
Determinants of Vaccine Hesitancy among African American and Black Individuals in the United States of America: A Systematic Literature Review

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
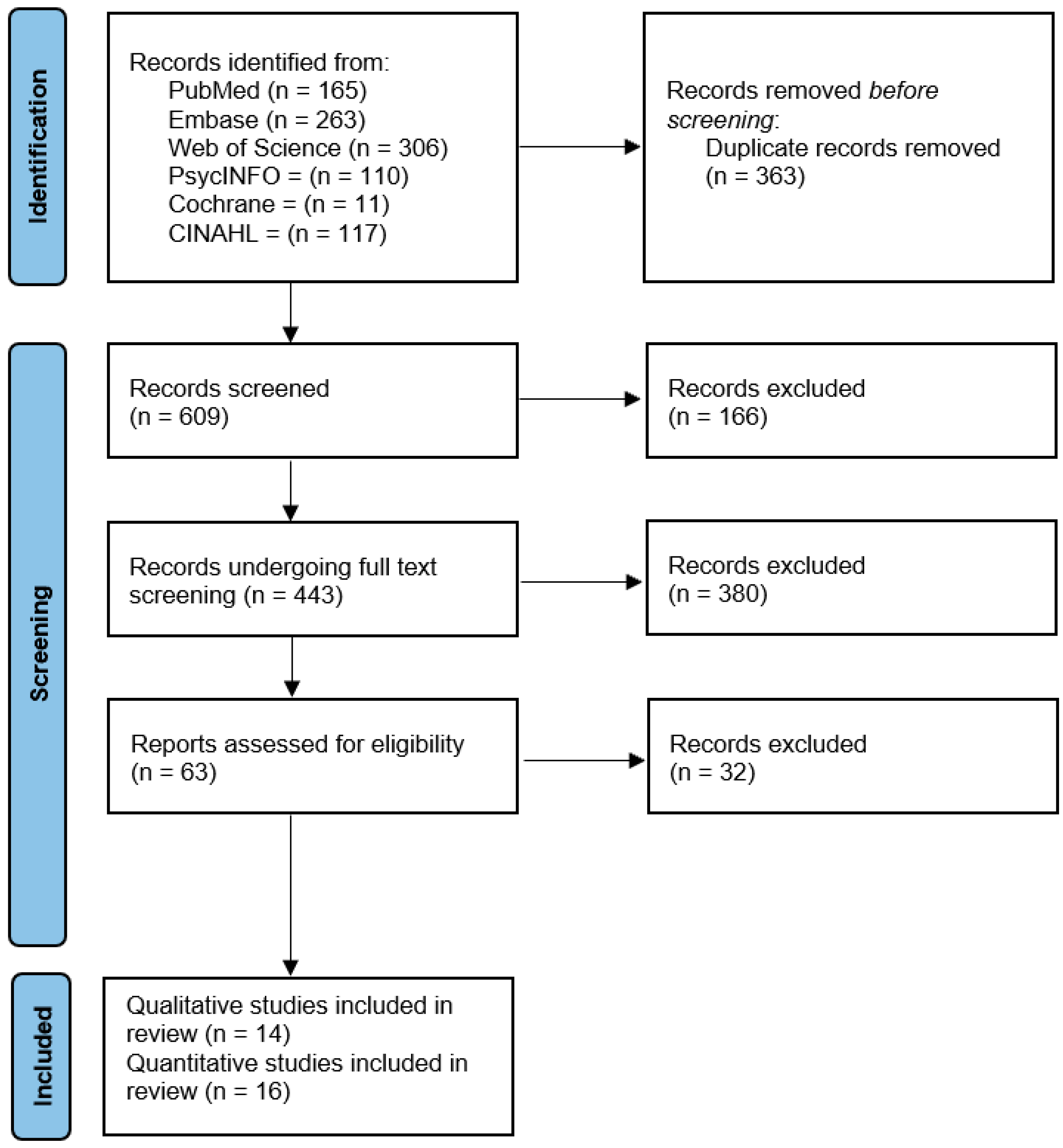
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Critical Appraisal
2.5. Synthesis Procedures
2.5.1. Analysis of the Quantitative Studies
2.5.2. Analysis of the Qualitative Studies
3. Results
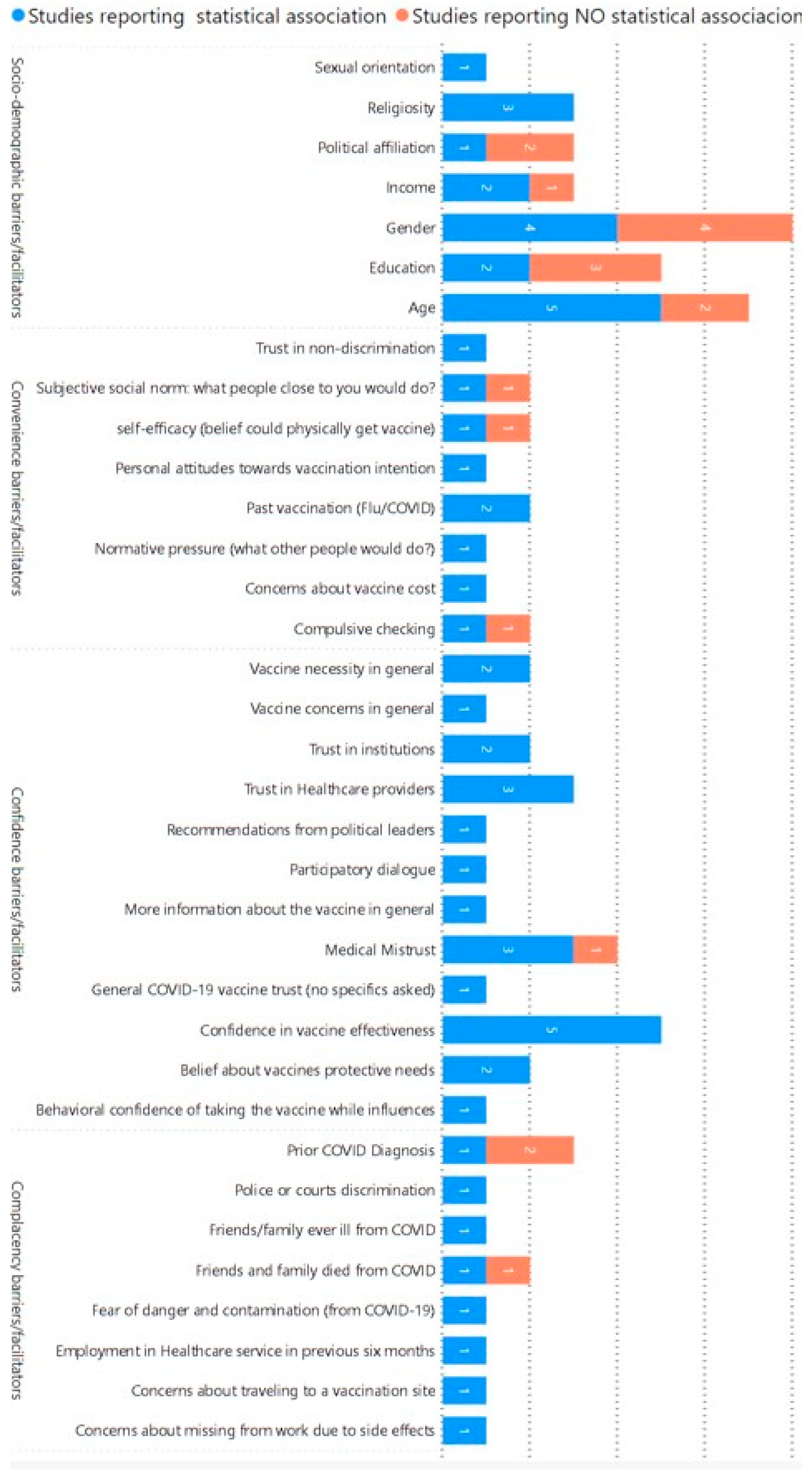
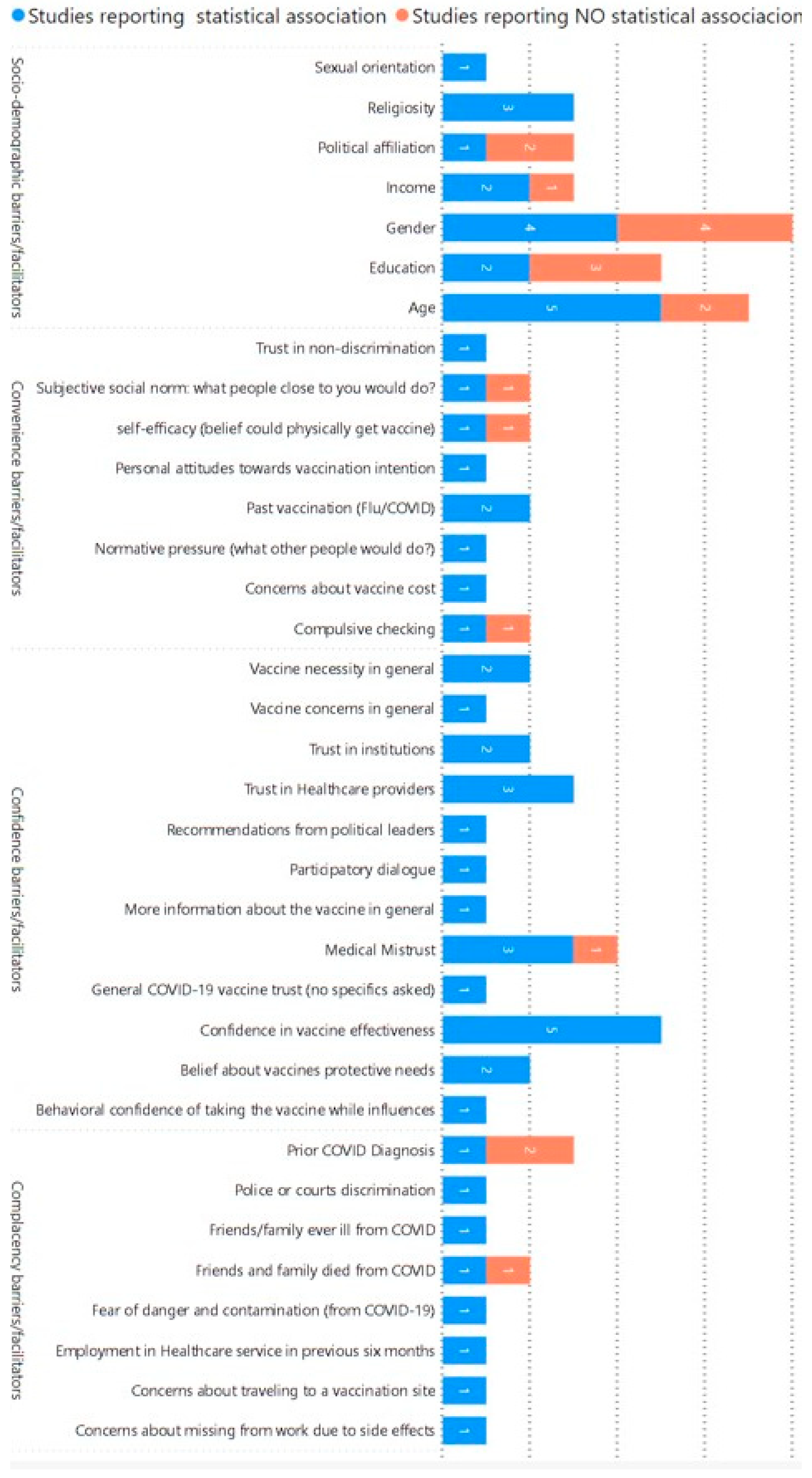
3.1. Cross-Sectional and Longitudinal Studies (n = 16)
- Characteristics of the Studies and Critical Appraisal
3.1.1. Age (n = 7)
3.1.2. Gender (n = 8)
3.1.3. Education Attainment (n = 5)
3.1.4. Income (n = 3)
3.1.5. Religiosity (n = 3)
3.1.6. Political Affiliation (n = 3)
3.1.7. Confidence/Trust in Vaccine Effectiveness/Safety (n = 5)
3.1.8. Mistrust/Trust in the Health System and Providers (n = 6)
3.1.9. Methodological Limitations
3.2. Qualitative Studies (n = 14)
- Characteristics of the Studies and Critical Appraisal
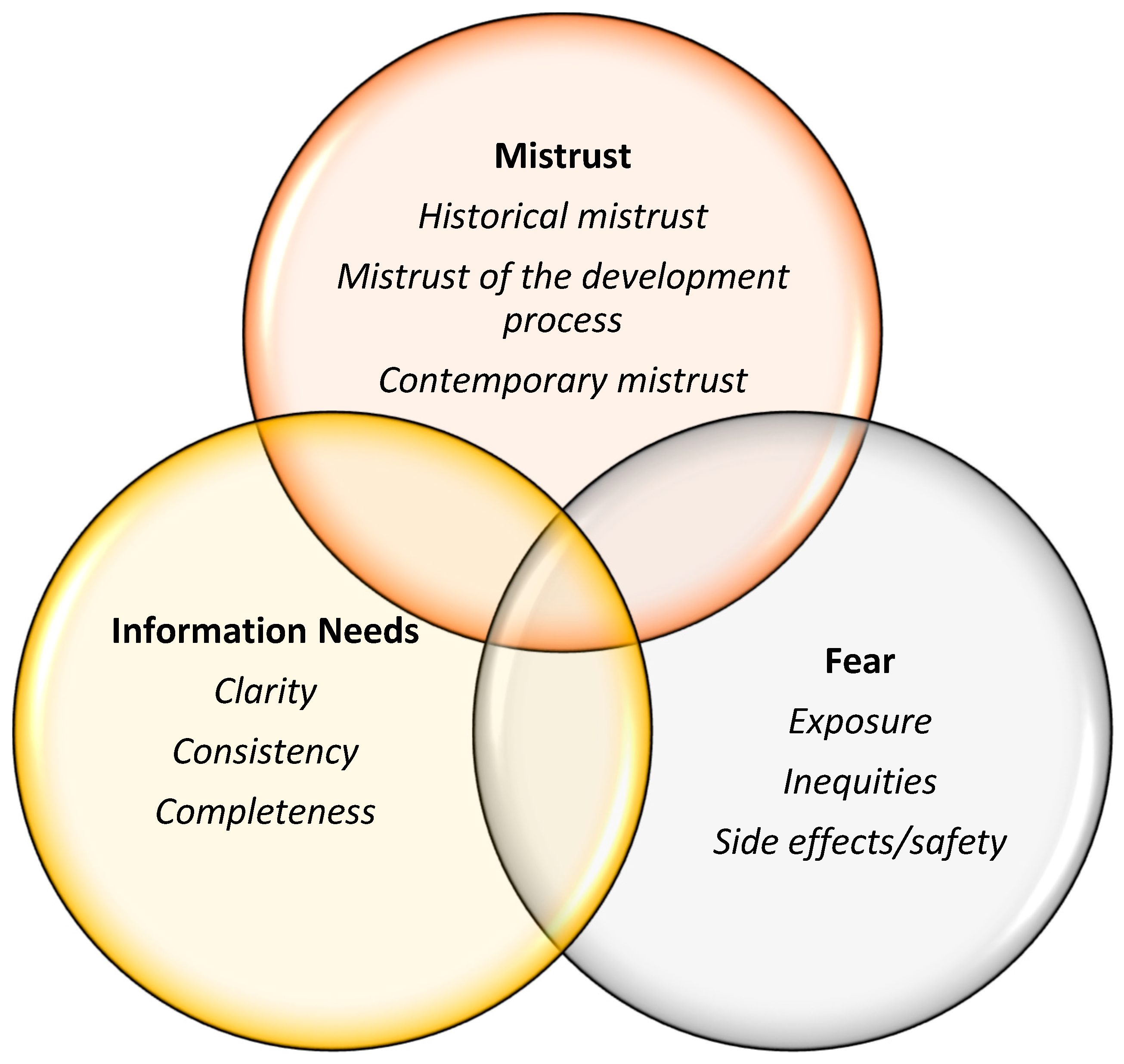
- Thematic Analysis
3.2.1. Mistrust
- Historical Mistrust
- Mistrust of the Vaccine Development Process
- Contemporary Mistrust
3.2.2. Fear of the COVID-19 Vaccine
- Fear of Unknown Side Effects and the Vaccine being Unsafe
- Fear of being Exposed to SARS-CoV-2 by the Vaccine Itself
- Fear of Inequitable Treatment or of being an Object of Experimentation
3.2.3. Information Needs
3.2.4. Recommended Interventions Based on the Qualitative Studies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms | Results | Date of Search |
|---|---|---|---|
| PubMed | (“COVID-19 Vaccines”[Mesh]) AND (“Vaccination Refusal” [Mesh] OR “Vaccin Acceptance”) AND (“Race Factors”[Mesh] OR “Racial Groups”[Mesh] OR “black”[Title/Abstract] OR “african american”[Title/Abstract] OR “african-american”[Title/Abstract] OR racia[Title/Abstract] OR race[Tiab]) | n = 165 | 16 November 2022 |
| Embase | (“sars-cov-2 vaccine”/exp OR “coronavirus disease 2019”/exp) AND “vaccine”/exp AND (“vaccine refusal”/exp OR “vaccine hesitancy”/exp OR “vaccine acceptance”/exp) AND (“black”:ti,ab OR “african american”:ti,ab OR “african-american”:ti,ab OR “racia”:ti,ab OR “race”:ti,ab) AND [embase]/lim | n = 263 | 24 November 2022 |
| Web of Science | (coronavirus OR “corona virus” OR coronavirinae OR coronaviridae OR betacoronavirus OR covid19 OR “covid 19” OR nCoV OR “CoV 2” OR CoV2 OR sarscov2 OR 2019nCoV OR “novel CoV” OR “wuhan virus”) (All Fields) and (vaccin OR immunizat OR innoculat OR booster) (All Fields) and (black OR “african-american” OR “african american”) (All Fields) and (accept OR hesitan OR refusal) (All Fields) and Review Article or Article or Early Access (Document Types) and Article or Early Access or Review Article (Document Types) and Article or Early Access or Review Article (Document Types) | n = 306 | 7 December 2022 |
| PsycINFO | Any Field: Coronavirus”vaccin hesitancy” OR Any Field: “vaccin refusal” OR Any Field: “vaccin acceptance” OR Any Field: “vaccin attitudes” AND Any Field: Black OR Any Field: race OR Any Field: “Racial and Ethnic Attitudes” AND Any Field: “Covid-19” OR Any Field: “COVID-19” | n = 110 | 20 December 2022 |
