
Longitudinal Surveillance of COVID-19 Antibodies in Pediatric Healthcare Workers

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
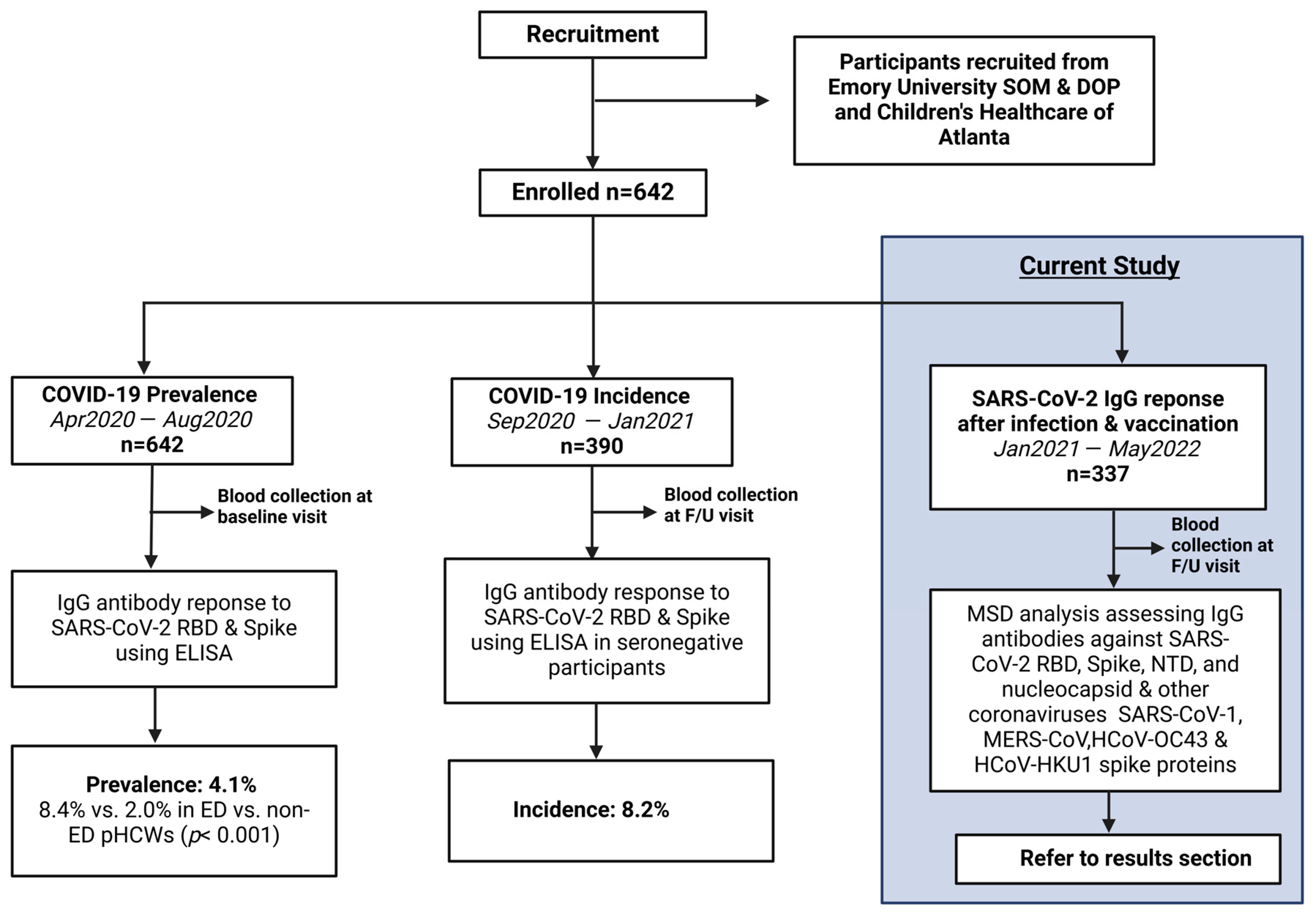
2.1. Study Design
2.2. Participants
2.3. Procedures
2.4. Laboratory Methods
2.5. Criteria for Defining Infection
2.6. Quantification and Statistical Analysis
3. Results
3.1. Demographics and Patient Characteristics
