
Long-Term Immune Response Profiles to SARS-CoV-2 Vaccination and Infection in People with Multiple Sclerosis on Anti-CD20 Therapy

 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Assessment of T-Cellular Responses to SARS-CoV-2
2.3. Assessment of Humoral Responses to SARS-CoV-2
2.4. Statistical Analysis
3. Results
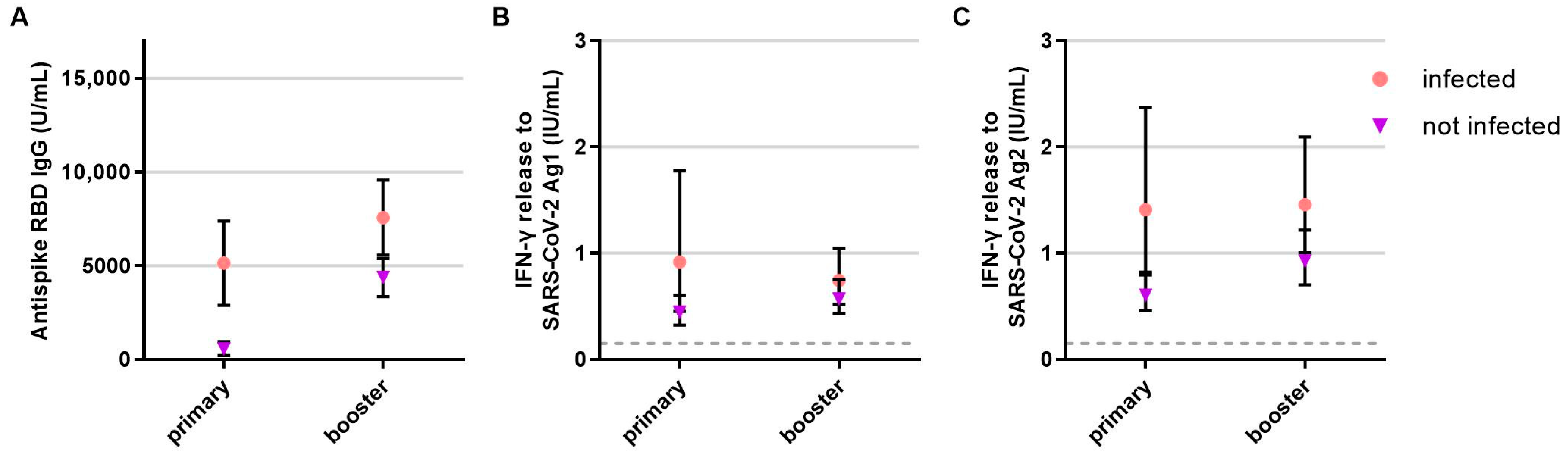
3.1. Patient Characteristics after Primary Vaccination
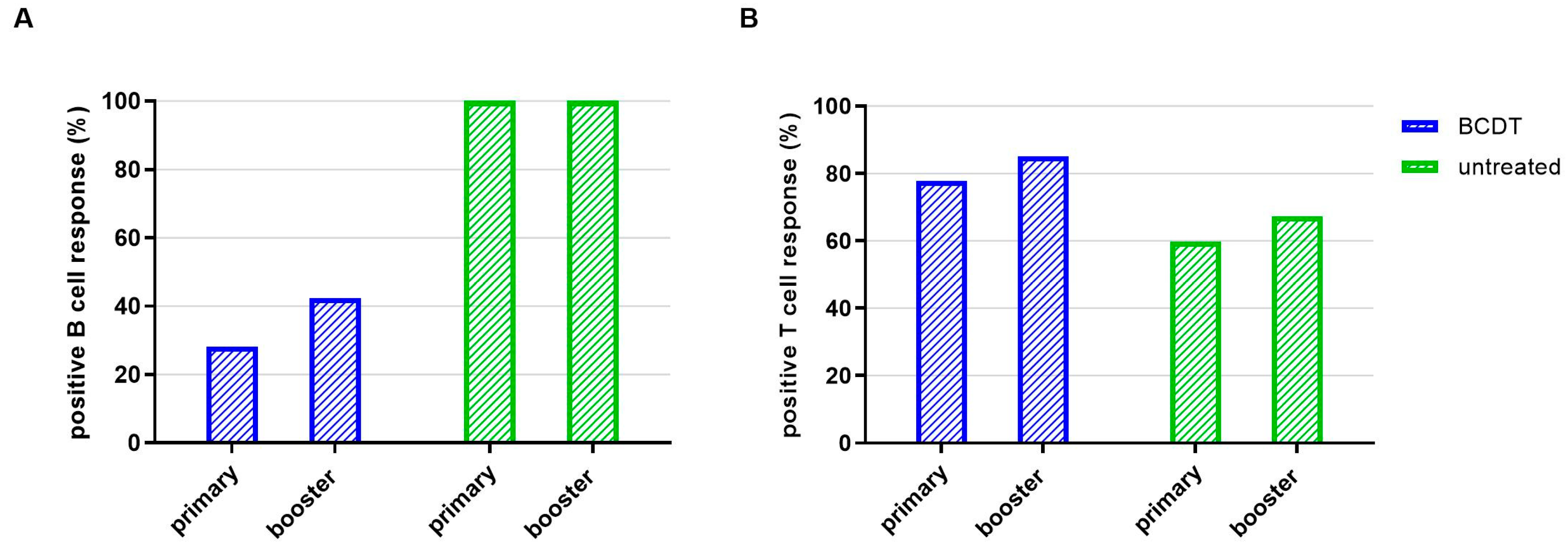
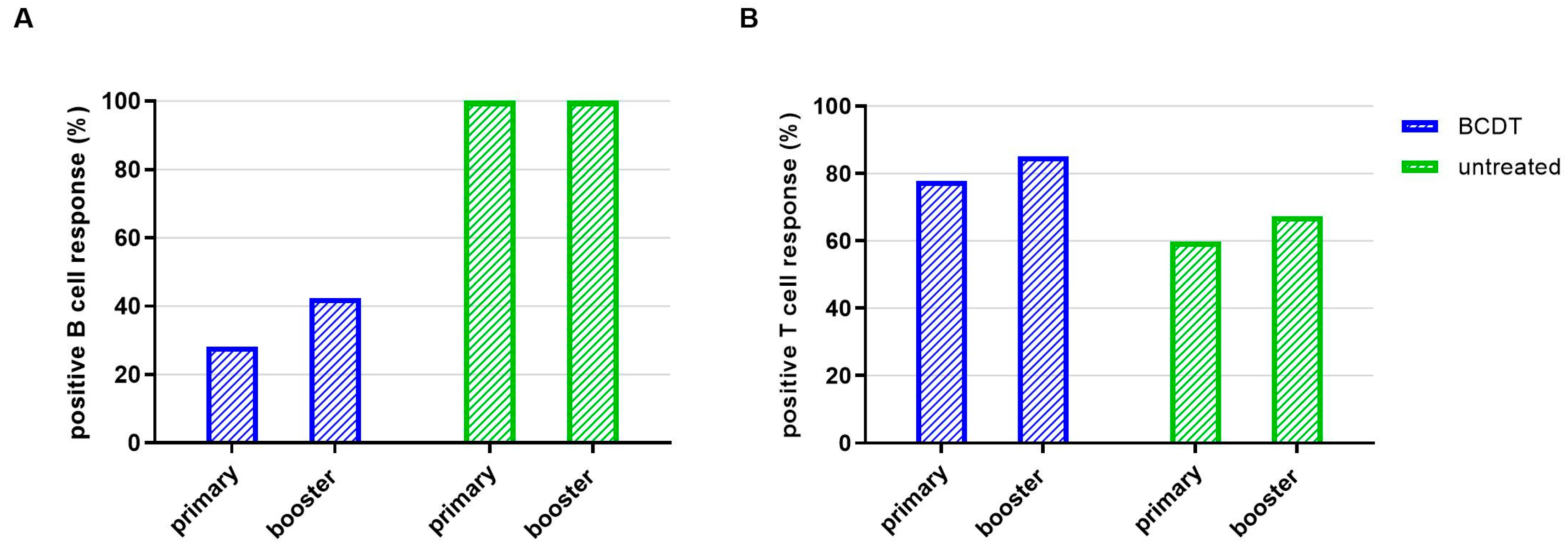
3.2. SARS-CoV-2-Specific T- and B-Cellular Immune Response after Primary Vaccination
3.3. Patient Characteristics in the Cohort after Booster Immunsation
3.4. SARS-CoV-2-Specific T- and B-Cellular Immune Response after Booster Vaccination
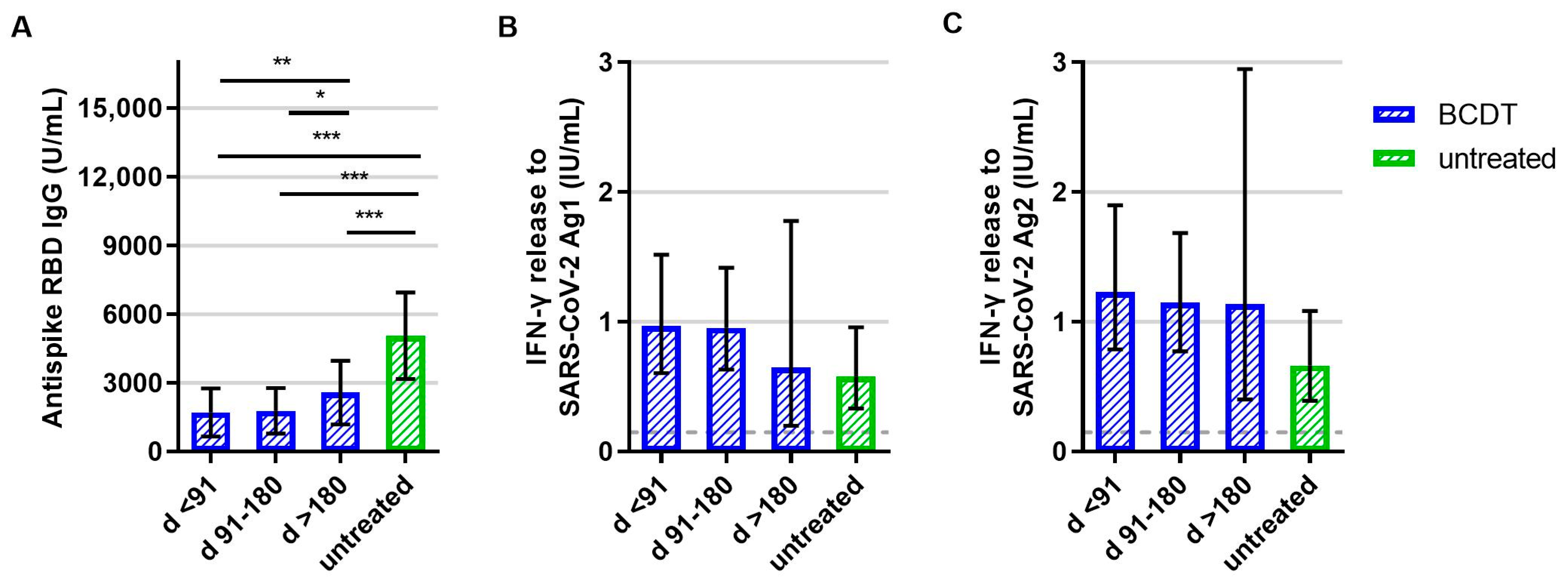
3.5. SARS-CoV-2-Specific T- and B-Cellular Immune Response at Follow Up
3.6. SARS-CoV-2-Specific T- and B-Cellular Immune Response in Patients with Therapy Switch to BCDT
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Multiple Sclerosis International Federation (MSIF). Atlas of MS, 3rd ed.; The Multiple Sclerosis International Federation (MSIF): London, UK, 2020. [Google Scholar]
- Kornek, B.; Leutmezer, F.; Rommer, P.S.; Koblischke, M.; Schneider, L.; Haslacher, H.; Thalhammer, R.; Zimprich, F.; Zulehner, G.; Bsteh, G.; et al. B Cell Depletion and SARS-CoV-2 Vaccine Responses in Neuroimmunologic Patients. Ann. Neurol. 2022, 91, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Milo, R.; Staun-Ram, E.; Karussis, D.; Karni, A.; Hellmann, M.A.; Bar-Haim, E.; Miller, A.; Glass-Marmor, L.; Volkovitz, A.; Dishon, S.; et al. Humoral and Cellular Immune Responses to SARS-CoV-2 MRNA Vaccination in Patients with Multiple Sclerosis: An Israeli Multi-Center Experience Following 3 Vaccine Doses. Front. Immunol. 2022, 13, 868915. [Google Scholar] [CrossRef] [PubMed]
- Apostolidis, S.A.; Kakara, M.; Painter, M.M.; Goel, R.R.; Mathew, D.; Lenzi, K.; Rezk, A.; Patterson, K.R.; Espinoza, D.A.; Kadri, J.C.; et al. Cellular and Humoral Immune Responses Following SARS-CoV-2 MRNA Vaccination in Patients with Multiple Sclerosis on Anti-CD20 Therapy. Nat. Med. 2021, 27, 1990–2001. [Google Scholar] [CrossRef] [PubMed]
