requirements: Secular trends and association of state policies with pertussis incidence. JAMA 2006, 296, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Freed, G.L.; Clark, S.J.; Butchart, A.T.; Singer, D.C.; Davis, M.M. Parental Vaccine Safety Concerns in 2009. Pediatrics 2010, 125, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Gellin, B.G.; Maibach, E.W.; Marcuse, E.K. Do Parents Understand Immunizations? A National Telephone Survey. Pediatrics 2000, 106, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Kempe, A.; Daley, M.F.; McCauley, M.M.; Crane, L.A.; Suh, C.A.; Kennedy, A.M.; Basket, M.M.; Stokley, S.K.; Dong, F.; Babbel, C.I.; et al. Prevalence of parental concerns about childhood vaccines: The experience of primary care physicians. Am. J. Prev. Med. 2011, 40, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Olive, J.K.; Hotez, P.J.; Damania, A.; Nolan, M.S. The state of the antivaccine movement in the United States: A focused examination of nonmedical exemptions in states and counties. PLoS Med. 2018, 15, e1002578. [Google Scholar]
- Evans, D.; Clark, N.M.; Levison, M.J.; Levin, B.; Mellins, R.B. Can children teach their parents about asthma? Health Educ. Behav. 2001, 28, 500–511. [Google Scholar] [CrossRef] [PubMed]
- Lwin, M.O.; Malik, S.; Chua, T.S.; Chee, T.S.; Tan, Y.S. Intergenerational transfer of blood pressure knowledge and screening: A school-based hypertension awareness program in Singapore. Glob. Health Promot. 2016, 23, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Huong, L.T.T.; Long, T.K.; Anh, L.V.; Cook, M.; Capra, M. Decreasing In-home Smoking of Adults—Results from a School-based Intervention Program in Viet Nam. AIMS Public Health 2016, 3, 863–879. [Google Scholar] [CrossRef] [PubMed]
- Nyhan, B.; Reifler, J.; Richey, S.; Freed, G.L. Effective Messages in Vaccine Promotion: A Randomized Trial. Pediatrics 2014, 133, e835–e842. [Google Scholar] [CrossRef] [PubMed]
- Nyhan, B.; Reifler, J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine 2015, 33, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Dube, E.; Vivion, M.; MacDonald, N.E. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2015, 14, 99–117. [Google Scholar] [CrossRef] [PubMed]
- Leask, J. Should we do battle with antivaccination activists? Public Health Res. Pract. 2015, 25, e2521515. [Google Scholar] [PubMed]
- Lewandowsky, S.; Gignac, G.E.; Oberauer, K. The Role of Conspiracist Ideation and Worldviews in Predicting Rejection of Science. PLoS ONE 2013, 8, e75637. [Google Scholar] [CrossRef] [PubMed]
- Popper, K. Conjectures and Refutations: The Growth of Scientific Knowledge, 2nd ed.; Routledge: London, UK, 2014. [Google Scholar] [CrossRef]
- Horne, Z.; Powell, D.; Hummel, J.E.; Holyoak, K.J. Countering antivaccination attitudes. Proc. Natl. Acad. Sci. USA 2015, 112, 10321–10324. [Google Scholar] [CrossRef] [PubMed]
- Parikh, R.K. Fighting for the Reputation of Vaccines: Lessons from American Politics. Pediatrics 2008, 121, 621–622. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class Demographics | Total % (n) | Bio 100 % (n) | MMBio 240 % (n) | MMBio 261 % (n) |
|---|---|---|---|---|
| Total | 100% (425) | 13% (56) | 70% (298) | 17% (71) |
| Gender | ||||
| Male | 62% (263) | 70% (39) | 61% (182) | 59% (42) |
| Female | 38% (162) | 30% (17) | 39% (116) | 41% (29) |
| Age | 21.2 ± 0.21 | 19.7 ± 0.50 | 21.3 ± 0.24 | 22.1 ± 0.40 |
| Pre-Intervention Vaccine Attitude Score | ||||
| Vaccine-Hesitant | 13% (56) | 18% (10) | 14% (41) | 7% (5) |
| Pro-Vaccine | 87% (369) | 82% (46) | 86% (257) | 93% (66) |
| Sociodemographic Characteristic | Total % (n) | Vaccine-Hesitant % (n) | Pro-Vaccine % (n) |
|---|---|---|---|
| Total | 100% (425) | 13% (56) | 87% (369) |
| Gender | |||
| Male | 62% (263) | 14% (36) | 86% (227) |
| Female | 38% (162) | 12% (20) | 88% (142) |
| Age | 21.2 ± 0.21 | 21.0 ± 0.74 | 21.3 ± 0.21 |
| Race/Ethnicity | |||
| African American | 1% (3) | - | 100% (3) |
| Asian | 3% (11) | 27% (3) | 73% (8) |
| Caucasian | 87% (370) | 13% (48) | 87% (322) |
| Hispanic | 3% (12) | 17% (2) | 83% (10) |
| Native American | 0.2% (1) | 100% (1) | - |
| Other | 6% (26) | 8% (2) | 92% (24) |
| Change Post-Treatment | Overall VH % (n) | BIO 100 % (n) | MMBio 240 % (n) | MMBio 261 % (n) |
|---|---|---|---|---|
| Total | 56 | 10 | 41 | 5 |
| VAS Increased | 75% (42) | 80% (8) | 71% (29) | 100% (5) |
| VAS No Change | 11% (6) | 0% (0) | 17% (7) | 0% (0) |
| VAS Decreased | 14% (8) | 20% (2) | 12% (5) | 0% (0) |
| Pro-Vaccine VAS (20+ points) | 50% (28) | 50% (5) | 46% (19) | 80% (4) |
| Pre-Intervention VAS | 11–15 Points | 16 or 17 Points | 18 or 19 Points |
|---|---|---|---|
| Total | 11 | 15 | 30 |
| Post-intervention VAS | |||
| VH | 82% (9) | 40% (6) | 43% (13) |
| VP | 18% (2) | 60% (9) | 57% (17) |
| Change (average) | 2.91 ± 2.74 | 4.00 ± 3.07 | 1.27 ± 2.02 |
| VAS Decreased | 9% (1) | 7% (1) | 20% (6) |
| Age (average) | 20.9 ± 0.9 | 21.0 ± 0.2 | 21.1 ± 1.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, D.K.; Mello, E.J.; Walker, T.D.; Hood, S.J.; Jensen, J.L.; Poole, B.D. Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students. Vaccines 2019, 7, 39. https://doi.org/10.3390/vaccines7020039
Johnson DK, Mello EJ, Walker TD, Hood SJ, Jensen JL, Poole BD. Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students. Vaccines. 2019; 7(2):39. https://doi.org/10.3390/vaccines7020039
Chicago/Turabian StyleJohnson, Deborah K., Emily J. Mello, Trent D. Walker, Spencer J. Hood, Jamie L. Jensen, and Brian D. Poole. 2019. "Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students" Vaccines 7, no. 2: 39. https://doi.org/10.3390/vaccines7020039
APA StyleJohnson, D. K., Mello, E. J., Walker, T. D., Hood, S. J., Jensen, J. L., & Poole, B. D. (2019). Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students. Vaccines, 7(2), 39. https://doi.org/10.3390/vaccines7020039