| Cochrane | “COVID-19” OR “Coronavirus” OR “Covid-19” OR “coronavirus” OR “corona virus” OR covid19 OR “covid 19” OR “2019nCoV” in All Text AND “Black” OR “african-american” OR “african american” in All Text AND “vaccin hesitancy” OR “vaccin refusal” OR “vaccin acceptance” OR “vaccin attitudes” in All Text (Word variations have been searched) | n = 11 | 23 December 2022 |
| CINAHL | (coronavirus OR “corona virus” OR covid19 OR “covid 19” OR 2019nCoV) (vaccin OR immunizat OR innoculat OR booster) (accept OR hesitan OR refusal) (black OR “african-american” OR “african american”) | n = 117 | 29 December 2022 |
| Citation | Study Period | Study Location | Study Population (AA and Black Individuals) | Study Outcome | Variables Statistically Associated with the Outcome |
|---|---|---|---|---|---|
| Cunningham Erves J. et al., 2021 [29] | October–December 2020 | Southeastern U.S. | 1715 | Vaccine willingness | Age Gender Education Religiosity Confidence in vaccine effectiveness Recommendations from political leaders Past vaccination Concerns about vaccine cost |
| Nguyen T, 2021 [38] | November 2020–March 2021 | Baltimore, Maryland | 140 | Vaccine willingness | Medical mistrust |
| Thompson HS, 2021 [37] | June–December 2020 | Michigan | 394 | Vaccine willingness | Medical mistrust |
| King WC, 2021 [13] | May 2021 | U.S. representative sample | 28,546 | Vaccine hesitancy | Age |
| McClaran N, 2022 [35] | April–September 2020 | U.S. representative sample | 121 | Vaccine willingness | Confidence in vaccine effectiveness Trust in COVID-19 vaccine |
| Bleakley A, 2021 [64] | November–December 2020 | U.S. representative sample | 1056 | Vaccine willingness | Personal attitudes toward vaccination intention Normative pressure (What would other people do?) Self-efficacy (The belief that one could physically get the vaccine) |
| Ogunbajo A, 2022 [34] | January–February 2021 | U.S. representative sample | 388 | Vaccine hesitancy | Gender Sexual orientation Prior COVID-19 diagnosis Employment in healthcare service in the previous six months |
| Bogart LM, 2021 [12] | November–December 2020 | U.S. representative sample | 207 | Vaccine willingness | Belief in vaccine necessity Confidence in vaccine effectiveness Subjective social norm (What would people close to you do?) |
| Wagner AL, 2022 [27] | June 2021 | Detroit | 714 | Vaccine hesitancy | Gender Education Income Trust in institutions Trust in healthcare providers Friends or family ever ill from COVID-19 Friends or family ever died of COVID-19 |
| Reinhart AM, 2022 [8] | July 2021 | U.S. representative sample | 1008 | Vaccine hesitancy | Age Gender Religiosity Political affiliation Trust in institutions Trust in healthcare providers Trust in non-discrimination |
| Willis DE, 2022 [30] | July–August 2021 | Arkansas | 350 | Vaccine hesitancy | Age Belief in police/court discrimination Past vaccination |
| Sharma M, 2021 [31] | July–August 2021 | U.S. representative sample | 428 | Vaccine hesitancy | Age Participatory dialog Religiosity Behavioral confidence in taking the vaccine while influenced |
| Taylor CAL, 2022 [36] | March–April 2021 | Southeast Michigan | 205 | Vaccine hesitancy | Confidence in vaccine effectiveness More information about the vaccine Concern about missing work due to side effects of the vaccine Concerns about traveling to a vaccination site |
