
Population-Level Risk Factors Related to Measles Case Fatality: A Conceptual Framework Based on Expert Consultation and Literature Review

 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Expert Consultation
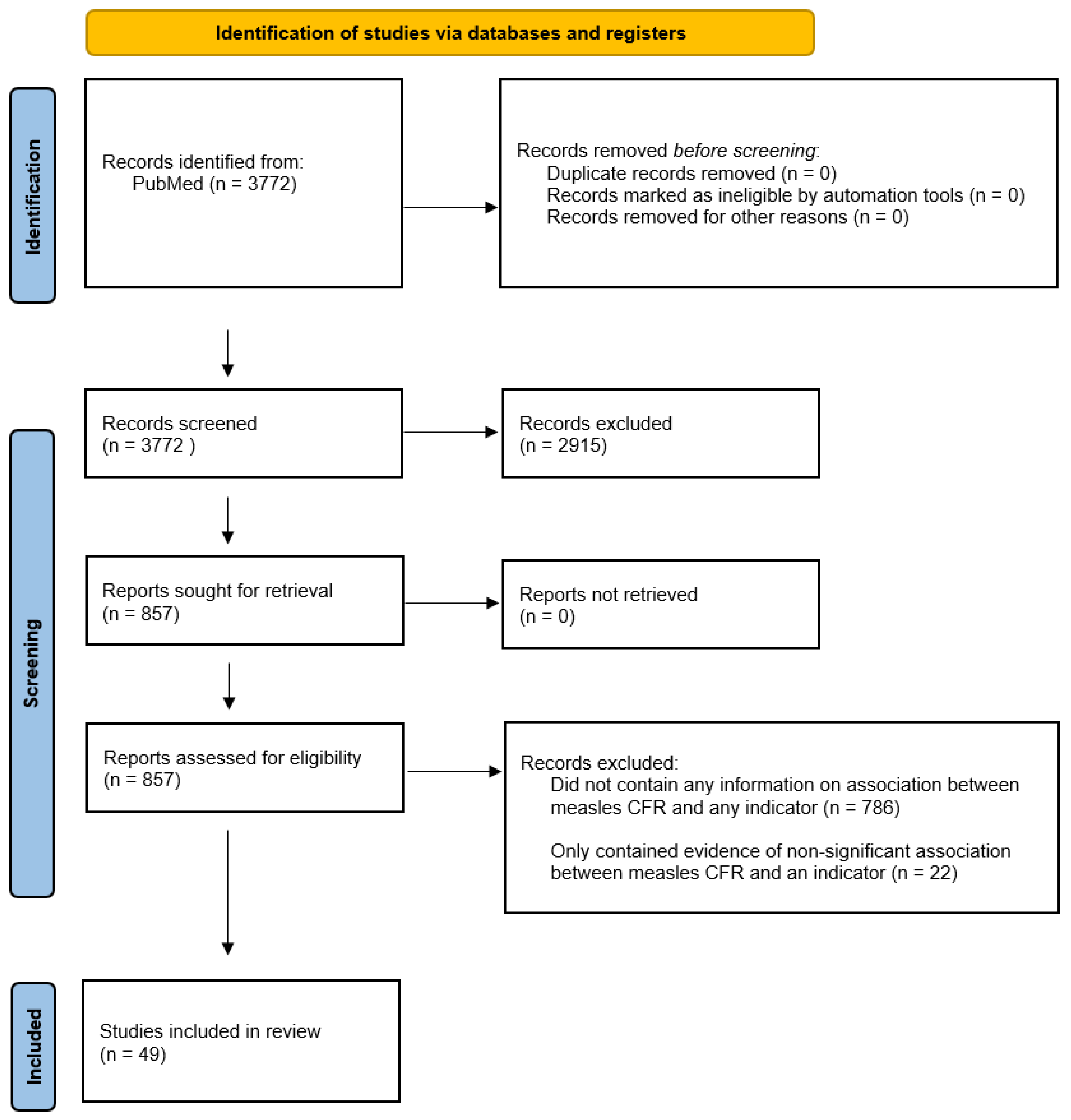
2.2. Literature Review
3. Results
3.1. Conceptual Framework
3.2. Literature Review
3.2.1. Health System Access and Care-Seeking Behaviors
Educational Attainment
Surrounding Conflict
Travel Time to Nearest Health Facility/Major City or Settlement
Indicators without Supporting Evidence
3.2.2. Health System Quality
Level of Health Care Available
Under-Five Mortality Rate
Indicators without Supporting Evidence
3.2.3. Nutritional Status
Malnutrition
Vitamin A Deficiency Prevalence
Vitamin A Supplementation
3.2.4. Risk of Secondary Infection
Average Household Size
HIV Prevalence
Indicators without Supporting Evidence
3.2.5. Measles Control and Epidemiology
First-Dose Coverage of Measles-Containing Vaccine (MCV1)
Second-Dose Coverage of Measles-Containing Vaccine (MCV2)
Vitamin A Treatment
Indicators without Supporting Evidence
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dixon, M.G.; Ferrari, M.; Antoni, S.; Li, X.; Portnoy, A.; Lambert, B.; Hauryski, S.; Hatcher, H.; Nedelec, Y.; Patel, M.; et al. Progress Toward Regional Measles Elimination—Worldwide, 2000–2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Simons, E.; Ferrari, M.; Fricks, J.; Wannemuehler, K.; Anand, A.; Burton, A.; Strebel, P. Assessment of the 2010 global measles mortality reduction goal: Results from a model of surveillance data. Lancet 2012, 379, 2173–2178. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, A.; Hsieh, Y.L.; Abbas, K.; Klepac, P.; Santos, H.; Brenzel, L.; Jit, M.; Ferrari, M. Differential health impact of intervention programs for time-varying disease risk: A measles vaccination modeling study. BMC Med. 2022, 20, 113. [Google Scholar] [CrossRef]
- World Health Organization. Reducing Global Measles Mortality. 2003. Available online: https://apps.who.int/iris/handle/10665/78321 (accessed on 28 June 2023).
- Li, X.; Mukandavire, C.; Cucunubá, Z.M.; Londono, S.E.; Abbas, K.; Clapham, H.E.; Jit, M.; Johnson, H.L.; Papadopoulos, T.; Vynnycky, E.; et al. Estimating the health impact of vaccination against ten pathogens in 98 low-income and middle-income countries from 2000 to 2030: A modelling study. Lancet 2021, 397, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, A.; Jit, M.; Ferrari, M.; Hanson, M.; Brenzel, L.; Verguet, S. Estimates of case-fatality ratios of measles in low-income and middle-income countries: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e472–e481. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Weekly Epidemiological Record; World Health Organization: Geneva, Switzerland, 2021; Volume 96, pp. 133–144. [Google Scholar]
- Hübschen, J.M.; Gouandjika-Vasilache, I.; Dina, J. Measles. Lancet 2022, 399, 678–690. [Google Scholar] [CrossRef]
- Perry, R.T.; Halsey, N.A. The clinical significance of measles: A review. J. Infect. Dis. 2004, 189 (Suppl. S1), S4–S16. [Google Scholar] [CrossRef]
