Abstract
Background/Objective: Maternal immunization is highly recommended, particularly in developed countries. However, its awareness among pregnant women in Japan remains low. This study aimed to assess the awareness and attitudes toward maternal immunization among pregnant women in Japan and to identify the factors that may promote its acceptance. Methods: We conducted a cross-sectional questionnaire survey among pregnant women attending antenatal checkups at nine facilities in Kanagawa Prefecture, Japan, from August 2024 to January 2025. The survey assessed knowledge and intention regarding maternal immunization for influenza, pertussis, respiratory syncytial virus (RSV), and group B streptococcus (GBS) as well as attitudes toward vaccination costs and information sources. Results: Overall, 523 respondents were included in this study. The overall awareness of maternal immunization was 16%. Willingness to receive vaccinations during pregnancy was reported for influenza (68%), pertussis (58%), RSV (59%), and GBS (71%). A common reason for vaccine hesitancy included uncertainty about its effects on the fetus. The key factors associated with vaccine acceptance were higher educational attainment and prior knowledge of maternal immunization. Regarding costs, most respondents were willing to pay up to JPY 5000 (approximately USD 35). The most frequently prioritized sources were explanations from physicians, followed by explanations from midwives. Conclusions: Despite low awareness, vaccination intention was comparable to that reported in other countries. Points that may contribute to improved vaccine uptake were also identified. These findings may lead to the prevention of infectious diseases in newborns and infants in Japan and possibly improve public health.
1. Introduction
Maternal infection during pregnancy is a known contributor to serious maternal illness. Since immune responses in early infancy remain immature and largely rely on maternally derived antibodies, maternal immunization, which promotes the transplacental transfer of protective antibodies, plays an essential role in safeguarding both maternal and neonatal health [1]. Accordingly, maternal immunization is actively recommended and widely implemented in countries, such as the United States [2,3]. Currently, the CDC and WHO recommend the administration of vaccines against COVID-19, influenza, respiratory syncytial virus (RSV), and tetanus, diphtheria, and acellular pertussis (Tdap) during pregnancy [4,5]. Conversely, although seasonal influenza vaccination during pregnancy is common in Japan, the administration of pertussis-containing vaccines to pregnant women is hardly performed, partly due to the absence of strong recommendations in clinical guidelines, a situation similarly observed for COVID-19 and RSV vaccines [6,7]. Consequently, awareness of maternal immunization among pregnant women in Japan remains low. A previous study conducted in 2019 reported a recognition rate of only 3.9% [8], which may reflect the absence of Tdap approval, financial burden, and insufficient recommendations from healthcare providers [7]. In 2024, a vaccine against RSV was approved for pregnant women and became available in Japan. Currently, several maternal immunization vaccines, including those under development for the prevention of group B streptococcus (GBS), a major cause of severe infections during neonatal and early infancy, are being developed [9,10]. These developments highlight the growing significance of maternal immunization.
This study aimed to assess the awareness and attitudes toward maternal immunization among pregnant women in Japan and identify factors that may promote its acceptance.
2. Materials and Methods
2.1. Study Design and Participants
This multicenter cross-sectional study was conducted at two university hospitals, six general hospitals, and one obstetric clinic in Kanagawa Prefecture, Japan. Pregnant women attending routine antenatal checkups at any of these facilities were invited to participate in this study. Pregnant women who provided informed consent were enrolled between August 2024 and January 2025. The survey was conducted anonymously using Google Forms. Consent for participation was obtained from participants at the beginning of the questionnaire. Pregnant women who declined to provide consent were excluded.
The study protocol was approved by the Ethics Committee of Yokohama City University Medical Center Hospital (approval no. IPPAN 2024-019) and was conducted in accordance with the Declaration of Helsinki.
2.2. Data Collection
Participants were provided with a simplified explanation sheet about maternal immunization as well as specific information on pertussis, RSV, and GBS. Subsequently, participants scanned the QR code attached to the sheet, accessed the questionnaire page, and answered the questionnaire. Consent was obtained upon submission of responses. For questions related to GBS vaccination, a note clarified that the vaccine was assumed to be safe and effective for both mothers and infants.
The questionnaire included items on demographic and obstetric characteristics, disease awareness, vaccination intentions, and acceptable costs. Some items allowed the respondents to skip questions. The full questionnaire is provided in the Supplementary File. No skip logic was implemented; all participants were presented with the same set of questions regardless of their previous answers. This study was exploratory in nature, aimed at understanding current awareness and attitudes toward maternal immunization to inform clinical promotion strategies. Therefore, the questionnaire items were developed de novo by the study team rather than adapted from pre-validated instruments.
2.3. Statistical Analyses
Categorical data are reported as frequencies (percentages), and continuous data are provided as medians and interquartile ranges. Missing data were excluded from each relevant analysis and not imputed.
Statistical analysis was performed using the chi-square test for categorical variables and the Wilcoxon test for continuous ones. Logistic regression analyses were performed in a univariate manner; each variable was evaluated separately without adjustment for potential confounders. All variables collected in the questionnaire were tested individually, without preselection, to explore their associations with vaccination intention. Odds Ratios (ORs) and 95% Confidence Intervals (CIs) were determined. Differences were considered statistically significant at p < 0.05. Data were analyzed using JMP Pro 17 software (version 17.0.0; SAS Institute Inc., Cary, NC, USA).