| Minaya C, 2022 [32] | December 2020 | U.S. representative sample | 270 | Vaccine willingness | Medical mistrust Fear of danger and contamination from COVID-19 Compulsive checking |
| Williamson LD, 2022 [33] | January 2021 | U.S. representative sample | 210 | Vaccine willingness | Income Belief in vaccine necessity Concerns about COVID-19 vaccine Trust in healthcare providers |
| Padamsee TJ, 2022 [28] | December 2020–June 2021 | U.S. representative sample | 107 | Vaccine hesitancy | Confidence in vaccine effectiveness Belief in vaccine necessity |
| Citation | Data Collection Methods and Number of Participants | Racial/Ethnic Composition | Sample | Geographic Area | Themes and Sub-Themes | Results | CASP Score |
|---|---|---|---|---|---|---|---|
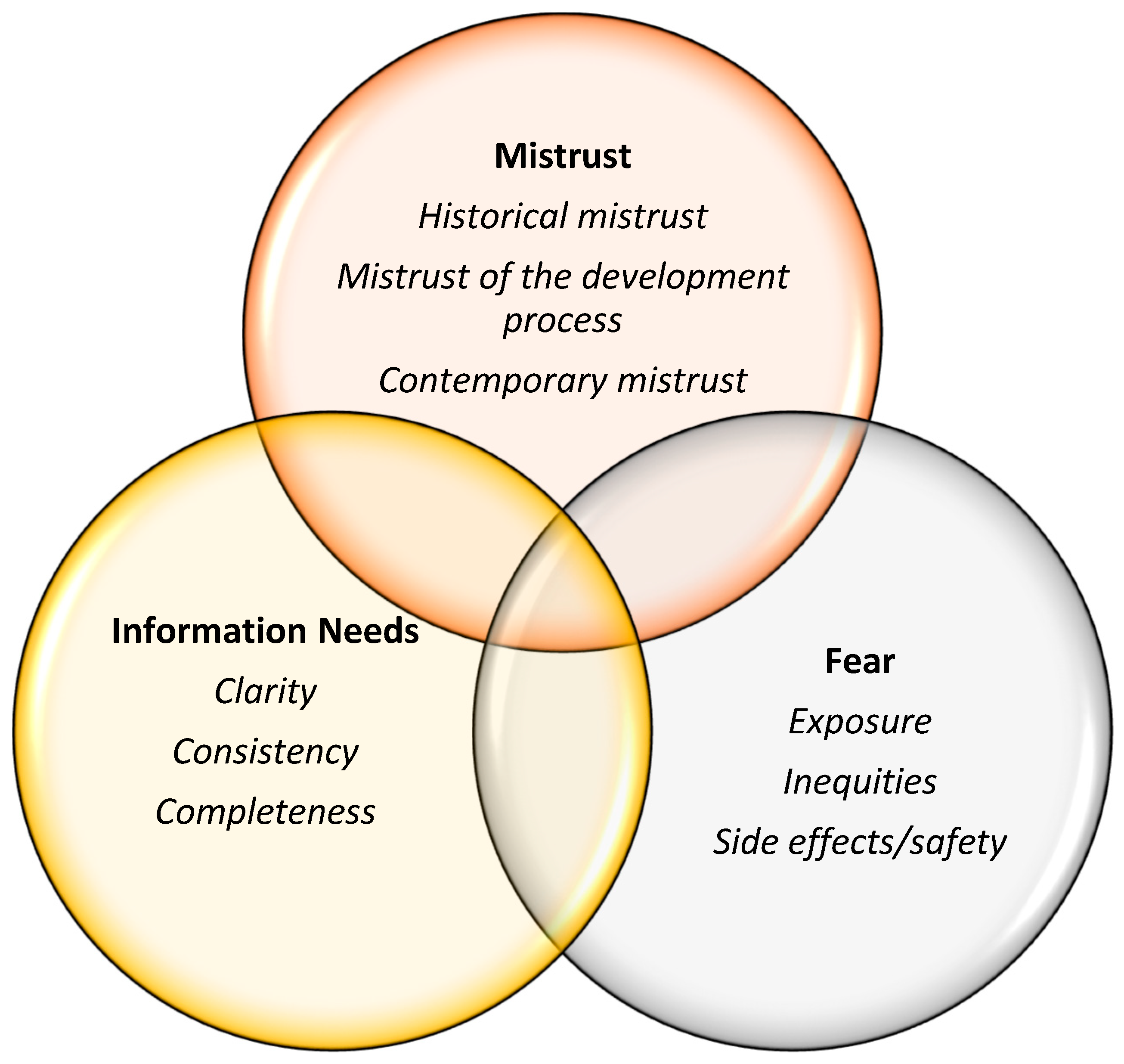
| Bateman LB, 2022 [42] | 8 focus groups; n = 67 | 6 AA focus groups + 2 Latinx | 19 years old and older | Alabama and Texas Counties: Jefferson (urban), Mobile County (urban), and Dallas (rural) | Mistrust, Fear, Information Needs | The primary themes driving COVID-19 vaccine hesitancy/acceptance—ordered from most to least discussed—included mistrust, fear, and lack of information. Additionally, they suggest that interventions to decrease vaccine hesitancy should be multi-modal and community-engaged, and they should provide consistent, comprehensive messages delivered by trusted sources. | 8 |
| Budhwani H, 2021 [46] | Interviews; n = 28 | All AA | Age 15–17 | Alabama (rural areas) | Mistrust, Fear, Misinformation, Elder Influence | The primary themes driving COVID-19 vaccine hesitancy/acceptance included the influence of community leaders and elders, fear of side effects and misinformation, and institutional mistrust. The findings suggest that the sentiments and behaviors of older family members and Church leaders may influence AAB adolescents’ vaccine acceptance, particularly in rural communities. | 7 |
| Carson S, 2021 [45] | 13 focus groups; n = 70, of whom 17 are AA | 3 Black/AA focus groups (n = 17); 3 Latino (n = 15); 3 American Indian (n = 17); 2 Filipino (n = 11); 2 Pacific Islander (n = 10) | 50 Females | California (LA County) | Mistrust, Misinformation, Concern about Accessibility of the Vaccine, Unclear Information | The primary themes driving vaccine hesitancy/acceptance included misinformation/unclear information, medical mistrust, concern about inequitable access, and accessibility barriers. | 8 |
| Ignacio M, 2023 [10] | 34 focus groups; n = 153 | 10 AA groups; 10 Native American; 14 Hispanic | >18 years of age | Arizona | Mistrust, Uncertainty due to Disinformation | The primary themes driving vaccine hesitancy/acceptance included mistrust due to historical and contemporary experiences with racism and uncertainty created by disinformation and the speed of vaccine development. The findings across all three racial/ethnic groups strongly suggest that an effective way of promoting trust in science and increasing COVID-19 vaccine confidence is through the use of community-based testimonials or narratives from local leaders, local elected officials, local elders, and other community members who have received the COVID-19 vaccine and who are able to encourage others in their community to do the same. | 9 |