- Wolfson, L.J.; Grais, R.F.; Luquero, F.J.; Birmingham, M.E.; Strebel, P.M. Estimates of measles case fatality ratios: A comprehensive review of community-based studies. Int. J. Epidemiol. 2009, 38, 192–205. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Bhuiya, A.; Wojtyniak, B.; D’Souza, S.; Nahar, L.; Shaikh, K. Measles case fatality among the under-fives: A multivariate analysis of risk factors in a rural area of Bangladesh. Soc. Sci. Med. 1987, 24, 439–443. [Google Scholar] [CrossRef]
- Clemens, J.D.; Stanton, B.F.; Chakraborty, J.; Chowdhury, S.; Rao, M.R.; Ali, M.; Zimicki, S.; Wojtyniak, B. Measles vaccination and childhood mortality in rural Bangladesh. Am. J. Epidemiol. 1988, 128, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Ndikuyeze, A.; Cook, A.; Cutts, F.T.; Bennett, S. Priorities in global measles control: Report of an outbreak in N’Djamena, Chad. Epidemiol. Infect. 1995, 115, 309–314. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Moss, W.J.; Fisher, C.; Scott, S.; Monze, M.; Ryon, J.J.; Quinn, T.C.; Griffin, D.E.; Cutts, F.T. HIV type 1 infection is a risk factor for mortality in hospitalized Zambian children with measles. Clin. Infect. Dis. 2008, 46, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Murhekar, M.V.; Ahmad, M.; Shukla, H.; Abhishek, K.; Perry, R.T.; Bose, A.S.; Shimpi, R.; Kumar, A.; Kaliaperumal, K.; Sethi, R.; et al. Measles case fatality rate in Bihar, India, 2011–2012. PLoS ONE 2014, 9, e96668. [Google Scholar] [CrossRef] [PubMed]
- Salama, P.; Assefa, F.; Talley, L.; Spiegel, P.; van Der Veen, A.; Gotway, C.A. Malnutrition, measles, mortality, and the humanitarian response during a famine in Ehiopia. JAMA 2001, 286, 563–571. [Google Scholar] [CrossRef]
- Joshi, A.B.; Luman, E.T.; Nandy, R.; Subedi, B.K.; Liyanage, J.B.; Wierzba, T.F. Measles deaths in Nepal: Estimating the national case-fatality ratio. Bull. World Health Organ. 2009, 87, 456–465. [Google Scholar] [CrossRef]
- Meteke, S.; Stefopulos, M.; Als, D.; Gaffey, M.; Kamali, M.; Siddiqui, F.J.; Munyuzangabo, M.; Jain, R.P.; Shah, S.; Radhakrishnan, A.; et al. Delivering infectious disease interventions to women and children in conflict settings: A systematic reviefw. BMJ Glob. Health 2020, 5, e001967. [Google Scholar] [CrossRef]
- Moss, W.J. Measles still has a devastating impact in unvaccinated populations. PLoS Med. 2007, 4, e24. [Google Scholar] [CrossRef]
- Gignoux, E.; Polonsky, J.; Ciglenecki, I.; Bichet, M.; Coldiron, M.; Thuambe Lwiyo, E.; Akonda, I.; Serafini, M.; Porten, K. Risk factors for measles mortality and the importance of decentralized case management during an unusually large measles epidemic in eastern Democratic Republic of Congo in 2013. PLoS ONE 2018, 13, e0194276. [Google Scholar] [CrossRef]
- Lee, C.T.; Hagan, J.E.; Jantsansengee, B.; Tumurbaatar, O.E.; Altanchimeg, S.; Yadamsuren, B.; Demberelsuren, S.; Tserendorj, C.; Munkhtogoo, O.; Badarch, D.; et al. Increase in Infant Measles Deaths During a Nationwide Measles Outbreak-Mongolia, 2015–2016. J. Infect. Dis. 2019, 220, 1771–1779. [Google Scholar] [CrossRef]
