
Burden and Impact of Reactogenicity among Adults Receiving COVID-19 Vaccines in the United States and Canada: Results from a Prospective Observational Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
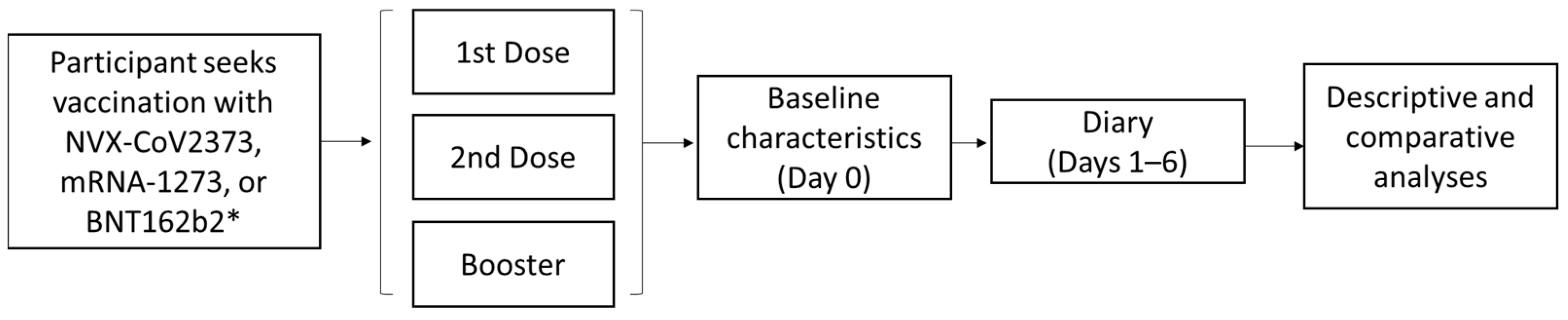
2.1. Study Design
2.2. Participants
2.3. Survey Instruments
2.4. Objectives
2.5. Statistics
Sample Size and Analyses
3. Results
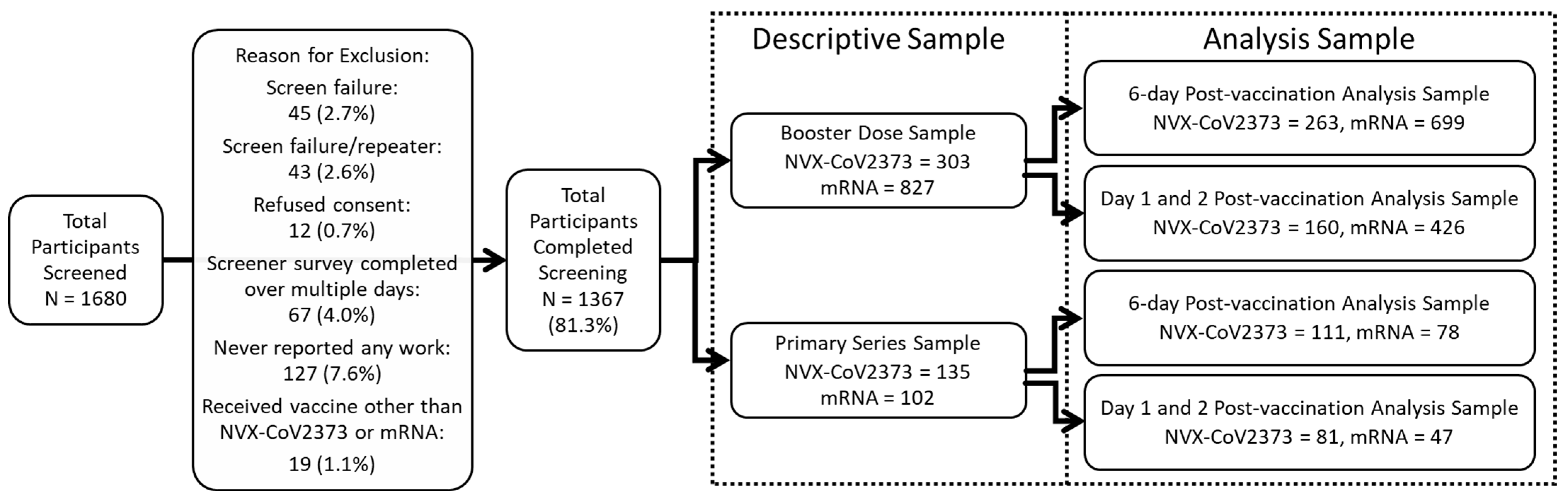
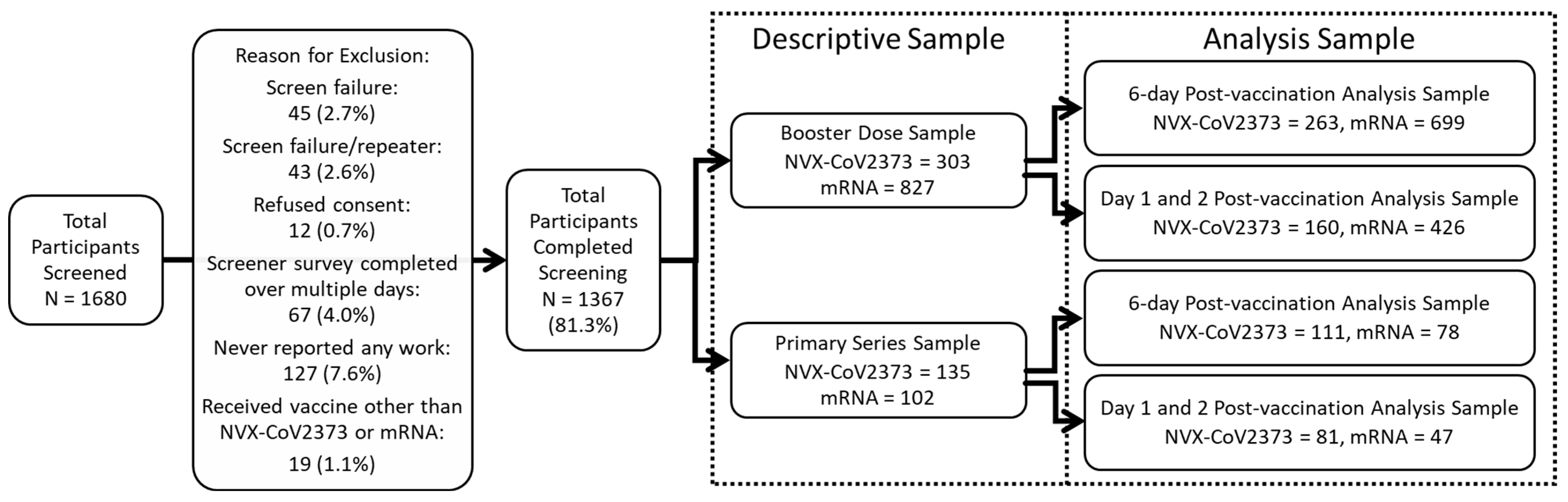
3.1. Participants
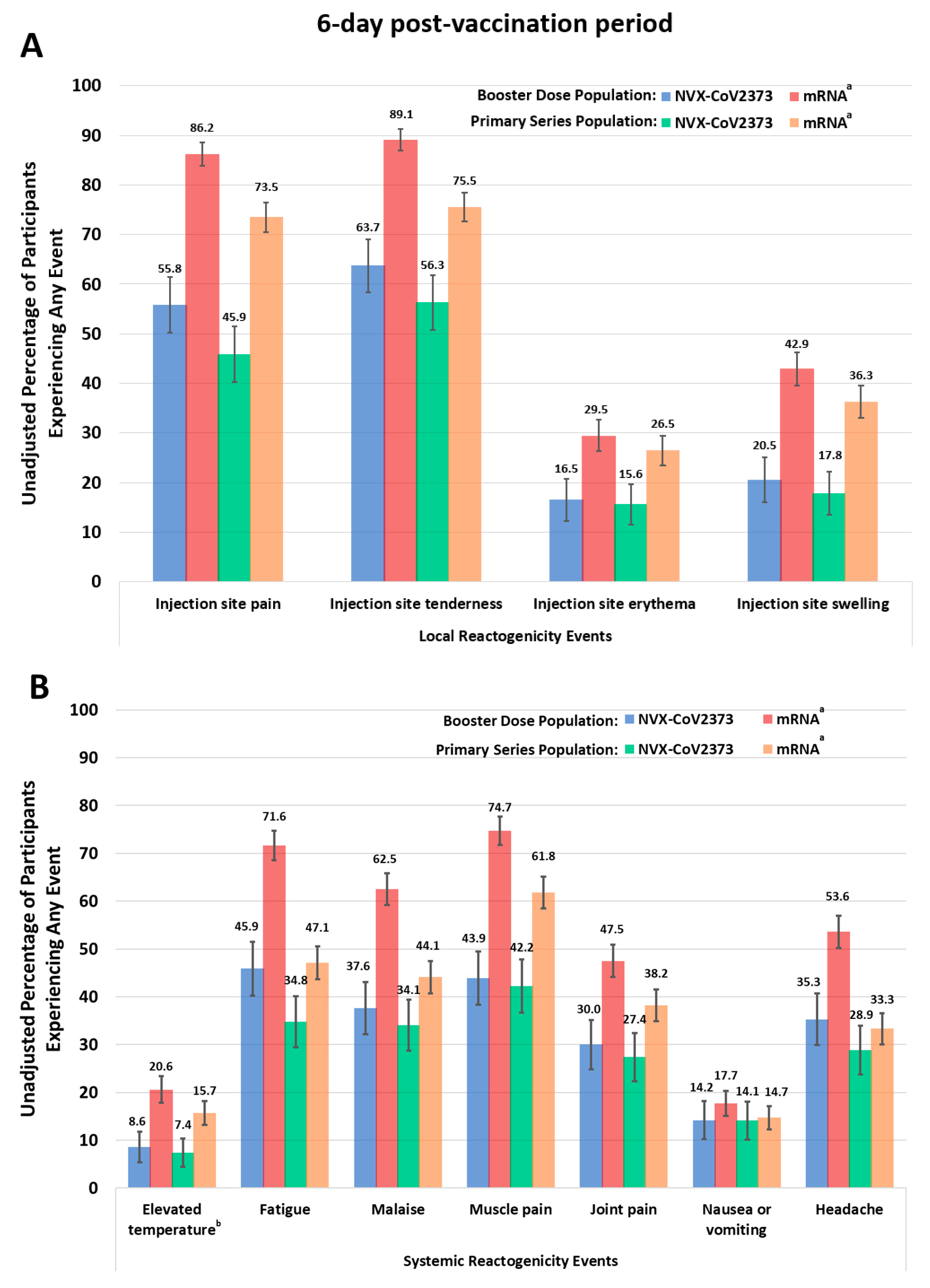
3.2. Responses to Vaccine-Related Local and Systemic Reactogenicity Symptoms
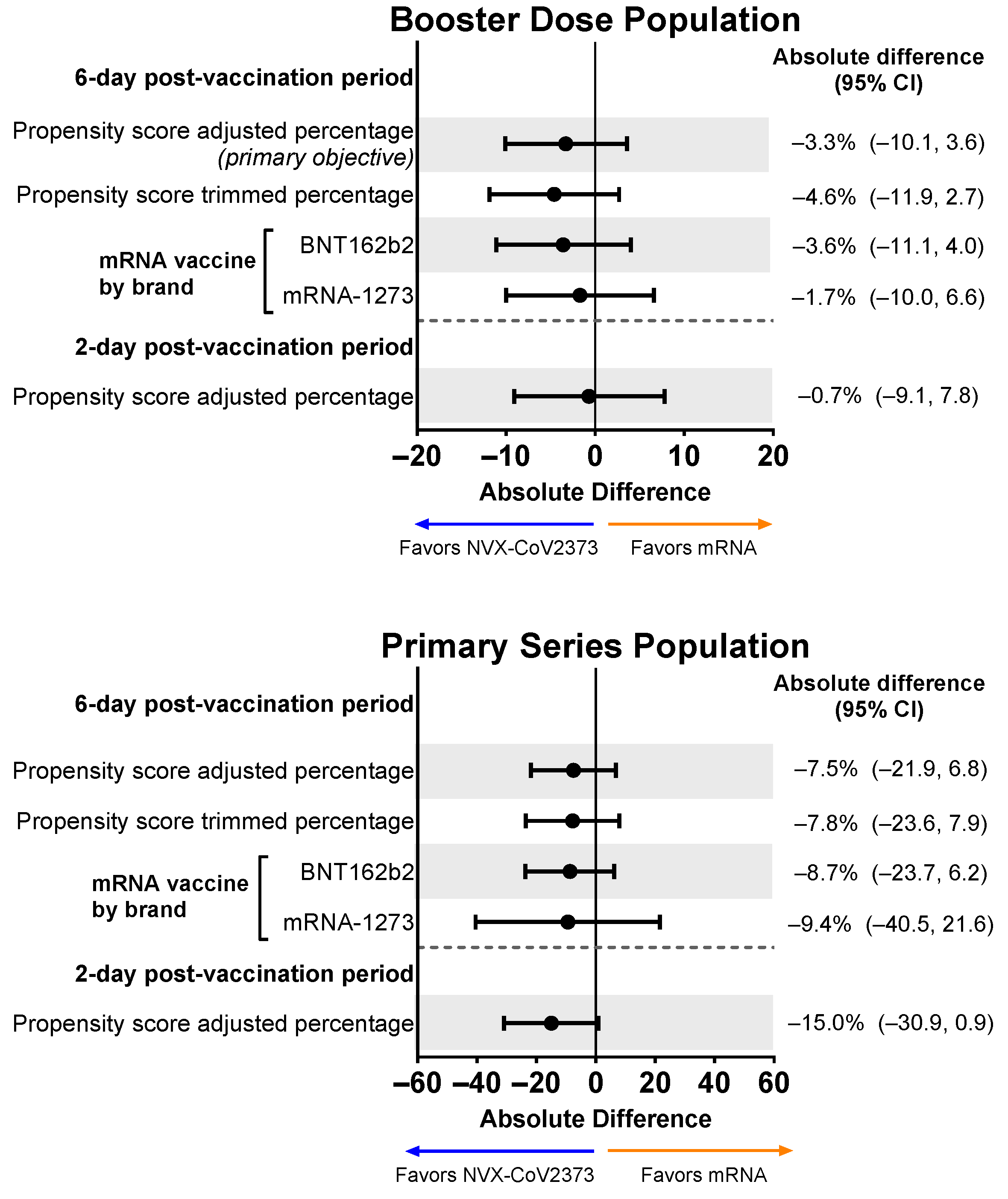
3.3. Overall Work Impairment after Vaccination
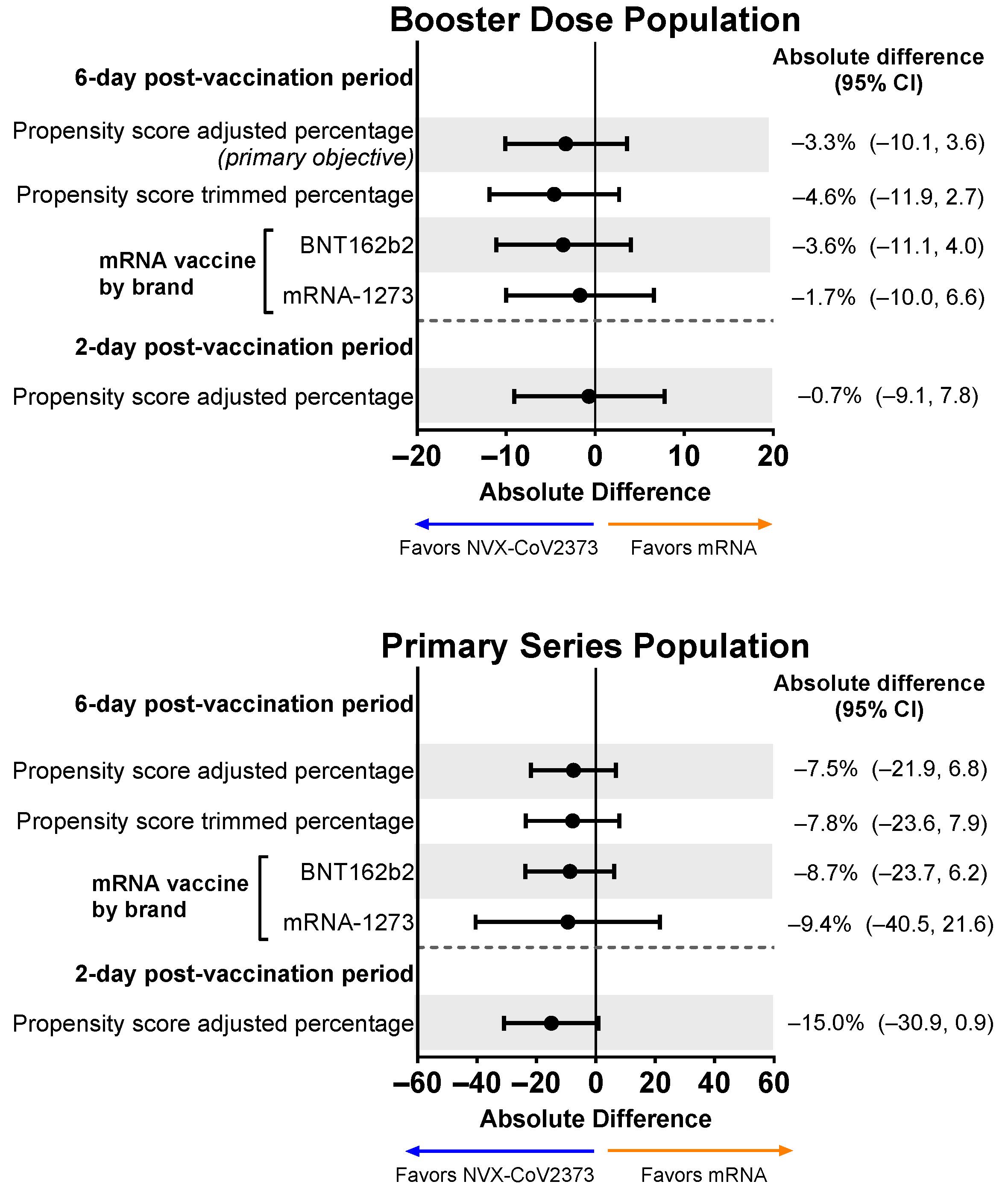
3.3.1. Participants with an Overall Work Impairment Score of ≥50%