| Jimenez ME, 2021 [47] | 13 focus groups; n = 111 | 4 AAB (n = 34); 3 Latinx (n = 24); 4 Mixed Groups (n = 36); 2 Healthcare Worker Groups (n = 9); Total Black Participants across Groups (n = 68) | Median age 43 years; 87 women (78.4%); Age 18–93 years | New Jersey counties | Mistrust | Mistrust among Black participants was the main reason for vaccine skepticism. | 8 |
| Kerrigan D, 2023 [39] | 5 focus groups (n = 36); 40 interview participants + crowdsourcing contest (n = 208) | 2 AA (n = 16); 2 Latinx (n = 16); 1 African Immigrant (n = 5). Interviews: AA (n = 19); Latinx (n = 13); African Immigrant (n = 7) | 19–92 years old | D.C. | Medical Mistreatment, Mistrust in Government, Information Needs | The prominent themes among AA participants included mistrust in government and the medical establishment, lack of information, and misinformation. Trusted channels were listed for grassroots’ mobilization and working with religious leaders. | 9 |
| Majee W, 2023 [43] | 21 individual interviews (16 phone, 5 in person) | 20 AAB interviewees, 1 White | 14.29% (n = 3) 30–40 years old; 85.71% (n = 18) 60+ years old. Lifestyle coaches, Church leaders, and program participants | Central Missouri | Mistrust | Most participants expressed a lack of trust in the government concerning their health and felt unsafe/lacked confidence in government. Continued acts of injustice influence AAs’ perceptions of the healthcare system. | 9 |
| Momplaisir F, 2019 [41] | 4 focus groups; n = 24 | All Black, 1 Mixed Race | 20–63 years old, avg 46 years old. 17 Non-Hispanic Black; 1 Black Hispanic; 1 Mixed Race. Black barbershop and salon owners. | West Philadelphia | Mistrust in Government, Information Needs | The primary reasons for vaccine hesitancy were mistrust in government, hesitancy based on unethical historical practices in research toward the Black community, and skepticism, which was not effectively addressed. | 9 |
| Okoro O, 2022 [15] | 8 focus groups (n = 49) + 30 interviews + surveys (n = 183, of whom 120 are AA, 40 are African, 23 are Biracial) + One-on-one interviews (n = 30) | 32 AA, 12 African/Jamaican, 4 Bi/Multi-racial in focus groups; All AAB in interviews and surveys | >18 years old, 18–81; 47% male | Minnesota and Wisconsin | Information Needs, Mistrust | The primary reasons included mistrust in government and misinformation, lack of information, and vaccine literacy. The recommendations included use of community spaces as vaccination sites, engagement of community members as outreach coordinators, and timely provision of information in multiple formats. | 9 |
| Osakwe ZT, 2022 [44] | One-on-one semi-structured interviews; n = 50 | Black individuals (n = 34); Hispanic (n = 9); Black/Hispanic (n = 3); White/Hispanic (n = 4) | 64% women, avg age 42; 44% had high-school-level education or less | New York | Information Needs | The primary reasons included the influence of social networks, lack of information and communication. This qualitative study found that among Black and Hispanic participants, the receipt of reliable vaccine-related information, social networks, seeing people like themselves receive the vaccination, and trusted doctors were the key drivers of vaccine acceptance. | 8 |