- Rey, M.; Celers, J.; Mouton, Y.; Netter, R. Impact of measles in France. Rev. Infect. Dis. 1983, 5, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M.; Peña Reyes, M.E.; Little, B.B. Epidemiologic transition in an isolated indigenous community in the Valley of Oaxaca, Mexico. Am. J. Phys. Anthropol. 2008, 137, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Spencer, H.C.; Kaseje, D.C.; Mosley, W.H.; Sempebwa, E.K.; Huong, A.Y.; Roberts, J.M. Impact on mortality and fertility of a community-based malaria control programme in Saradidi, Kenya. Ann. Trop. Med. Parasitol. 1987, 81 (Suppl. S1), 36–45. [Google Scholar] [CrossRef] [PubMed]
- Rosero-Bixby, L. Socioeconomic development, health interventions and mortality decline in Costa Rica. Scand. J. Soc. Med. Suppl. 1991, 46, 33–42. [Google Scholar] [PubMed]
- Sepúlveda, J.; Bustreo, F.; Tapia, R.; Rivera, J.; Lozano, R.; Oláiz, G.; Partida, V.; García-García, L.; Valdespino, J.L. Improvement of child survival in Mexico: The diagonal approach. Lancet 2006, 368, 2017–2027. [Google Scholar] [CrossRef] [PubMed]
- Aurangzeb, B.; Fatmee, A.; Waris, R.; Haider, N.; Berjees, A.; Raza, S.H. Risk factors for mortality among admitted children with complications of measles in Pakistan: An observational study. J. Pak. Med. Assoc. 2021, 71, 497–501. [Google Scholar] [CrossRef]
- Barclay, A.J.; Foster, A.; Sommer, A. Vitamin A supplements and mortality related to measles: A randomised clinical trial. Br. Med. J. (Clin. Res. Ed.) 1987, 294, 294–296. [Google Scholar] [CrossRef]
- Dollimore, N.; Cutts, F.; Binka, F.N.; Ross, D.A.; Morris, S.S.; Smith, P.G. Measles incidence, case fatality, and delayed mortality in children with or without vitamin A supplementation in rural Ghana. Am. J. Epidemiol. 1997, 146, 646–654. [Google Scholar] [CrossRef]
- Lagunju, I.A.; Orimadegun, A.E.; Oyedemi, D.G. Measles in Ibadan: A continuous scourge. Afr. J. Med. Med. Sci. 2005, 34, 383–387. [Google Scholar]
- Ahmed, P.A.; Babaniyi, I.B.; Otuneye, A.T. Review of childhood measles admissions at the National Hospital, Abuja. Niger. J. Clin. Pract. 2010, 13, 413–416. [Google Scholar]
- le Roux, D.M.; le Roux, S.M.; Nuttall, J.J.; Eley, B.S. South African measles outbreak 2009–2010 as experienced by a paediatric hospital. S. Afr. Med. J. 2012, 102, 760–764. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Coetzee, S.; Morrow, B.M.; Argent, A.C. Measles in a South African paediatric intensive care unit: Again! J. Paediatr. Child Health 2014, 50, 379–385. [Google Scholar] [CrossRef]
- Commey, J.O.; Richardson, J.E. Measles in Ghana—1973–1982. Ann. Trop. Paediatr. 1984, 4, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Avila-Figueroa, C.; Navarrete-Navarro, S.; Martínez-Aguilar, M.; Ruiz-Gutiérrez, E.; Santos, J.I. Complications in children with measles. Bol. Med. Hosp. Infant. Mex. 1990, 47, 520–523. [Google Scholar] [PubMed]
- Samsi, T.K.; Ruspandji, T.; Susanto, I.; Gunawan, K. Risk factors for severe measles. Southeast Asian J. Trop. Med. Public Health 1992, 23, 497–503. [Google Scholar] [PubMed]
