
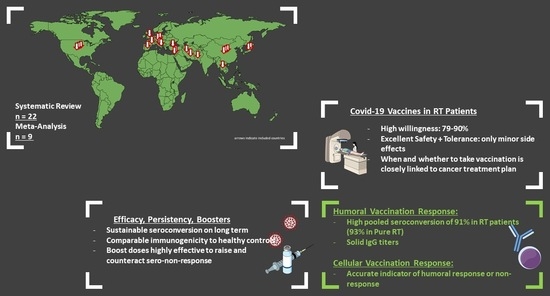
Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Radiation–Oncology Patients: A Systematic Review and Meta-Analysis
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
- (1)
- The study investigated an oncologic population of individuals aged 18 years or older.
- (2)
- Individuals received COVID-19 vaccination and underwent RT within the preceding 12 months.
- (3)
- Vaccine administration preceded RT, except in studies considering the circumstances of vaccination, e.g., willingness, hesitancy, or decision-influencing factors.
- (4)
- Immunological information, including side effects and/or data about the circumstances of vaccination, was reported.
- (5)
- The study design corresponded to at least level II evidence, in line with the Oxford Centre for Evidence-Based Medicine [12].
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AU | Arbitrary Units |
| BAU | Binding Antibody Units |
| CI | Confidence Interval |
| COVID-19 | Coronavirus Disease 2019 |
| IgG | Immunoglobulin G |
| mRNA | Messenger Ribonucleic Acid |
| OR | Odds Ratio |
| RT | Radiotherapy |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SC | Seroconversion |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICO-Strategy. | |
|---|---|
| Patients | Cancer patients undergoing radiotherapy, aged 18 years or older |
| Intervention | COVID-19 vaccination administered before or concurrently to radiotherapy |
| Comparison | If applicable: healthy controls or other treatment modalities |
| Outcome | Immunogenicity and circumstances of vaccination |




References
- Nogueira, L.M.; Schafer, E.J.; Fan, Q.; Wagle, N.S.; Zhao, J.; Shi, K.S.; Han, X.; Jemal, A.; Yabroff, K.R. Assessment of Changes in Cancer Treatment During the First Year of the COVID-19 Pandemic in the US. JAMA Oncol. 2024, 10, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Spencer, K.; Jones, C.M.; Girdler, R.; Roe, C.; Sharpe, M.; Lawton, S.; Miller, L.; Lewis, P.; Evans, M.; Sebag-Montefiore, D.; et al. The impact of the COVID-19 pandemic on radiotherapy services in England, UK: A population-based study. Lancet Oncol. 2021, 22, 309–320. [Google Scholar] [CrossRef]
- Lemos, A.E.G.; Silva, G.R.; Gimba, E.R.P.; Matos, A.D.R. Susceptibility of lung cancer patients to COVID-19: A review of the pandemic data from multiple nationalities. Thorac. Cancer 2021, 12, 2637–2647. [Google Scholar] [CrossRef] [PubMed]
- Di Felice, G.; Visci, G.; Teglia, F.; Angelini, M.; Boffetta, P. Effect of cancer on outcome of COVID-19 patients: A systematic review and meta-analysis of studies of unvaccinated patients. eLife 2022, 11, e74634. [Google Scholar] [CrossRef]
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst. Rev. 2022, 12, CD015477. [Google Scholar] [CrossRef] [PubMed]
- Javadinia, S.A.; Alizadeh, K.; Mojadadi, M.-S.; Nikbakht, F.; Dashti, F.; Joudi, M.; Harati, H.; Welsh, J.S.; Farahmand, S.A.; Attarian, F. COVID-19 Vaccination in Patients With Malignancy; A Systematic Review and Meta-Analysis of the Efficacy and Safety. Front. Endocrinol. 2022, 13, 860238. [Google Scholar] [CrossRef]
- Hwang, J.K.; Zhang, T.; Wang, A.Z.; Li, Z. COVID-19 vaccines for patients with cancer: Benefits likely outweigh risks. J. Hematol. Oncol. 2021, 14, 38. [Google Scholar] [CrossRef] [PubMed]
- Piras, A.; Venuti, V.; D’Aviero, A.; Cusumano, D.; Pergolizzi, S.; Daidone, A.; Boldrini, L. COVID-19 and radiotherapy: A systematic review after 2 years of pandemic. Clin. Transl. Imaging 2022, 10, 611–630. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Ottawa Hospital Research Institute. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 24 June 2025).