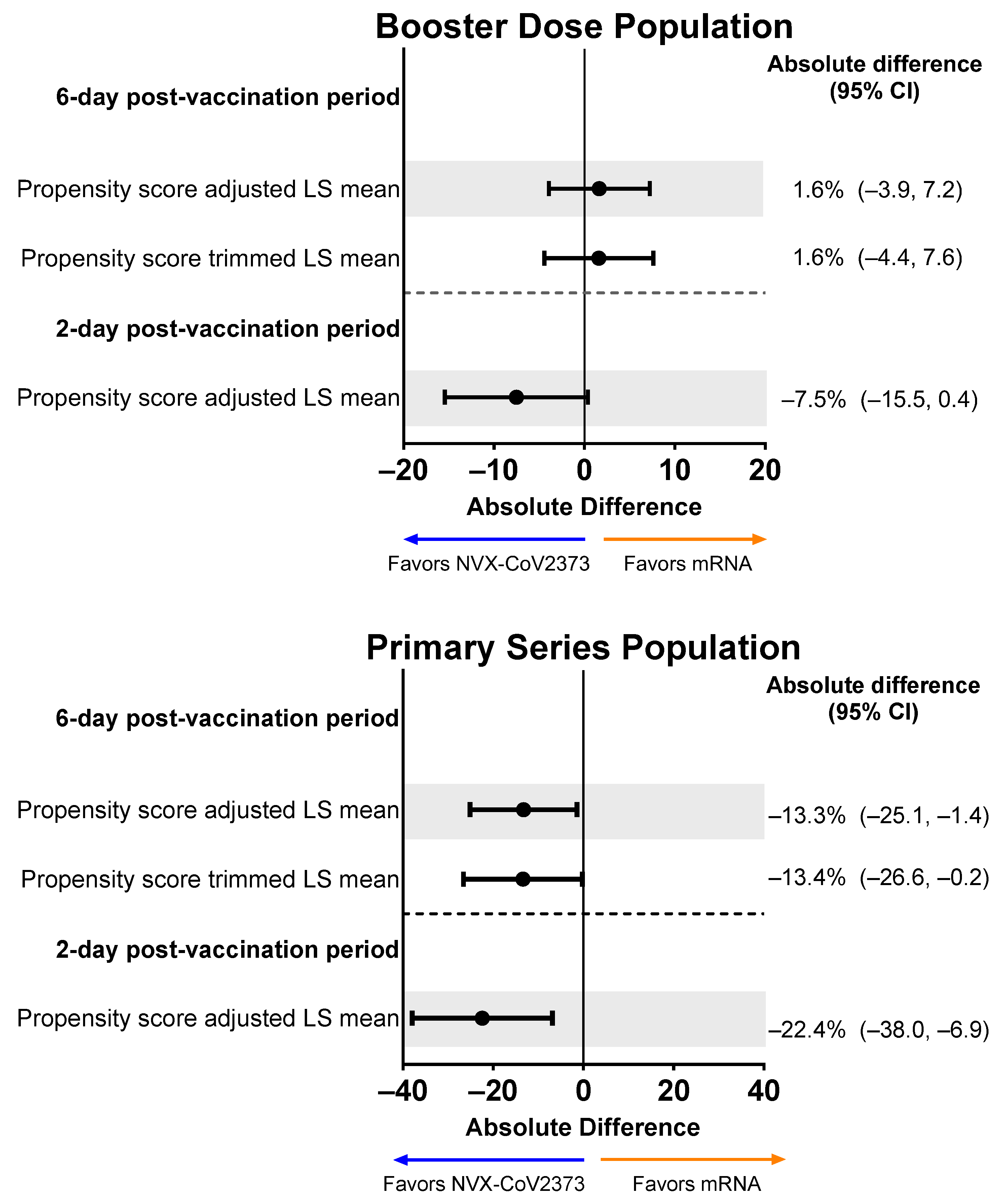
3.3.2. Mean Percentages of Overall Work Impairment
3.4. Missed Work after Vaccination
3.5. Impairment While Working after Vaccination
3.6. Non-Work Activity Impairment after Vaccination
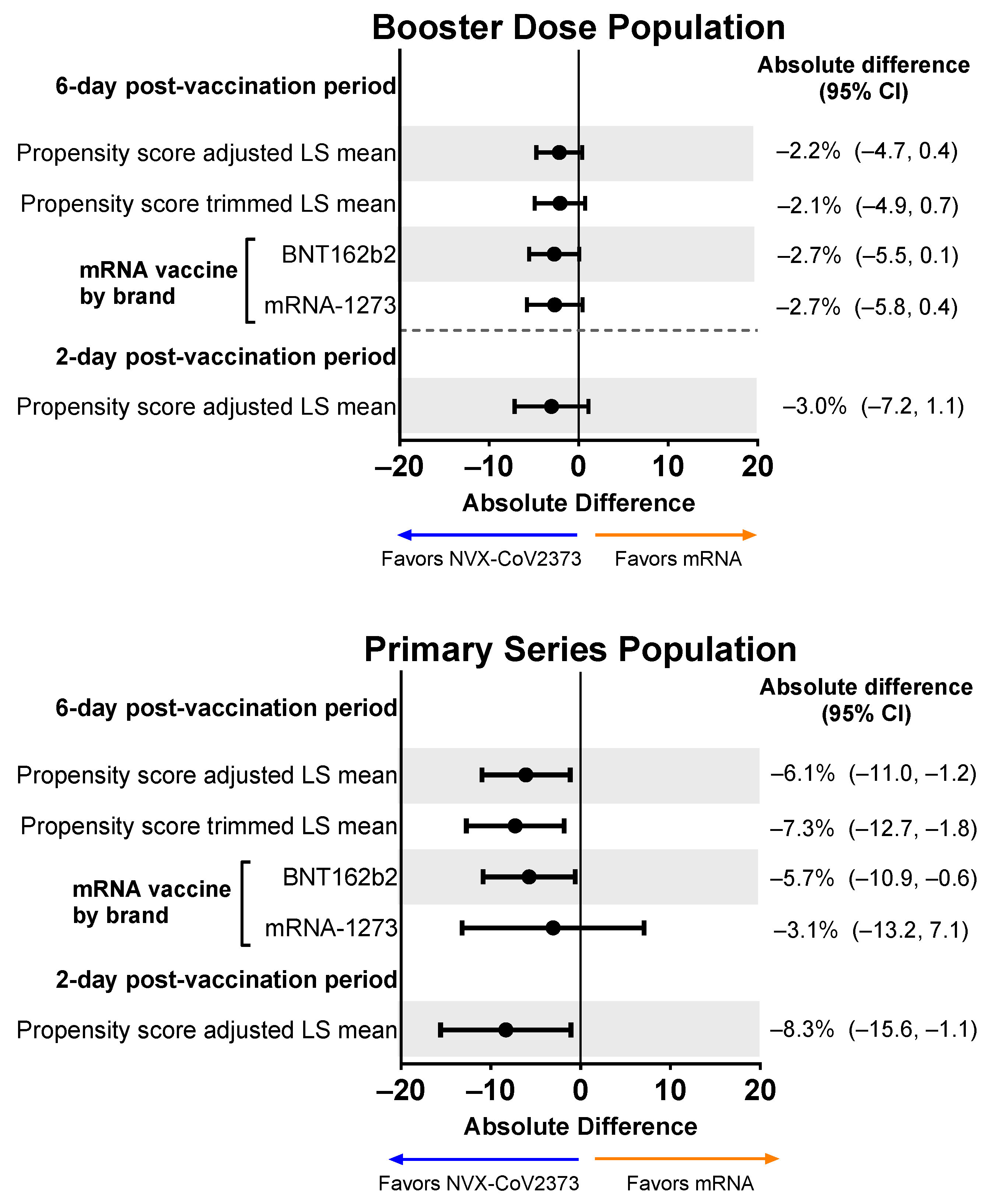
3.7. Diminished Work Performance after Vaccination
3.8. Healthcare Utilization
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Legal Disclosure
References
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; Consortium, C.-G.U.; Peacock, S.J.; Barclay, W.S.; de Silva, T.I.; Towers, G.J.; et al. SARS-CoV-2 variant biology: Immune escape, transmission and fitness. Nat. Rev. Microbiol. 2023, 21, 162–177. [Google Scholar] [CrossRef]