- Räuber, S.; Korsen, M.; Huntemann, N.; Rolfes, L.; Müntefering, T.; Dobelmann, V.; Hermann, A.M.; Kölsche, T.; von Wnuck Lipinski, K.; Schroeter, C.B.; et al. Immune Response to SARS-CoV-2 Vaccination in Relation to Peripheral Immune Cell Profiles among Patients with Multiple Sclerosis Receiving Ocrelizumab. J. Neurol. Neurosurg. Psychiatry 2022, 93, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, C.; Aiello, A.; Gasperini, C.; Agrati, C.; Castilletti, C.; Ruggieri, S.; Meschi, S.; Matusali, G.; Colavita, F.; Farroni, C.; et al. Humoral- and T-Cell–Specific Immune Responses to SARS-CoV-2 MRNA Vaccination in Patients with MS Using Different Disease-Modifying Therapies. Neurology 2022, 98, e541–e554. [Google Scholar] [CrossRef] [PubMed]
- Sabatino-Jr, J.J.; Mittl, K.; Rowles, W.M.; McPolin, K.; Rajan, J.V.; Laurie, M.T.; Zamecnik, C.R.; Dandekar, R.; Alvarenga, B.D.; Loudermilk, R.P.; et al. Multiple Sclerosis Therapies Differentially Impact SARS-CoV-2 Vaccine-Induced Antibody and T Cell Immunity and Function. JCI Insight 2022, 7, e156978. [Google Scholar] [CrossRef]
- Meyer-Arndt, L.; Braun, J.; Fauchere, F.; Vanshylla, K.; Loyal, L.; Henze, L.; Kruse, B.; Dingeldey, M.; Jürchott, K.; Mangold, M.; et al. SARS-CoV-2 MRNA Vaccinations Fail to Elicit Humoral and Cellular Immune Responses in Patients with Multiple Sclerosis Receiving Fingolimod. J. Neurol. Neurosurg. Psychiatry 2022, 93, 960–971. [Google Scholar] [CrossRef]
- Gadani, S.P.; Reyes-Mantilla, M.; Jank, L.; Harris, S.; Douglas, M.; Smith, M.D.; Calabresi, P.A.; Mowry, E.M.; Fitzgerald, K.C.; Bhargava, P. Discordant Humoral and T Cell Immune Responses to SARS-CoV-2 Vaccination in People with Multiple Sclerosis on Anti-CD20 Therapy. eBioMedicine 2021, 73, 103636. [Google Scholar] [CrossRef]
- Brill, L.; Rechtman, A.; Zveik, O.; Haham, N.; Oiknine-Djian, E.; Wolf, D.G.; Levin, N.; Raposo, C.; Vaknin-Dembinsky, A. Humoral and T-Cell Response to SARS-CoV-2 Vaccination in Patients with Multiple Sclerosis Treated with Ocrelizumab. JAMA Neurol. 2021, 78, 1510–1514. [Google Scholar] [CrossRef]
- Woopen, C.; Dunsche, M.; Haase, R.; Raposo, C.; Pedotti, R.; Akgün, K.; Ziemssen, T. Timing of SARS-CoV-2 Vaccination Matters in People with Multiple Sclerosis on Pulsed Anti-CD20 Treatment. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9, e200031. [Google Scholar] [CrossRef]