- Alwar, A.J. The effect of protein energy malnutrition on morbidity and mortality due to measles at Kenyatta National Hospital, Nairobi (Kenya). East Afr. Med. J. 1992, 69, 415–418. [Google Scholar]
- Choudhry, V.P.; Atmar, M.; Amin, I.; Aram, G.N.; Ghani, R. Effect of protein energy malnutrition on the immediate outcome of measles. Indian J. Pediatr. 1987, 54, 717–722. [Google Scholar] [CrossRef]
- Madhulika; Kabra, S.K.; Talati, A. Vitamin A supplementation in post-measles complications. J. Trop. Pediatr. 1994, 40, 305–307. [Google Scholar] [CrossRef]
- Fetuga, M.B.; Jokanma, O.F.; Ogunfowora, O.B.; Abiodun, R. A ten-year study of measles admissions in a Nigerian teaching hospital. Niger. J. Clin. Pract. 2007, 10, 41–46. [Google Scholar]
- Moss, W.J. Measles. Lancet 2017, 390, 2490–2502. [Google Scholar] [CrossRef]
- Courtright, P.; Fine, D.; Broadhead, R.L.; Misoya, L.; Vagh, M. Abnormal vitamin A cytology and mortality in infants aged 9 months and less with measles. Ann. Trop. Paediatr. 2002, 22, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Nojilana, B.; Norman, R.; Bradshaw, D.; van Stuijvenberg, M.E.; Dhansay, M.A.; Labadorios, D. Estimating the burden of disease attributable to vitamin A deficiency in South Africa in 2000. S. Afr. Med. J. 2007, 97, 748–753. [Google Scholar] [PubMed]
- Mayo-Wilson, E.; Imdad, A.; Herzer, K.; Yakoob, M.Y.; Bhutta, Z.A. Vitamin A supplements for preventing mortality, illness, and blindness in children aged under 5: Systematic review and meta-analysis. BMJ 2011, 343, d5094. [Google Scholar] [CrossRef] [PubMed]
- Burström, B.; Diderichsen, F.; Smedman, L. Child mortality in Stockholm during 1885–1910: The impact of household size and number of children in the family on the risk of death from measles. Am. J. Epidemiol. 1999, 149, 1134–1141. [Google Scholar] [CrossRef][Green Version]
- Aaby, P.; Bukh, J.; Lisse, I.M.; Smits, A.J. Measles mortality, state of nutrition, and family structure: A community study from Guinea-Bissau. J. Infect. Dis. 1983, 147, 693–701. [Google Scholar] [CrossRef]
- Aaby, P.; Bukh, J.; Lisse, I.M.; Smits, A.J. Overcrowding and intensive exposure as determinants of measles mortality. Am. J. Epidemiol. 1984, 120, 49–63. [Google Scholar] [CrossRef]
- Nandy, R.; Handzel, T.; Zaneidou, M.; Biey, J.; Coddy, R.Z.; Perry, R.; Strebel, P.; Cairns, L. Case-fatality rate during a measles outbreak in eastern Niger in 2003. Clin. Infect. Dis. 2006, 42, 322–328. [Google Scholar] [CrossRef]
- Oshitani, H.; Suzuki, H.; Mpabalwani, M.E.; Mizuta, K.; Numazaki, Y. Measles case fatality by sex, vaccination status, and HIV-1 antibody in Zambian children. Lancet 1996, 348, 415. [Google Scholar] [CrossRef]
- Jeena, P.M.; Wesley, A.G.; Coovadia, H.M. Infectious diseases at the paediatric isolation units of Clairwood and King Edward VIII Hospitals, Durban. Trends in admission and mortality rates (1985–1996) and the early impact of HIV (1994–1996). S. Afr. Med. J. 1998, 88, 867–872. [Google Scholar]
- Coakley, K.J.; Coakley, C.A.; Spooner, V.; Smith, T.A.; Javati, A.; Kajoi, M. A review of measles admissions and deaths in the paediatric ward of Goroka Base Hospital during 1989. Papua New Guin. Med. J. 1991, 34, 6–12. [Google Scholar]