- OCEBM Levels of Evidence Working Group. The Oxford Levels of Evidence 2, Oxford Centre for Evidence-Based Medicine; OCEBM Levels of Evidence Working Group: Oxford, UK, 2011. [Google Scholar]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Kohl, C.; McIntosh, E.J.; Unger, S.; Haddaway, N.R.; Kecke, S.; Schiemann, J.; Wilhelm, R. Online tools supporting the conduct and reporting of systematic reviews and systematic maps: A case study on CADIMA and review of existing tools. Environ. Evid. 2018, 7, 8. [Google Scholar] [CrossRef]
- Clopper, C.J.; Pearson, E.S. The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Ariamanesh, M.; Porouhan, P.; PeyroShabany, B.; Fazilat-Panah, D.; Dehghani, M.; Nabavifard, M.; Hatami, F.; Fereidouni, M.; Welsh, J.S.; Javadinia, S.A. Immunogenicity and Safety of the Inactivated SARS-CoV-2 Vaccine (BBIBP-CorV) in Patients with Malignancy. Cancer Investig. 2022, 40, 26–34. [Google Scholar] [CrossRef]
- Bowes, C.L.; Naranbhai, V.; St Denis, K.J.; Lam, E.C.; Bertaux, B.; Keane, F.K.; Khandekar, M.J.; Balazs, A.B.; Iafrate, J.A.; Gainor, J.F.; et al. Heterogeneous immunogenicity of SARS-CoV-2 vaccines in cancer patients receiving radiotherapy. Radiother. Oncol. 2022, 166, 88–91. [Google Scholar] [CrossRef]
- Chen, C.; Dai, L.; Zheng, C.; Li, H.; Li, X.; Yang, M.; Gao, R.; Yao, J.; Zhang, Z.; Shi, Y.; et al. Antibody response to SARS-CoV-2 WT and Omicron BA.4/5 of inactivated -19 vaccine in patients with lung cancer after second and booster immunization. J. Hematol. Oncol. 2023, 16, 47. [Google Scholar] [CrossRef]
- Geinitz, H.; Silberberger, E.; Spiegl, K.; Feichtinger, J.; Wagner, H.; Hermann, P.; Bräutigam, E.; Track, C.; Weis, E.M.; Venhoda, C.; et al. SARS-CoV-2 vaccination willingness and humoral vaccination response in radiation oncology patients. Vaccine 2024, 42, 945–959. [Google Scholar] [CrossRef] [PubMed]
- Haidar, G.; Agha, M.; Bilderback, A.; Lukanski, A.; Linstrum, K.; Troyan, R.; Rothenberger, S.; McMahon, D.K.; Crandall, M.D.; Sobolewksi, M.D.; et al. Prospective Evaluation of Coronavirus Disease 2019 (COVID-19) Vaccine Responses Across a Broad Spectrum of Immunocompromising Conditions: The COVID-19 Vaccination in the Immunocompromised Study (COVICS). Clin. Infect. Dis. 2022, 75, e630–e644. [Google Scholar] [CrossRef]
- Hong, J.; Xu, X.; Yang, J.; Zheng, J.; Dai, S.; Zhou, J.; Zhang, Q.; Ruan, Y.; Ling, C. Knowledge about, attitude and acceptance towards, and predictors of intention to receive the COVID-19 vaccine among cancer patients in Eastern China: A cross-sectional survey. J. Integr. Med. 2022, 20, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Joudi, M.; Moradi Binabaj, M.; Porouhan, P.; PeyroShabany, B.; Tabasi, M.; Fazilat-Panah, D.; Khajeh, M.; Mehrabian, A.; Dehghani, M.; Welsh, J.S.; et al. A Cohort Study on the Immunogenicity and Safety of the Inactivated SARS-CoV-2 Vaccine (BBIBP-CorV) in Patients With Breast Cancer; Does Trastuzumab Interfere With the Outcome? Front. Endocrinol. 2022, 13, 798975. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef]
