
Effect of Influenza Vaccination on Rate of Influenza Virus Infection in Chinese Military Personnel, 2015–2016: A Cluster Randomized Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Primary and Secondary Outcomes
2.3. Vaccines
2.4. Procedures
2.4.1. Randomization of Clusters
2.4.2. Administration of Study Vaccine
2.4.3. Follow-Up of Adverse Events
2.4.4. Active Surveillance for Influenza-like Illness (ILI) Cases
2.4.5. Laboratory Methods
2.5. Study Oversight
2.6. Statistical Analysis
3. Results
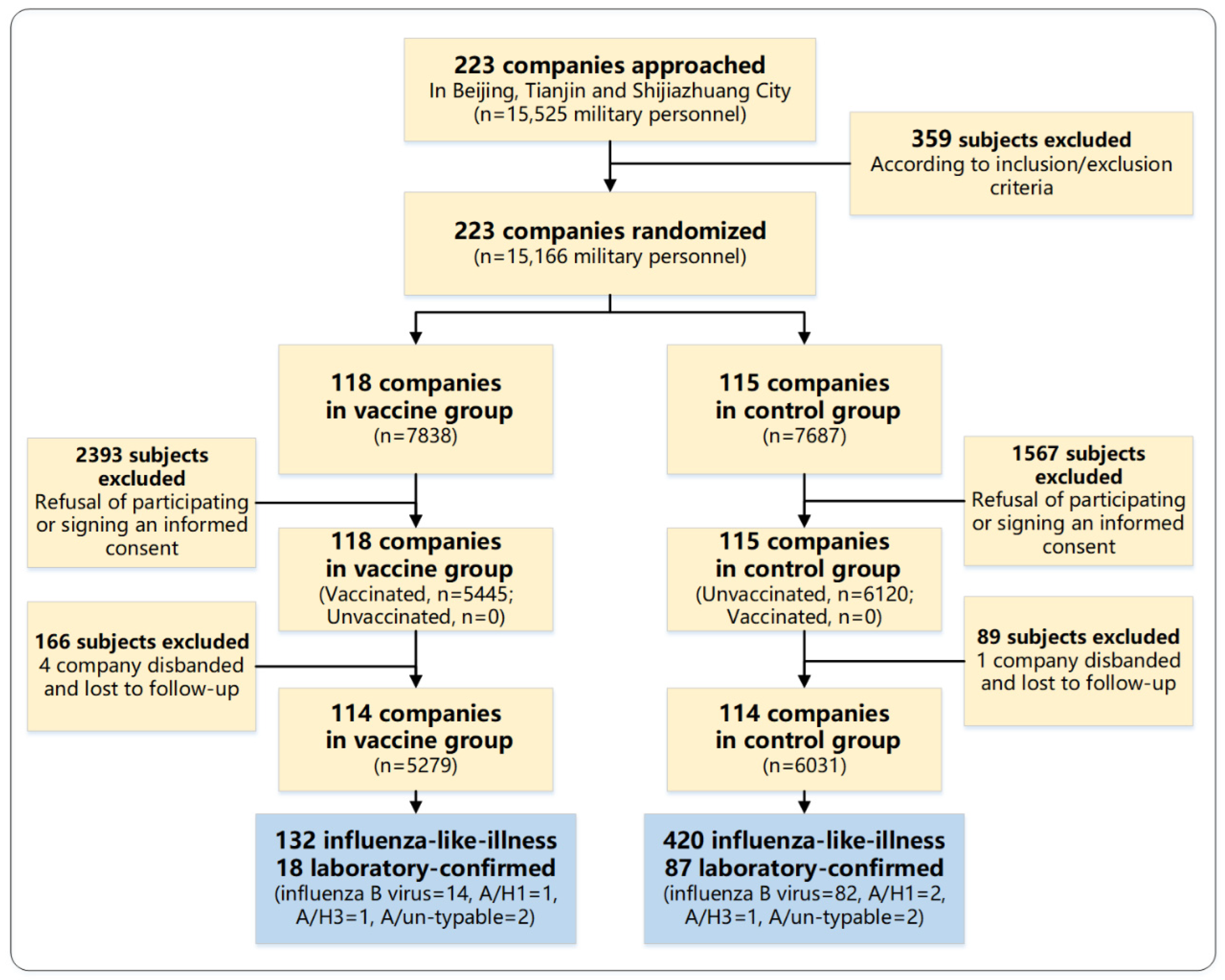
3.1. Characteristics of Participants
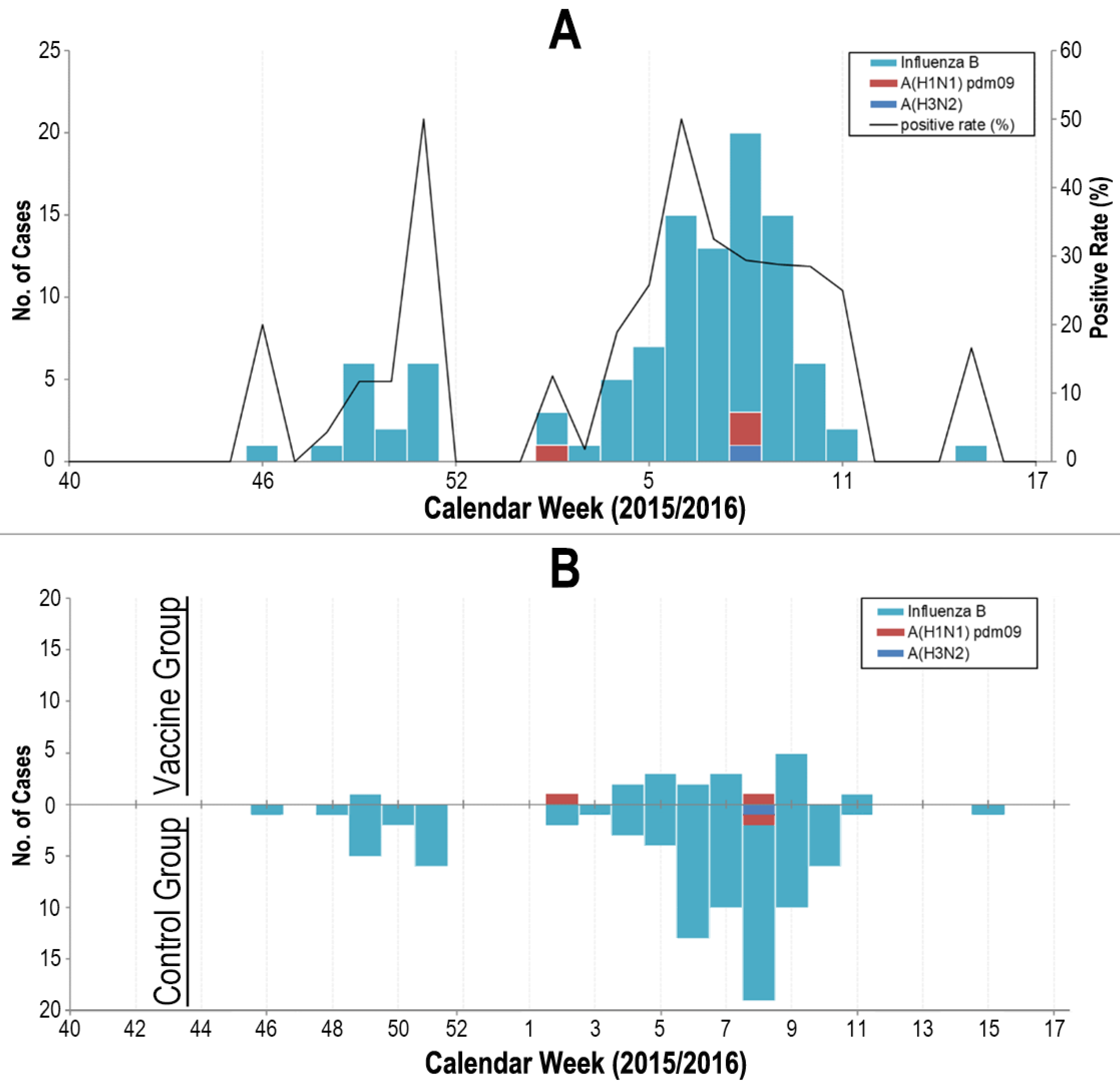
3.2. Total Protection
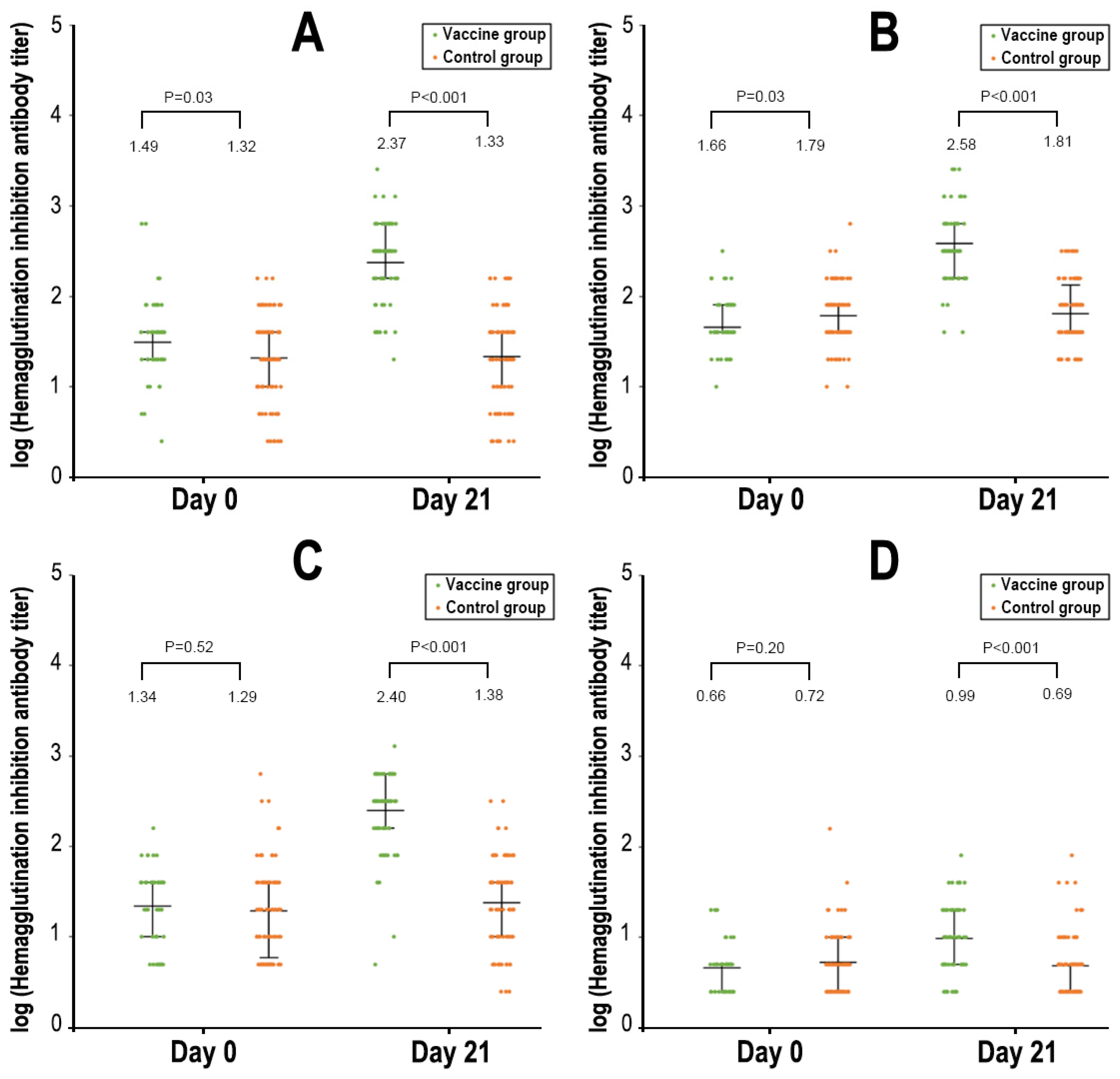
3.3. Serologic Responses
3.4. Safety and Reactogenicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vaccines against influenza: WHO position paper—May 2022. Wkly. Epidemiol. Rec. 2022, 97, 185–208. [Google Scholar]
- Li, L.; Liu, Y.; Wu, P.; Peng, Z.; Wang, X.; Chen, T.; Wong, J.Y.T.; Yang, J.; Bond, H.S.; Wang, L.; et al. Influenza-associated excess respiratory mortality in China, 2010–15: A population-based study. Lancet Public Health 2019, 4, e473–e481. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, T.; Rivetti, A.; Di Pietrantonj, C.; Demicheli, V. Vaccines for preventing influenza in healthy children. Cochrane Database Syst. Rev. 2018, 2, CD004879. [Google Scholar] [CrossRef] [PubMed]
