
Economic Impacts of Initiating Vaccination at 3 Months vs. 6 Months in an Influenza Pandemic in the United States

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Objective
2.2. Epidemiological Model of Influenza Transmission and Health Outcomes
2.3. Economic Assumptions
2.4. Vaccination Scenarios
2.5. Subgroup Analysis
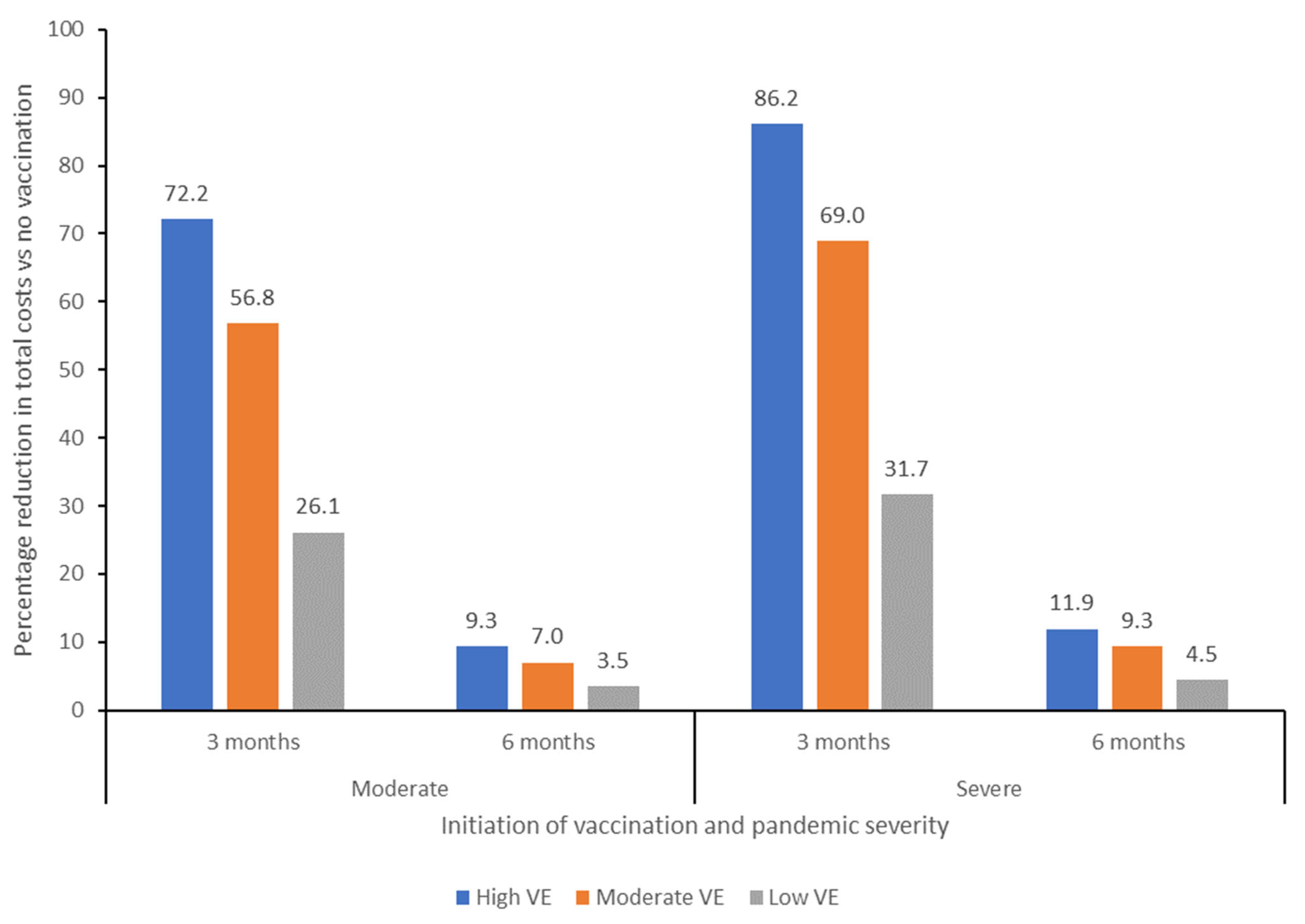
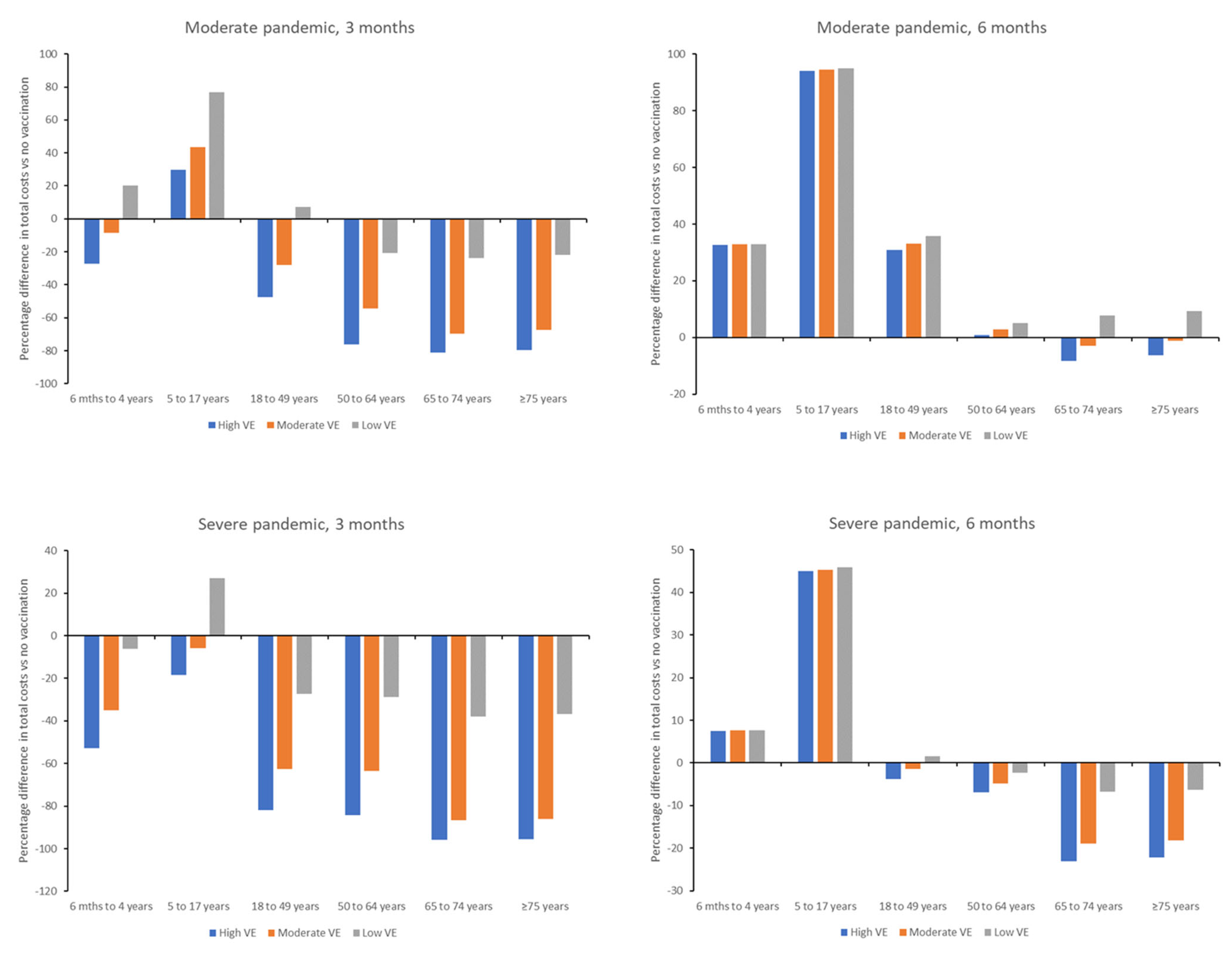
3. Results
Costs per Age Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dynik. Forecasted Global Real GDP Growth 2019–2024. Available online: https://www.statista.com/statistics/1102889/covid-19-forecasted-global-real-gdp-growth/ (accessed on 16 October 2024).
