
Efficacy of Six Different SARS-CoV-2 Vaccines during a Six-Month Follow-Up and Five COVID-19 Waves in Brazil and Mexico


 , , , , , , , , , and
, , , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
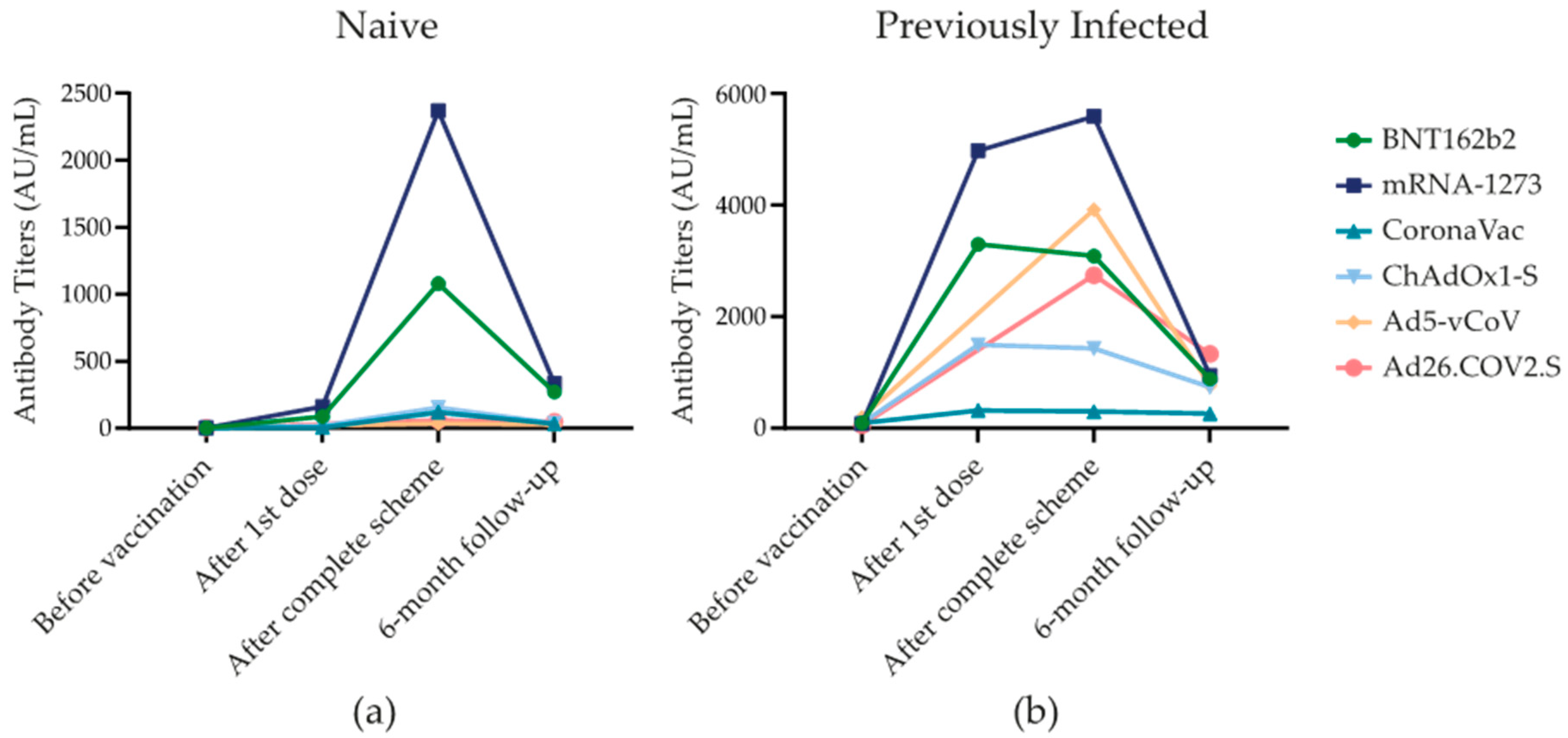
3.1. SARS-CoV-2 Spike 1–2 IgG Antibodies during Six-Month Follow-Up
3.2. Ordinary Least Square Model for the Antibody Titers at the 6-Month Follow-Up