- Nayir, T.; Nazlıcan, E.; Şahin, M.; Kara, F.; Alp Meşe, E. Effects of immunization program on morbidity and mortality rates ofvaccine-preventable diseases in Turkey. Turk. J. Med. Sci. 2020, 50, 1909–1915. [Google Scholar] [CrossRef]
- Aaby, P.; Bhuiya, A.; Nahar, L.; Knudsen, K.; de Francisco, A.; Strong, M. The survival benefit of measles immunization may not be explained entirely by the prevention of measles disease: A community study from rural Bangladesh. Int. J. Epidemiol. 2003, 32, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Samb, B.; Aaby, P.; Whittle, H.; Seck, A.M.; Simondon, F. Decline in measles case fatality ratio after the introduction of measles immunization in rural Senegal. Am. J. Epidemiol. 1997, 145, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Oshitani, H.; Mpabalwani, M.; Kasolo, F.; Mizuta, K.; Luo, N.P.; Bhat, G.J.; Suzuki, H.; Numazaki, Y. Measles infection in hospitalized children in Lusaka, Zambia. Ann. Trop. Paediatr. 1995, 15, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Mgone, J.M.; Mgone, C.S.; Duke, T.; Frank, D.; Yeka, W. Control measures and the outcome of the measles epidemic of 1999 in the Eastern Highlands Province. Papua New Guin. Med. J. 2000, 43, 91–97. [Google Scholar]
- Aurangzeb, B.; Nisar, Y.B.; Hazir, T.; Burki, F.; Hassan, M. Clinical outcome in children hospitalized with complicated measles. J. Coll. Physicians Surg. Pak. 2005, 15, 547–551. [Google Scholar]
- Gutu, M.A.; Bekele, A.; Seid, Y.; Woyessa, A.B. Epidemiology of measles in Oromia region, Ethiopia, 2007–2016. Pan Afr. Med. J. 2020, 37, 171. [Google Scholar] [CrossRef]
- Hussey, G.D.; Klein, M. A randomized, controlled trial of vitamin A in children with severe measles. N. Engl. J. Med. 1990, 323, 160–164. [Google Scholar] [CrossRef]
- Hussey, G.D.; Klein, M. Routine high-dose vitamin A therapy for children hospitalized with measles. J. Trop. Pediatr. 1993, 39, 342–345. [Google Scholar] [CrossRef]
- Dzeyie, K.A.; Lowang, D.; Dikid, T.; Wangsu, W.; Tamir, T. Measles outbreak investigation at Indo-Myanmar border, Longding District, Arunachal Pradesh, India, 2017. Indian J. Public Health 2021, 65, S23–S28. [Google Scholar] [CrossRef]
- Grais, R.F.; Dubray, C.; Gerstl, S.; Guthmann, J.P.; Djibo, A.; Nargaye, K.D.; Coker, J.; Alberti, K.P.; Cochet, A.; Ihekweazu, C.; et al. Unacceptably high mortality related to measles epidemics in Niger, Nigeria, and Chad. PLoS Med. 2007, 4, e16. [Google Scholar] [CrossRef] [PubMed]
- Aaby, P.; Bukh, J.; Lisse, I.M.; da Silva, M.C. Further community studies on the role of overcrowding and intensive exposure on measles mortality. Rev. Infect. Dis. 1988, 10, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.M.; Crowcroft, N.S.; Friedman, L.; Deeks, S.L.; Halperin, S.A.; Severini, A.; Hatchette, T.F.; Bolotin, S. Waning of measles maternal antibody in infants in measles elimination settings—A systematic literature review. Vaccine 2018, 36, 1248–1255. [Google Scholar] [CrossRef]