3. Results
Overall, 523 valid responses were obtained. The participant characteristics are shown in Table 1. The overall awareness of maternal immunization was 16%. Moreover, the proportion of respondents who expressed willingness to receive vaccination during pregnancy was 68%, 58%, 59%, and 71% for influenza, pertussis, RSV, and GBS, respectively, with statistically significant differences among the vaccines (p < 0.001). The intention rate for GBS vaccination was assessed under the hypothetical assumption that the vaccine would be safe and effective. These proportions were calculated using only the number of respondents who answered each respective item: 521 for influenza (352/521), 518 for pertussis (303/518), 518 for RSV (305/518), and 519 for GBS (366/519). Summaries of response counts and missing data for each vaccine item are provided in Supplementary Table S1.

Table 1.
Background characteristics of pregnant respondents.
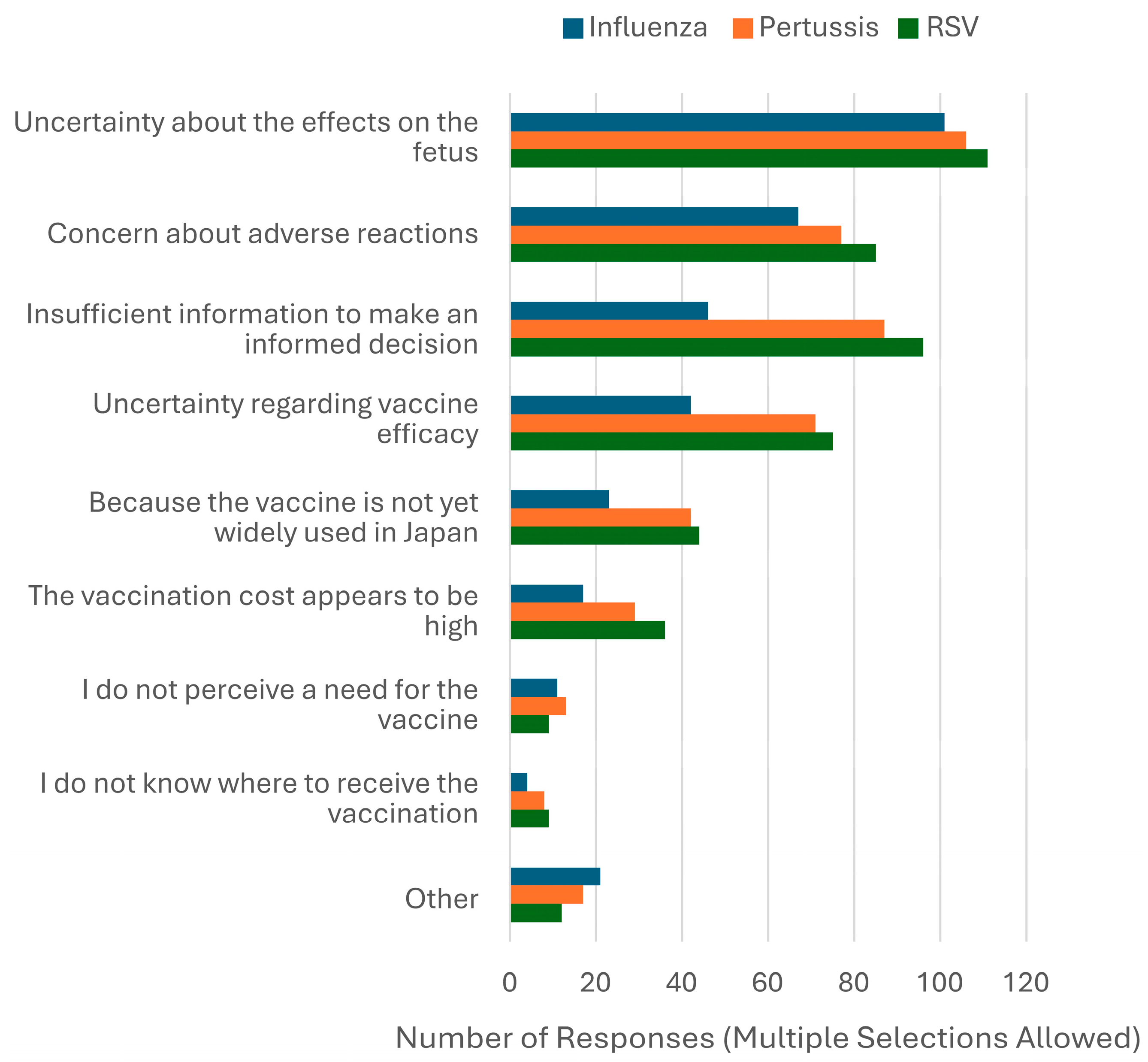
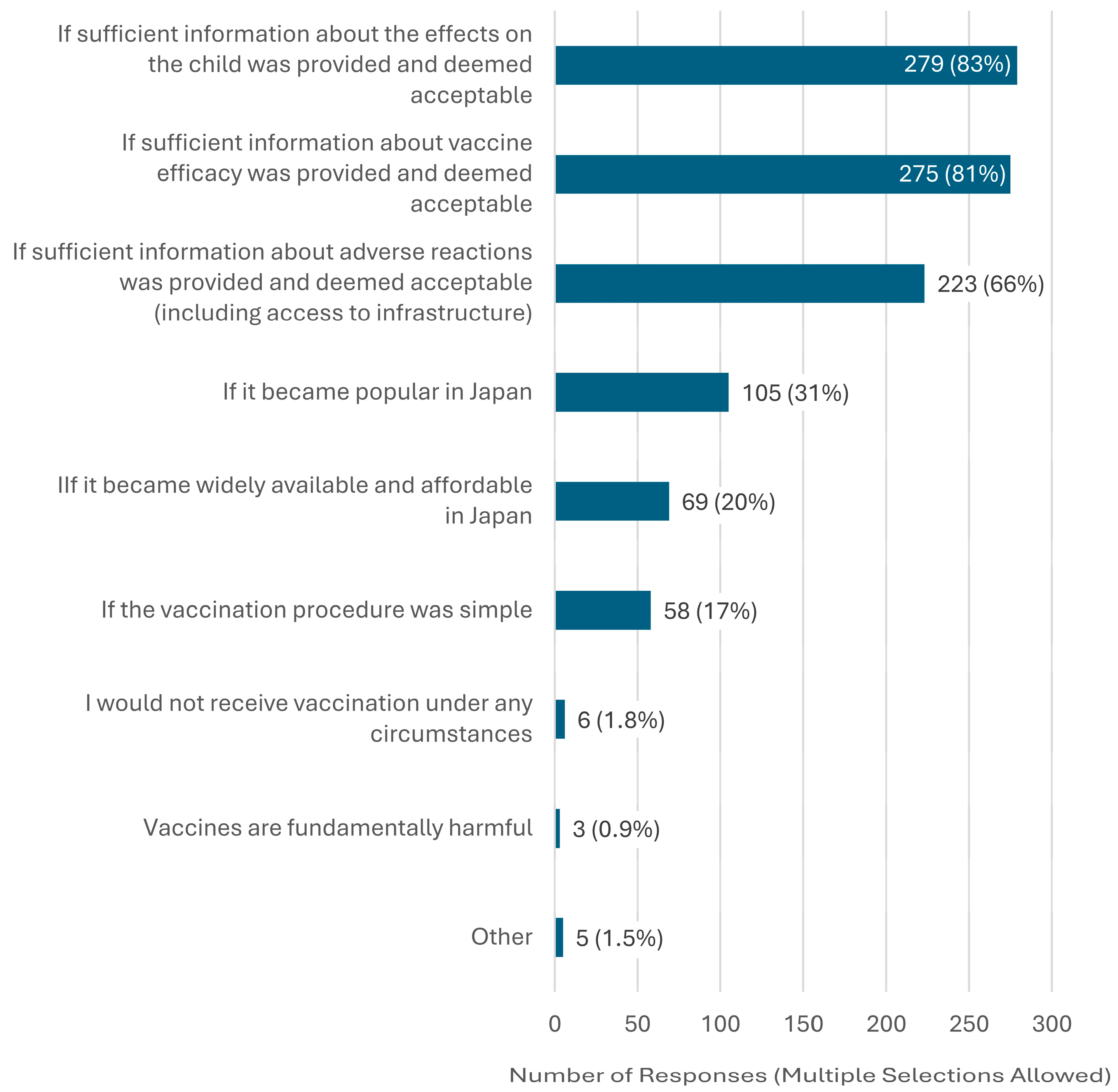