- Cutler, D.M.; Summers, L.H. The COVID-19 Pandemic and the $16 Trillion Virus. JAMA 2020, 324, 1495–1496. [Google Scholar] [CrossRef]
- Kelso, J.K.; Halder, N.; Milne, G.J. Vaccination strategies for future influenza pandemics: A severity-based cost effectiveness analysis. BMC Infect. Dis. 2013, 13, 81. [Google Scholar] [CrossRef] [PubMed]
- Saville, M.; Cramer, J.P.; Downham, M.; Hacker, A.; Lurie, N.; Van der Veken, L.; Whelan, M.; Hatchett, R. Delivering Pandemic Vaccines in 100 Days—What Will It Take? N. Engl. J. Med. 2022, 387, e3. [Google Scholar] [CrossRef] [PubMed]
- CEPI. Delivery Pandemic Vacicnes in 100 Days-What Will It Take? Available online: https://cepi.net/wp-content/uploads/2022/11/CEPI-100-Days-Report-Digital-Version_29-11-22.pdf (accessed on 12 January 2024).
- US Department of Health and Human Services. Influenza and Emerging Infectious Diseases Pandemic Vaccines and Adjuvants Program. Available online: https://medicalcountermeasures.gov/barda/influenza-and-emerging-infectious-diseases/pandemic-vaccines-adjuvants/ (accessed on 12 January 2024).
- Nguyen, V.H.; Crépey, P.; Williams, B.A.; Welch, V.L.; Pivette, J.M.; Jones, C.H.; True, J.M. Modeling the impact of early vaccination in an influenza pandemic in the United States. NPJ Vaccines 2025, 10, 62. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Lansbury, L.E.; Smith, S.; Beyer, W.; Karamehic, E.; Pasic-Juhas, E.; Sikira, H.; Mateus, A.; Oshitani, H.; Zhao, H.; Beck, C.R.; et al. Effectiveness of 2009 pandemic influenza A(H1N1) vaccines: A systematic review and meta-analysis. Vaccine 2017, 35, 1996–2006. [Google Scholar] [CrossRef]
- Belongia, E.A.; Simpson, M.D.; King, J.P.; Sundaram, M.E.; Kelley, N.S.; Osterholm, M.T.; McLean, H.Q. Variable influenza vaccine effectiveness by subtype: A systematic review and meta-analysis of test-negative design studies. Lancet Infect. Dis. 2016, 16, 942–951. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Influenza (Flu) Coverage by Season. Available online: https://www.cdc.gov/flu/fluvaxview/coverage-by-season.htm (accessed on 25 April 2024).
- Centers for Disease Control and Prevention. COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 29 June 2024).
- Jefferson, T.; Jones, M.A.; Doshi, P.; Del Mar, C.B.; Hama, R.; Thompson, M.J.; Spencer, E.A.; Onakpoya, I.; Mahtani, K.R.; Nunan, D.; et al. Neuraminidase inhibitors for preventing and treating influenza in adults and children. Cochrane Database Syst. Rev. 2014, 2014, Cd008965. [Google Scholar] [CrossRef]
- Burch, J.; Paulden, M.; Conti, S.; Stock, C.; Corbett, M.; Welton, N.J.; Ades, A.E.; Sutton, A.; Cooper, N.; Elliot, A.J.; et al. Antiviral drugs for the treatment of influenza: A systematic review and economic evaluation. Health Technol. Assess. 2009, 13, 1–290. [Google Scholar] [CrossRef]
- Taieb, V.; Ikeoka, H.; Wojciechowski, P.; Jablonska, K.; Aballea, S.; Hill, M.; Hirotsu, N. Efficacy and safety of baloxavir marboxil versus neuraminidase inhibitors in the treatment of influenza virus infection in high-risk and uncomplicated patients-a Bayesian network meta-analysis. Curr. Med. Res. Opin. 2021, 37, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Muthuri, S.G.; Venkatesan, S.; Myles, P.R.; Leonardi-Bee, J.; Al Khuwaitir, T.S.; Al Mamun, A.; Anovadiya, A.P.; Azziz-Baumgartner, E.; Báez, C.; Bassetti, M.; et al. Effectiveness of neuraminidase inhibitors in reducing mortality in patients admitted to hospital with influenza A H1N1pdm09 virus infection: A meta-analysis of individual participant data. Lancet Respir. Med. 2014, 2, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, L.R.; Lee, V.J.; Chen, M.I.; Matchar, D.B.; Thompson, J.P.; Cook, A.R. Strategies for antiviral stockpiling for future influenza pandemics: A global epidemic-economic perspective. J. R. Soc. Interface 2011, 8, 1307–1313. [Google Scholar] [CrossRef]