- Liu, W.; Wu, Y.; Yang, R.; Chen, R.; Huang, Y.; Zhao, X.; Xie, M.; Li, Q.; Wang, Q.; Chen, J. COVID-19 Vaccination Status and Hesitancy among Breast Cancer Patients after Two Years of Pandemic: A Cross-Sectional Survey. Vaccines 2022, 10, 1530. [Google Scholar] [CrossRef]
- Kian, W.; Zemel, M.; Kestenbaum, E.H.; Rouvinov, K.; Alguayn, W.; Levitas, D.; Ievko, A.; Michlin, R.; Abod, M.A.; Massalha, I.; et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in oncologic patients undergoing numerous cancer treatment options: A retrospective single-center study. Medicine 2022, 101, e28561. [Google Scholar] [CrossRef] [PubMed]
- Narita, D.; Ebina-Shibuya, R.; Miyauchi, E.; Tsukita, Y.; Saito, R.; Murakami, K.; Kimura, N.; Sugiura, H. Antibody responses to second doses of COVID-19 vaccination in lung cancer patients undergoing treatment. Respir. Investig. 2023, 61, 247–253. [Google Scholar] [CrossRef]
- Prayongrat, A.; Noppaving, P.; Chobarporn, T.; Sudhinaraset, N.; Teeyapun, N.; Pakvisal, N.; Jantarabenjakul, W.; Sophonphan, J.; Lertbutsayanukul, C.; Poovorawan, Y. Safety and Immunogenicity of Homologous and Heterologous Adenoviral-Vectored and mRNA COVID-19 Vaccine Regimens in Radiotherapy Patients. Vaccines 2023, 11, 1135. [Google Scholar] [CrossRef] [PubMed]
- Provencio, M.; Estival, A.; Franco, F.; López-Vivanco, G.; Saigí, M.; Arasanz, H.; Diz, P.; Carcereny, E.; García, J.; Aguado, C.; et al. Immunogenicity of COVID-19 vaccines in lung cancer patients. Lung Cancer 2023, 184, 107323. [Google Scholar] [CrossRef]
- Riaz, A.; Alam, A.; Saleem, N. Administration of Sinopharm COVID-19 Vaccine in Cancer Patients. Pak. J. Pharm. Sci. 2023, 36, 67–70. [Google Scholar] [CrossRef]
- Scoccianti, S.; Delli Paoli, C.; Grilli Leonulli, B.; Paoletti, L.; Alpi, P.; Caini, S.; Barca, R.; Fondelli, S.; Russo, S.; Perna, M.; et al. Acute tolerance of Moderna mRNA-1273 vaccine against COVID-19 in patients with cancer treated with radiotherapy. Lancet Oncol. 2021, 22, 1212–1214. [Google Scholar] [CrossRef]
- Scoccianti, S.; Delli Paoli, C.; Infantino, M.; Paoletti, L.; Caini, S.; Meacci, F.; Russo, S.; Esposito, M.; Fondelli, S.; Grilli Leonulli, B.; et al. Immunogenicity after two and three doses of mRNA vaccine in patients with cancer treated with exclusive radiotherapy. Int. Immunopharmacol. 2023, 122, 110460. [Google Scholar] [CrossRef]
- Seegers, V.; Rousseau, G.; Zhou, K.; Blanc-Lapierre, A.; Bigot, F.; Mahammedi, H.; Lambert, A.; Moreau-Bachelard, C.; Campone, M.; Conroy, T.; et al. COVID-19 Infection despite Previous Vaccination in Cancer Patients and Healthcare Workers: Results from a French Prospective Multicenter Cohort (PAPESCO-19). Cancers 2023, 15, 4777. [Google Scholar] [CrossRef]
- Shmueli, E.S.; Itay, A.; Margalit, O.; Berger, R.; Halperin, S.; Jurkowicz, M.; Levin, E.G.; Levy, I.; Olmer, L.; Regev-Yochay, G.; et al. Efficacy and safety of BNT162b2 vaccination in patients with solid cancer receiving anticancer therapy—A single centre prospective study. Eur. J. Cancer 2021, 157, 124–131. [Google Scholar] [CrossRef]