The most common reason for unwillingness to receive vaccination was “Uncertainty about the effects of influenza, pertussis, and RSV on the fetus.” Other frequently cited reasons included concerns about adverse reactions and insufficient information to make an informed decision (Figure 1). Participants could select multiple reasons. Detailed counts and percentages of reasons for vaccine hesitancy, categorized by vaccine (influenza, pertussis, or RSV), are presented in Supplementary Table S2. Regarding GBS, the most frequently cited condition under which respondents would consider vaccination was “If sufficient information about the effects on the child was provided and deemed acceptable” (Figure 2). The GBS vaccine remains under development and has not yet received regulatory approval in Japan or any other country. Accordingly, the survey did not assess vaccine hesitancy per se but rather explored respondents’ willingness to receive the vaccine in the future and the conditions under which they would consider doing so.
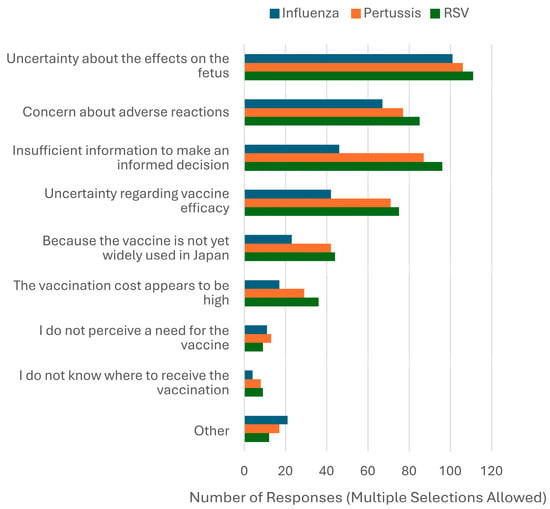
Figure 1.
Reported reasons for unwillingness to receive maternal vaccines.
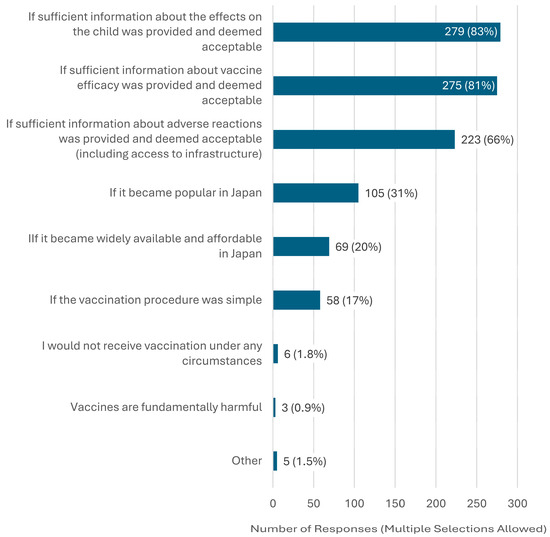
Figure 2.