- Monto, A.S.; Comanor, L.; Shay, D.K.; Thompson, W.W. Epidemiology of Pandemic Influenza: Use of Surveillance and Modeling for Pandemic Preparedness. J. Infect. Dis. 2006, 194, S92–S97. [Google Scholar] [CrossRef]
- Wiemken, T.L.; Khan, F.; Puzniak, L.; Yang, W.; Simmering, J.; Polgreen, P.; Nguyen, J.L.; Jodar, L.; McLaughlin, J.M. Seasonal trends in COVID-19 cases, hospitalizations, and mortality in the United States and Europe. Sci. Rep. 2023, 13, 3886. [Google Scholar] [CrossRef]
- Fingar, K.R.; Liang, L.; Stocks, C. Inpatient Hospital Stays and Emergency Department Visits Involving Influenza, 2006–2016. HCUP Statistical Brief #253. Available online: https://hcup-us.ahrq.gov/reports/statbriefs/sb253-Influenza-Hospitalizations-ED-Visits-2006-2016.jsp (accessed on 17 June 2024).
- Lina, B.; Georges, A.; Burtseva, E.; Nunes, M.C.; Andrew, M.K.; McNeil, S.A.; Ruiz-Palacios, G.M.; Feng, L.; Kyncl, J.; Vanhems, P.; et al. Complicated hospitalization due to influenza: Results from the Global Hospital Influenza Network for the 2017–2018 season. BMC Infect. Dis. 2020, 20, 465. [Google Scholar] [CrossRef]
- de Boer, P.T.; Crépey, P.; Pitman, R.J.; Macabeo, B.; Chit, A.; Postma, M.J. Cost-Effectiveness of Quadrivalent versus Trivalent Influenza Vaccine in the United States. Value Health 2016, 19, 964–975. [Google Scholar] [CrossRef]
- Prosser, L.A.; Lavelle, T.A.; Fiore, A.E.; Bridges, C.B.; Reed, C.; Jain, S.; Dunham, K.M.; Meltzer, M.I. Cost-effectiveness of 2009 pandemic influenza A(H1N1) vaccination in the United States. PLoS ONE 2011, 6, e22308. [Google Scholar] [CrossRef]
- Turner, H.C.; Archer, R.A.; Downey, L.E.; Isaranuwatchai, W.; Chalkidou, K.; Jit, M.; Teerawattananon, Y. An Introduction to the Main Types of Economic Evaluations Used for Informing Priority Setting and Resource Allocation in Healthcare: Key Features, Uses, and Limitations. Front. Public Health 2021, 9, 722927. [Google Scholar] [CrossRef]
- Plotkin, S.; Robinson, J.M.; Cunningham, G.; Iqbal, R.; Larsen, S. The complexity and cost of vaccine manufacturing-An overview. Vaccine 2017, 35, 4064–4071. [Google Scholar] [CrossRef]
- Lugnér, A.K.; van Boven, M.; de Vries, R.; Postma, M.J.; Wallinga, J. Cost effectiveness of vaccination against pandemic influenza in European countries: Mathematical modelling analysis. BMJ Br. Med. J. 2012, 345, e4445. [Google Scholar] [CrossRef]
- Khazeni, N.; Hutton, D.W.; Garber, A.M.; Hupert, N.; Owens, D.K. Effectiveness and cost-effectiveness of vaccination against pandemic influenza (H1N1) 2009. Ann. Intern. Med. 2009, 151, 829–839. [Google Scholar] [CrossRef]
- Halder, N.; Kelso, J.K.; Milne, G.J. A model-based economic analysis of pre-pandemic influenza vaccination cost-effectiveness. BMC Infect. Dis. 2014, 14, 266. [Google Scholar] [CrossRef] [PubMed]
- Khazeni, N.; Hutton, D.W.; Collins, C.I.; Garber, A.M.; Owens, D.K. Health and economic benefits of early vaccination and nonpharmaceutical interventions for a human influenza A (H7N9) pandemic: A modeling study. Ann. Intern. Med. 2014, 160, 684–694. [Google Scholar] [CrossRef]
- Reichert, T.A.; Sugaya, N.; Fedson, D.S.; Glezen, W.P.; Simonsen, L.; Tashiro, M. The Japanese Experience with Vaccinating Schoolchildren against Influenza. N. Engl. J. Med. 2001, 344, 889–896. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Roadmap to Implementing Pandemic Inluenza Vaccination of Critical Workforce. Available online: https://stacks.cdc.gov/view/cdc/88961 (accessed on 30 June 2024).