- Suzuki, H.; Akiyama, T.; Ueda, N.; Matsumura, S.; Mori, M.; Namiki, M.; Yamada, N.; Tsutsumi, C.; Tozaki, S.; Iwamoto, H.; et al. COVID-19 Vaccination in Patients with Cancer. Cancers 2022, 14, 2556. [Google Scholar] [CrossRef]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.E2. [Google Scholar] [CrossRef]
- Thöne, P.; Egger, M.; Geroldinger-Simic, M.; Kindermann, H.; Kocik, L.; Karasek, N.; Fischerlehner, B.; Spiegl, K.; Gruber, G.; Aschacher, B.; et al. Immunogenicity Parameters of Cancer Patients Receiving the mRNA Vaccine BNT162b2 While Obtaining Radiotherapy: A Longitudinal Cohort Evaluation. Vaccines 2024, 12, 275. [Google Scholar] [CrossRef]
- Uslu, G.H.; Rakici, S.Y.; Cicek, A.C.; Yazici, Z.A. COVID-19 vaccine immunity in oncology patients. Bratisl. Med. J. 2023, 124, 187–192. [Google Scholar] [CrossRef]
- Soyfer, V.; Gutfeld, O.; Shamai, S.; Schlocker, A.; Merimsky, O. COVID-19 Vaccine-Induced Radiation Recall Phenomenon. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 957–961. [Google Scholar] [CrossRef]
- Marples, R.; Douglas, C.; Xavier, J.; Collins, A.-J. Breast Radiation Recall Phenomenon After Astra-Zeneca COVID-19 Vaccine: A Case Series. Cureus 2022, 14, e21499. [Google Scholar] [CrossRef] [PubMed]
- Tatekawa, S.; Hoshino, S.; Takemoto, N.; Oda, M.; Akino, Y.; Iwahori, K.; Hirata, T.; Hayashi, K.; Tamari, K.; Seo, Y.; et al. COVID-19 vaccine-induced Recurrence of the Radiation Recall Phenomenon in the Laryngeal Mucosa Due to a VEGF Inhibitor. Adv. Radiat. Oncol. 2022, 7, 101048. [Google Scholar] [CrossRef] [PubMed]
- Steber, C.R.; Ponnatapura, J.; Hughes, R.T.; Farris, M.K. Rapid Development of Clinically Symptomatic Radiation Recall Pneumonitis Immediately Following COVID-19 Vaccination. Cureus 2021, 13, e14303. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.W.; Ionescu, M.C.; Starkey, T.; Little, M.; Tilby, M.; Tripathy, A.R.; Mckenzie, H.S.; Al-Hajji, Y.; Appanna, N.; Barnard, M.; et al. COVID-19: Third dose booster vaccine effectiveness against breakthrough coronavirus infection, hospitalisations and death in patients with cancer: A population-based study. Eur. J. Cancer 2022, 175, 1–10. [Google Scholar] [CrossRef]
- Mariniello, D.F.; Aronne, L.; Vitale, M.; Schiattarella, A.; Pagliaro, R.; Komici, K. Current challenges and perspectives in lung cancer care during COVID-19 waves. Curr. Opin. Pulm. Med. 2023, 29, 239–247. [Google Scholar] [CrossRef]
- Prabani, K.I.P.; Weerasekara, I.; Damayanthi, H.D.W.T. COVID-19 vaccine acceptance and hesitancy among patients with cancer: A systematic review and meta-analysis. Public Health 2022, 212, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Chun, J.Y.; Kim, S.I.; Park, E.Y.; Park, S.-Y.; Koh, S.-J.; Cha, Y.; Yoo, H.J.; Joung, J.Y.; Yoon, H.M.; Eom, B.W.; et al. Cancer Patients’ Willingness to Take COVID-19 Vaccination: A Nationwide Multicenter Survey in Korea. Cancers 2021, 13, 3883. [Google Scholar] [CrossRef]
- Thomas, S.J.; Perez, J.L.; Lockhart, S.P.; Hariharan, S.; Kitchin, N.; Bailey, R.; Liau, K.; Lagkadinou, E.; Türeci, Ö.; Şahin, U.; et al. Efficacy and safety of the BNT162b2 mRNA COVID-19 vaccine in participants with a history of cancer: Subgroup analysis of a global phase 3 randomized clinical trial. Vaccine 2022, 40, 1483–1492. [Google Scholar] [CrossRef]