- Alfonso-Dunn, R.; Lin, J.; Kirschner, V.; Lei, J.; Feuer, G.; Malin, M.; Liu, J.; Roche, M.; Sadiq, S.A. Strong T-Cell Activation in Response to COVID-19 Vaccination in Multiple Sclerosis Patients Receiving B-Cell Depleting Therapies. Front. Immunol. 2022, 13, 926318. [Google Scholar] [CrossRef] [PubMed]
- Verstegen, N.J.; Hagen, R.R.; van den Dijssel, J.; Kuijper, L.H.; Kreher, C.; Ashhurst, T.; Kummer, L.Y.; Steenhuis, M.; Duurland, M.; de Jongh, R.; et al. Immune Dynamics in SARS-CoV-2 Experienced Immunosuppressed Rheumatoid Arthritis or Multiple Sclerosis Patients Vaccinated with MRNA-1273. eLife 2022, 11, e77969. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, T.; Otto, C.; Jones, T.C.; Pache, F.; Schindler, P.; Niederschweiberer, M.; Schmidt, F.A.; Drosten, C.; Corman, V.M.; Ruprecht, K. Preserved T Cell Responses to SARS-CoV-2 in Anti-CD20 Treated Multiple Sclerosis. Mult. Scler. J. 2022, 28, 1041–1050. [Google Scholar] [CrossRef] [PubMed]
- Pitzalis, M.; Idda, M.L.; Lodde, V.; Loizedda, A.; Lobina, M.; Zoledziewska, M.; Virdis, F.; Delogu, G.; Pirinu, F.; Marini, M.G.; et al. Effect of Different Disease-Modifying Therapies on Humoral Response to BNT162b2 Vaccine in Sardinian Multiple Sclerosis Patients. Front. Immunol. 2021, 12, 781843. [Google Scholar] [CrossRef]
- Cabeza, V.P.; Kummer, L.Y.; Wieske, L.; Hagen, R.R.; Duurland, M.; Konijn, V.A.; van Dam, K.P.; Stalman, E.W.; van de Sandt, C.E.; Boekel, L.; et al. Longitudinal T-Cell Responses after a Third SARS-CoV-2 Vaccination in Patients with Multiple Sclerosis on Ocrelizumab or Fingolimod. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9, e1178. [Google Scholar] [CrossRef]
- Jaber, A.; Patel, M.; Sylvester, A.; Yarussi, M.; Kalina, J.T.; Mendoza, J.P.; Avila, R.L.; Tremblay, M.A. COVID-19 Vaccine Response in People with Multiple Sclerosis Treated with Dimethyl Fumarate, Diroximel Fumarate, Natalizumab, Ocrelizumab, or Interferon Beta Therapy. Neurol. Ther. 2023, 12, 687–700. [Google Scholar] [CrossRef]
- Brill, L.; Raposo, C.; Rechtman, A.; Zveik, O.; Levin, N.; Oiknine-Djian, E.; Wolf, D.G.; Vaknin-Dembinsky, A. Severe Acute Respiratory Syndrome Coronavirus 2 Third Vaccine Immune Response in Multiple Sclerosis Patients Treated with Ocrelizumab. Ann. Neurol. 2022, 91, 796–800. [Google Scholar] [CrossRef]