| Rios-Fetchko F, 2022 [48] | 6 focus groups (n = 45); One of the six focus groups was of mixed race. | AAB (n = 13); Latinx (n = 20); AAPI (n = 12) | 18–30 years of age | San Francisco Bay Area | Mistrust, Information Needs | The primary reasons among all three racial–ethnic groups included mistrust in medical and government institutions, strong conviction about self-agency in health decision making, and exposure to contradictory information and misinformation on social media. Social benefit and a sense of familial and societal responsibility were often mentioned as reasons to get vaccinated. | 7 |
| Sekimitsu S, 2022 [17] | Individual interviews; n = 18 | n = 18 Black individuals | 20–79 years old, Black, identified as “vaccine-hesitant” | Boston, MA | Mistrust, Fear, Information Needs | The primary reasons for vaccine hesitancy included a lack of trust in the government, healthcare, and pharmaceutical companies, concerns about the rushed development of the vaccine, fear of side effects, history of medical mistreatment, and a perception of low risk of disease. The motivators likely to increase COVID-19 vaccine uptake included more data on vaccine safety, friends and family getting vaccinated (not celebrities), and increased opportunities, which come with being vaccinated. | 9 |
| Zhang R, 2022 [18] | 2 focus groups; n = 18 | All AA | 18–30 (n = 12); 31–49 (n = 4); 50+ (n = 2) Participants primarily worked in colleges, Churches, and health agencies; 72% female | Three counties in South Carolina | Information Needs, Mistrust | The primary reasons included challenges in accessing reliable vaccine information. In AA communities, the challenges primarily included structural barriers, information barriers, and a lack of trust. Community stakeholders recommended recruiting trusted messengers, using social events to reach target populations, and conducting health communication campaigns through open dialog among stakeholders. Health communication interventions directed at COVID-19 vaccine uptake should be grounded in ongoing community engagement, trust-building activities, and transparent communication about vaccine development. | 8 |
| Zhou S, 2022 [40] | Interviews; n = 18 | 5 Latinx; 8 AAs; 5 AI/ANs | 21–54 | Denver Metropolitan Area | Fear, Information Needs, Mistrust | Negative perceptions of the COVID-19 vaccine were driven by concerns about vaccine safety due to the rapid development process and side effects. AA participants identified seeing others—especially government officials—get the vaccine first as a facilitator for accepting the vaccine, and low trust in the government and healthcare system as barriers to vaccine acceptance. To address the barriers, campaigns should increase credibility of the information and reduce inconsistencies, build trust with communities, and frame messages in a positive manner. | 9 |
References
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Allen, J.D.; Abuelezam, N.N.; Rose, R.; Fontenot, H.B. Factors associated with the intention to obtain a COVID-19 vaccine among a racially/ethnically diverse sample of women in the USA. Transl. Behav. Med. 2021, 11, 785–792. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ten Health Issues WHO Will Tackle This Year. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 15 January 2024).