- Food and Drug Administration. Pfizer-BioNTech COVID-19 Vaccines. 2023. Available online: https://www.fda.gov/vaccines-blood-biologics/coronavirus-covid-19-cber-regulated-biologics/pfizer-biontech-covid-19-vaccines (accessed on 7 July 2023).
- Food and Drug Administration. Moderna COVID-19 Vaccines. 6 June 2023. Available online: https://www.fda.gov/vaccines-blood-biologics/coronavirus-covid-19-cber-regulated-biologics/moderna-covid-19-vaccines (accessed on 7 July 2023).
- Food and Drug Administration. Janssen COVID-19 Vaccine. 6 June 2023. Available online: https://www.fda.gov/vaccines-blood-biologics/coronavirus-covid-19-cber-regulated-biologics/janssen-covid-19-vaccine (accessed on 7 July 2023).
- Food and Drug Administration. Novavax COVID-19 Vaccine, Adjuvanted. 6 June 2023. Available online: https://www.fda.gov/vaccines-blood-biologics/coronavirus-covid-19-cber-regulated-biologics/novavax-covid-19-vaccine-adjuvanted (accessed on 7 July 2023).
- Health Canada. Approved COVID-19 Vaccines. 17 April 2023. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/drugs-vaccines-treatments/vaccines.html (accessed on 7 July 2023).
- Health Canada. Medicago Covifenz COVID-19 Vaccine. 17 April 2023. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/drugs-vaccines-treatments/vaccines/medicago.html (accessed on 7 July 2023).
- Mbaeyi, S.; Oliver, S.E.; Collins, J.P.; Godfrey, M.; Goswami, N.D.; Hadler, S.C.; Jones, J.; Moline, H.; Moulia, D.; Reddy, S.; et al. The Advisory Committee on Immunization Practices′ Interim Recommendations for Additional Primary and Booster Doses of COVID-19 Vaccines—United States, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Ao, D.; He, X.; Hong, W.; Wei, X. The rapid rise of SARS-CoV-2 Omicron subvariants with immune evasion properties: XBB.1.5 and BQ.1.1 subvariants. MedComm 2023, 4, e239. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. FDA Authorizes Moderna, Pfizer-BioNTech Bivalent COVID-19 Vaccines for Use as a Booster Dose. 31 August 2022. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-moderna-pfizer-biontech-bivalent-covid-19-vaccines-use (accessed on 29 September 2022).
- European Medicines Agency. EMA and ECDC Statement on Updating COVID-19 Vaccines to Target New SARS-CoV-2 Virus Variants. 2023. Available online: https://www.ema.europa.eu/en/news/ema-ecdc-statement-updating-covid-19-vaccines-target-new-sars-cov-2-virus-variants (accessed on 7 July 2023).