3.2. Infection and Vaccination Rates
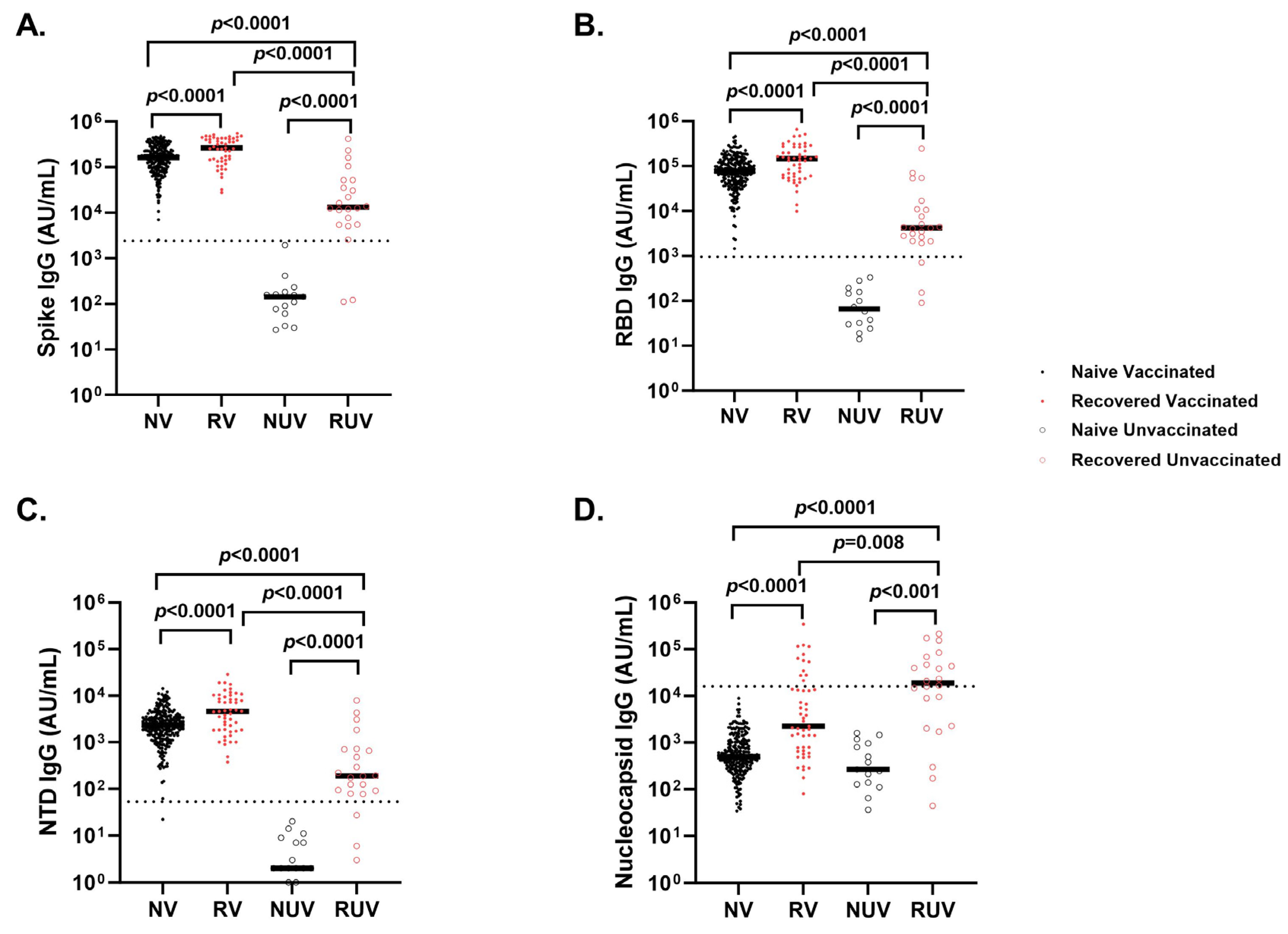
3.3. Analyses of SARS-CoV-2 IgG Antibody Response After Primary COVID-19 Vaccination
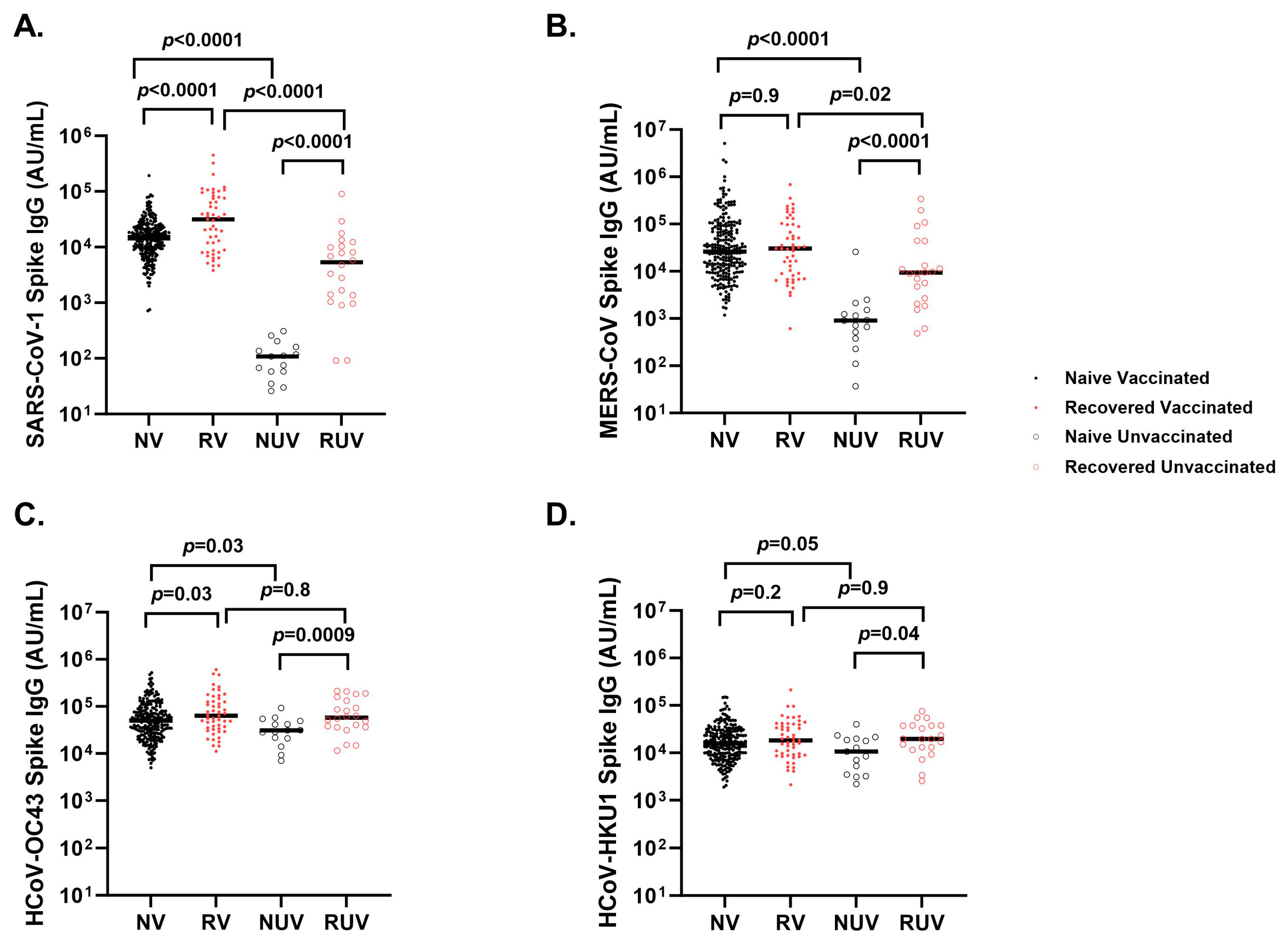
3.4. Cross-Reactivity of Seasonal and Other Coronaviruses After COVID-19 Vaccination and Infection
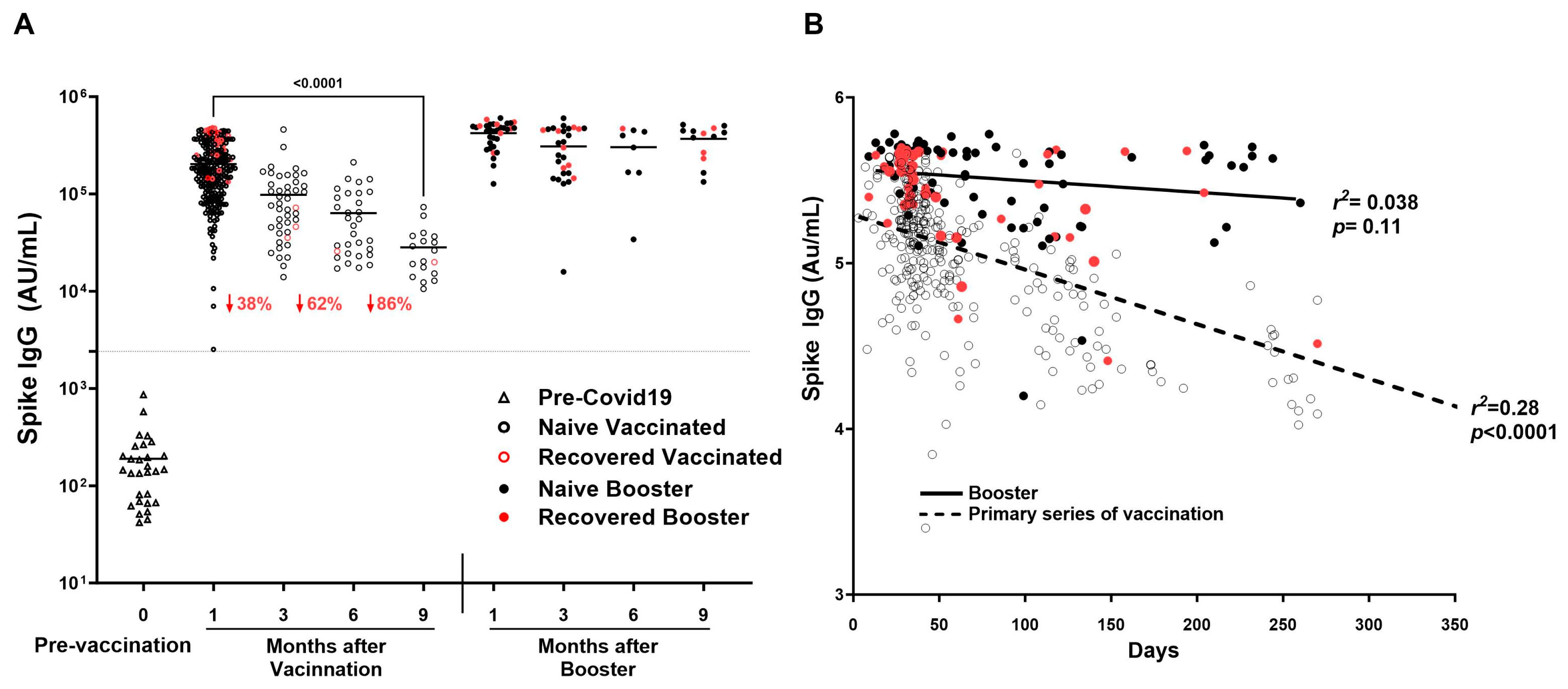
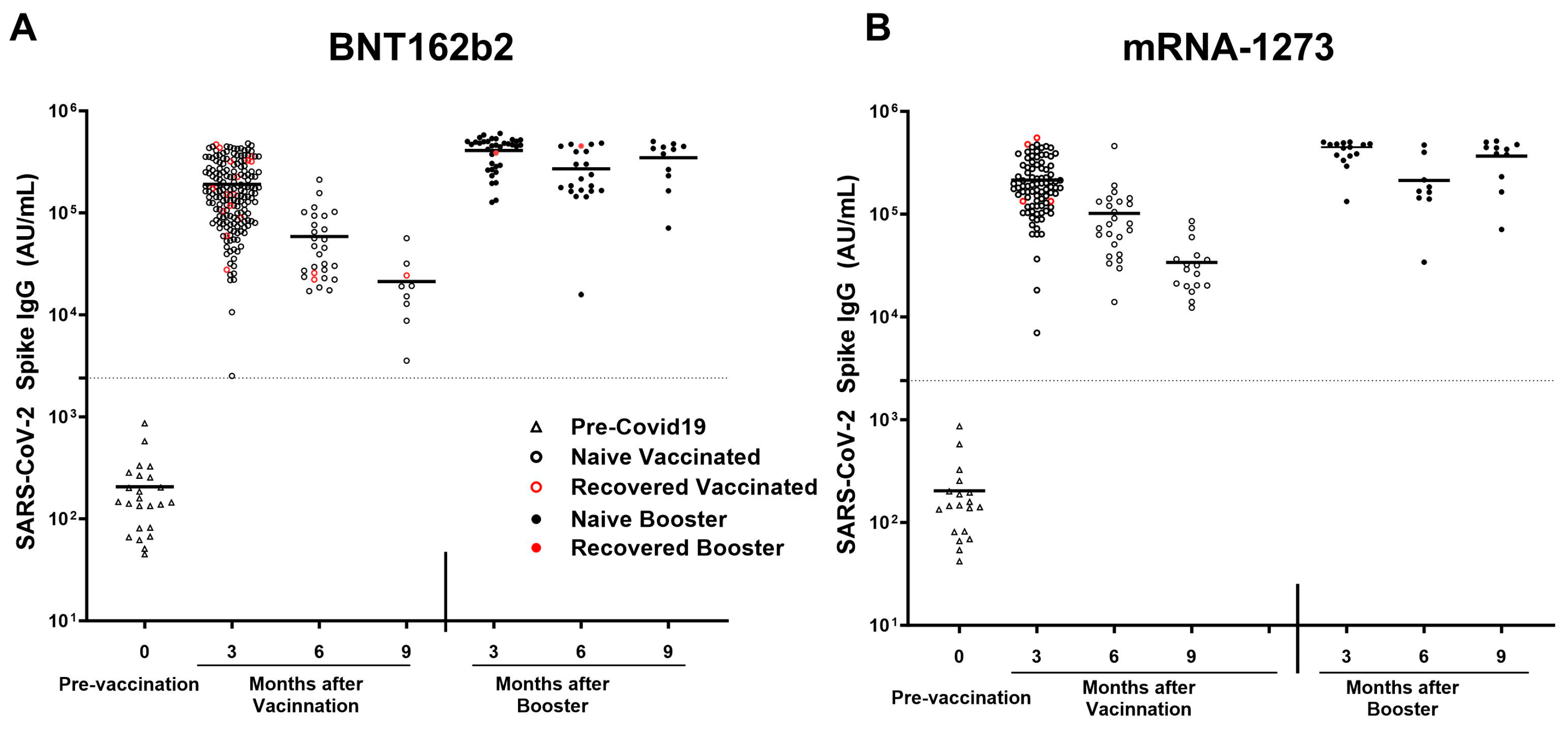
3.5. Durability of SARS-CoV-2 Anti-Spike IgG Antibodies over Time After COVID-19 Primary Vaccination and Booster
3.6. Analyses of SARS-CoV-2 Spike IgG Antibody Response to mRNA-1273 vs. BNT162b2 Vaccines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| HCWs | Healthcare workers |
| pHCWs | Pediatric healthcare workers |
| PPE | Personal Protective Equipment |
| IgG | Immunoglobulin G |
| RBD | Receptor Binding Domain |
| NTD | N-terminal domain |
| MERS-CoV | Middle East Respiratory Syndrome Coronavirus |
| SARS-CoV-1 | Severe Acute Respiratory Syndrome Coronavirus 1 |
| HCoV-HKU1 | Human coronavirus HKU1 |
| HCoV-OC43 | Human coronavirus OC43 |
References
- World Health Organization. Number of COVID-19 Deaths Reported to WHO (Cumulative Total). Available online: https://data.who.int/dashboards/covid19/deaths?n=o (accessed on 15 November 2024).