- Shear, S.L.; Shams, K.; Weisberg, J.; Hamidi, N.; Scott, S.C. COVID-19 Vaccination Safety Profiles in Patients With Solid Tumour Cancers: A Systematic Review. Clin. Oncol. 2023, 35, e421–e433. [Google Scholar] [CrossRef]
- So, A.C.P.; McGrath, H.; Ting, J.; Srikandarajah, K.; Germanou, S.; Moss, C.; Russell, B.; Monroy-Iglesias, M.; Dolly, S.; Irshad, S.; et al. COVID-19 Vaccine Safety in Cancer Patients: A Single Centre Experience. Cancers 2021, 13, 3573. [Google Scholar] [CrossRef]
- Becerril-Gaitan, A.; Vaca-Cartagena, B.F.; Ferrigno, A.S.; Mesa-Chavez, F.; Barrientos-Gutiérrez, T.; Tagliamento, M.; Lambertini, M.; Villarreal-Garza, C. Immunogenicity and risk of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection after Coronavirus Disease 2019 (COVID-19) vaccination in patients with cancer: A systematic review and meta-analysis. Eur. J. Cancer 2022, 160, 243–260. [Google Scholar] [CrossRef]
- Yin, J.; Chen, Y.; Li, Y.; Zhang, X.; Wang, C. Seroconversion rate after COVID-19 vaccination in patients with solid cancer: A systematic review and meta-analysis. Hum. Vaccines Immunother. 2022, 18, 2119763. [Google Scholar] [CrossRef]
- Zhang, Z.; Mateus, J.; Coelho, C.H.; Dan, J.M.; Moderbacher, C.R.; Gálvez, R.I.; Cortes, F.H.; Grifoni, A.; Tarke, A.; Chang, J.; et al. Humoral and cellular immune memory to four COVID-19 vaccines. Cell 2022, 185, 2434–2451.E17. [Google Scholar] [CrossRef] [PubMed]
- Martins-Branco, D.; Nader-Marta, G.; Tecic Vuger, A.; Debien, V.; Ameye, L.; Brandão, M.; Punie, K.; Loizidou, A.; Willard-Gallo, K.; Spilleboudt, C.; et al. Immune response to anti-SARS-CoV-2 prime-vaccination in patients with cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2023, 149, 3075–3080. [Google Scholar] [CrossRef]
- Gong, I.Y.; Vijenthira, A.; Betschel, S.D.; Hicks, L.K.; Cheung, M.C. COVID-19 vaccine response in patients with hematologic malignancy: A systematic review and meta-analysis. Am. J. Hematol. 2022, 97, E132–E135. [Google Scholar] [CrossRef]
- Tang, K.; Wei, Z.; Wu, X. Impaired serological response to COVID-19 vaccination following anticancer therapy: A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 4860–4868. [Google Scholar] [CrossRef]
- Yang, W.; Zhang, D.; Li, Z.; Zhang, K. Predictors of poor serologic response to COVID-19 vaccine in patients with cancer: A systematic review and meta-analysis. Eur. J. Cancer 2022, 172, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Rachman, A.; Iriani, A.; Sukrisman, L.; Rajabto, W.; Mulansari, N.A.; Lubis, A.M.; Cahyanur, R.; Prasetyawati, F.; Priantono, D.; Rumondor, B.B.; et al. A comparative study of the COVID-19 vaccine efficacy among cancer patients: mRNA versus non-mRNA. PLoS ONE 2023, 18, e0281907. [Google Scholar] [CrossRef] [PubMed]
- Geinitz, H.; Zimmermann, F.B.; Stoll, P.; Thamm, R.; Kaffenberger, W.; Ansorg, K.; Keller, M.; Busch, R.; Van Beuningen, D.; Molls, M. Fatigue, serum cytokine levels, and blood cell counts during radiotherapy of patients with breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 691–698. [Google Scholar] [CrossRef]