- Demicheli, V.; Jefferson, T.; Di Pietrantonj, C.; Ferroni, E.; Thorning, S.; Thomas, R.E.; Rivetti, A. Vaccines for preventing influenza in the elderly. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Demicheli, V.; Jefferson, T.; Ferroni, E.; Rivetti, A.; Di Pietrantonj, C. Vaccines for preventing influenza in healthy adults. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Paules, C.; Subbarao, K. Influenza. Lancet 2017, 390, 697–708. [Google Scholar] [CrossRef]
- Grohskopf, L.A.; Blanton, L.H.; Ferdinands, J.M.; Chung, J.R.; Broder, K.R.; Talbot, H.K.; Morgan, R.L.; Fry, A.M. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022-23 Influenza Season. MMWR Recomm. Rep. 2022, 71, 1–28. [Google Scholar] [CrossRef]
- Sencer, D.J.; Millar, J.D. Reflections on the 1976 swine flu vaccination program. Emerg. Infect. Dis. 2006, 12, 29–33. [Google Scholar] [CrossRef]
- Grabenstein, J.D.; Pittman, P.R.; Greenwood, J.T.; Engler, R.J. Immunization to protect the US Armed Forces: Heritage, current practice, and prospects. Epidemiol. Rev. 2006, 28, 3–26. [Google Scholar] [CrossRef]
- Wang, Z.; Tobler, S.; Roayaei, J.; Eick, A. Live attenuated or inactivated influenza vaccines and medical encounters for respiratory illnesses among US military personnel. JAMA 2009, 301, 945–953. [Google Scholar] [CrossRef] [PubMed]
- D’Amelio, R.; Biselli, R.; Calì, G.; Peragallo, M.S. Vaccination policies in the military: An insight on influenza. Vaccine 2002, 20, B36–B39. [Google Scholar] [CrossRef] [PubMed]
