
Strengthening Vaccine Regulation: Insights from COVID-19 Vaccines, Best Practices, and Lessons for Future Public Health Emergencies

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Setting and Participants
2.3. Data Collection Methods
2.4. Variables and Measures
3. Results
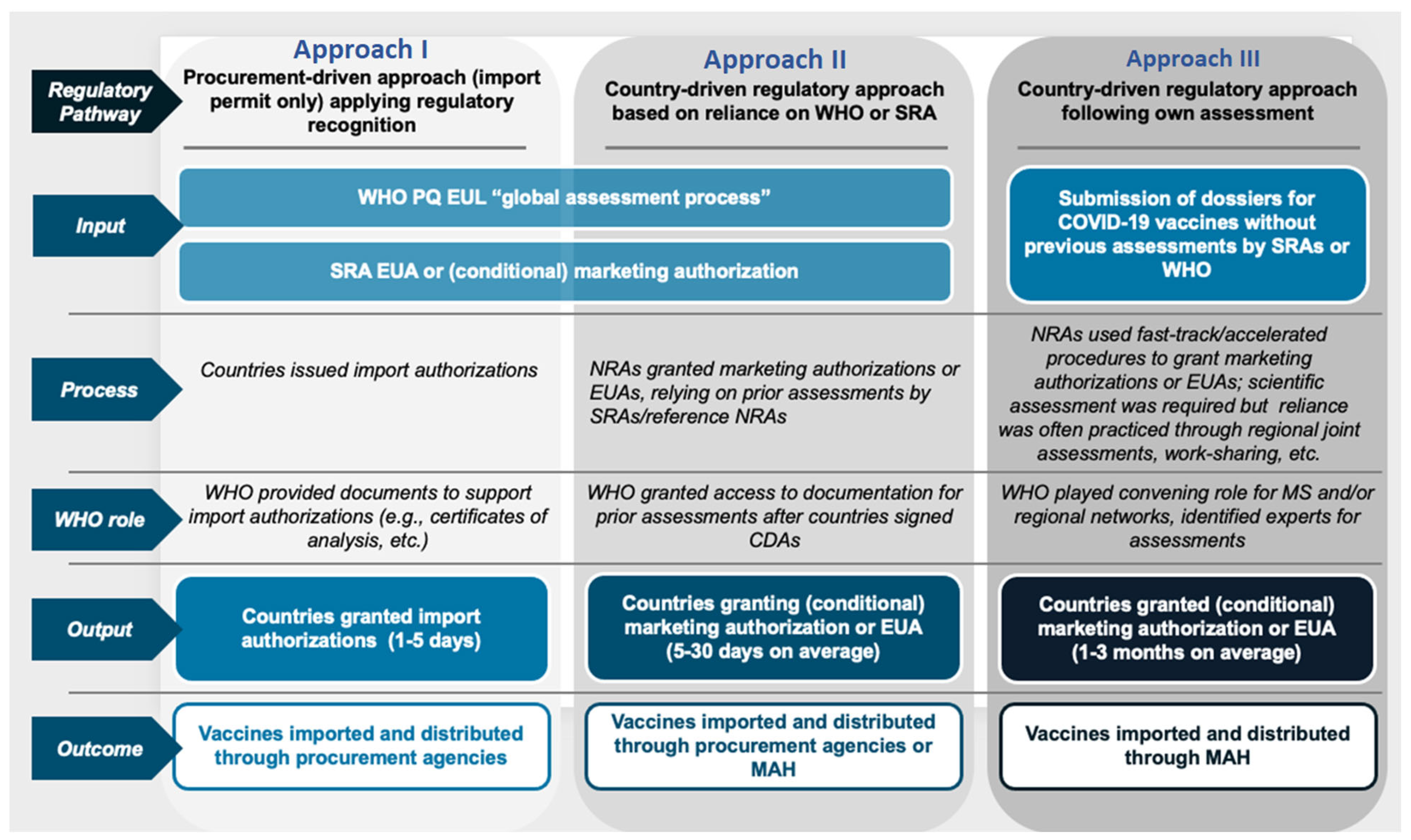
3.1. Approaches to Regulatory Approvals
3.2. Types of Regulatory Flexibilities Applied to COVID-19 Regulatory Approvals
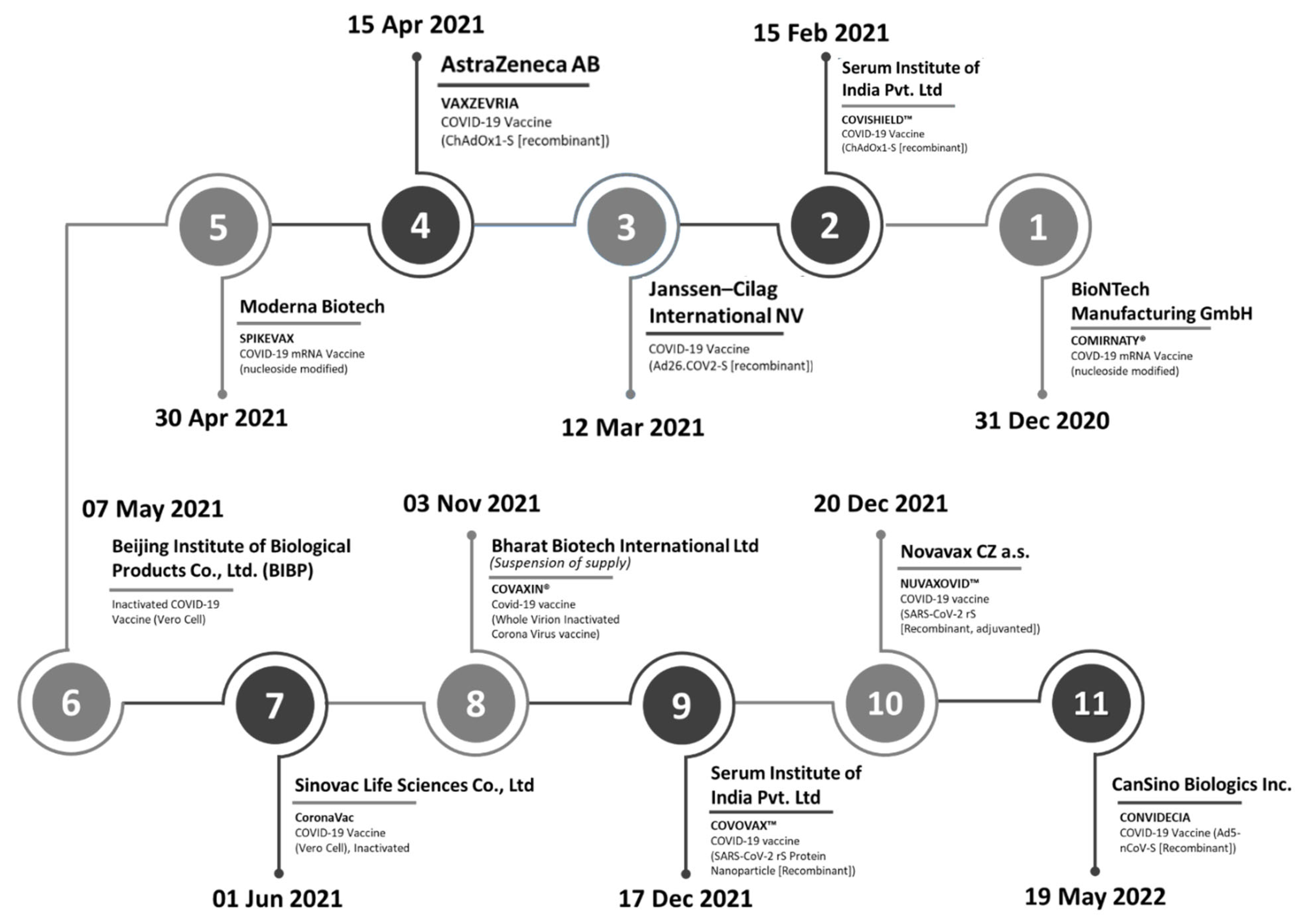
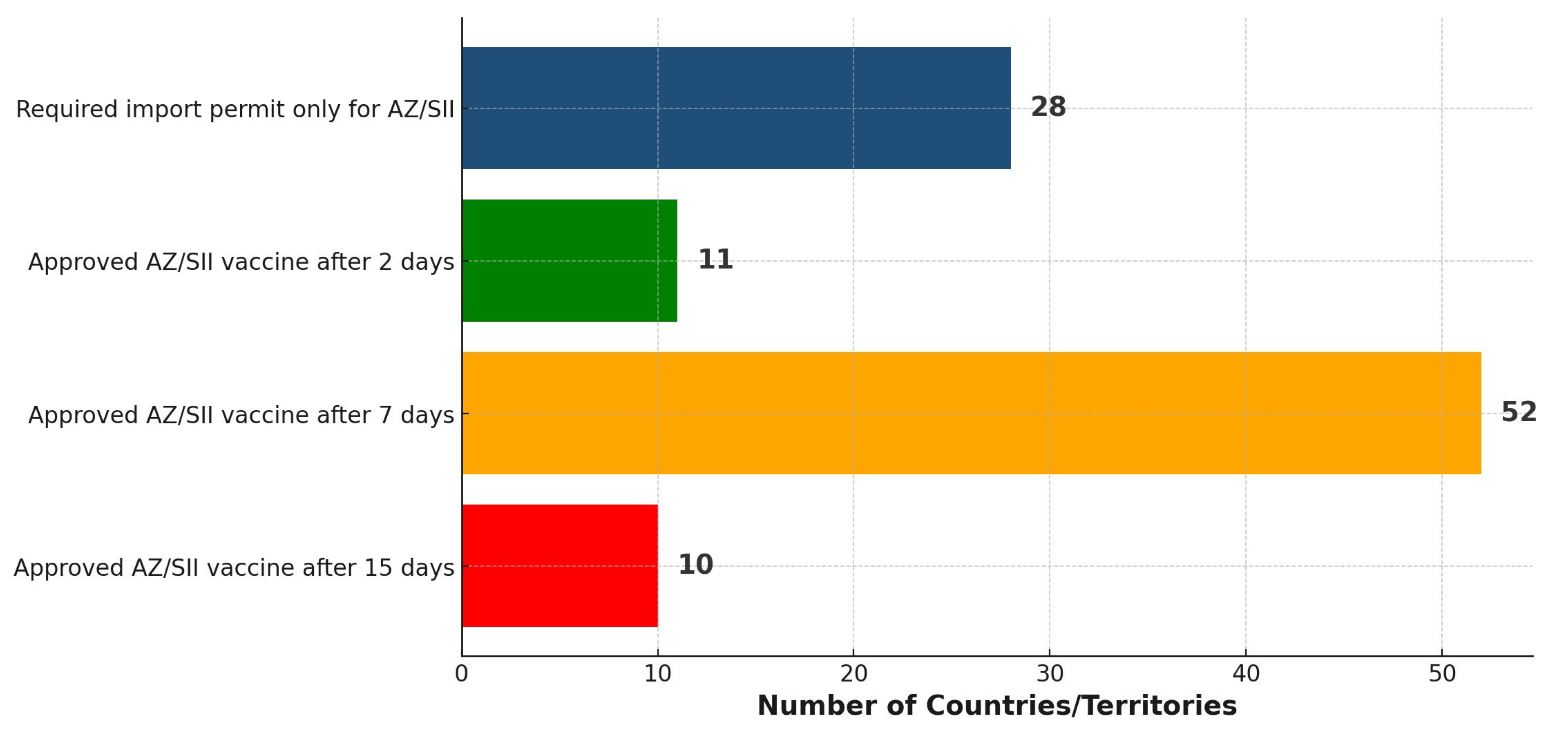
3.3. Status and Timing of Member State Approvals
3.4. Wealth Status and Regulatory Maturity Level as Predictors of Timely Acceptance of Vaccines
3.5. Other Reported Best Practices Around Approvals of COVID-19 Vaccines
3.6. Lessons Learned
4. Discussion
4.1. Approaches to Issuing Regulatory Approval for COVID-19 Vaccines by NRAs
4.2. Adopted Regulatory Flexibilities for Approval of COVID-19 Vaccines
4.3. Effect of WHO EUL on the Status and Timing of COVID-19 Regulatory Approvals
4.4. Variation of COVID-19 Vaccines Approval Timelines with Wealth Status and Regulatory Maturity Levels
4.5. Adopted Best Practices and the Essence of Sustaining Them Beyond the Pandemic
4.6. Lessons Learned: Integrating Key Insights