- Alshurman, B.A.; Khan, A.F.; Mac, C.; Majeed, M.; Butt, Z.A. What Demographic, Social, and Contextual Factors Influence the Intention to Use COVID-19 Vaccines: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9342. [Google Scholar] [CrossRef]
- Batelaan, K. ‘It’ s not the science we distrust; it’ s the scientists’: Reframing the anti-vaccination movement within Black communities. Glob. Public Health 2022, 17, 1099–1112. [Google Scholar] [CrossRef] [PubMed]
- Hildreth, J.E.K.; Alcendor, D.J. Targeting COVID-19 Vaccine Hesitancy in Minority Populations in the US: Implications for Herd Immunity. Vaccines 2021, 9, 489. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Ramirez, C.M.; Alvarez, R.M. The politics of vaccine hesitancy in the United States. Soc. Sci. Q. 2022, 103, 42–54. [Google Scholar] [CrossRef]
- Marie Reinhart, A.; Tian, Y.; Lilly, A.E. The role of trust in COVID-19 vaccine hesitancy and acceptance among Black and White Americans. Vaccine 2022, 40, 7247–7254. [Google Scholar] [CrossRef] [PubMed]
- Kriss, J.L.; Hung, M.; Srivastav, A.; Black, C.L.; Lindley, M.C.; Lee, J.T.; Koppaka, R.; Tsai, Y.; Lu, P.-J.; Yankey, D.; et al. COVID-19 Vaccination Coverage, by Race and Ethnicity—National Immunization Survey Adult COVID Module, United States, December 2020–November 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 757–763. [Google Scholar] [CrossRef]
- Ignacio, M.; Oesterle, S.; Mercado, M.; Carver, A.; Lopez, G.; Wolfersteig, W.; Ayers, S.; Ki, S.; Hamm, K.; Parthasarathy, S.; et al. Narratives from African American/Black, American Indian/Alaska Native, and Hispanic/Latinx community members in Arizona to enhance COVID-19 vaccine and vaccination uptake. J. Behav. Med. 2022, 46, 140–152. [Google Scholar] [CrossRef] [PubMed]
- Dada, D.; Nguemo, J.; Sarahann, D.; Demeke, J.; Vlahov, D.; Wilton, L.; Wang, M.; Nelson, L.E. Strategies That Promote Equity in COVID-19 Vaccine Uptake for Black Communities: A Review. J. Urban Health 2022, 99, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Bogart, L.M.; Dong, L.; Gandhi, P.; Klein, D.J.; Smith, T.L.; Ryan, S.; Ojikutu, B. COVID-19 Vaccine Intentions and Mistrust in a National Sample of Black Americans. J. Natl. Med. Assoc. 2022, 113, 599–611. [Google Scholar] [CrossRef] [PubMed]
- King, W.C.; Rubinstein, M.; Reinhart, A.; Mejia, R. Time trends, factors associated with, and reasons for COVID-19 vaccine hesitancy: A massive online survey of US adults from January–May 2021. PLoS ONE 2021, 16, e0260731. [Google Scholar] [CrossRef] [PubMed]
- Rabin, Y.; Kohler, R.E. COVID-19 Vaccination Messengers, Communication Channels, and Messages Trusted Among Black Communities in the USA: A Review. J. Racial Ethn. Health Disparities 2023. [Google Scholar] [CrossRef] [PubMed]
- Okoro, O.; Kennedy, J.; Simmons, G.; Vosen, E.C.; Allen, K.; Singer, D.; Scott, D.; Roberts, R. Exploring the Scope and Dimensions of Vaccine Hesitancy and Resistance to Enhance COVID-19 Vaccination in Black Communities. J Racial Ethn. Health Disparit. 2022, 9, 2117–2130. [Google Scholar] [CrossRef] [PubMed]
- Bagasra, A.B.; Doan, S.; Allen, C.T. Racial differences in institutional trust and COVID-19 vaccine hesitancy and refusal. BMC Public Health 2021, 21, 2104. [Google Scholar] [CrossRef] [PubMed]
- Sekimitsu, S.; Simon, J.; Lindsley, M.M.; Jones, M.; Jalloh, U.; Mabogunje, T.; Kerr, J.; Willingham, M.; Ndousse-Fetter, S.B.; White-Hammond, G.; et al. Exploring COVID-19 Vaccine Hesitancy Amongst Black Americans: Contributing Factors and Motivators. Am. J. Health Promot. 2022, 36, 1304–1315. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Qiao, S.; McKeever, B.W.; Olatosi, B.; Li, X. Listening to Voices from African American Communities in the Southern States about COVID-19 Vaccine Information and Communication: A Qualitative Study. Vaccines 2022, 10, 1046. [Google Scholar] [CrossRef] [PubMed]
- Kricorian, K.; Turner, K. COVID-19 Vaccine Acceptance and Beliefs among Black and Hispanic Americans. PLoS ONE 2021, 16, e0256122. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group. PRISMA-S: An extension to the PRISMA statement for reporting literature searches in systematic reviews. J. Med. Libr. Assoc. 2021, 109, 174–200. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 15 January 2024).