- D’Amelio, R.; Biselli, R.; Natalicchio, S.; Lista, F.; Peragallo, M.S. Vaccination programmes in the Italian military. Vaccine 2003, 21, 3530–3533. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.Z.; Yang, P.; Zhang, T.; Yang, J.; Fu, C.X.; Qin, Y.; Zhang, Y.; Ma, C.N.; Liu, Z.Q.; Wang, Q.Y.; et al. Technical guidelines for the application of seasonal influenza vaccine in China (2014–2015). Chin. J. Epidemiol. 2014, 35, 1295–1319. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, J.Y.; Wang, X.; Chen, J.T.; Xia, M.; Hu, W.; Zou, Y.; Yin, W.D. Review of 10 years of clinical experience with Chinese domestic trivalent influenza vaccine Anflu(R). Hum. Vaccines Immunother. 2014, 10, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.P.; LI, R.C.; Chen, J.T.; Liu, Y.; Nong, Y.; Luo, D.; Gao, H.; Song, N.S.; Wang, X.; Fang, H.H. Research on Safety and Immunogenicity of Trivalent Split Influenza Vaccine. Chin. J. Vaccines Immun. 2006, 11, 343–347. [Google Scholar]
- Luo, F.J.; Yang, L.Q.; Ai, X.; Bai, Y.H.; Wu, J.; Li, S.M.; Zhang, Z.; Lu, M.; Li, L.; Wang, Z.Y.; et al. Immunogenicity and safety of three 2010-2011 seasonal trivalent influenza vaccines in Chinese toddlers, children and older adults: A double-blind and randomized trial. Hum. Vaccines Immunother. 2013, 9, 1725–1734. [Google Scholar] [CrossRef]