- Food and Drug Administration. Recommendation for the 2023–2024 Formula of COVID-19 Vaccines in the U.S. 6 June 2023. Available online: https://www.fda.gov/media/169591/download (accessed on 7 July 2023).
- World Health Organization. Statement on the Antigen Composition of COVID-19 Vaccines. 18 May 2023. Available online: https://www.who.int/news/item/18-05-2023-statement-on-the-antigen-composition-of-covid-19-vaccines (accessed on 7 July 2023).
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cardenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Alves, K.; Plested, J.S.; Galbiati, S.; Chau, G.; Cloney-Clark, S.; Zhu, M.; Kalkeri, R.; Patel, N.; Smith, K.; Marcheschi, A.; et al. Immunogenicity and safety of a fourth homologous dose of NVX-CoV2373. Vaccine 2023, 41, 4280–4286. [Google Scholar] [CrossRef]
- Anez, G.; Dunkle, L.M.; Gay, C.L.; Kotloff, K.L.; Adelglass, J.M.; Essink, B.; Campbell, J.D.; Cloney-Clark, S.; Zhu, M.; Plested, J.S.; et al. Safety, Immunogenicity, and Efficacy of the NVX-CoV2373 COVID-19 Vaccine in Adolescents: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e239135. [Google Scholar] [CrossRef]
- Dunkle, L.M.; Kotloff, K.L.; Gay, C.L.; Anez, G.; Adelglass, J.M.; Barrat Hernandez, A.Q.; Harper, W.L.; Duncanson, D.M.; McArthur, M.A.; Florescu, D.F.; et al. Efficacy and Safety of NVX-CoV2373 in Adults in the United States and Mexico. N. Engl. J. Med. 2022, 386, 531–543. [Google Scholar] [CrossRef]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef]
- Al-Obaydi, S.; Hennrikus, E.; Mohammad, N.; Lehman, E.B.; Thakur, A.; Al-Shaikhly, T. Hesitancy and reactogenicity to mRNA-based COVID-19 vaccines-Early experience with vaccine rollout in a multi-site healthcare system. PLoS ONE 2022, 17, e0272691. [Google Scholar] [CrossRef] [PubMed]
- Breeher, L.E.; Wolf, M.E.; Geyer, H.; Brinker, T.; Tommaso, C.; Kohlnhofer, S.; Hainy, C.; Swift, M. Work Absence Following COVID-19 Vaccination in a Cohort of Healthcare Personnel. J. Occup. Environ. Med. 2022, 64, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Chrissian, A.A.; Oyoyo, U.E.; Patel, P.; Lawrence Beeson, W.; Loo, L.K.; Tavakoli, S.; Dubov, A. Impact of COVID-19 vaccine-associated side effects on health care worker absenteeism and future booster vaccination. Vaccine 2022, 40, 3174–3181. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Greenberg, P.; Formanowski, B.; Parikh, P.D. Are COVID-19 mRNA vaccine side effects severe enough to cause missed work? Cross-sectional study of health care-associated workers. Medicine 2022, 101, e28839. [Google Scholar] [CrossRef] [PubMed]
- Costa, K. Older Adults’ Intentions and Attitudes Toward the Updated Bivalent COVID-19 Booster: 241 Survey, United States, April 2023. Available online: https://www.healthcanal.com/health/the-bivalent-covid24219-booster-survey (accessed on 7 June 2023).
- Long, S.; Wu, J.; Wang, S.; Zhao, Y.; Wang, J.; Zhao, S.; Niu, Q.; Jin, H. Changes of factors associated with vaccine hesitancy in Chinese residents: A qualitative study. Front. Public Health 2022, 10, 929407. [Google Scholar] [CrossRef] [PubMed]
- Rief, W. Fear of Adverse Effects and COVID-19 Vaccine Hesitancy: Recommendations of the Treatment Expectation Expert Group. JAMA Health Forum 2021, 2, e210804. [Google Scholar] [CrossRef]
- Rosiello, D.F.; Anwar, S.; Yufika, A.; Adam, R.Y.; Ismaeil, M.I.H.; Dahman, N.B.H.; Hafsi, M.; Ferjani, M.; Sami, F.S.; Monib, F.A.; et al. Acceptance of COVID-19 vaccination at different hypothetical efficacy and safety levels in ten countries in Asia, Africa, and South America. Narra J 2021, 1, e55. [Google Scholar] [CrossRef]
- D′Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Glynn, R.J.; Schneeweiss, S.; Sturmer, T. Indications for propensity scores and review of their use in pharmacoepidemiology. Basic Clin. Pharm. Toxicol. 2006, 98, 253–259. [Google Scholar] [CrossRef]
- Perkins, S.M.; Tu, W.; Underhill, M.G.; Zhou, X.H.; Murray, M.D. The use of propensity scores in pharmacoepidemiologic research. Pharmacoepidemiol. Drug Saf. 2000, 9, 93–101. [Google Scholar] [CrossRef]
- Robins, J.M.; Hernan, M.A.; Brumback, B. Marginal structural models and causal inference in epidemiology. Epidemiology 2000, 11, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity Following Receipt of mRNA-Based COVID-19 Vaccines. JAMA 2021, 325, 2201–2202. [Google Scholar] [CrossRef] [PubMed]
- Nachtigall, I.; Bonsignore, M.; Hohenstein, S.; Bollmann, A.; Gunther, R.; Kodde, C.; Englisch, M.; Ahmad-Nejad, P.; Schroder, A.; Glenz, C.; et al. Effect of gender, age and vaccine on reactogenicity and incapacity to work after COVID-19 vaccination: A survey among health care workers. BMC Infect. Dis. 2022, 22, 291. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Fact Sheet For Healthcare Providers Administering Vaccine: Emergency Use Authorization of Novavax COVID-19 Vac-cine, Adjuvanted (2023-2024 Formula), for Individuals 12 Years of Age and Older. 2023. Available online: https://www.fda.gov/media/159897/download (accessed on 27 October 2023).