- US Food and Drug Adminstration. Available online: https://www.federalregister.gov/documents/2021/01/19/2021-01022/authorizations-of-emergency-use-of-two-biological-products-during-the-covid-19-pandemic-availability (accessed on 22 November 2024).
- COVID-19 Working Group. Successes and Lessons Learned in Responding to the Needs of Pediatricians, Children, and Families During the COVID-19 Pandemic. Pediatrics 2024, 153, e2024066634. [Google Scholar] [CrossRef]
- Dawood, F.S.; Porucznik, C.A.; Veguilla, V.; Stanford, J.B.; Duque, J.; Rolfes, M.A.; Dixon, A.; Thind, P.; Hacker, E.; Castro, M.J.E.; et al. Incidence Rates, Household Infection Risk, and Clinical Characteristics of SARS-CoV-2 Infection Among Children and Adults in Utah and New York City, New York. JAMA Pediatr. 2022, 176, 59–67. [Google Scholar] [CrossRef]
- Laws, R.L.; Chancey, R.J.; Rabold, E.M.; Chu, V.T.; Lewis, N.M.; Fajans, M.; Reses, H.E.; Duca, L.M.; Dawson, P.; Conners, E.E.; et al. Symptoms and Transmission of SARS-CoV-2 Among Children—Utah and Wisconsin, March-May 2020. Pediatrics 2021, 147, e2020027268. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, R.E.; Deng, Y.; Deng, X.; Lee, A.; Meyer, W.A., 3rd; Letovsky, S.; Charles, M.D.; Gundlapalli, A.V.; MacNeil, A.; Hall, A.J.; et al. Estimated SARS-CoV-2 antibody seroprevalence trends and relationship to reported case prevalence from a repeated, cross-sectional study in the 50 states and the District of Columbia, United States-October 25, 2020-February 26, 2022. Lancet Reg. Health Am. 2023, 18, 100403. [Google Scholar] [CrossRef] [PubMed]
- Shrwani, K.; Sharma, R.; Krishnan, M.; Jones, T.; Mayora-Neto, M.; Cantoni, D.; Temperton, N.J.; Dobson, S.L.; Subramaniam, K.; McNamara, P.S.; et al. Detection of Serum Cross-Reactive Antibodies and Memory Response to SARS-CoV-2 in Prepandemic and Post-COVID-19 Convalescent Samples. J. Infect. Dis. 2021, 224, 1305–1315. [Google Scholar] [CrossRef]
- Tamminen, K.; Salminen, M.; Blazevic, V. Seroprevalence and SARS-CoV-2 cross-reactivity of endemic coronavirus OC43 and 229E antibodies in Finnish children and adults. Clin. Immunol. 2021, 229, 108782. [Google Scholar] [CrossRef]
- Dowell, A.C.; Butler, M.S.; Jinks, E.; Tut, G.; Lancaster, T.; Sylla, P.; Begum, J.; Bruton, R.; Pearce, H.; Verma, K.; et al. Children develop robust and sustained cross-reactive spike-specific immune responses to SARS-CoV-2 infection. Nat. Immunol. 2022, 23, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Woudenberg, T.; Pelleau, S.; Anna, F.; Attia, M.; Donnadieu, F.; Gravet, A.; Lohmann, C.; Seraphin, H.; Guiheneuf, R.; Delamare, C.; et al. Humoral immunity to SARS-CoV-2 and seasonal coronaviruses in children and adults in north-eastern France. EBioMedicine 2021, 70, 103495. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, H.; Tiley, K.S.; Longet, S.; Tonry, C.; Roarty, C.; Watson, C.; Amirthalingam, G.; Vichos, I.; Morey, E.; Douglas, N.L.; et al. Serum HCoV-spike specific antibodies do not protect against subsequent SARS-CoV-2 infection in children and adolescents. iScience 2023, 26, 108500. [Google Scholar] [CrossRef]
- Morris, C.; Sullivan, P.; Mantus, G.; Sanchez, T.; Zlotorzynska, M.; Hanberry, B.; Iyer, S.; Heilman, S.; Camacho-Gonzalez, A.; Figueroa, J.; et al. Prevalence of SARS-CoV-2 antibodies in pediatric healthcare workers. Int. J. Infect. Dis. 2021, 105, 474–481. [Google Scholar] [CrossRef]
- Griffiths, M.; Hatabah, D.; Sullivan, P.; Mantus, G.; Sanchez, T.; Zlotorzynska, M.; Heilman, S.; Camacho-Gonzalez, A.; Leake, D.; Korman, R.; et al. Incidence of SARS-CoV-2 seropositivity in pediatric healthcare workers prior to widespread vaccination: A 5-month longitudinal cohort study. Int. J. Infect. Dis. 2024, 144, 107064. [Google Scholar] [CrossRef]