- Wu, J.; Zhong, X.; Li, C.K.; Zhou, J.F.; Lu, M.; Huang, K.Y.; Dong, M.; Liu, Y.; Luo, F.J.; Du, N.; et al. Optimal vaccination strategies for 2009 pandemic H1N1 and seasonal influenza vaccines in humans. Vaccine 2011, 29, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.P.; Li, W.; Liang, X.F.; Liu, Y.; Huang, X.C.; Li, C.G.; Li, R.C.; Wang, J.Z.; Wang, H.Q.; Yin, W.D. Immunogenicity and safety of a 2009 pandemic influenza A (H1N1) monovalent vaccine in Chinese infants aged 6-35 months: A randomized, double-blind, controlled phase I clinical trial. Influenza Other Respir. Viruses 2013, 7, 1297–1307. [Google Scholar] [CrossRef]
- Gao, D.; Yang, H.; Deng, B.; Yin, G.; Song, W.; Zhang, H.; Li, Y. Safety and immunogenicity of 3 seasonal trivalent influenza vaccines in the Chinese military. Hum. Vaccines Immunother. 2016, 12, 2634–2639. [Google Scholar] [CrossRef] [PubMed]
- Chinese Center for Disease Control and Prevention. Study Protocol of National Influenza Surveillance Program (2017); Chinese Center for Disease Control and Prevention: Beijing, China, 2017; Available online: https://www.chinacdc.cn/jkzt/crb/bl/lxxgm/jszl_2251/201810/t20181010_194587.html (accessed on 20 July 2023).
- Office of the Ministry of Health. Guidelines for the Diagnosis and Treatment of Influenza (2011 Edition); Ministry of Health, People’s Republic of China: Beiing, China, 2011. [Google Scholar]
- World Health Organization. Recommended Composition of Influenza Virus Vaccines for Use in the 2015–2016 Northern Hemisphere Influenza Season; World Health Organization: Geneva, Switzerland, 2015.