- Young, J.M.; Solomon, M.J. How to critically appraise an article. Nat. Clin. Pract. Gastroenterol. Hepatol. 2009, 6, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Critical Appraisal Skills Programme. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 7 January 2024).
- Appraisal Tool for Cross-Sectional Studies. Available online: https://bmjopen.bmj.com/content/bmjopen/6/12/e011458/DC2/embed/inline-supplementary-material-2.pdf?download=true (accessed on 27 December 2023).
- Wagner, A.L.; Wileden, L.; Shanks, T.R.; Goold, S.D.; Morenoff, J.D.; Sheinfeld Gorin, S.N. Mediators of Racial Differences in COVID-19 Vaccine Acceptance and Uptake: A Cohort Study in Detroit, MI. Vaccines 2021, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Padamsee, T.J.; Bond, R.M.; Dixon, G.N.; Hovick, S.R.; Na, K.; Nisbet, E.C.; Wegener, D.T.; Garrett, R.K. Changes in COVID-19 Vaccine Hesitancy Among Black and White Individuals in the US. JAMA Netw. Open 2022, 5, e2144470. [Google Scholar] [CrossRef] [PubMed]
- Cunningham-Erves, J.; Mayer, C.S.; Han, X.; Fike, L.; Yu, C.; Tousey, P.M.; Schlundt, D.G.; Gupta, D.K.; Mumma, M.T.; Walkley, D.; et al. Factors influencing intent to receive COVID-19 vaccination among Black and White adults in the southeastern United States, October–December 2020. Hum. Vaccines Immunother. 2021, 17, 4761–4798. [Google Scholar] [CrossRef] [PubMed]
- Willis, D.E.; Andersen, J.A.; Montgomery, B.E.E.; Selig, J.P.; Shah, S.K.; Zaller, N.; Bryant-Moore, K.; Scott, A.J.; Williams, M.; McElfish, P.A. COVID-19 Vaccine Hesitancy and Experiences of Discrimination among Black Adults. J. Racial Ethn. Health Disparit. 2023, 10, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Batra, K.; Batra, R. A Theory-Based Analysis of COVID-19 Vaccine Hesitancy among African Americans in the United States: A Recent Evidence. Healthcare 2021, 9, 1273. [Google Scholar] [CrossRef]
- Minaya, C.; McKay, D.; Benton, H.; Blanc, J.; Seixas, A.A. Medical Mistrust, COVID-19 Stress, and Intent to Vaccinate in Racial-Ethnic Minorities. Behav. Sci. 2022, 12, 186. [Google Scholar] [CrossRef]
- Williamson, L.D.; Tarfa, A. Examining the relationships between trust in providers and information, mistrust, and COVID-19 vaccine concerns, necessity, and intentions. BMC Public Health 2022, 22, 2033. [Google Scholar] [CrossRef]
- Ogunbajo, A.; Ojikutu, B.O. Acceptability of COVID-19 vaccines among Black immigrants living in the United States. Vaccine X 2022, 12, 100196. [Google Scholar] [CrossRef]
- McClaran, N.; Rhodes, N.; Yao, S.X. Trust and Coping Beliefs Contribute to Racial Disparities in COVID-19 Vaccination Intention. Health Commun. 2022, 37, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.L.; Sarathchandra, D.; Kessler, M. COVID-19 Vaccination Intake and Intention Among Black and White Residents in Southeast Michigan. J. Immigr. Minor Health 2023, 25, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.S.; Manning, M.; Mitchell, J.; Kim, S.; Harper, F.W.K.; Cresswell, S.; Johns, K.; Pal, S.; Dowe, B.; Tariq, M.; et al. Factors Associated With Racial/Ethnic Group-Based Medical Mistrust and Perspectives on COVID-19 Vaccine Trial Participation and Vaccine Uptake in the US. JAMA Netw. Open 2021, 4, e2111629. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.C.; Gathecha, E.; Kauffman, R.; Wright, S.; Harris, C.M. Healthcare distrust among hospitalised black patients during the COVID-19 pandemic. Postgrad. Med. J. 2022, 98, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Kerrigan, D.; Mantsios, A.; Karver, T.S.; Davis, W.; Taggart, T.; Calabrese, S.K.; Mathews, A.; Robinson, S.; Ruffin, R.; Feaster-Bethea, G.; et al. Context and Considerations for the Development of Community-Informed Health Communication Messaging to Support Equitable Uptake of COVID-19 Vaccines among Communities of Color in Washington, DC. J. Racial Ethn. Health Disparit. 2023, 10, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Villalobos, J.P.; Munoz, A.; Bull, S. Ethnic Minorities’ Perceptions of COVID-19 Vaccines and Challenges in the Pandemic: A Qualitative Study to Inform COVID-19 Prevention Interventions. Health Commun. 2022, 37, 1476–1487. [Google Scholar] [CrossRef] [PubMed]
- Momplaisir, F.; Haynes, N.; Nkwihoreze, H.; Nelson, M.; Werner, R.M.; Jemmott, J. Understanding Drivers of Coronavirus Disease 2019 Vaccine Hesitancy among Blacks. Clin. Infect. Dis. 2021, 73, 1784–1789. [Google Scholar] [CrossRef] [PubMed]
- Bateman, L.B.; Hall, A.G.; Anderson, W.A.; Cherrington, A.L.; Helova, A.; Judd, S.; Kimberly, R.; Oates, G.R.; Osborne, T.; Ott, C.; et al. Exploring COVID-19 Vaccine Hesitancy Among Stakeholders in African American and Latinx Communities in the Deep South Through the Lens of the Health Belief Model. Am. J. Health Promot. 2022, 36, 288–295. [Google Scholar] [CrossRef]
- Majee, W.; Anakwe, A.; Onyeaka, K.; Harvey, I.S. The Past is so Present: Understanding COVID-19 Vaccine Hesitancy among African American Adults Using Qualitative Data. J. Racial Ethn Health Disparit. 2023, 10, 462–474. [Google Scholar] [CrossRef]
- Osakwe, Z.T.; Osborne, J.C.; Osakwe, N.; Stefancic, A. Facilitators of COVID-19 vaccine acceptance among Black and Hispanic individuals in New York: A qualitative study. Am. J. Infect. Control 2022, 50, 268–272. [Google Scholar] [CrossRef]
- Carson, S.L.; Casillas, A.; Castellon-Lopez, Y.; Mansfield, L.N.; Morris, D.; Barron, J.; Ntekume, E.; Landovitz, R.; Vassar, S.D.; Norris, K.C.; et al. COVID-19 Vaccine Decision-making Factors in Racial and Ethnic Minority Communities in Los Angeles, California. JAMA Netw. Open 2021, 4, e2127582. [Google Scholar] [CrossRef]
- Budhwani, H.; Maycock, T.; Murrell, W.; Simpson, T. COVID-19 Vaccine Sentiments among African American or Black Adolescents in Rural Alabama. J. Adolesc. Health 2021, 69, 1041–1043. [Google Scholar] [CrossRef]
- Jimenez, M.E.; Rivera-Núñez, Z.; Crabtree, B.F.; Hill, D.; Pellerano, M.B.; Devance, D.; Macenat, M.; Lima, D.; Martinez Alcaraz, E.; Ferrante, J.M.; et al. Black and Latinx Community Perspectives on COVID-19 Mitigation Behaviors, Testing, and Vaccines. JAMA Netw. Open 2021, 4, e2117074. [Google Scholar] [CrossRef]
- Rios-Fetchko, F.; Carson, M.; Gonzalez Ramirez, M.; Butler, J.Z.; Vargas, R.; Cabrera, A.; Gallegos-Castillo, A.; LeSarre, M.; Liao, M.; Woo, K.; et al. COVID-19 Vaccination Perceptions among Young Adults of Color in the San Francisco Bay Area. Health Equity 2022, 6, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Disparities in COVID-19 Vaccination Rates across Racial and Ethnic Minority Groups in the United States. Issue Brief April 2021. Available online: https://aspe.hhs.gov/sites/default/files/private/pdf/265511/vaccination-disparities-brief.pdf (accessed on 15 January 2024).