- Cappetto, K.D.; Brown, J.C.; Englund, J.A.; Zerr, D.M.; Dickerson, J.A.; Wang, X.; Strelitz, B.; Klein, E.J. Paediatric healthcare and hospital worker SARS-CoV-2 IgG antibody: A longitudinal cohort study. Int. J. Infect. Dis. 2023, 7, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Suthar, M.S.; Zimmerman, M.G.; Kauffman, R.C.; Mantus, G.; Linderman, S.L.; Hudson, W.H.; Vanderheiden, A.; Nyhoff, L.; Davis, C.W.; Adekunle, O.; et al. Rapid Generation of Neutralizing Antibody Responses in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100040. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.N.; Martin-Blais, R.; Tobin, N.H.; Wang, Y.; Brooker, S.L.; Li, F.; Gadoth, A.; Elliott, J.; Faure-Kumar, E.; Halbrook, M.; et al. Humoral responses to SARS-CoV-2 mRNA vaccines: Role of past infection. PLoS ONE 2021, 16, e0259703. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Zirou, C.; Sklirou, A.D.; Apostolakou, F.; Gumeni, S.; Charitaki, I.; Papanagnou, E.D.; Bagratuni, T.; Liacos, C.I.; et al. Comparative kinetics of SARS-CoV-2 anti-spike protein RBD IgGs and neutralizing antibodies in convalescent and naïve recipients of the BNT162b2 mRNA vaccine versus COVID-19 patients. BMC Med. 2021, 19, 208. [Google Scholar] [CrossRef] [PubMed]
- Saadat, S.; Rikhtegaran Tehrani, Z.; Logue, J.; Newman, M.; Frieman, M.B.; Harris, A.D.; Sajadi, M.M. Binding and Neutralization Antibody Titers After a Single Vaccine Dose in Health Care Workers Previously Infected With SARS-CoV-2. JAMA 2021, 325, 1467–1469. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Rodríguez, R.; Valentín-Quiroga, J.; Avendaño-Ortiz, J.; Martín-Quirós, A.; Pascual-Iglesias, A.; Terrón-Arcos, V.; Montalbán-Hernández, K.; Casalvilla-Dueñas, J.C.; Bergón-Gutiérrez, M.; Alcamí, J.; et al. Cellular and humoral functional responses after BNT162b2 mRNA vaccination differ longitudinally between naive and subjects recovered from COVID-19. Cell Rep. 2022, 38, 110235. [Google Scholar] [CrossRef] [PubMed]
- Tokareva, Y.; Englund, J.A.; Dickerson, J.A.; Brown, J.C.; Zerr, D.M.; Walter, E.; Tsogoo, A.; Cappetto, K.; Valdez Gonzalez, J.; Strelitz, B.; et al. Prevalence of Health Care and Hospital Worker SARS-CoV-2 IgG Antibody in a Pediatric Hospital. Hosp. Pediatr. 2021, 11, e48–e53. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Korosec, C.S.; Dick, D.W.; Moyles, I.R.; Watmough, J. SARS-CoV-2 booster vaccine dose significantly extends humoral immune response half-life beyond the primary series. Sci. Rep. 2024, 14, 8426. [Google Scholar] [CrossRef]
- Moore, S.C.; Kronsteiner, B.; Longet, S.; Adele, S.; Deeks, A.S.; Liu, C.; Dejnirattisai, W.; Reyes, L.S.; Meardon, N.; Faustini, S.; et al. Evolution of long-term vaccine-induced and hybrid immunity in healthcare workers after different COVID-19 vaccine regimens. Med 2023, 4, 191–215. [Google Scholar] [CrossRef]
- Choi, M.J.; Hyun, H.; Heo, J.Y.; Seo, Y.B.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Kim, H.J.; Choi, J.-y.; Lee, Y.J.; et al. Longitudinal immune kinetics of COVID-19 booster versus primary series vaccination: Insight into the annual vaccination strategy. Heliyon 2024, 10, e27211. [Google Scholar] [CrossRef]
- Qu, P.; Faraone, J.N.; Evans, J.P.; Zheng, Y.M.; Yu, L.; Ma, Q.; Carlin, C.; Lozanski, G.; Saif, L.J.; Oltz, E.M.; et al. Durability of Booster mRNA Vaccine against SARS-CoV-2 BA.2.12.1, BA.4, and BA.5 Subvariants. N. Engl. J. Med. 2022, 387, 1329–1331. [Google Scholar] [CrossRef] [PubMed]