- Borse, R.H.; Shrestha, S.S.; Fiore, A.E.; Atkins, C.Y.; Singleton, J.A.; Furlow, C.; Meltzer, M.I. Effects of vaccine program against pandemic influenza A(H1N1) virus, United States, 2009–2010. Emerg. Infect. Dis. 2013, 19, 439–448. [Google Scholar] [CrossRef]
- Yang, J.; Vaghela, S.; Yarnoff, B.; De Boisvilliers, S.; Di Fusco, M.; Wiemken, T.L.; Kyaw, M.H.; McLaughlin, J.M.; Nguyen, J.L. Estimated global public health and economic impact of COVID-19 vaccines in the pre-omicron era using real-world empirical data. Expert Rev. Vaccines 2023, 22, 54–65. [Google Scholar] [CrossRef]
- Kirson, N.; Swallow, E.; Lu, J.; Mesa-Frias, M.; Bookhart, B.; Maynard, J.; Shivdasani, Y.; Lefebvre, P. The societal economic value of COVID-19 vaccines in the United States. J. Med. Econ. 2022, 25, 119–128. [Google Scholar] [CrossRef]
- Behrouzi, B.; Bhatt, D.L.; Cannon, C.P.; Vardeny, O.; Lee, D.S.; Solomon, S.D.; Udell, J.A. Association of Influenza Vaccination With Cardiovascular Risk: A Meta-analysis. JAMA Netw. Open 2022, 5, e228873. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Pandemic Severity | Vaccination Scenario | Symptomatic Cases | Hospital Visits | GP Visits | Deaths |
|---|---|---|---|---|---|
| Vaccination at 3 Months | |||||
| Moderate | No vaccination (antiviral only) | 88,942,473 | 717,554 | 39,607,982 | 206,487 |
| High effectiveness vaccine | 17,940,821 | 91,206 | 6,935,595 | 9634 | |
| Moderate effectiveness vaccine | 36,025,035 | 204,249 | 14,776,717 | 32,231 | |
| Low effectiveness vaccine | 66,741,092 | 490,893 | 28,380,923 | 129,199 | |
| Severe | No vaccination (antiviral only) | 88,942,473 | 9,618,426 | 47,529,578 | 2,088,333 |
| High effectiveness vaccine | 18,626,689 | 1,074,635 | 8,892,181 | 90,141 | |
| Moderate effectiveness vaccine | 37,555,149 | 2,560,741 | 18,994,985 | 314,237 | |
| Low effectiveness vaccine | 68,419,956 | 6,435,691 | 35,434,289 | 1,297,349 | |
| Vaccination at 6 Months | |||||
| Moderate | No vaccination (antiviral only) | 88,942,473 | 717,554 | 39,607,982 | 206,487 |
| High effectiveness vaccine | 83,066,866 | 618,770 | 35,940,361 | 161,574 | |
| Moderate effectiveness vaccine | 85,006,471 | 637,636 | 37,123,270 | 169,058 | |
| Low effectiveness vaccine | 86,739,568 | 681,795 | 38,197,193 | 190,798 | |
| Severe | No vaccination (antiviral only) | 88,942,473 | 9,618,426 | 47,529,578 | 2,088,333 |
| High effectiveness vaccine | 83,457,744 | 8,226,533 | 43,467,459 | 1,627,136 | |
| Moderate effectiveness vaccine | 85,411,755 | 8,494,008 | 44,901,333 | 1,703,959 | |
| Low effectiveness vaccine | 87,024,741 | 9,111,149 | 46,084,171 | 1,926,968 | |