- Sutton, N.; San Francisco Ramos, A.; Beales, E.; Smith, D.; Ikram, S.; Galiza, E.; Hsia, Y.; Heath, P.T. Comparing reactogenicity of COVID-19 vaccines: A systematic review and meta-analysis. Expert Rev. Vaccines 2022, 21, 1301–1318. [Google Scholar] [CrossRef] [PubMed]
- Werner, F.; Zeschick, N.; Kuhlein, T.; Steininger, P.; Uberla, K.; Kaiser, I.; Sebastiao, M.; Hueber, S.; Warkentin, L. Patient-reported reactogenicity and safety of COVID-19 vaccinations vs. comparator vaccinations: A comparative observational cohort study. BMC Med. 2023, 21, 358. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous COVID-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Lyke, K.E.; Atmar, R.L.; Dominguez Islas, C.; Posavad, C.M.; Deming, M.E.; Branche, A.R.; Johnston, C.; El Sahly, H.M.; Edupuganti, S.; Mulligan, M.J.; et al. Immunogenicity of NVX-CoV2373 heterologous boost against SARS-CoV-2 variants. NPJ Vaccines 2023, 8, 98. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Marchese, A.M.; Rousculp, M.; Macbeth, J.; Beyhaghi, H.; Seet, B.T.; Toback, S. The Novavax Heterologous COVID Booster Demonstrates Lower Reactogenicity Than mRNA: A Targeted Review. J. Infect. Dis. 2023, jiad519. [Google Scholar] [CrossRef]
- Salter, S.M.; Li, D.; Trentino, K.; Nissen, L.; Lee, K.; Orlemann, K.; Peters, I.; Murray, K.; Leeb, A.; Deng, L. Safety of Four COVID-19 Vaccines across Primary Doses 1, 2, 3 and Booster: A Prospective Cohort Study of Australian Community Pharmacy Vaccinations. Vaccines 2022, 10, 2017. [Google Scholar] [CrossRef] [PubMed]
- Stuart, A.S.V.; Shaw, R.H.; Liu, X.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Immunogenicity, safety, and reactogenicity of heterologous COVID-19 primary vaccination incorporating mRNA, viral-vector, and protein-adjuvant vaccines in the UK (Com-COV2): A single-blind, randomised, phase 2, non-inferiority trial. Lancet 2022, 399, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Di Fusco, M.; Sun, X.; Moran, M.M.; Coetzer, H.; Zamparo, J.M.; Alvarez, M.B.; Puzniak, L.; Tabak, Y.P.; Cappelleri, J.C. Impact of COVID-19 and effects of booster vaccination with BNT162b2 on six-month long COVID symptoms, quality of life, work productivity and activity impairment during Omicron. J. Patient Rep. Outcomes 2023, 7, 77. [Google Scholar] [CrossRef]
- Di Fusco, M.; Sun, X.; Moran, M.M.; Coetzer, H.; Zamparo, J.M.; Puzniak, L.; Alvarez, M.B.; Tabak, Y.P.; Cappelleri, J.C. Impact of COVID-19 and effects of BNT162b2 on patient-reported outcomes: Quality of life, symptoms, and work productivity among US adult outpatients. J. Patient Rep. Outcomes 2022, 6, 123. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Booster Dose Population | Primary Series Population | |||
|---|---|---|---|---|
| Parameter | NVX-CoV2373 (n = 303) | mRNA Vaccine a (n = 827) | NVX-CoV2373 (n = 135) | mRNA Vaccine a (n = 102) |
| Age, mean (SD) years | 38.9 (11.8) | 40.1 (13.0) | 37.8 (11.0) | 34.9 (12.0) |
| Gender identity, n (%) | ||||
| Female | 156 (51.5) | 469 (56.7) | 65 (48.1) | 62 (60.8) |
| Male | 142 (46.9) | 355 (42.9) | 69 (51.1) | 40 (39.2) |
| Genderfluid | 1 (0.3) | 0 | 0 | 0 |
| Nonbinary | 2 (0.7) | 3 (0.4) | 0 | 0 |
| A gender identity not listed | 0 | 0 | 0 | 0 |
| Prefer not to answer | 2 (0.7) | 0 | 1 (0.7) | 0 |
| Race/ethnicity b, n (%) | ||||
| African American or Black | 33 (10.9) | 77 (9.3) | 16 (11.9) | 17 (16.7) |
| Alaska Native, American Indian, or Native American | 2 (0.7) | 4 (0.5) | 2 (1.5) | 0 |
| Asian c | 40 (13.2) | 189 (22.9) | 3 (2.2) | 0 |
| Hispanic, Latin American, or Latinx | 154 (50.8) | 207 (25.0) | 98 (72.6) | 67 (65.7) |
| Middle Eastern or North African d | 5 (1.7) | 21 (2.5) | 0 | 0 |
| Native Hawaiian or Pacific Islander e | 6 (2.0) | 75 (9.1) | 0 | 1 (1.0) |
| White | 152 (50.2) | 278 (33.6) | 23 (17.0) | 32 (31.4) |
| Race or ethnicity not listed | 3 (1.0) | 13 (1.6) | 0 | 0 |
| Prefer not to answer | 6 (2.0) | 5 (0.6) | 2 (1.5) | 1 (1.0) |
| Education level, n (%) | ||||
| Less than secondary (high) school graduation | 4 (1.3) | 15 (1.8) | 3 (2.2) | 3 (2.9) |
| Secondary (high) school diploma or equivalent | 70 (23.1) | 145 (17.5) | 73 (54.1) | 41 (40.2) |
| Some college/post-secondary school | 66 (21.8) | 153 (18.5) | 24 (17.8) | 32 (31.4) |