- Gilboa, M.; Regev-Yochay, G.; Mandelboim, M.; Indenbaum, V.; Asraf, K.; Fluss, R.; Amit, S.; Mendelson, E.; Doolman, R.; Afek, A.; et al. Durability of Immune Response After COVID-19 Booster Vaccination and Association With COVID-19 Omicron Infection. JAMA Netw. Open 2022, 5, e2231778. [Google Scholar] [CrossRef] [PubMed]
- Veli, N.; Martin, C.A.; Woolf, K.; Nazareth, J.; Pan, D.; Al-Oraibi, A.; Baggaley, R.F.; Bryant, L.; Nellums, L.B.; Gray, L.J.; et al. Hesitancy for receiving regular SARS-CoV-2 vaccination in UK healthcare workers: A cross-sectional analysis from the UK-REACH study. BMC Med. 2022, 20, 386. [Google Scholar] [CrossRef]
- Zhang, L.; Wu, Y.; Jing, S.; Liu, X.; Ren, T.; Liu, X.; Dai, Z.; Fu, J.; Chen, X.; Xiao, W.; et al. The second dose of COVID-19 vaccine booster hesitancy among health care workers in China: A multicenter cross-sectional study. Am. J. Infect. Control 2024, 52, 525–532. [Google Scholar] [CrossRef]
- Vellappally, S.; Naik, S.; Alsadon, O.; Al-Kheraif, A.A.; Alayadi, H.; Alsiwat, A.J.; Kumar, A.; Hashem, M.; Varghese, N.; Thomas, N.G.; et al. Perception of COVID-19 Booster Dose Vaccine among Healthcare Workers in India and Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 8942. [Google Scholar] [CrossRef] [PubMed]
- Maraqa, B.; Nazzal, Z.; Baroud, H.; Douden, M.; El Hamshary, Y.; Jalamneh, T. Healthcare workers’ attitudes toward and factors influencing their acceptance of an annual COVID-19 booster vaccine: A cross-sectional study in Palestine. BMC Health Serv. Res. 2024, 24, 624. [Google Scholar] [CrossRef]
- Kainth, M.K.; Sembajwe, G.N.; Ahn, H.; Qian, M.; Carrington, M.; Armellino, D.; Jan, S. Despite mandated primary series, health care personnel still hesitant about COVID-19 vaccine and immunizing children. Vaccine 2024, 42, 3122–3133. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Peiris, J.S.; Guan, Y.; Yuen, K.Y. Severe acute respiratory syndrome. Nat. Med. 2004, 10, S88–S97. [Google Scholar] [CrossRef] [PubMed]
- Zaki, A.M.; van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef]
- Zhou, W.; Wang, W.; Wang, H.; Lu, R.; Tan, W. First infection by all four non-severe acute respiratory syndrome human coronaviruses takes place during childhood. BMC Infect. Dis. 2013, 13, 433. [Google Scholar] [CrossRef] [PubMed]
- Zar, H.J.; Nicol, M.P.; MacGinty, R.; Workman, L.; Petersen, W.; Johnson, M.; Goldblatt, D. Antibodies to Seasonal Coronaviruses Rarely Cross-React With SARS-CoV-2: Findings From an African Birth Cohort. Pediatr. Infect. Dis. J. 2021, 40, e516–e519. [Google Scholar] [CrossRef] [PubMed]
- Sayama, Y.; Okamoto, M.; Saito, M.; Saito-Obata, M.; Tamaki, R.; Joboco, C.D.; Lupisan, S.; Oshitani, H. Seroprevalence of four endemic human coronaviruses and, reactivity and neutralization capability against SARS-CoV-2 among children in the Philippines. Sci. Rep. 2023, 13, 2310. [Google Scholar] [CrossRef]
- Gholami, M.; Fawad, I.; Shadan, S.; Rowaiee, R.; Ghanem, H.; Hassan Khamis, A.; Ho, S.B. COVID-19 and healthcare workers: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 104, 335–346. [Google Scholar] [CrossRef]
- Chutiyami, M.; Bello, U.M.; Salihu, D.; Ndwiga, D.; Kolo, M.A.; Maharaj, R.; Naidoo, K.; Devar, L.; Pratitha, P.; Kannan, P. COVID-19 pandemic-related mortality, infection, symptoms, complications, comorbidities, and other aspects of physical health among healthcare workers globally: An umbrella review. Int. J. Nurs. Stud. 2022, 129, 104211. [Google Scholar] [CrossRef]
- Schwartz, K.L.; Achonu, C.; Buchan, S.A.; Brown, K.A.; Lee, B.; Whelan, M.; Wu, J.H.; Garber, G. Epidemiology, clinical characteristics, household transmission, and lethality of severe acute respiratory syndrome coronavirus-2 infection among healthcare workers in Ontario, Canada. PLoS ONE 2020, 15, e0244477. [Google Scholar] [CrossRef]