Conditions under which pregnant women would consider GBS vaccination (n = 338). Note: n = 338 refers to all participants, regardless of their initial willingness to receive the GBS vaccine, who answered the question about conditions under which they would consider future GBS vaccination. Multiple responses were allowed.
Regarding costs, among those who were willing to be vaccinated, the amount most frequently selected as the upper limit for vaccination was under JPY 3000. There were no differences between the vaccines, and most respondents were willing to pay up to JPY 5000. The proportion of respondents who answered that they would not receive vaccination regardless of the cost was 7.8%, 8.6%, 7.8%, and 6.9% for influenza, pertussis, RSV, and GBS, respectively (Table 2).
Table 2.
Preferred vaccination cost among pregnant women willing to receive each vaccine.
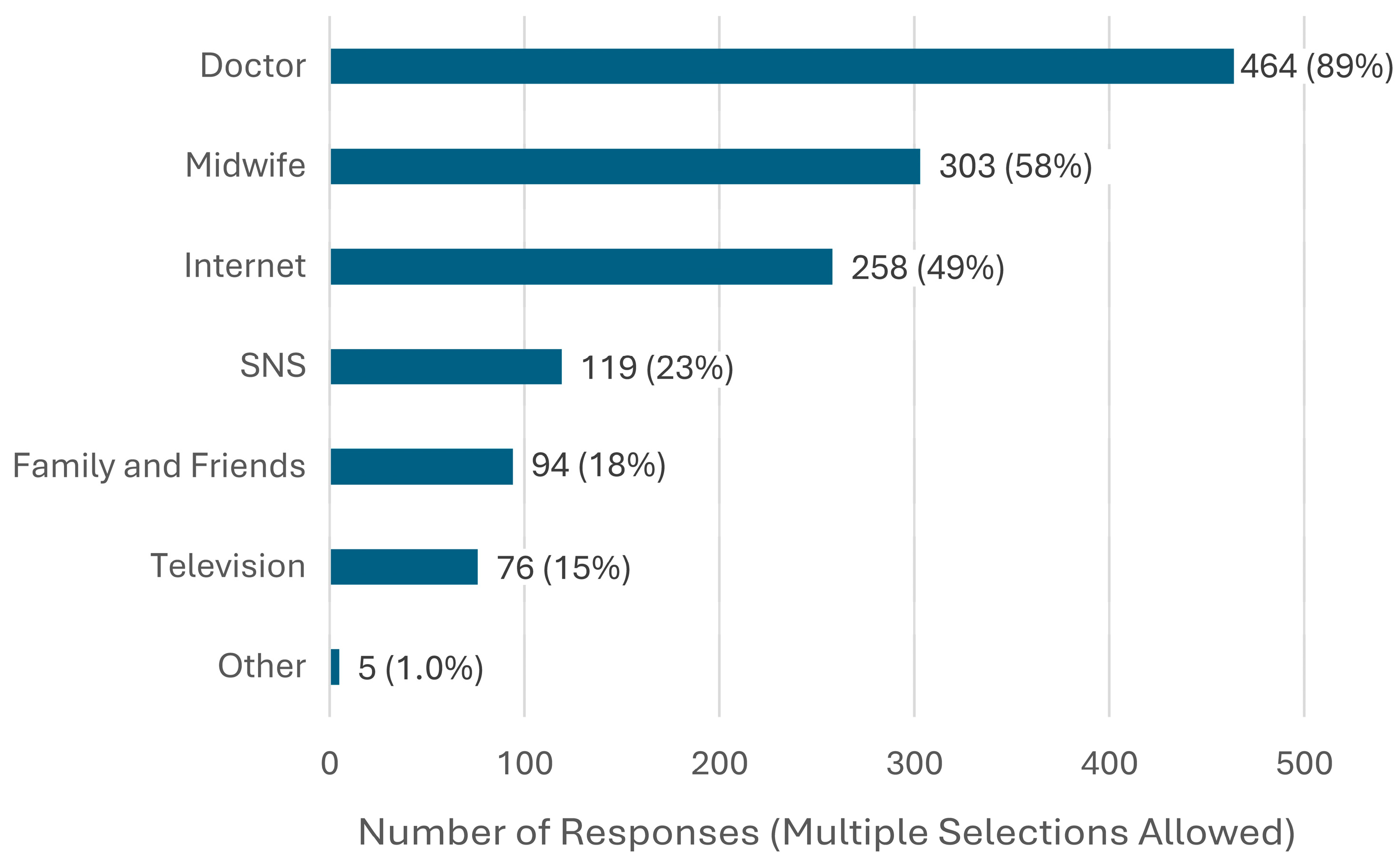
When obtaining information about vaccination during pregnancy, the most frequently prioritized sources were explanations from doctors, followed by explanations from midwives (Figure 3). In the analysis of factors associated with willingness to be vaccinated, factors commonly observed across all vaccines were final educational attainment (junior college, vocational school, or technical college graduate or higher) and knowledge of maternal immunization. Additionally, occupation was positively associated with vaccine acceptance for influenza, RSV, and GBS. Pregnant women who identified physicians or midwives as key sources of information were highly likely to accept influenza and pertussis vaccines. Disease awareness was also significantly associated with vaccine acceptance for influenza (OR 2.70, 95% CI: 1.04–6.61), RSV (OR 1.75, 95% CI: 1.16–2.64), and GBS (OR 2.13, 95% CI: 1.31–3.45). A history of RSV infection in the respondent or their child was frequently observed among those who were willing to be vaccinated (OR 1.70, 95% CI: 1.08–2.68). Finally, gestational age was significantly associated with vaccine acceptance only for GBS (Table 3, Table 4, Table 5 and Table 6). A summary of variables that showed statistically significant associations with willingness to receive each vaccine is presented in Supplementary Table S3.
