
Short-Term Active Safety Surveillance of the Spikevax and Nuvaxovid Priming Doses in Australia

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Sample Characteristics
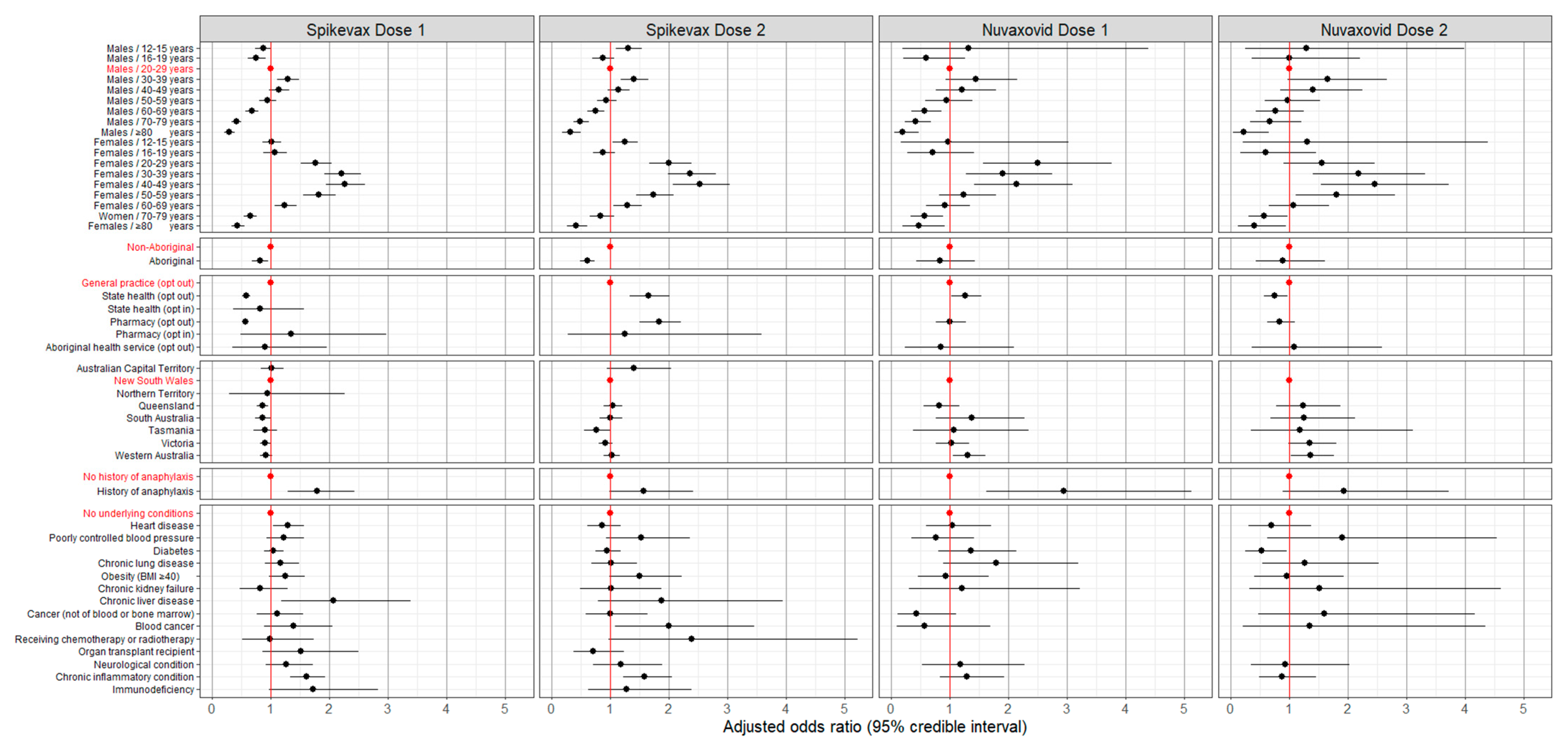
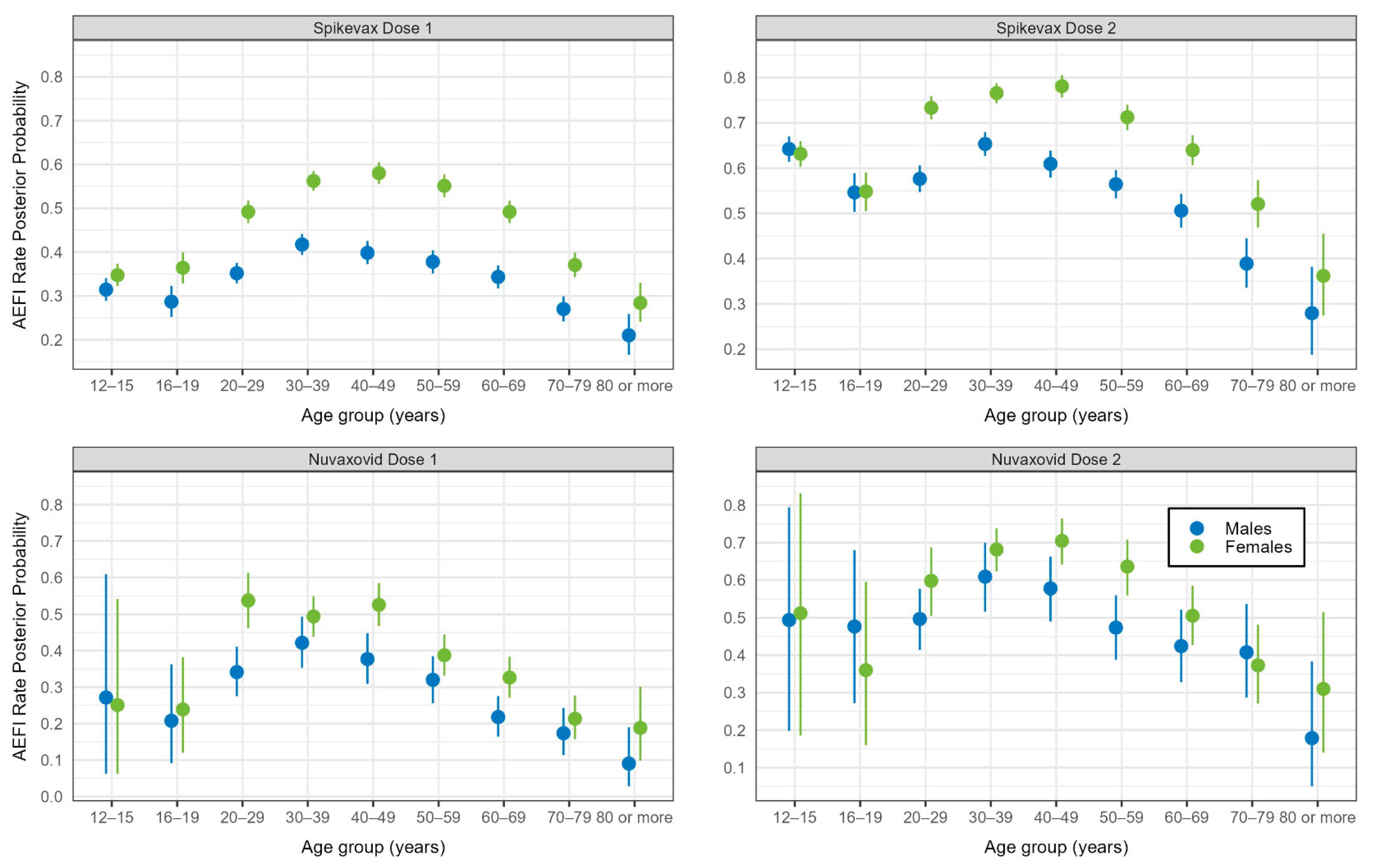
3.2. Adverse Events 0–3 and 4–7 Days after Vaccination
3.3. Impact on Routine Activities and Medical Review
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deng, L.; Glover, C.; Dymock, M.; Pillsbury, A.; Marsh, J.A.; Quinn, H.E.; Leeb, A.; Cashman, P.; Snelling, T.L.; Wood, N. The short term safety of COVID-19 vaccines in Australia: AusVaxSafety active surveillance, February–August 2021. Med. J. Aust. 2022, 217, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Australian Department of Health and Aged Care. COVID-19 Vaccines Regulatory Status. Available online: https://www.tga.gov.au/products/covid-19/covid-19-vaccines/covid-19-vaccines-regulatory-status (accessed on 20 October 2023).