- Capuano, R.; Altieri, M.; Conte, M.; Bisecco, A.; d’Ambrosio, A.; Donnarumma, G.; Grimaldi, E.; Coppola, N.; Medici, N.; Galdiero, M.; et al. Humoral Response and Safety of the Third Booster Dose of BNT162b2 MRNA COVID-19 Vaccine in Patients with Multiple Sclerosis Treated with Ocrelizumab or Fingolimod. J. Neurol. 2022, 269, 6185–6192. [Google Scholar] [CrossRef]
- Capuano, R.; Bisecco, A.; Conte, M.; Donnarumma, G.; Altieri, M.; Grimaldi, E.; Franci, G.; Chianese, A.; Galdiero, M.; Coppola, N.; et al. Six-Month Humoral Response to MRNA SARS-CoV-2 Vaccination in Patients with Multiple Sclerosis Treated with Ocrelizumab and Fingolimod. Mult. Scler. Relat. Disord. 2022, 60, 103724. [Google Scholar] [CrossRef]
- Disanto, G.; Galante, A.; Cantu’, M.; Sacco, R.; Mele, F.; Eisler, J.J.; Keller, F.; Bernasconi, E.; Sallusto, F.; Zecca, C.; et al. Longitudinal Postvaccine SARS-CoV-2 Immunoglobulin G Titers, Memory B-Cell Responses, and Risk of COVID-19 in Multiple Sclerosis Over 1 Year. Neurol.—Neuroimmunol. Neuroinflamm. 2023, 10, e200043. [Google Scholar] [CrossRef]
- Bajwa, H.M.; Novak, F.; Nilsson, A.C.; Nielsen, C.; Holm, D.K.; Østergaard, K.; Witt, A.H.; Byg, K.-E.; Johansen, I.S.; Mittl, K.; et al. Persistently Reduced Humoral and Sustained Cellular Immune Response from First to Third SARS-CoV-2 MRNA Vaccination in Anti-CD20-Treated Multiple Sclerosis Patients. Mult. Scler. Relat. Disord. 2022, 60, 103729. [Google Scholar] [CrossRef]
- Maniscalco, G.T.; Ferrara, A.L.; Liotti, A.; Manzo, V.; Battista, M.E.D.; Salvatore, S.; Graziano, D.; Viola, A.; Amato, G.; Moreggia, O.; et al. Long Term Persistence of SARS-CoV-2 Humoral Response in Multiple Sclerosis Subjects. Mult. Scler. Relat. Disord. 2022, 62, 103800. [Google Scholar] [CrossRef] [PubMed]
- Maglione, A.; Morra, M.; Meroni, R.; Matta, M.; Clerico, M.; Rolla, S. Humoral Response after the Booster Dose of Anti-SARS-CoV-2 Vaccine in Multiple Sclerosis Patients Treated with High-Efficacy Therapies. Mult. Scler. Relat. Disord. 2022, 61, 103776. [Google Scholar] [CrossRef] [PubMed]