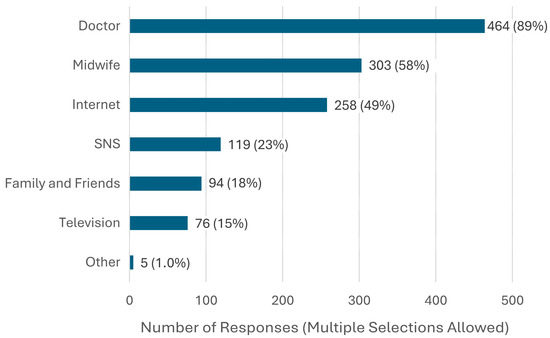
Figure 3.
Key sources of information on vaccines during pregnancy (n = 522).
Table 3.
Univariate logistic regression analysis of factors associated with willingness to receive influenza vaccination during pregnancy (n = 521).
Table 4.
Univariate logistic regression analysis of factors associated with willingness to receive pertussis vaccination during pregnancy (n = 518).
Table 5.
Univariate logistic regression analysis of factors associated with willingness to receive RSV vaccination during pregnancy (n = 518).
Table 6.
Univariate logistic regression analysis of factors associated with willingness to receive GBS vaccination during pregnancy (n = 519).
4. Discussion
This study showed that the awareness rate of maternal immunization among pregnant women in Japan was 16% and the intention to receive the vaccination was approximately 60%. In addition, factors associated with increased vaccination rates were prior knowledge of maternal immunization and the cost burden of vaccinations.
Although awareness of maternal immunization remains low in Japan compared to other countries, where more than half of pregnant women are reportedly aware of maternal immunization and willing to receive maternal vaccines [11,12,13], the intention to vaccinate observed in this study was comparable. For RSV, the most recent maternal immunization, international studies have reported intention rates ranging from 42% to 88% [14], which aligns with the rate found in our study. In Japan, awareness appears to be gradually increasing: the proportion of pregnant women aware of maternal pertussis vaccination rose from 3.9% in 2019 [8] to 16% in this study. This discrepancy between low awareness and relatively high intention may be interpreted through the WHO BeSD framework. Within the domain of Thinking and Feeling, contributing factors may include a lack of perceived safety, efficacy, and trustworthiness regarding each vaccine as well as insufficient understanding of the diseases among pregnant women [15]. Among participants who expressed unwillingness to receive maternal vaccines, the most commonly cited reasons for hesitancy were uncertainty about fetal effects, concerns about adverse reactions, and insufficient information to make an informed decision. These findings suggest that, while overall intention to vaccinate may be relatively high, emotional and informational barriers remain substantial within the hesitant subgroup. Addressing these concerns through improved risk communication and tailored educational strategies may help further increase vaccine uptake. In terms of Social Processes, the delayed inclusion of these vaccines in Japanese guidelines may have led to insufficient recommendations from healthcare professionals, including physicians and midwives [7]. Regarding Practical Issues, while influenza vaccination is now standard practice in maternity care, pertussis vaccination is not commonly offered in such facilities in Japan. Furthermore, access to vaccines such as the recently approved RSV vaccine may remain limited [6,7,16]. This situation may be partly due to the absence of Tdap vaccine implementation in Japan. Although the DTaP vaccine—containing a different formulation of pertussis, diphtheria, and tetanus antigens—is currently approved for use in pregnant women in Japan, evidence regarding its immunogenicity and safety in the context of maternal immunization remains limited [7]. Therefore, maternal vaccination rates are expected to increase through the dissemination of accurate information, improved accessibility—such as reduced financial burden and broader availability at maternity facilities—and the accumulation of domestic data on vaccine immunogenicity and safety to enhance public trust.
Furthermore, this study showed that the factors associated with increased vaccination rates were prior knowledge of maternal immunization and the cost burden of vaccination. Previous studies have reported that a lack of knowledge regarding maternal immunization for pertussis is associated with a lower vaccine intention [11], which is consistent with the findings of this study. Additionally, a study on pertussis in the United Kingdom reported that although not statistically significant, the vaccine uptake rate during pregnancy differed by 69% in areas with low levels of deprivation compared with 52% in areas with high deprivation [17]. Although this study did not investigate deprivation levels, it showed that vaccination intention varied among pregnant women in Japan depending on the cost of vaccination. This may be partly due to the fact that in Japan, there is no public subsidy for maternal immunization with pertussis or RSV vaccines during pregnancy, and the recipient bears the entire cost.
Among respondents who did not intend to receive vaccination, “insufficient information to make a decision” and “uncertainty about vaccine efficacy” were more frequently cited for pertussis and RSV vaccines than for influenza. These differences likely reflect the historical development of vaccine recommendations for pregnant women in Japan. Since 2008, influenza vaccination has been addressed as a separate topic in obstetric guidelines, with its safety and effectiveness for newborns emphasized from 2011 onward [18,19]. As a result, influenza vaccination is widely practiced, and awareness among pregnant women is relatively high [20]. In contrast, pertussis vaccination was only mentioned for the first time in the 2023 edition, and the RSV vaccine, approved in 2024, has not yet been included in the guidelines [21]. These delays may explain the limited awareness and lower frequency of provider recommendations, contributing to greater hesitancy for the pertussis and RSV vaccines [6,7,8].