- Yu, H.; Alonso, W.J.; Feng, L.; Tan, Y.; Shu, Y.; Yang, W.; Viboud, C. Characterization of regional influenza seasonality patterns in China and implications for vaccination strategies: Spatio-temporal modeling of surveillance data. PLoS Med. 2013, 10, e1001552. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Yang, P.; Zhang, T.; Yang, J.; Fu, C.; Qin, Y.; Zhang, Y.; Ma, C.; Liu, Z.; Wang, Q.; et al. Technical guidelines for the application of seasonal influenza vaccine in China (2014–2015). Hum. Vaccine Immunother. 2015, 11, 2077–2101. [Google Scholar] [CrossRef] [PubMed]
- National Medical Products Administration. Guidelines for Grading Standards of Adverse Events in Clinical Trials of Preventive Vaccine; National Medical Products Administration: Beijing, China, 2019. Available online: https://www.nmpa.gov.cn/xxgk/ggtg/qtggtg/20191231111901460.html (accessed on 20 July 2023).
- Chinese National Influenza Center. National Technical Guidelines for Surveillance of Influenza (2011 Version); Chinese Center for Diseases Control and Prevention: Beijing, China, 2011; Available online: https://ivdc.chinacdc.cn/cnic/zyzx/jcfa/201605/t20160520_129702.htm (accessed on 20 July 2023).
- World Health Organization. Manual for the Laboratory Diagnosis and Virological Surveillance of Influenza; World Health Organization: Geneva, Switzerland, 2011.