- Idda, M.L.; Pitzalis, M.; Lodde, V.; Loizedda, A.; Frau, J.; Lobina, M.; Zoledziewska, M.; Virdis, F.; Delogu, G.; Marini, M.G.; et al. Cross-Sectional Analysis of the Humoral Response after SARS-CoV-2 Vaccination in Sardinian Multiple Sclerosis Patients, a Follow-Up Study. Front. Immunol. 2022, 13, 946356. [Google Scholar] [CrossRef]
- Maniscalco, G.T.; Liotti, A.; Ferrara, A.L.; Prestipino, E.; Salvatore, S.; Battista, M.E.D.; Moreggia, O.; Cesare, D.D.G.; Vastano, R.; Belardo, M.; et al. Humoral Efficacy of the Third SARS-CoV-2 Vaccine Dose in Multiple Sclerosis Subjects Undergoing Different Disease-Modifying Therapies. Mult. Scler. Relat. Disord. 2022, 68, 104371. [Google Scholar] [CrossRef] [PubMed]
- König, M.; Torgauten, H.M.; Tran, T.T.; Holmøy, T.; Vaage, J.T.; Lund-Johansen, F.; Nygaard, G.O. Immunogenicity and Safety of a Third SARS-CoV-2 Vaccine Dose in Patients with Multiple Sclerosis and Weak Immune Response after COVID-19 Vaccination. JAMA Neurol. 2022, 79, 307–309. [Google Scholar] [CrossRef]
- Madelon, N.; Heikkilä, N.; Royo, I.S.; Fontannaz, P.; Breville, G.; Lauper, K.; Goldstein, R.; Grifoni, A.; Sette, A.; Siegrist, C.-A.; et al. Omicron-Specific Cytotoxic T-Cell Responses after a Third Dose of MRNA COVID-19 Vaccine among Patients with Multiple Sclerosis Treated with Ocrelizumab. JAMA Neurol. 2022, 79, 399–404. [Google Scholar] [CrossRef]
- Sabatino, J.J.; Mittl, K.; Rowles, W.; Zamecnik, C.R.; Loudermilk, R.P.; Gerungan, C.; Spencer, C.M.; Sagan, S.A.; Alexander, J.; Mcpolin, K.; et al. Longitudinal Adaptive Immune Responses Following Sequential SARS-CoV-2 Vaccinations in MS Patients on Anti-CD20 Therapies and Sphingosine-1-Phosphate Receptor Modulators. Mult. Scler. Relat. Disord. 2023, 70, 104484. [Google Scholar] [CrossRef]
- Torres, P.; Sancho-Saldaña, A.; Sánchez, A.G.; Peralta, S.; Solana, M.J.; Bakkioui, S.; González-Mingot, C.; Quibus, L.; Ruiz-Fernández, E.; Pedro-Murillo, E.S.; et al. A Prospective Study of Cellular Immune Response to Booster COVID-19 Vaccination in Multiple Sclerosis Patients Treated with a Broad Spectrum of Disease-Modifying Therapies. J. Neurol. 2023, 270, 2380–2391. [Google Scholar] [CrossRef]