- Roat, C.; Webber-Ritchey, K.J.; Spurlark, R.S.; Lee, Y.M. Black Americans Receiving the COVID-19 Vaccine and Effective Strategies to Overcome Barriers: An Integrative Literature Review. J. Racial Ethn Health Disparit. 2023, 10, 2577–2587. [Google Scholar] [CrossRef]
- Siegel, M.; Critchfield-Jain, I.; Boykin, M.; Owens, A.; Muratore, R.; Nunn, T.; Oh, J. Racial/Ethnic Disparities in State-Level COVID-19 Vaccination Rates and Their Association with Structural Racism. J. Racial Ethn. Health Disparit. 2022, 9, 2361–2374. [Google Scholar] [CrossRef]
- Getting the COVID-19 Vaccine: Progress and Equity Questions for the Next Phase. Brookings. 4 March 2021. Available online: https://www.brookings.edu/articles/getting-the-covid-19-vaccine-progress-and-equity-questions-for-the-next-phase/ (accessed on 15 January 2024).
- HRSA. Ensuring Equity in COVID-19 Vaccine Distribution. Available online: https://www.hrsa.gov/coronavirus/health-center-program (accessed on 15 January 2024).
- Yasmin, F.; Najeeb, H.; Moeed, A.; Naeem, U.; Asghar, M.S.; Chughtai, N.U.; Yousaf, Z.; Seboka, B.T.; Ullah, I.; Lin, C.Y.; et al. COVID-19 Vaccine Hesitancy in the United States: A Systematic Review. Front. Public Health 2021, 9, 770985. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Mortality in Adults Aged 65 and Over: United States, 2020. NCHS Data Brief No. 446. October 2022. Available online: https://www.cdc.gov/nchs/data/databriefs/db446.pdf (accessed on 15 January 2024).
- Ahmad, F.B.; Cisewski, J.A.; Xu, J.; Anderson, R.N. COVID-19 Mortality Update—United States, 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 493–496. [Google Scholar] [CrossRef]
- Thunström, L.; Ashworth, M.; Finnoff, D.; Newbold, S.C. Hesitancy toward a COVID-19 vaccine. Ecohealth 2021, 18, 44–60. [Google Scholar] [CrossRef]
- Viskupič, F.; Wiltse, D.L.; Meyer, B.A. Trust in physicians and trust in government predict COVID-19 vaccine uptake. Soc. Sci. Q. 2022, 103, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Fox, A.M. Mistrust in public health institutions is a stronger predictor of vaccine hesitancy and uptake than Trust in Trump. Soc. Sci. Med. 2022, 314, 115440. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccin Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Ohlsen, E.C.; Yankey, D.; Pezzi, C.; Kriss, J.L.; Lu, P.J.; Hung, M.C.; Bernabe, M.I.D.; Kumar, G.S.; Jentes, E.; Elam-Evans, L.D.; et al. Coronavirus Disease 2019 (COVID-19) Vaccination Coverage, Intentions, Attitudes, and Barriers by Race/Ethnicity, Language of Interview, and Nativity—National Immunization Survey Adult COVID Module, 22 April 2021–29 January 2022. Clin. Infect. Dis. 2022, 75 (Suppl. 2), S182–S192. [Google Scholar] [CrossRef] [PubMed]
- Adeagbo, M.; Olukotun, M.; Musa, S.; Alaazi, D.; Allen, U.; Renzaho, A.M.N.; Sekyi-Otu, A.; Salami, B. Improving COVID-19 Vaccine Uptake among Black Populations: A Systematic Review of Strategies. Int. J. Environ. Res. Public Health 2022, 19, 11971. [Google Scholar] [CrossRef]
- Southwell, B.G.; Otero Machuca, J.; Cherry, S.T.; Burnside, M.; Barrett, N.J. Health Misinformation Exposure and Health Disparities: Observations and Opportunities. Annu. Rev. Public Health 2023, 44, 113–130. [Google Scholar] [CrossRef]
- Bleakley, A.; Hennessy, M.; Maloney, E.; Young, D.G.; Crowley, J.; Silk, K.; Langbaum, J.B. Psychosocial Determinants of COVID-19 Vaccination Intention among White, Black, and Hispanic Adults in the US. Ann. Behav. Med. 2022, 56, 347–356. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savoia, E.; Masterson, E.; Olander, D.R.; Anderson, E.; Mohamed Farah, A.; Pirrotta, L. Determinants of Vaccine Hesitancy among African American and Black Individuals in the United States of America: A Systematic Literature Review. Vaccines 2024, 12, 277. https://doi.org/10.3390/vaccines12030277
Savoia E, Masterson E, Olander DR, Anderson E, Mohamed Farah A, Pirrotta L. Determinants of Vaccine Hesitancy among African American and Black Individuals in the United States of America: A Systematic Literature Review. Vaccines. 2024; 12(3):277. https://doi.org/10.3390/vaccines12030277
Chicago/Turabian StyleSavoia, Elena, Evelyn Masterson, David R. Olander, Emma Anderson, Anisa Mohamed Farah, and Luca Pirrotta. 2024. "Determinants of Vaccine Hesitancy among African American and Black Individuals in the United States of America: A Systematic Literature Review" Vaccines 12, no. 3: 277. https://doi.org/10.3390/vaccines12030277
APA StyleSavoia, E., Masterson, E., Olander, D. R., Anderson, E., Mohamed Farah, A., & Pirrotta, L. (2024). Determinants of Vaccine Hesitancy among African American and Black Individuals in the United States of America: A Systematic Literature Review. Vaccines, 12(3), 277. https://doi.org/10.3390/vaccines12030277