4.7. Study Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khorram-Manesh, A.; Goniewicz, K.; Burkle, F.M., Jr. Unleashing the global potential of public health: A framework for future pandemic response. J. Infect. Public Health 2024, 17, 82–95. [Google Scholar] [CrossRef] [PubMed]
- Prieto, A.; Huang, R.; Eusebi, C.A.; Shostak, M. A Brief Overview of Emerging Vaccine Technologies for Pandemic Preparedness. Rand Health Q. 2023, 11, 6. [Google Scholar] [PubMed]
- Ahonkhai, V.; Martins, S.F.; Portet, A.; Lumpkin, M.; Hartman, D. Speeding access to vaccines and medicines in low-and middle-income countries: A case for change and a framework for optimized product market authorization. PLoS ONE 2016, 11, e0166515. [Google Scholar] [CrossRef]
- WHO. Guidelines on Regulatory Preparedness for the Oversight of Pandemic or Other Emergency Use Vaccines in Importing Countries; TRS 1054, Annex 2; WHO: Geneva, Switzerland, 2024. [Google Scholar]
- Mukherjee, S.; Goodman, L. Strengthening regulatory systems globally: A crucial step towards pandemic preparedness and response. BMJ Glob. Health 2023, 8, e012883. [Google Scholar] [CrossRef]
- Baylor, N.W.; Goodman, J.L. Vaccine preparedness for the next influenza pandemic: A regulatory perspective. Vaccines 2022, 10, 2136. [Google Scholar] [CrossRef]