| Scenario | GP Costs | Hospitalization Costs | Workday Cost | Administration Costs | Antiviral Costs | Cost of Lost Productivity Due to Excess Mortality | Total Costs |
|---|---|---|---|---|---|---|---|
| Vaccination at 3 Months | |||||||
| No vaccination (antiviral only) | $20,599,453,279 | $28,978,034,803 | $12,604,418,645 | $19,415,048,680 | $1,118,113,040 | $33,719,406,329 | $116,434,474,776 |
| High effectiveness vaccine | $2,405,596,950 | $3,406,805,683 | $2,592,480,598 | $19,415,048,680 | $209,306,610 | $4,333,698,370 | $32,362,936,891 |
| Moderate effectiveness vaccine | $6,545,903,147 | $8,463,078,017 | $5,072,670,071 | $19,415,048,680 | $432,101,841 | $10,346,938,544 | $50,275,740,300 |
| Low effectiveness vaccine | $13,535,209,281 | $19,520,301,978 | $9,288,304,732 | $19,415,048,680 | $835,576,668 | $23,437,642,287 | $86,032,083,626 |
| Vaccination at 6 Months | |||||||
| No vaccination (antiviral only) | $20,599,453,279 | $28,978,034,803 | $12,604,418,645 | $19,415,048,680 | $1,118,113,040 | $33,719,406,329 | $116,434,474,776 |
| High effectiveness vaccine | $18,048,536,313 | $25,454,554,885 | $11,810,945,816 | $19,415,048,680 | $1,043,851,428 | $29,820,764,952 | $105,593,702,074 |
| Moderate effectiveness vaccine | $18,832,091,464 | $26,206,934,960 | $12,049,890,261 | $19,415,048,680 | $1,068,215,875 | $30,630,414,373 | $108,202,595,613 |
| Low effectiveness vaccine | $19,572,794,262 | $27,648,503,767 | $12,290,021,200 | $19,415,048,680 | $1,090,276,084 | $32,292,287,457 | $112,308,931,450 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, V.H.; Crepey, P.; Williams, B.A.; Welch, V.L.; Pivette, J.M.; Jones, C.H.; True, J.M. Economic Impacts of Initiating Vaccination at 3 Months vs. 6 Months in an Influenza Pandemic in the United States. Vaccines 2025, 13, 828. https://doi.org/10.3390/vaccines13080828
Nguyen VH, Crepey P, Williams BA, Welch VL, Pivette JM, Jones CH, True JM. Economic Impacts of Initiating Vaccination at 3 Months vs. 6 Months in an Influenza Pandemic in the United States. Vaccines. 2025; 13(8):828. https://doi.org/10.3390/vaccines13080828
Chicago/Turabian StyleNguyen, Van Hung, Pascal Crepey, B. Adam Williams, Verna L. Welch, Jean Marie Pivette, Charles H. Jones, and Jane M. True. 2025. "Economic Impacts of Initiating Vaccination at 3 Months vs. 6 Months in an Influenza Pandemic in the United States" Vaccines 13, no. 8: 828. https://doi.org/10.3390/vaccines13080828
APA StyleNguyen, V. H., Crepey, P., Williams, B. A., Welch, V. L., Pivette, J. M., Jones, C. H., & True, J. M. (2025). Economic Impacts of Initiating Vaccination at 3 Months vs. 6 Months in an Influenza Pandemic in the United States. Vaccines, 13(8), 828. https://doi.org/10.3390/vaccines13080828