- Australian Department of Health and Aged Care. Vaxzevria (AstraZeneca) Vaccine and Thrombosis with Thrombocytopenia (TTS). Available online: https://www.health.gov.au/our-work/covid-19-vaccines/advice-for-providers/clinical-guidance/tts (accessed on 9 February 2024).
- Australian Department of Health and Aged Care. Guidance on Myocarditis and Pericarditis after COVID-19 Vaccines. Available online: https://www.health.gov.au/sites/default/files/2024-01/covid-19-vaccination-guidance-on-myocarditis-and-pericarditis-after-covid-19-vaccines.pdf (accessed on 20 June 2024).
- Rittle, C.; Walter, L. COVID-19 Vaccines and mRNA Technology: Not as New as Many Believe. Online J. Issues Nurs. 2022, 27, 1–11. [Google Scholar] [CrossRef]
- Carter, N.; King, C.; Deng, L.; Wood, N.; Quinn, H. Australian health-care providers awareness of and practices related to vaccine safety surveillance. Public Health Res. Pract. 2024; submitted for publication. [Google Scholar]
- Pillsbury, A.; Cashman, P.; Leeb, A.; Regan, A.; Westphal, D.; Snelling, T.; Blyth, C.; Crawford, N.; Wood, N.; Macartney, K. Real-time safety surveillance of seasonal influenza vaccines in children, Australia, 2015. Eurosurveillance 2015, 20, 30050. [Google Scholar] [CrossRef] [PubMed]
- Jacoby, P.; Glover, C.; Damon, C.; Fathima, P.; Pillsbury, A.; Durrheim, D.; Gold, M.S.; Leeb, A.; Snelling, T. Timeliness of signal detection for adverse events following influenza vaccination in young children: A simulation case study. BMJ Open 2020, 10, e031851. [Google Scholar] [CrossRef]
- Australian Department of Health and Aged Care. COVID-19 Vaccine Safety Monitoring and Reporting. Information on How the TGA Monitors COVID-19 Vaccine Safety, Reporting Suspected Side Effects and COVID-19 Safety Updates. Available online: https://www.tga.gov.au/products/covid-19/covid-19-vaccines/covid-19-vaccine-safety-monitoring-and-reporting (accessed on 9 February 2024).
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity following receipt of mRNA-based COVID-19 vaccines. JAMA 2021, 325, 2201–2202. [Google Scholar] [CrossRef]
- Kant, A.; Jansen, J.; van Balveren, L.; van Hunsel, F. Description of frequencies of reported adverse events following immunization among four different COVID-19 vaccine brands. Drug Saf. 2022, 45, 319–331. [Google Scholar] [CrossRef]
- Guerra-Estévez, D.; Palomo-Palomo, C.; Parrado-González, A.; Estaire-Gutiérrez, J.; Reyes-Malia, M.; Romero-Alonso, M.M. Self-reported adverse events within the seven days following the Spikevax®(Moderna) vaccination. Farm. Hosp. 2022, 46, 301–307. [Google Scholar]
- Kim, S.; Ko, M.; Heo, Y.; Lee, Y.-K.; Kwon, Y.; Choi, S.-K.; Bahng, E. Safety surveillance of the NVX-CoV2373 COVID-19 vaccine among Koreans aged 18 years and over. Vaccine 2023, 41, 5066–5071. [Google Scholar] [CrossRef]
- Salter, S.M.; Li, D.; Trentino, K.; Nissen, L.; Lee, K.; Orlemann, K.; Peters, I.; Murray, K.; Leeb, A.; Deng, L. Safety of Four COVID-19 Vaccines across Primary Doses 1, 2, 3 and Booster: A Prospective Cohort Study of Australian Community Pharmacy Vaccinations. Vaccines 2022, 10, 2017. [Google Scholar] [CrossRef]
- Vaxtracker. About Vaxtracker. Available online: https://www.vaxtracker.net/About/Index (accessed on 2 July 2023).
- SmartVax. About SmartVax. Available online: https://www.smartvax.com.au/about-smartvax-vaccine-surveillance-system/ (accessed on 2 July 2023).
- Department of Health (Victoria). Victorian COVID-19 Vaccination Program. COVID-19 Vaccination Management System Operating Model and Process Considerations for Health Services. 19 February 2021. Available online: https://coronavirus.wh.org.au/wp-content/uploads/2021/03/C-CVMS-operating-model-and-process-considerations-for-health-services-19.02.2021.pdf (accessed on 5 July 2023).