- Jochum, S.; Kirste, I.; Hortsch, S.; Grunert, V.P.; Legault, H.; Eichenlaub, U.; Kashlan, B.; Pajon, R. Clinical Utility of Elecsys Anti-SARS-CoV-2 S Assay in COVID-19 Vaccination: An Exploratory Analysis of the MRNA-1273 Phase 1 Trial. Front. Immunol. 2022, 12, 798117. [Google Scholar] [CrossRef]
- Räuber, S.; Willison, A.; Korsen, M.; Kölsche, T.; Golombeck, K.S.; Plaack, B.; Schüller, J.; Huntemann, N.; Rolfes, L.; Schroeter, C.B.; et al. Vaccine-Based Clinical Protection against SARS-CoV-2 Infection and the Humoral Immune Response: A 1-Year Follow-Up Study of Patients with Multiple Sclerosis Receiving Ocrelizumab. Front. Immunol. 2022, 13, 1037214. [Google Scholar] [CrossRef]
- Kister, I.; Curtin, R.; Pei, J.; Perdomo, K.; Bacon, T.E.; Voloshyna, I.; Kim, J.; Tardio, E.; Velmurugu, Y.; Nyovanie, S.; et al. Hybrid and Vaccine-induced Immunity against SAR-CoV-2 in MS Patients on Different Disease-modifying Therapies. Ann. Clin. Transl. Neurol. 2022, 9, 1643–1659. [Google Scholar] [CrossRef] [PubMed]
- Sette, A.; Crotty, S. Immunological Memory to SARS-CoV-2 Infection and COVID-19 Vaccines. Immunol. Rev. 2022, 310, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Stoll, S.; Desai, S.; Levit, E. A Retrospective Evaluation of Seroconversion after COVID-19 during the Early Omicron Wave in Fully Vaccinated Multiple Sclerosis Patients Receiving Anti-CD20 Therapies. Mult. Scler. Relat. Disord. 2023, 71, 104574. [Google Scholar] [CrossRef]
- van Dam, K.P.J.; Hogenboom, L.; Stalman, E.W.; Kummer, L.Y.L.; Steenhuis, M.; Keijser, J.B.D.; ten Brinke, A.; van Ham, S.M.; Kuijpers, T.W.; Rispens, T.; et al. Longitudinal SARS-CoV-2 Humoral Response in MS Patients with and without SARS-CoV-2 Infection Prior to Vaccination. Front. Neurol. 2022, 13, 1032830. [Google Scholar] [CrossRef] [PubMed]
- van Kempen, Z.L.E.; Stalman, E.W.; Steenhuis, M.; Kummer, L.Y.L.; van Dam, K.P.J.; Wilbrink, M.F.; Brinke, A.T.; van Ham, S.M.; Kuijpers, T.; Rispens, T.; et al. SARS-CoV-2 Omicron Breakthrough Infections in Patients with Multiple Sclerosis. J. Neurol. Neurosurg. Psychiatry 2022, 94, 280–283. [Google Scholar] [CrossRef]