- National Medical Products Adninistration. Good Clinical Practice for Drugs; National Medical Products Adninistration: Beijing, China, 2020. Available online: https://www.nmpa.gov.cn/xxgk/fgwj/xzhgfxwj/20200426162401243.html (accessed on 20 July 2023).
- National Medical Products Adninistration. Good Clinical Practice for Vaccines: Guideline and Principles; National Medical Products Administration: Beijing, China, 2013. Available online: https://www.nmpa.gov.cn/xxgk/fgwj/gzwj/gzwjyp/20131031120001201.html (accessed on 20 July 2023).
- Treanor, J.J.; El Sahly, H.; King, J.; Graham, I.; Izikson, R.; Kohberger, R.; Patriarca, P.; Cox, M. Protective efficacy of a trivalent recombinant hemagglutinin protein vaccine (FluBlok(R)) against influenza in healthy adults: A randomized, placebo-controlled trial. Vaccine 2011, 29, 7733–7739. [Google Scholar] [CrossRef]
- Dermont, M.A.; Elmer, T. Influenza syndromic surveillance and vaccine efficacy in the UK Armed Forces, 2017–2018. J. R. Army Med. Corps 2019, 165, 395–399. [Google Scholar] [CrossRef] [PubMed]
- DiazGranados, C.A.; Dunning, A.J.; Robertson, C.A.; Talbot, H.K.; Landolfi, V.; Greenberg, D.P. Effect of Previous-Year Vaccination on the Efficacy, Immunogenicity, and Safety of High-Dose Inactivated Influenza Vaccine in Older Adults. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 62, 1092–1099. [Google Scholar] [CrossRef]
- Chinese National Influenza Center. Influenza Activity Weekly Report, China; Chinese Center for Diseases Control and Prevention: Beijing, China, 2016; Available online: https://ivdc.chinacdc.cn/cnic/zyzx/lgzb/ (accessed on 20 July 2023).
- European Committee for Medicinal Products for Human Use. Note for Guidance on Harmonization of Requirements for Influenza Vaccines (CPMP/ BWP/214/96); The European Medicines Agency: Amsterdam, The Netherlands, 1997. Available online: http://www.ema.europa.eu/pdfs/human/bwp/021496en.pdf (accessed on 20 July 2023).
- Food and Drug Administration. FDA Guidance for Industry Clinical Data Needed to Support the Licensure of Seasonal Inactivated Influenza Vaccines. 2007. Available online: https://www.gmp-compliance.org/files/guidemgr/trifluvac.pdf (accessed on 20 July 2023).
- Koutsakos, M.; Wheatley, A.K.; Laurie, K.; Kent, S.J.; Rockman, S. Influenza lineage extinction during the COVID-19 pandemic? Nat. Rev. Microbiol. 2021, 19, 741–742. [Google Scholar] [CrossRef] [PubMed]
- Loeb, M.; Russell, M.L.; Moss, L.; Fonseca, K.; Fox, J.; Earn, D.J.; Aoki, F.; Horsman, G.; Van Caeseele, P.; Chokani, K.; et al. Effect of influenza vaccination of children on infection rates in Hutterite communities: A randomized trial. JAMA 2010, 303, 943–950. [Google Scholar] [CrossRef]
- Clemens, J.; Shin, S.; Ali, M. New approaches to the assessment of vaccine herd protection in clinical trials. Lancet Infect. Dis. 2011, 11, 482–487. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Influenza Vaccine Group 114 Clusters (n = 5279) | Control Group 114 Clusters (n = 6031) |
|---|---|---|
| Individual level | ||