- Queensland Health. Vaccination Readiness Assurance Plan 3.0. Available online: https://www.health.qld.gov.au/__data/assets/pdf_file/0022/1130278/covid-19-vaccination-readiness-plan-vrap.pdf (accessed on 5 July 2023).
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 30 July 2023).
- MedDRA MSSO. Introductory Guide to MedDRA Version 26.0.; MedDRA Maintenance and Support Services Organization: McLean, VA, USA, 2023. [Google Scholar]
- Gelman, A.; Carlin, J.B.; Stern, H.S.; Dunson, D.B.; Veharti, A.; Rubin, D.B. Baysian Data Analysis, 3rd ed.; Chapman and Hall/CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- McElreath, R. Statistical Rethinking: A Bayesian Course with Examples in R and STAN, 2nd ed.; Chapman & Hall/CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 Covid-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Estimates of Aboriginal and Torres Strait Islander Australians. Available online: https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/estimates-aboriginal-and-torres-strait-islander-australians/latest-release (accessed on 2 April 2024).
- Australian Department of Health. COVID-19 Vaccine Roll-Out. 20 January 2022. Available online: https://www.health.gov.au/sites/default/files/documents/2022/01/covid-19-vaccine-rollout-update-20-january-2022.pdf (accessed on 23 May 2023).
- Attwoll, J. How Many People Were ‘Waiting for Novavax?’. Available online: https://www1.racgp.org.au/newsgp/clinical/how-many-people-were-waiting-for-novavax (accessed on 27 May 2024).
- O’Neill, G.K.; Taylor, J.; Kok, J.; Dwyer, D.E.; Dilcher, M.; Hua, H.; Levy, A.; Smith, D.; Minney-Smith, C.A.; Wood, T. Circulation of influenza and other respiratory viruses during the COVID-19 pandemic in Australia and New Zealand, 2020–2021. West. Pac. Surveill. Response J. WPSAR 2023, 14, 1. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spikevax | Nuvaxovid | |||
|---|---|---|---|---|
| Characteristic | Dose 1 n/N (%) | Dose 2 n/N (%) | Dose 1 n/N (%) | Dose 2 n/N (%) |
| All respondents | 10,948/26,254 (41.7%) | 12,585/19,611 (64.2%) | 1088/2972 (36.6%) | 1079/1884 (57.3%) |
| Sex 1 | ||||
| Female | 5553/11,615 (47.8%) | 5394/7817 (69.0%) | 624/1518 (41.1%) | 579/946 (61.2%) |
| Male | 3732/10,557 (35.4%) | 4263/7314 (58.3%) | 335/1084 (30.9%) | 313/619 (50.6%) |
| Other | 18/30 (60.0%) | 12/15 (80.0%) | <5 (100.0%) | <5 (100.0%) |
| Missing data | 4052 | 4465 | 369 | 318 |
| Age (years) 1 | ||||
| Median (IQR) | 39 (26, 55) | 35 (21, 49) | 43 (33, 56) | 43 (34, 55) |
| Missing data | 13 | 9 | 10 | 8 |
| Indigenous status 1 | ||||
| Aboriginal | 276/733 (37.7%) | 287/529 (54.3%) | 21/61 (34.4%) | 20/41 (48.8%) |
| Non-Aboriginal | 10,405/24,907 (41.8%) | 12,028/18,652 (64.5%) | 1037/2858 (36.3%) | 1031/1804 (57.2%) |
| Missing data | 614 | 430 | 53 | 39 |
| Anaphylaxis history | ||||
| No | 10,618/25,634 (41.4%) | 12,242/19,145 (63.9%) | 1008/2833 (35.6%) | 1007/1781 (56.5%) |
| Yes | 330/620 (53.2%) | 343/466 (73.6%) | 80/139 (57.6%) | 72/103 (69.9%) |
| Underlying medical condition | ||||
| No | 9046/22,634 (40.0%) | 11,129/17,510 (63.6%) | 834/2374 (35.1%) | 896/1566 (57.2%) |