Based on our findings, two key strategies may help promote maternal immunization in Japan. First, given that prior knowledge of maternal immunization was more prevalent among those who expressed willingness to be vaccinated, the integration of educational interventions on vaccination into preconception care settings may represent a promising approach. However, this proposition should be interpreted with caution, as current evidence directly linking preconception education to increased vaccine uptake during pregnancy is limited. This concept aligns with international recommendations, such as those from FIGO [22]. In the context of Japan’s relatively high prevalence of fertility treatment [23], preconception care, especially in settings involving assisted reproductive technology (ART), may offer structured opportunities for anticipatory guidance on maternal immunization. Nevertheless, this hypothesis remains speculative and requires empirical validation in future research. Second, since the most frequently selected cost limit was JPY 3000, with most respondents willing to pay up to JPY 5000 for vaccination, financial support for vaccination programs may improve their uptake. In the United Kingdom and France, vaccination is currently subsidized by the government [16]; although it depends on the insurance plan, in the United States, it is often included as a covered service [24]. Although cost-effectiveness analyses of RSV vaccines have not been conducted in Japan, studies on influenza and pertussis vaccines have been conducted [25,26]. The cost-effectiveness of RSV vaccination according to epidemic season has been reported in other countries [27,28]. Although this depends on future epidemiological trends, financial subsidies may be a potential strategy from a social perspective in Japan, given that the absence of public financial support constitutes a well-recognized barrier to vaccine acceptance [29,30]. It is important to note that institutional barriers to maternal immunization in Japan are not limited to the lack of financial support systems. Notably, maternal immunization is not included in the official recommendation section of the Japanese clinical practice guidelines [16]. Due to this absence of strong recommendations, even if pregnant women are willing to be vaccinated, they may not receive active encouragement from healthcare providers in clinical settings, which may result in limited increases in actual vaccination coverage [31]. Although the present study did not assess whether participants received information about maternal immunization from healthcare providers during their current pregnancy, repeated counseling by healthcare professionals is known to be a key factor in promoting vaccine uptake [32]. Furthermore, there is evidence that reductions in institutional support may negatively impact vaccination coverage [33], suggesting that vaccine intention alone is insufficient to sustain behavioral change. Structural support and access must also be ensured. In recent years, chatbot-based interventions have been shown to enhance vaccine literacy and acceptance. Thus, the incorporation of digital tools—such as educational platforms and reminder systems—may be effective in translating high vaccination intent into actual uptake [34].
The strength of this study lies in its detailed clarification of vaccination awareness among pregnant women in Japan, which has not been reported in recent years, and the findings are important in terms of vaccination policies.
This study had some limitations. First, we recruited pregnant women from a wide range of facilities, from primary to tertiary obstetric ones; however, owing to the study design, we did not know the number of questionnaires collected at each facility. Furthermore, although the questionnaire was distributed to all pregnant women, the rate of response refusal was not measurable. Therefore, there may have been biases in the facilities and respondents, and participant bias cannot be excluded. Second, the study was conducted during the initial rollout phase of RSV vaccine availability in Japan, and future trends may differ. Third, as the questionnaire was developed de novo without formal validation or the use of established instruments, the reliability and validity of some items may be limited. Moreover, in the absence of cognitive pre-testing, respondents may have interpreted certain survey items inconsistently. Furthermore, the information sheet, which was provided to raise awareness, may have unintentionally influenced responses, introducing potential bias. Combined with the self-reported nature of the questionnaire, these factors may have introduced social desirability bias. Finally, this study was conducted exclusively at facilities located in urban settings. As the residential distribution of the respondents was not assessed, potential differences in health behaviors and vaccine literacy between urban and rural pregnant women could not be explored. As a result, the generalizability of the findings to rural or nationwide populations is limited, and different patterns may emerge in more diverse settings.
5. Conclusions
This study showed that awareness of maternal immunization among pregnant women in Japan remains low and the intention to be vaccinated is relatively high. Additionally, factors associated with increased vaccination rates are prior knowledge of maternal immunization and the cost burden of vaccination. To increase maternal immunization rates, integrating vaccine counseling into routine prenatal care may represent a feasible and effective strategy. Given the widespread preference for low-cost vaccination, implementing public financial support systems should also be considered to mitigate economic barriers. Future interventional studies are needed to evaluate the effectiveness of educational interventions, healthcare provider recommendations, and financial subsidies on actual vaccine uptake during pregnancy.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/vaccines13080779/s1, Question Items and Tables S1–S3. Table S1: Numbers of responses, missing values, and acceptance rates for each vaccine item. Abbreviations: RSV, respiratory syncytial virus; GBS, group B streptococcus.; Table S2: Reported reasons for unwillingness to receive maternal vaccines by vaccine type (influenza, pertussis, and RSV). Note: Among participants who expressed unwillingness to receive each vaccine, the numbers of respondents who answered the question on reasons for hesitancy were as follows: influenza, 143 of 169; pertussis, 193 of 215; and RSV, 195 of 213. Each column shows the number of respondents and the corresponding percentage among those who answered the question for each vaccine. Multiple responses were allowed; thus, totals may exceed 100%. Abbreviation: RSV, respiratory syncytial virus.; Table S3: Summary of variables significantly associated with willingness to receive each maternal vaccine in univariate logistic regression. Note: This summary table highlights variables that showed statistically significant positive associations with willingness to receive each vaccine based on univariate logistic regression analyses (Table 3, Table 4, Table 5 and Table 6). “+” indicates an Odds Ratio (OR) with a 95% Confidence Interval (CI) entirely above 1.0, suggesting a statistically significant positive association. “—” indicates no statistically significant association. Abbreviations: RSV, respiratory syncytial virus; GBS, group B streptococcus.