- Sage, E.K.; Schmid, T.E.; Sedelmayr, M.; Gehrmann, M.; Geinitz, H.; Duma, M.N.; Combs, S.E.; Multhoff, G. Comparative analysis of the effects of radiotherapy versus radiotherapy after adjuvant chemotherapy on the composition of lymphocyte subpopulations in breast cancer patients. Radiother. Oncol. 2016, 118, 176–180. [Google Scholar] [CrossRef]
- Mai, A.S.; Lee, A.R.Y.B.; Tay, R.Y.K.; Shapiro, L.; Thakkar, A.; Halmos, B.; Grinshpun, A.; Herishanu, Y.; Benjamini, O.; Tadmor, T.; et al. Booster doses of COVID-19 vaccines for patients with haematological and solid cancer: A systematic review and individual patient data meta-analysis. Eur. J. Cancer 2022, 172, 65–75. [Google Scholar] [CrossRef]
- Petrelli, F.; Luciani, A.; Borgonovo, K.; Ghilardi, M.; Parati, M.C.; Petrò, D.; Lonati, V.; Pesenti, A.; Cabiddu, M. Third dose of SARS-CoV-2 vaccine: A systematic review of 30 published studies. J. Med. Virol. 2022, 94, 2837–2844. [Google Scholar] [CrossRef]
- Al Hajji, Y.; Taylor, H.; Starkey, T.; Lee, L.Y.W.; Tilby, M. Antibody response to a third booster dose of SARS-CoV-2 vaccination in adults with haematological and solid cancer: A systematic review. Br. J. Cancer 2022, 127, 1827–1836. [Google Scholar] [CrossRef] [PubMed]
- Corti, C.; Antonarelli, G.; Scotté, F.; Spano, J.P.; Barrière, J.; Michot, J.M.; André, F.; Curigliano, G. Seroconversion rate after vaccination against COVID-19 in patients with cancer—A systematic review. Ann. Oncol. 2022, 33, 158–168. [Google Scholar] [CrossRef] [PubMed]




| No. | Study | Year | Country | N Total | N Pure Radiotherapy | Study Design | Level of Evidence | Source |
|---|---|---|---|---|---|---|---|---|
| 1 | Ariamanesh et al. | 2021 | Iran | 364 | 49 | Longitudinal | II | [18] |
| 2 | Bowes et al. | 2021 | USA | 33 | 33 | Longitudinal | II | [19] |
| 3 | Chen et al. | 2023 | China | 260 | 17 | Longitudinal | II | [20] |
| 4 | Geinitz et al. | 2024 | Austria | 1142 | 1142 | Cross-sectional | II | [21] |
| 5 | Haidar et al. | 2022 | USA | 1099 | 61 | Cross-sectional | II | [22] |
| 6 | Hong et al. | 2021 | China | 2158 | 82 | Cross-sectional | II | [23] |
| 7 | Joudi et al. | 2022 | Iran | 160 | 20 | Longitudinal | II | [24] |
| 8 | Lee et al. | 2022 | UK | 2,258,553 | not specified | Longitudinal | II | [25] |
| 9 | Liu et al. | 2022 | China | 1132 | 117 | Cross-sectional | II | [26] |
| 10 | Kian et al. | 2022 | Israel | 210 | 9 | Longitudinal | II | [27] |
| 11 | Narita et al. | 2022 | Japan | 69 | 3 | Cross-sectional | II | [28] |
| 12 | Prayongrat et al. | 2023 | Thailand | 53 | 53 | Longitudinal | II | [29] |
| 13 | Provenico et al. | 2023 | Spain | 1973 | 186 | Cross-sectional | II | [30] |
| 14 | Riaz et al. | 2023 | Pakistan | 150 | 20 | Longitudinal | II | [31] |
| 15 | Scoccianti et al. | 2021 | Italy | 153 | 153 | Longitudinal | II | [32] |
| 16 | Scoccianti et al. | 2023 | Italy | 92 | 92 | Longitudinal | II | [33] |
| 17 | Seegers et al. | 2023 | France | 840 | 361 | Longitudinal | II | [34] |
| 18 | Shmueli et al. | 2021 | Israel | 129 | 6 | Longitudinal | I | [35] |