| Yes | 1902/3620 (52.5%) | 1456/2101 (69.3%) | 254/598 (42.5%) | 183/318 (57.5%) |
| Spikevax | Nuvaxovid | |||
|---|---|---|---|---|
| Characteristic | Dose 1 n/N (%) | Dose 2 n/N (%) | Dose 1 n/N (%) | Dose 2 n/N (%) |
| Missed work, study, or routine activities 1 | N = 26,254 | N = 19,611 | N = 2972 | N = 1884 |
| 3493/26,220 (13.3%) | 6849/19,583 (35.0%) | 383/2971 (12.9%) | 471/1882 (25.0%) | |
| Missing | 34 | 28 | 1 | 2 |
| Number of days missed from routine activities 1 | N = 3493 | N = 6849 | N = 383 | N = 471 |
| Less than a day | 326/3484 (9.4%) | 470/6836 (6.9%) | 35/378 (9.3%) | 30/471 (6.4%) |
| One day | 1462/3484 (42.0%) | 3032/6836 (44.4%) | 126/378 (33.3%) | 187/471 (39.7%) |
| Two days | 1179/3484 (33.8%) | 2358/6836 (34.5%) | 130/378 (34.4%) | 139/471 (29.5%) |
| Three or more days | 517/3484 (14.8%) | 976/6836 (14.3%) | 87/378 (23.0%) | 115/471 (24.4%) |
| Missing data | 9 | 13 | 5 | 0 |
| Medical review sought | N = 26,254 | N = 19,611 | N = 2972 | N = 1884 |
| 493/26,254 (1.9%) | 931/19,611 (4.8%) | 81/2972 (2.7%) | 73/1884 (3.9%) | |
| Highest level medical review obtained 1 | N = 493 | N = 931 | N = 81 | N = 73 |
| ED | 113/450 (25.1%) | 182/869 (20.9%) | 20/75 (26.7%) | 11/72 (15.3%) |
| GP or Aboriginal HCW | 201/450 (44.7%) | 409/869 (47.1%) | 39/75 (52.0%) | 40/72 (55.6%) |
| Phone | 136/450 (30.2%) | 278/869 (32.0%) | 16/75 (21.3%) | 21/72 (29.2%) |
| Missing data | 43 | 62 | 6 | 1 |
| Symptom resolution by day 3 1,2 | N = 6585 | N = 7362 | N = 655 | N = 683 |
| 4443/6559 (67.7%) | 4479/7334 (61.1%) | 311/653 (47.6%) | 306/680 (45.0%) | |
| Missing data | 26 | 28 | 2 | 3 |
| Symptom resolution by day 8 1,2 | N = 6585 | N = 7362 | N = 655 | N = 683 |
| 4800/6499 (73.9%) | 5385/6708 (80.3%) | 357/629 (56.8%) | 422/633 (66.7%) | |
| Missing data | 86 | 654 | 26 | 50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reynolds, R.; Tay, E.; Dymock, M.; Deng, L.; Glover, C.; Lopez, L.K.; Huang, Y.A.; Cashman, P.; Leeb, A.; Marsh, J.A.; et al. Short-Term Active Safety Surveillance of the Spikevax and Nuvaxovid Priming Doses in Australia. Vaccines 2024, 12, 971. https://doi.org/10.3390/vaccines12090971
Reynolds R, Tay E, Dymock M, Deng L, Glover C, Lopez LK, Huang YA, Cashman P, Leeb A, Marsh JA, et al. Short-Term Active Safety Surveillance of the Spikevax and Nuvaxovid Priming Doses in Australia. Vaccines. 2024; 12(9):971. https://doi.org/10.3390/vaccines12090971
Chicago/Turabian StyleReynolds, Renee, Evelyn Tay, Michael Dymock, Lucy Deng, Catherine Glover, Laura K. Lopez, Yuanfei Anny Huang, Patrick Cashman, Alan Leeb, Julie A. Marsh, and et al. 2024. "Short-Term Active Safety Surveillance of the Spikevax and Nuvaxovid Priming Doses in Australia" Vaccines 12, no. 9: 971. https://doi.org/10.3390/vaccines12090971
APA StyleReynolds, R., Tay, E., Dymock, M., Deng, L., Glover, C., Lopez, L. K., Huang, Y. A., Cashman, P., Leeb, A., Marsh, J. A., Snelling, T., Wood, N., & Macartney, K. (2024). Short-Term Active Safety Surveillance of the Spikevax and Nuvaxovid Priming Doses in Australia. Vaccines, 12(9), 971. https://doi.org/10.3390/vaccines12090971