Author Contributions
Conceptualization, K.H., S.O., M.T., E.M. and S.A.; methodology, K.H., S.O., M.T., E.M. and S.A.; software, K.H.; validation, K.H. and S.O.; formal analysis, K.H.; investigation, K.H., M.Y., M.S., C.A., A.T., M.H., A.M. and A.K.; resources, K.H.; data curation, K.H.; writing—original draft preparation, K.H.; writing—review and editing, K.H., S.O., M.T., E.M. and S.A.; visualization, K.H.; supervision, K.H.; project administration, K.H.; funding acquisition, S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by JSPS KAKENHI, grant number 25K11763.
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Yokohama City University Medical Center Hospital (Approval No. IPPAN 2024-019; date of approval: 17 July 2024).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The datasets presented in this article are not readily available because they are part of an ongoing study. Requests to access the datasets were made by the corresponding author.
Acknowledgments
We express our sincere gratitude to all medical professionals who cooperated in distributing the questionnaire and to all respondents who took the time to respond. We would also like to express our sincere gratitude to Namiki for his cooperation in distributing the questionnaires.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| CI | Confidence Interval |
| DTaP | diphtheria, tetanus, and acellular pertussis (vaccine) |
| FIGO | International Federation of Gynecology and Obstetrics |
| GBS | group B streptococcus |
| ICSI | Intracytoplasmic Sperm Injection |
| IVF | In Vitro Fertilization |
| JPY | Japanese Yen |
| OR | Odds Ratio |
| DT | respiratory syncytial virus |
| SNS | Social Networking Service |
| Tdap | tetanus, diphtheria, and acellular pertussis (vaccine) |
References
- Chu, H.Y.; Englund, J.A. Maternal immunization. Clin. Infect. Dis. 2014, 59, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.L. Prevention of pertussis, tetanus, and diphtheria with vaccines in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MWR Recomm. Rep. 2018, 67, 1. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Pertussis vaccines: WHO position paper—September 2015. Wkly Epidemiol. Rec. 2015, 90, 433–458. [Google Scholar]
- CDC. Guidelines for Vaccinating Pregnant Women. Available online: https://www.cdc.gov/vaccines-pregnancy/hcp/vaccination-guidelines/ (accessed on 15 July 2025).
- WHO. WHO Vaccine Position Papers. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/policies/position-papers (accessed on 15 July 2025).
- Hiiragi, K.; Obata, S.; Miyagi, E.; Aoki, S. The current status, attitudes, and practices concerning maternal pertussis vaccination in obstetric delivery facilities in Kanagawa Prefecture, Japan: A questionnaire survey. Hum. Vaccin. Immunother. 2021, 17, 4235–4238. [Google Scholar] [CrossRef] [PubMed]
- Kurasawa, K. Maternal vaccination-current status, challenges, and opportunities. J. Obstet. Gynaecol. Res. 2023, 49, 493–509. [Google Scholar] [CrossRef] [PubMed]
- Kitano, T.; Onishi, T.; Takeyama, M.; Shima, M. Questionnaire survey on maternal pertussis vaccination for pregnant women and mothers in Nara Prefecture, Japan. Hum. Vaccin. Immunother. 2020, 16, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Anderson, A.S.; Absalon, J.; Radley, D.; Simon, R.; Jongihlati, B.; Strehlau, R.; van Niekerk, A.M.; Izu, A.; Naidoo, N.; et al. Potential for maternally administered vaccine for infant Group B streptococcus. N. Engl. J. Med. 2023, 389, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Blázquez-Gamero, D.; Bernstein, D.I.; Gantt, S.; Bautista, O.; Beck, K.; Conlon, A.; Rosenbloom, D.I.S.; Wang, D.; Ritter, M.; et al. Safety, efficacy, and immunogenicity of a replication-defective human cytomegalovirus vaccine, V160, in cytomegalovirus-seronegative women: A double-blind, randomised, placebo-controlled, phase 2b trial. Lancet Infect. Dis. 2023, 23, 1383–1394. [Google Scholar] [CrossRef] [PubMed]
- Hansen, B.T.; Winje, B.A.; Stålcrantz, J.; Greve-Isdahl, M. Predictors of maternal pertussis vaccination acceptance among pregnant women in Norway. Hum. Vaccin. Immunother. 2024, 20, 2361499. [Google Scholar] [CrossRef] [PubMed]
- Li, W.F.; Huang, S.Y.; Peng, H.H.; Chang, Y.L.; Chang, S.D.; Cheng, P.J.; Taiwan Prenatal Pertussis Immunization Program (PPIP) Collaboration Group. Factors affecting pregnant women’s decisions regarding prenatal pertussis vaccination: A decision-making study in the nationwide Prenatal Pertussis Immunization Program in Taiwan. Taiwan J. Obstet. Gynecol. 2020, 59, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Dudley, M.Z.; Limaye, R.J.; Omer, S.B.; O’Leary, S.T.; Ellingson, M.K.; Spina, C.I.; Brewer, S.E.; Chamberlain, A.T.; Bednarczyk, R.A.; Malik, F.; et al. Characterizing the vaccine knowledge, attitudes, beliefs, and intentions of pregnant women in Georgia and Colorado. Hum. Vaccin. Immunother. 2020, 16, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Gavaruzzi, T.; Ceccarelli, A.; Nanni, C.; Vignali, C.; Colonnello, V.; Caserotti, M.; Riccò, M.; Gori, D. Knowledge and attitudes regarding respiratory syncytial virus (RSV) prevention: A systematic review. Vaccines 2025, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Yahata, Y.; Kamiya, H.; Griffith, M.M.; Tsuchihashi, Y.; Kawakami, S.; Nii, S.; Sunagawa, T. Knowledge, attitudes, and practices associated with pertussis vaccination during pregnancy: Japan, 2016–2017. Jpn. J. Infect. Dis. 2021, 74, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Oka, E.; Ueda, Y.; Yagi, A.; Machida, M.; Furuse, Y.; Tabuchi, T. Challenges to promoting maternal respiratory syncytial virus vaccination in Japan. Vaccine 2025, 48, 126767. [Google Scholar] [CrossRef] [PubMed]
- McAuslane, H.; Utsi, L.; Wensley, A.; Coole, L. Inequalities in maternal pertussis vaccination uptake: A cross-sectional survey of maternity units. J. Public Health 2018, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Japan Society of Obstetrics and Gynecology; Japan Association of Obstetricians and Gynecologists. 2008 Guidelines for Obstetrics and Gynecology, Obstetrics Part. Available online: http://www.jaog.or.jp/wp/wp-content/uploads/2017/01/guide_2008.pdf (accessed on 28 June 2025). (In Japanese).