- World Health Organization. Considerations for Evaluation of COVID-19 Vaccines (Revised); World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Guzman, J.; O’Connell, E.; Kikule, K.; Hafner, T. The WHO Global Benchmarking Tool: A game changer for strengthening national regulatory capacity. BMJ Glob. Health 2020, 5, e003181. [Google Scholar] [CrossRef]
- Khadem Broojerdi, A.; Baran Sillo, H.; Ostad Ali Dehaghi, R.; Ward, M.; Refaat, M.; Parry, J. The World Health Organization global benchmarking tool an instrument to strengthen medical products regulation and promote universal health coverage. Front. Med. 2020, 7, 457. [Google Scholar] [CrossRef]
- Khadem Broojerdi, A.; Alfonso, C.; Ostad Ali Dehaghi, R.; Refaat, M.; Sillo, H.B. Worldwide assessment of low-and middle-income countries’ regulatory preparedness to approve medical products during public health emergencies. Front. Med. 2021, 8, 722872. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Benchmarking Tool (GBT) for Evaluation of National Regulatory Systems of Medical Products, Revision VI; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Good reliance practices in the regulation of medical products: High level principles and considerations. In WHO Expert Committee On Specifications for Pharmaceutical Preparations: Fifty-Fifth Report; Annex 10; World Health Organization: Geneva, Switzerland, 2021; pp. 237–267. [Google Scholar]
- Ngum, N.; Ndomondo-Sigonda, M.; Habonimana, R.; Siyoi, F.; Irasabwa, C.; Ojukwu, J.; Apolinary, F.; Okello, A.; Ahmada, S.; Walker, S. Evaluation of the review models and approval timelines of authorities participating in the East African Medicine Regulatory Harmonisation initiative: Alignment and strategies for moving forward. Front. Med. 2024, 11, 1438041. [Google Scholar] [CrossRef]
- Broojerdi, A.K.; Salvati, A.L.; Abdelfattah, M.R.; Dehaghi, R.O.A.; Sillo, H.B.; Gaspar, R. WHO-listed authorities (WLA) framework: Transparent evidence-based approach for promoting regulatory reliance towards increased access to quality-assured medical products. Front. Med. 2024, 11, 1467229. [Google Scholar] [CrossRef]
- Collaborative Registration Procedure for Medical Products. Available online: https://www.who.int/teams/regulation-prequalification/regulation-and-safety/facilitated-product-introduction/collaborative-registration-procedure (accessed on 4 June 2025).