- Gouma, S.; Weirick, M.E.; Bolton, M.J.; Arevalo, C.P.; Goodwin, E.C.; Anderson, E.M.; McAllister, C.M.; Christensen, S.R.; Dunbar, D.; Fiore, D.; et al. Health care worker seromonitoring reveals complex relationships between common coronavirus antibodies and COVID-19 symptom duration. JCI Insight 2021, 6, e150449. [Google Scholar] [CrossRef]
- Asamoah-Boaheng, M.; Grunau, B.; Karim, M.E.; Jassem, A.N.; Bolster, J.; Marquez, A.C.; Scheuermeyer, F.X.; Goldfarb, D.M. Are higher antibody levels against seasonal human coronaviruses associated with a more robust humoral immune response after SARS-CoV-2 vaccination? Front. Immunol. 2022, 13, 954093. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Wang, L.; Davis, P.B.; Kaelber, D.C.; Volkow, N.D.; Xu, R. Comparison of mRNA-1273 and BNT162b2 Vaccines on Breakthrough SARS-CoV-2 Infections, Hospitalizations, and Death During the Delta-Predominant Period. JAMA 2022, 327, 678–680. [Google Scholar] [CrossRef]
- Montoya, J.G.; Adams, A.E.; Bonetti, V.; Deng, S.; Link, N.A.; Pertsch, S.; Olson, K.; Li, M.; Dillon, E.C.; Frosch, D.L. Differences in IgG Antibody Responses following BNT162b2 and mRNA-1273 SARS-CoV-2 Vaccines. Microbiol. Spectr. 2021, 9, e0116221. [Google Scholar] [CrossRef] [PubMed]
- Kelliher, M.T.; Levy, J.J.; Nerenz, R.D.; Poore, B.; Johnston, A.A.; Rogers, A.R.; Stella, M.E.O.; Snow, S.E.; Cervinski, M.A.; Hubbard, J.A. Comparison of Symptoms and Antibody Response Following Administration of Moderna or Pfizer SARS-CoV-2 Vaccines. Arch. Pathol. Lab. Med. 2022, 146, 677–685. [Google Scholar] [CrossRef]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 337) |
|---|---|
| Median Age Range (years) | 31–40 |
| Gender-Female n (%) | 286 (84%) |
| Vaccinated n (% of ALL) | 301 (89%) |
| BNT162b2 n (% of vaccinated) | 203 (67%) |
| mRNA-1273 n (% of vaccinated) | 97 (32%) |
| Ad26.COV2.S n (% of vaccinated) | 1 (1%) |
| Booster a-Yes n (%) | 59 (18%) |
| Infected b-Yes n (%) | 76 (23%) |
| Comorbidities c-Yes n (%) | 85 (25%) |
| Emergency Department Visit-Yes n (%) | 0 (0%) |
| Hospitalization-Yes n (%) | 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatabah, D.; Gupta, S.L.; Mantus, G.; Sullivan, P.; Heilman, S.; Camacho-Gonzalez, A.; Leake, D.; Le, M.; Griffiths, M.; Norwood, C.; et al. Longitudinal Surveillance of COVID-19 Antibodies in Pediatric Healthcare Workers. Vaccines 2025, 13, 163. https://doi.org/10.3390/vaccines13020163
Hatabah D, Gupta SL, Mantus G, Sullivan P, Heilman S, Camacho-Gonzalez A, Leake D, Le M, Griffiths M, Norwood C, et al. Longitudinal Surveillance of COVID-19 Antibodies in Pediatric Healthcare Workers. Vaccines. 2025; 13(2):163. https://doi.org/10.3390/vaccines13020163
Chicago/Turabian StyleHatabah, Dunia, Sneh Lata Gupta, Grace Mantus, Patrick Sullivan, Stacy Heilman, Andres Camacho-Gonzalez, Deborah Leake, Mimi Le, Mark Griffiths, Carson Norwood, and et al. 2025. "Longitudinal Surveillance of COVID-19 Antibodies in Pediatric Healthcare Workers" Vaccines 13, no. 2: 163. https://doi.org/10.3390/vaccines13020163
APA StyleHatabah, D., Gupta, S. L., Mantus, G., Sullivan, P., Heilman, S., Camacho-Gonzalez, A., Leake, D., Le, M., Griffiths, M., Norwood, C., Shih, S., Korman, R., Maziashvili, G., Rees, C. A., Benedit, L., Wynn, B. A., Suthar, M., Vos, M. B., Wrammert, J., & Morris, C. R. (2025). Longitudinal Surveillance of COVID-19 Antibodies in Pediatric Healthcare Workers. Vaccines, 13(2), 163. https://doi.org/10.3390/vaccines13020163