- Wakui, M.; Uwamino, Y.; Yatabe, Y.; Nakagawa, T.; Sakai, A.; Kurafuji, T.; Shibata, A.; Tomita, Y.; Noguchi, M.; Tanabe, A.; et al. Assessing Anti-SARS-CoV-2 Cellular Immunity in 571 Vaccines by Using an IFN-γ Release Assay. Eur. J. Immunol. 2022, 52, 1961–1971. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and Cellular Immunity to SARS-CoV-2 Vaccination in Renal Transplant versus Dialysis Patients: A Prospective, Multicenter Observational Study Using MRNA-1273 or BNT162b2 MRNA Vaccine. Lancet Reg. Health—Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Tan, A.T.; Lim, J.M.E.; Bert, N.L.; Kunasegaran, K.; Chia, A.; Qui, M.D.C.; Tan, N.; Chia, W.N.; de Alwis, R.; Ying, D.; et al. Rapid Measurement of SARS-CoV-2 Spike T Cells in Whole Blood from Vaccinated and Naturally Infected Individuals. J. Clin. Investig. 2021, 131, e152379. [Google Scholar] [CrossRef]
- de Vries, R.D.; van der Heiden, M.; Geers, D.; Imhof, C.; van Baarle, D.; Collaborators, R.-I. Difference in Sensitivity between SARS-CoV-2–Specific T Cell Assays in Patients with Underlying Conditions. J. Clin. Investig. 2021, 131, e155499. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analysis after | Primary Vaccination | Booster Vaccination |
|---|---|---|
| n (%) | 368 (100) | 305 (100) |
| Age years, mean (SD) | 46.4 (11.9) | 47.2 (12.2) |
| Female patients n (%) | 257 (69.8) | 210 (68.9) |
| Time between primary vaccination and blood sampling, days, mean (SD) | 127.3 (64.09) | 271.9 (48.03) |
| Time between booster vaccination and blood sampling, days, mean (SD) | - | 52.4 (33.63) |
| Treatment duration until blood sampling, days, mean (SD) | 915.8 (772.4) | 831.7 (503.87) |
| Treatment | ||
| Ocrelizumab treated, n (%) | 285 (77.4) | 248 (81.3) |
| Rituximab treated, n (%) | 2 (0.5) | 3 (1.0) |
| Ofatumumab treated, n (%) | 2 (0.5) | 2 (0.7) |
| Untreated n (%) | 79 (21.5) | 52 (17.0) |
| Disease course | ||
| RRMS, n (%) | 286 (77.7) | 233 (76.4) |
| SPMS, n (%) | 35 (9.5) | 35 (11.5) |
| PPMS, n (%) | 47 (12.8) | 37 (12.1) |
| Vaccines | ||
| BNT162b2 vaccine, n (%) | 309 (84.0) | 260 (85.2) |
| mRNA-1273 vaccine, n (%) | 23 (6.3) | 19 (6.2) |
| AZD1222 vaccine, n (%) | 25 (6.8) | 24 (7.9) |
| Ad26.COV2.S vaccine, n (%) | 11 (3.0) | 2 (0.7) |
| BCDT | Untreated | |
|---|---|---|
| complete primary vaccination (p = 0.193) | ||
| COVID-19 infection, n (%) | 35 (12.1) | 14 (18.2) |
| no COVID-19 infection, n (%) | 254 (87.9) | 63 (81.8) |
| booster vaccination (p = 0.999) | ||