- Dellepiane, N.; Wood, D. Twenty-five years of the WHO vaccines prequalification programme (1987–2012): Lessons learned and future perspectives. Vaccine 2015, 33, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Kim, E. Exploring Future Pandemic Preparedness Through the Development of Preventive Vaccine Platforms and the Key Roles of International Organizations in a Global Health Crisis. Vaccines 2025, 13, 56. [Google Scholar] [CrossRef] [PubMed]
- Saeed, M.A.; Saltan, B.A.; Saeed, M.R.; Khokhar, H.; Zaidi, A.; Usman, M.; Marzook, F. Unveiling the Emergency Use Authorization of COVID-19 Vaccines: Safety, Efficacy and Public Trust. Fortune J. Health Sci. 2024, 7, 656–664. [Google Scholar] [CrossRef]
- Edo, K.; Kawano, M.; Maeda, H. Comparison of regulatory approval system for medicines in emergency among Japan, the United States, the United Kingdom, Europe, and China. PLoS ONE 2024, 19, e0309992. [Google Scholar] [CrossRef]
- van der Zee, I.T.; Vreman, R.A.; Liberti, L.; Garza, M.A. Regulatory reliance pathways during health emergencies: Enabling timely authorizations for COVID-19 vaccines in Latin America. Rev. Panam. Salud Pública 2023, 46, e115. [Google Scholar] [CrossRef]
- Bolislis, W.R.; De Lucia, M.L.; Dolz, F.; Mo, R.; Nagaoka, M.; Rodriguez, H.; Woon, M.L.; Yu, W.; Kühler, T.C. Regulatory agilities in the time of covid-19: Overview, trends, and opportunities. Clin. Ther. 2021, 43, 124–139. [Google Scholar] [CrossRef]
- Geraci, G.; Bernat, J.; Rodier, C.; Acha, V.; Acquah, J.; Beakes-Read, G. Medicinal Product Development and Regulatory Agilities Implemented During the Early Phases of the COVID-19 Pandemic: Experiences and Implications for the Future—An Industry View. Ther. Innov. Regul. Sci. 2023, 57, 940–951. [Google Scholar] [CrossRef]
- Wagner, R.; Hildt, E.; Grabski, E.; Sun, Y.; Meyer, H.; Lommel, A.; Keller-Stanislawski, B.; Müller-Berghaus, J.; Cichutek, K. Accelerated development of COVID-19 vaccines: Technology platforms, benefits, and associated risks. Vaccines 2021, 9, 747. [Google Scholar] [CrossRef]
- Klein, K.; Stolk, P.; Tellner, P.; Acha, V.; Montagne, S.; Stöckert, I. Regulatory flexibilities and guidances for addressing the challenges of COVID-19 in the EU: What can we learn from company experiences? Ther. Innov. Regul. Sci. 2022, 56, 366–377. [Google Scholar] [CrossRef]
- Tshering, D.; Chejor, P. Regulatory flexibilities and access to COVID-19 vaccines during the pandemic in Bhutan. Exp. Res. Clin. Soc. Pharm. 2022, 7, 100156. [Google Scholar] [CrossRef]