| Age, median (IQR), yr | 21 (19–24) | 21 (19–24) |
| Age groups, y, No. (%) | ||
| 18–22 | 3600 (68.2) | 3966 (65.8) |
| 23–30 | 1506 (28.5) | 1844 (30.6) |
| 31–38 | 173 (3.3) | 221 (3.7) |
| Female sex, No. (%) | 43 (0.8) | 22 (0.4) |
| Ethnicity, No. (%) | ||
| Han | 5069 (96.0) | 5795 (96.1) |
| Other | 210 (4.0) | 236 (3.9) |
| Educational attainment, No. (%) | ||
| Primary school or illiterate | 748 (14.2) | 738 (12.2) |
| High school | 3236 (61.3) | 3785 (62.8) |
| College level | 852 (16.1) | 1030 (17.1) |
| Undergraduate and above | 443 (8.4) | 478 (7.9) |
| Cluster level, median (IQR) | ||
| All persons—no./cluster | 60 (43–87) | 63 (36–89) |
| Enrolled participants—No./cluster | 36 (20–65) | 43 (27–83) |
| Vaccinated subjects—No./cluster | 36 (20–65) | 0 (0–0) |
| Variable | Vaccine Group (n = 5279) | Control Group (n = 6031) | Protective Effectiveness of Influenza Vaccination (95% CI) | ||
|---|---|---|---|---|---|
| No. of Subjects | Incidence, % | No. of Subjects | Incidence, % | ||
| Influenza-like illness | 132 | 2.50 (2.10–2.96) | 420 | 6.96 (6.33–7.64) | 64.1 (56.2 to 70.6) |
| Laboratory-confirmed influenza | 18 | 0.34 (0.20–0.54) | 87 | 1.44 (1.16–1.78) | 76.4 (60.7 to 85.8) |
| Influenza B virus | 14 | 0.27 (0.15–0.44) | 82 | 1.36 (1.08–1.68) | 80.5 (65.6 to 88.9) |
| Influenza A virus | 4 | 0.08 (0.02–0.19) | 5 | 0.08 (0.03–0.19) | 8.6 (−241 to 75.5) |
| Influenza A subtype H1 | 1 | 0.02 (0.00–0.11) | 2 | 0.03 (0.00–0.12) | 42.9 (−530 to 94.8) |
| Influenza A subtype H3 | 1 | 0.02 (0.00–0.11) | 1 | 0.02 (0.00–0.09) | −14.2 (−1727 to 92.9) |
| Influenza A un-typable | 2 | 0.04 (0.00–0.14) | 2 | 0.03 (0.00–0.12) | −14.2 (−711 to 83.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Yu, J.; Li, Q.; Yu, D.; Song, W.; Liu, Q.; Gao, D.; Chen, Q.; Zhang, H.; Huo, L.; et al. Effect of Influenza Vaccination on Rate of Influenza Virus Infection in Chinese Military Personnel, 2015–2016: A Cluster Randomized Trial. Vaccines 2023, 11, 1439. https://doi.org/10.3390/vaccines11091439
Li Y, Yu J, Li Q, Yu D, Song W, Liu Q, Gao D, Chen Q, Zhang H, Huo L, et al. Effect of Influenza Vaccination on Rate of Influenza Virus Infection in Chinese Military Personnel, 2015–2016: A Cluster Randomized Trial. Vaccines. 2023; 11(9):1439. https://doi.org/10.3390/vaccines11091439
Chicago/Turabian StyleLi, Yapin, Jianxing Yu, Qingfeng Li, Dan Yu, Wenjing Song, Qi Liu, Dongqi Gao, Qiulan Chen, Haiyang Zhang, Liqun Huo, and et al. 2023. "Effect of Influenza Vaccination on Rate of Influenza Virus Infection in Chinese Military Personnel, 2015–2016: A Cluster Randomized Trial" Vaccines 11, no. 9: 1439. https://doi.org/10.3390/vaccines11091439
APA StyleLi, Y., Yu, J., Li, Q., Yu, D., Song, W., Liu, Q., Gao, D., Chen, Q., Zhang, H., Huo, L., Wang, J., Wang, J., Yang, H., & Zeng, G. (2023). Effect of Influenza Vaccination on Rate of Influenza Virus Infection in Chinese Military Personnel, 2015–2016: A Cluster Randomized Trial. Vaccines, 11(9), 1439. https://doi.org/10.3390/vaccines11091439