| College degree/post-secondary certificate, diploma, or degree | 80 (26.4) | 305 (36.9) | 21 (15.6) | 19 (18.6) |
| Professional, advanced, or graduate degree | 49 (16.2) | 202 (24.4) | 12 (8.9) | 5 (4.9) |
| Prefer not to answer | 34 (11.2) | 7 (0.8) | 2 (1.5) | 2 (2.0) |
| Work from home or work outside of the home, n (%) | ||||
| Work from home | 55 (18.2) | 196 (23.7) | 18 (13.3) | 7 (6.9) |
| Work outside the home | 237 (78.2) | 616 (74.5) | 115 (85.2) | 93 (91.2) |
| Prefer not to answer | 11 (3.6) | 15 (1.8) | 2 (1.5) | 2 (2.0) |
| Type of job, n (%) | ||||
| Executive, administrator, or senior manager | 10 (3.3) | 57 (6.9) | 3 (2.2) | 1 (1.0) |
| Professional | 58 (19.1) | 257 (31.1) | 11 (8.1) | 8 (7.8) |
| Technical support | 30 (9.9) | 63 (7.6) | 7 (5.2) | 5 (4.9) |
| Sales | 37 (12.2) | 59 (7.1) | 17 (12.6) | 16 (15.7) |
| Clerical and administrative support | 18 (5.9) | 91 (11.0) | 6 (4.4) | 8 (7.8) |
| Service occupation | 44 (14.5) | 118 (14.3) | 46 (34.1) | 38 (37.3) |
| Precision production and crafts worker | 8 (2.6) | 17 (2.1) | 23 (17.0) | 4 (3.9) |
| Operator or laborer | 23 (7.6) | 84 (10.2) | 17 (12.6) | 15 (14.7) |
| Active military | 1 (0.3) | 0 | 0 | 0 |
| Prefer not to answer | 74 (24.4) | 81 (9.8) | 5 (3.7) | 7 (6.9) |
| Annual income from all employment, n (%) | ||||
| $1 to $9999 | 5 (1.7) | 25 (3.0) | 7 (5.2) | 6 (5.9) |
| $10,000 to $24,999 | 37 (12.2) | 114 (13.8) | 26 (19.3) | 22 (21.6) |
| $25,000 to $49,999 | 88 (29.0) | 216 (26.1) | 36 (26.7) | 42 (41.2) |
| $50,000 to $99,999 | 63 (20.8) | 223 (27.0) | 20 (14.8) | 11 (10.8) |
| $100,000 to $199,999 | 29 (9.6) | 106 (12.8) | 3 (2.2) | 0 |
| $200,000 to $499,999 | 1 (0.3) | 17 (2.1) | 0 | 0 |
| $500,000 or more | 0 | 1 (0.1) | 0 | 0 |
| Prefer not to answer | 80 (26.4) | 125 (15.1) | 43 (31.9) | 21 (20.6) |
| Essential worker, n (%) | ||||
| Yes | 134 (44.2) | 390 (47.2) | 73 (54.1) | 56 (54.9) |
| No | 137 (45.2) | 400 (48.4) | 36 (26.7) | 33 (32.4) |
| Prefer not to answer | 32 (10.6) | 37 (4.5) | 26 (19.3) | 13 (12.7) |
| Prior COVID-19 diagnosis, n (%) | 119 (39.3) | 433 (52.4) | 47 (34.8) | 49 (48.0) |
| Medical condition that puts participant at high risk for severe COVID-19 b, n (%) | 19 (6.3) | 45 (5.4) | 1 (0.7) | 4 (3.9) |
| Diabetes | 6 (31.6) | 21 (46.7) | 0 | 0 |
| Hypertension | 7 (36.8) | 13 (28.9) | 0 | 0 |
| Heart disease | 2 (10.5) | 8 (17.8) | 0 | 0 |
| Respiratory conditions | 5 (26.3) | 11 (24.4) | 0 | 1 (25.0) |
| Other | 5 (26.3) | 13 (28.9) | 1 (100) | 3 (75.0) |
| Booster dose, n (%) | ||||
| First | 184 (60.7) | 309 (37.4) | – | – |
| Second or later | 119 (39.3) | 518 (62.6) | – | – |
| mRNA vaccine type, n (%) | ||||
| Monovalent | – | 652 (78.8) | - | 102 (100) |
| Bivalent | – | 175 (21.2) | - | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rousculp, M.D.; Hollis, K.; Ziemiecki, R.; Odom, D.; Marchese, A.M.; Montazeri, M.; Odak, S.; Jackson, L.; Miller, A.; Toback, S. Burden and Impact of Reactogenicity among Adults Receiving COVID-19 Vaccines in the United States and Canada: Results from a Prospective Observational Study. Vaccines 2024, 12, 83. https://doi.org/10.3390/vaccines12010083
Rousculp MD, Hollis K, Ziemiecki R, Odom D, Marchese AM, Montazeri M, Odak S, Jackson L, Miller A, Toback S. Burden and Impact of Reactogenicity among Adults Receiving COVID-19 Vaccines in the United States and Canada: Results from a Prospective Observational Study. Vaccines. 2024; 12(1):83. https://doi.org/10.3390/vaccines12010083
Chicago/Turabian StyleRousculp, Matthew D., Kelly Hollis, Ryan Ziemiecki, Dawn Odom, Anthony M. Marchese, Mitra Montazeri, Shardul Odak, Laurin Jackson, Angela Miller, and Seth Toback. 2024. "Burden and Impact of Reactogenicity among Adults Receiving COVID-19 Vaccines in the United States and Canada: Results from a Prospective Observational Study" Vaccines 12, no. 1: 83. https://doi.org/10.3390/vaccines12010083
APA StyleRousculp, M. D., Hollis, K., Ziemiecki, R., Odom, D., Marchese, A. M., Montazeri, M., Odak, S., Jackson, L., Miller, A., & Toback, S. (2024). Burden and Impact of Reactogenicity among Adults Receiving COVID-19 Vaccines in the United States and Canada: Results from a Prospective Observational Study. Vaccines, 12(1), 83. https://doi.org/10.3390/vaccines12010083