- Lumpkin, M.M.; Lim, J.C. Pandemic best regulatory practices: An urgent need in the COVID-19 pandemic. Clin. Pharmacol. Ther. 2020, 108, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, J.; Maanvizhi, S. Regulatory approval pathway for COVID-19 vaccine in USA, Europe and India. Ann. Med. Surg. 2023, 85, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Maeda, H.; Endo, H.; Yamamoto, H.; Miyata, H.; Munekage, M.; Taketomi, A.; Kakeji, Y.; Seto, Y.; Yoshida, K.; Yamaue, H. Effects of the COVID-19 pandemic on gastroenterological surgeries in 2020: A study using the National Clinical Database of Japan. Ann. Gastroenterol. Surg. 2023, 7, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Banoun, H. mRNA: Vaccine or gene therapy? The safety regulatory issues. Int. J. Mol. Sci. 2023, 24, 10514. [Google Scholar] [CrossRef]
- Acharya, K.P.; Ghimire, T.R.; Subramanya, S.H. Access to and equitable distribution of COVID-19 vaccine in low-income countries. NPJ Vaccines 2021, 6, 54. [Google Scholar] [CrossRef]
- Duan, Y.; Shi, J.; Wang, Z.; Zhou, S.; Jin, Y.; Zheng, Z.-J. Disparities in COVID-19 vaccination among low-, middle-, and high-income countries: The mediating role of vaccination policy. Vaccines 2021, 9, 905. [Google Scholar] [CrossRef]
- Markowitz, L.E.; Hopkins, R.H., Jr.; Broder, K.R.; Lee, G.M.; Edwards, K.M.; Daley, M.F.; Jackson, L.A.; Nelson, J.C.; Riley, L.E.; McNally, V.V. COVID-19 Vaccine Safety Technical (VaST) Work Group: Enhancing vaccine safety monitoring during the pandemic. Vaccine 2024, 42, 125549. [Google Scholar] [CrossRef]
- Ghafari, M.; Hosseinpour, S.; Rezaee-Zavareh, M.S.; Dascalu, S.; Rostamian, S.; Aramesh, K.; Madani, K.; Kordasti, S. A quantitative evaluation of the impact of vaccine roll-out rate and coverage on reducing deaths: Insights from the first 2 years of COVID-19 epidemic in Iran. BMC Med. 2023, 21, 429–437. [Google Scholar] [CrossRef]
- Duroseau, B.; Kipshidze, N.; Limaye, R.J. The impact of delayed access to COVID-19 vaccines in low-and lower-middle-income countries. Front. Public Health 2023, 10, 1087138. [Google Scholar] [CrossRef]
- Okello, J.S.; Ginindza, T.; Nyerere, J. Protocol: Multi-Sectoral Coordination during the COVID-19 Pandemic—Practices, Challenges, and Recommendations for Future Preparedness-A Systematic Literature Review Protocol. medRxiv 2025. [Google Scholar] [CrossRef]
- Mukherjee, S.; Kalra, K.; Phelan, A.L. Expanding global vaccine manufacturing capacity: Strategic prioritization in small countries. PLoS Glob. Public Health 2023, 3, e0002098. [Google Scholar] [CrossRef]
- Maccaro, A.; Audia, C.; Stokes, K.; Masud, H.; Sekalala, S.; Pecchia, L.; Piaggio, D. Pandemic Preparedness: A Scoping Review of Best and Worst Practices from COVID-19. Healthcare 2023, 11, 2572. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SN | Parameter | Classes | Frequency |
|---|---|---|---|
| 1 | WHO region | AFR | 47 |
| AMR | 35 | ||
| EMR | 21 | ||
| EUR | 54 | ||
| SEAR | 11 | ||
| WPR | 27 | ||
| 2 | World Bank economic status | Low income | 28 |
| Lower-middle income | 53 | ||
| Upper-middle income | 55 | ||
| High income | 58 | ||
| 3 | WHO-GBT maturity level | Level 1 | 111 |
| Level 2 | 25 | ||
| Level 3 | 33 | ||
| Level 4 | 25 |