| COVID-19 infection, n (%) | 43 (17.0) | 9 (17.3) |
| no COVID-19 infection, n (%) | 210 (83.0) | 43 (82.7) |
| After Primary Vaccination | After Booster Vaccination | |
|---|---|---|
| Primary vaccination before BCDT | ||
| Antispike RBD IgG (U/mL) (mean [95% CI]) | 550.8 [175.74–925.90] | 3035.1 [−457.29–6527.49] |
| IFN-g release to SARS-CoV-2 Ag1 (IU/mL) (mean [95% CI]) | 0.28 [−0.01–0.56] | 0.26 [0.04–0.49] |
| IFN-g release to SARS-CoV-2 Ag2 (IU/mL) (mean [95% CI]) | 0.33 [−0.12–0.78] | 0.47 [−0.13–1.07]; |
| Primary vaccination on BCDT | ||
| Antispike RBD IgG (U/mL) (mean [95% CI]) | 95.3 [30.85–159.73] | 1139.5 [524.04–1754.96] |
| IFN-g release to SARS-CoV-2 Ag1 (IU/mL) (mean [95% CI]) | 0.64 [0.50–0.82] | 0.84 [0.62–1.12] |
| IFN-g release to SARS-CoV-2 Ag2 (IU/mL) (mean [95% CI]) | 0.97 [0.75–1.24] | 1.39 [1.08–1.78] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woopen, C.; Dunsche, M.; Al Rahbani, G.K.; Dillenseger, A.; Atta, Y.; Haase, R.; Raposo, C.; Pedotti, R.; Ziemssen, T.; Akgün, K. Long-Term Immune Response Profiles to SARS-CoV-2 Vaccination and Infection in People with Multiple Sclerosis on Anti-CD20 Therapy. Vaccines 2023, 11, 1464. https://doi.org/10.3390/vaccines11091464
Woopen C, Dunsche M, Al Rahbani GK, Dillenseger A, Atta Y, Haase R, Raposo C, Pedotti R, Ziemssen T, Akgün K. Long-Term Immune Response Profiles to SARS-CoV-2 Vaccination and Infection in People with Multiple Sclerosis on Anti-CD20 Therapy. Vaccines. 2023; 11(9):1464. https://doi.org/10.3390/vaccines11091464
Chicago/Turabian StyleWoopen, Christina, Marie Dunsche, Georges Katoul Al Rahbani, Anja Dillenseger, Yassin Atta, Rocco Haase, Catarina Raposo, Rosetta Pedotti, Tjalf Ziemssen, and Katja Akgün. 2023. "Long-Term Immune Response Profiles to SARS-CoV-2 Vaccination and Infection in People with Multiple Sclerosis on Anti-CD20 Therapy" Vaccines 11, no. 9: 1464. https://doi.org/10.3390/vaccines11091464
APA StyleWoopen, C., Dunsche, M., Al Rahbani, G. K., Dillenseger, A., Atta, Y., Haase, R., Raposo, C., Pedotti, R., Ziemssen, T., & Akgün, K. (2023). Long-Term Immune Response Profiles to SARS-CoV-2 Vaccination and Infection in People with Multiple Sclerosis on Anti-CD20 Therapy. Vaccines, 11(9), 1464. https://doi.org/10.3390/vaccines11091464