| 19 | Suzuki et al. | 2022 | Japan | 1182 | 20 | Longitudinal | II | [36] |
| 20 | Takkar et al. | 2021 | USA | 200 | 55 | Cross-sectional | II | [37] |
| 21 | Thöne et al. | 2024 | Austria | 46 | 46 | Longitudinal | II | [38] |
| 22 | Uslu et al. | 2023 | Turkey | 81 | 72 | Cross-sectional | II | [39] |
| Ref. | Study | Seroconversion (%) | N Total | N Pure Radiotherapy | Chemotherapy | Vaccine | Prior Radiotherapy | Cancer Types in Total Study Population | Serology After | Assay | Threshold |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [18] | Ariamanesh 2021 | 92.5% | 40 | 40 | - | 5 | ongoing | solid 93.4%, hematologic 6.6% | 2 months | ELIZA | 8 mg/mL |
| [19] | Bowes 2021 | 100.0% | 33 | 20 | 13 | 1, 2, 4 | <3 months | solid 100% | ≥2 weeks | Elecsys | 0.8 U/mL |
| [22] | Haidar 2022 | 82.1% | 67 | <12 months | solid 91.0%, hematologic 9.0% | ≥2_weeks | Beckman Coulter | 0.8 U/mL | |||
| [28] | Narita 2022 | 100.0% | 3 | 3 | - | 1, 2 | <3 months | solid 100% | 2–40 days | Lumipulse | |
| [29] | Prayongrat 2023 | 97.1% | 35 | 1, 2, 3 | <4 weeks | solid 100% | 4 weeks | Elecsys | 0.8 U/mL | ||
| [31] | Riaz 2023 | 90.0% | 20 | 20 | - | 5 | ongoing | solid 93.3%, hematologic 6.7% | 2 months | ELIZA | 8 µg/mL |
| [33] | Scoccianti 2023 | 93.5% | 92 | 92 | - | 1, 2 | <6 months | solid 88.1%, hematologic 4.3%, further | 4–5 months | EliA | 40 BAU/mL |
| [35] | Shmueli 2021 | 50.0% | 6 | 5 | 1 | 1 | ongoing | solid 100% | 2–4 weeks | ELIZA | 0.8 U/mL |
| [38] | Thöne 2024 Pure RT | 95.2% | 21 | 21 | - | 1 | ongoing | solid 100% | 2 weeks | ELIZA | 0.8 U/mL |
| [38] | Thöne 2024 RT + Chemo | 77.8% | 18 | 18 | 1 | ongoing | solid 100% | 2 weeks | ELIZA | 0.8 U/mL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thöne, P.; Egger, M.; Gruber, M.S.; Gruber, G.; Kasassov, C.; Nyiri, D.; Weis, E.; Werl, H.; Trinkl, L.; Lilleby, W.; et al. Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Radiation–Oncology Patients: A Systematic Review and Meta-Analysis. Vaccines 2025, 13, 715. https://doi.org/10.3390/vaccines13070715
Thöne P, Egger M, Gruber MS, Gruber G, Kasassov C, Nyiri D, Weis E, Werl H, Trinkl L, Lilleby W, et al. Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Radiation–Oncology Patients: A Systematic Review and Meta-Analysis. Vaccines. 2025; 13(7):715. https://doi.org/10.3390/vaccines13070715
Chicago/Turabian StyleThöne, Paul, Margot Egger, Michael Stephan Gruber, Georg Gruber, Christina Kasassov, Dalma Nyiri, Eva Weis, Helene Werl, Leonhard Trinkl, Wolfgang Lilleby, and et al. 2025. "Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Radiation–Oncology Patients: A Systematic Review and Meta-Analysis" Vaccines 13, no. 7: 715. https://doi.org/10.3390/vaccines13070715
APA StyleThöne, P., Egger, M., Gruber, M. S., Gruber, G., Kasassov, C., Nyiri, D., Weis, E., Werl, H., Trinkl, L., Lilleby, W., Clodi, M., Bräutigam, E., Dieplinger, B., Aigner, A., & Geinitz, H. (2025). Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Radiation–Oncology Patients: A Systematic Review and Meta-Analysis. Vaccines, 13(7), 715. https://doi.org/10.3390/vaccines13070715