| Category | AFR | AMR | EMR | EUR | SEAR | WPR |
|---|---|---|---|---|---|---|
| Approach I: Import permits only (procurement based) | 11 | 0 | 1 | 14 | 1 | 0 |
| Approach II: Approved based on reliance on expedited regulatory pathways | 11 | 30 | 11 | 0 | 7 | 12 |
| Approach II: Not yet approved but relies on at least one expedited regulatory pathway | 12 | 0 | 3 | 1 | 1 | 4 |
| Approach III: Approved based on self or collective regional evaluation | 0 | 0 | 0 | 34 | 0 | 0 |
| Regulatory Function | Employed Flexibility Practices | Key Outcomes |
|---|---|---|
| Registration and marketing authorization (MA) | Submission:
|
|
Evaluation:
|
| |
Authorization:
|
| |
| Market surveillance and control (MC) |
|
|
| Licensing of establishments (LE) |
|
|
| Regulatory inspection (RI) |
|
|
| Clinical trials |
|
|
| Lot release (LR) |
|
|
| Independent Variables | Dependent Variable | Spearman’s Rank Correlation Coefficient |
|---|---|---|
| World Bank status ranks | Time of approval ranks | ρ = 0.36 (two tailed p value = 0.00) |
|
| |
| WHO maturity level ranks | ρ = 0.51 (two tailed p value = 0.00) | |
|
| Best Practices | Involved Activities (What to Do?) |
|---|---|
| Having an emergency preparedness plan |
|
| Practicing regulatory reliance on reference authorities and institutions |
|
| Responding with flexibility |
|
| Optimal coordination of key stakeholders |
|
| Sustaining regulatory efficiency post-pandemic |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostad Ali Dehaghi, R.; Khadem Broojerdi, A.; Magdy, A.; Valentin, M.; Dahlan, J.; Malik, O.; Siggers, R.H.; Nkansah, E.; Sillo, H.B. Strengthening Vaccine Regulation: Insights from COVID-19 Vaccines, Best Practices, and Lessons for Future Public Health Emergencies. Vaccines 2025, 13, 638. https://doi.org/10.3390/vaccines13060638
Ostad Ali Dehaghi R, Khadem Broojerdi A, Magdy A, Valentin M, Dahlan J, Malik O, Siggers RH, Nkansah E, Sillo HB. Strengthening Vaccine Regulation: Insights from COVID-19 Vaccines, Best Practices, and Lessons for Future Public Health Emergencies. Vaccines. 2025; 13(6):638. https://doi.org/10.3390/vaccines13060638
Chicago/Turabian StyleOstad Ali Dehaghi, Razieh, Alireza Khadem Broojerdi, Alaa Magdy, Marie Valentin, Juliati Dahlan, Obaidullah Malik, Richard H. Siggers, Edwin Nkansah, and Hiiti B. Sillo. 2025. "Strengthening Vaccine Regulation: Insights from COVID-19 Vaccines, Best Practices, and Lessons for Future Public Health Emergencies" Vaccines 13, no. 6: 638. https://doi.org/10.3390/vaccines13060638
APA StyleOstad Ali Dehaghi, R., Khadem Broojerdi, A., Magdy, A., Valentin, M., Dahlan, J., Malik, O., Siggers, R. H., Nkansah, E., & Sillo, H. B. (2025). Strengthening Vaccine Regulation: Insights from COVID-19 Vaccines, Best Practices, and Lessons for Future Public Health Emergencies. Vaccines, 13(6), 638. https://doi.org/10.3390/vaccines13060638