- Scott, S.; Cumberland, P.; Shulman, C.E.; Cousens, S.; Cohen, B.J.; Brown, D.W.; Bulmer, J.N.; Dorman, E.K.; Kawuondo, K.; Marsh, K.; et al. Neonatal measles immunity in rural Kenya: The influence of HIV and placental malaria infections on placental transfer of antibodies and levels of antibody in maternal and cord serum samples. J. Infect. Dis. 2005, 191, 1854–1860. [Google Scholar] [CrossRef]
- Moss, W.J.; Scott, S.; Mugala, N.; Ndhlovu, Z.; Beeler, J.A.; Audet, S.A.; Ngala, M.; Mwangala, S.; Nkonga-Mwangilwa, C.; Ryon, J.J.; et al. Immunogenicity of standard-titer measles vaccine in HIV-1-infected and uninfected Zambian children: An observational study. J. Infect. Dis. 2007, 196, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Perry, R.T.; Mmiro, F.; Ndugwa, C.; Semba, R.D. Measles infection in HIV-infected African infants. Ann. N. Y. Acad. Sci. 2000, 918, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Mina, M.J.; Metcalf, C.J.; de Swart, R.L.; Osterhaus, A.D.; Grenfell, B.T. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science 2015, 348, 694–699. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mechanisms | Indicators |
|---|---|
| Health system access and care-seeking behaviors |
|
| Health system quality |
|
| Measles control and epidemiology |
|
| Nutritional status |
|
| Risk of secondary infection |
|
| Published Literature Includes Randomized Controlled Trial with Significant Relationship | Published Literature Supports Significant Observational Association | Published Literature Supports Qualitative Association | Published Literature with Non-Significant Evidence | No Evidence Found in Published Literature |
|---|---|---|---|---|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sbarra, A.N.; Jit, M.; Mosser, J.F.; Ferrari, M.; Cutts, F.; Papania, M.; Kretsinger, K.; McCarthy, K.A.; Thakkar, N.; Gaythorpe, K.A.M.; et al. Population-Level Risk Factors Related to Measles Case Fatality: A Conceptual Framework Based on Expert Consultation and Literature Review. Vaccines 2023, 11, 1389. https://doi.org/10.3390/vaccines11081389
Sbarra AN, Jit M, Mosser JF, Ferrari M, Cutts F, Papania M, Kretsinger K, McCarthy KA, Thakkar N, Gaythorpe KAM, et al. Population-Level Risk Factors Related to Measles Case Fatality: A Conceptual Framework Based on Expert Consultation and Literature Review. Vaccines. 2023; 11(8):1389. https://doi.org/10.3390/vaccines11081389
Chicago/Turabian StyleSbarra, Alyssa N., Mark Jit, Jonathan F. Mosser, Matthew Ferrari, Felicity Cutts, Mark Papania, Katrina Kretsinger, Kevin A. McCarthy, Niket Thakkar, Katy A. M. Gaythorpe, and et al. 2023. "Population-Level Risk Factors Related to Measles Case Fatality: A Conceptual Framework Based on Expert Consultation and Literature Review" Vaccines 11, no. 8: 1389. https://doi.org/10.3390/vaccines11081389
APA StyleSbarra, A. N., Jit, M., Mosser, J. F., Ferrari, M., Cutts, F., Papania, M., Kretsinger, K., McCarthy, K. A., Thakkar, N., Gaythorpe, K. A. M., Gamage, D., Krause, L. K., Dansereau, E., Crowcroft, N., & Portnoy, A. (2023). Population-Level Risk Factors Related to Measles Case Fatality: A Conceptual Framework Based on Expert Consultation and Literature Review. Vaccines, 11(8), 1389. https://doi.org/10.3390/vaccines11081389