- Japan Society of Obstetrics and Gynecology; Japan Association of Obstetricians and Gynecologists. 2011 Guidelines for Obstetrics and Gynecology, Obstetrics Part. Available online: http://www.jaog.or.jp/sep2012/diagram/notes/guide_2011.pdf (accessed on 28 June 2025). (In Japanese).
- Shono, A.; Hoshi, S.L.; Kondo, M. Maternal influenza vaccination relates to receiving relevant information among pregnant women in Japan. Hum. Vaccin. Immunother. 2020, 16, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Japan Society of Obstetrics and Gynecology; Japan Association of Obstetricians and Gynecologists. 2023 Guidelines for Obstetrics and Gynecology, Obstetrics Part. Available online: https://www.jsog.or.jp/activity/pdf/gl_sanka_2023.pdf (accessed on 28 June 2025). (In Japanese).
- Benedetto, C.; Borella, F.; Divakar, H.; O’Riordan, S.L.; Mazzoli, M.; Hanson, M.; O’Reilly, S.; Jacobsson, B.; Conry, J.A.; McAuliffe, F.M.; et al. FIGO Preconception Checklist: Preconception care for mother and baby. Int. J. Gynaecol. Obstet. 2024, 165, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kupka, M.S.; Chambers, G.M.; Dyer, S.; Zegers-Hochschild, F.; de Mouzon, J.; Ishihara, O.; Banker, M.; Jwa, S.C.; Fu, B.; Elgindy, E.; et al. World Report. International Committee for Monitoring Assisted Reproductive Technology world report: Assisted reproductive technology, 2015 and 2016. Fertil. Steril. 2024, 122, 875–893. [Google Scholar] [CrossRef] [PubMed]
- ACOG Maternal RSV Vaccination. Available online: https://www.acog.org/clinical-information/physician-faqs/maternal-rsv-vaccination (accessed on 13 March 2025).
- Hoshi, S.L.; Seposo, X.; Okubo, I.; Kondo, M. Cost-effectiveness analysis of pertussis vaccination during pregnancy in Japan. Vaccine 2018, 36, 5133–5140. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, S.L.; Shono, A.; Seposo, X.; Okubo, I.; Kondo, M. Cost-effectiveness analysis of influenza vaccination during pregnancy in Japan. Vaccine 2020, 38, 7363–7371. [Google Scholar] [CrossRef] [PubMed]
- Gebretekle, G.B.; Yeung, M.W.; Ximenes, R.; Cernat, A.; Simmons, A.E.; Killikelly, A.; Siu, W.; Rafferty, E.; Brousseau, N.; Tunis, M.; et al. Cost-effectiveness of RSVpreF vaccine and nirsevimab for the prevention of respiratory syncytial virus disease in Canadian infants. Vaccine 2024, 42, 126164. [Google Scholar] [CrossRef] [PubMed]
- Hutton, D.W.; Prosser, L.A.; Rose, A.M.; Mercon, K.; Ortega-Sanchez, I.R.; Leidner, A.J.; McMorrow, M.L.; Fleming-Dutra, K.E.; Prill, M.M.; Pike, J.; et al. Cost-effectiveness of maternal vaccination to prevent respiratory syncytial virus illness. Pediatrics 2024, 154, e2024066481. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: An overview. Hum. Vaccin. Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, H.; Takei, Y.; Ishikawa, Y.; Saga, Y.; Machida, S.; Taneichi, A.; Suzuki, M. Community-based interventions to improve HPV vaccination coverage among 13- to 15-year-old females: Measures implemented by local governments in Japan. PLoS ONE 2013, 8, e84126. [Google Scholar] [CrossRef] [PubMed]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Tao, L.; Liu, J. Association between risk perception and influenza vaccine hesitancy for children among reproductive women in China during the COVID-19 pandemic: A national online survey. BMC Public Health 2022, 22, 385. [Google Scholar] [CrossRef] [PubMed]
- Del Riccio, M.; Guida, A.; Boudewijns, B.; Heemskerk, S.; van Summeren, J.; Schneeberger, C.; Stelma, F.; van Der Velden, K.; Timen, A.; Caini, S. A missed opportunity? Exploring changes in influenza vaccination coverage during the COVID-19 pandemic: Data from 12 countries worldwide. Influenza Other Respir. Viruses 2025, 19, e70057. [Google Scholar] [CrossRef] [PubMed]
- Cosma, C.; Radi, A.; Cattano, R.; Zanobini, P.; Bonaccorsi, G.; Lorini, C.; Del Riccio, M. Exploring chatbot contributions to enhancing vaccine literacy and uptake: A scoping review of the literature. Vaccine 2025, 44, 126559. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).