3.3. SARS-CoV-2 Infection
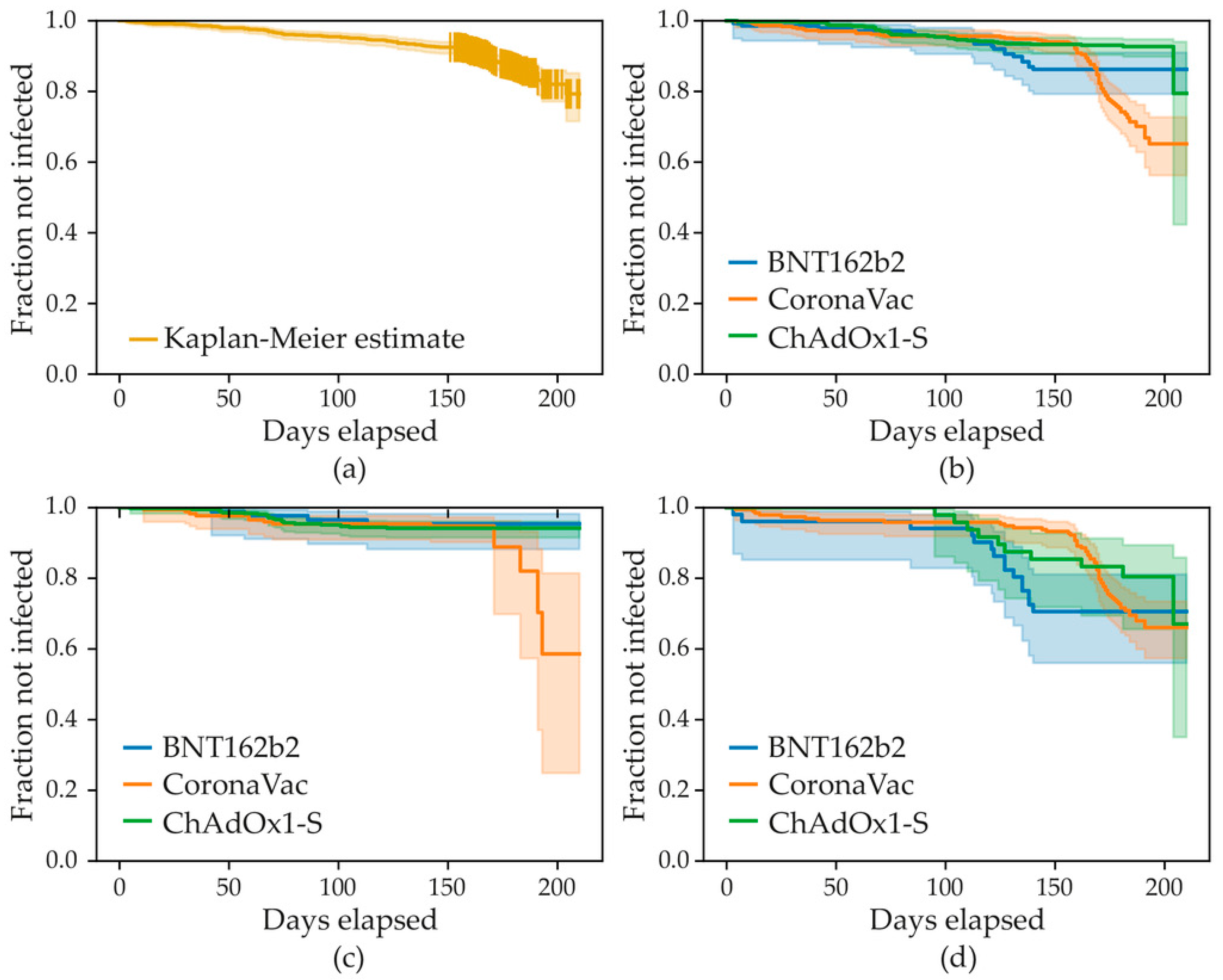
3.4. Survival Analysis and Cox Proportional Hazard Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Basta, N.E.; Moodie, E.E.E.M. COVID-19 Vaccine Tracker. Available online: https://covid19.trackvaccines.org/ (accessed on 28 December 2022).
- Chi, W.-Y.; Li, Y.-D.; Huang, H.-C.; Chan, T.E.H.; Chow, S.-Y.; Su, J.-H.; Ferrall, L.; Hung, C.-F.; Wu, T.-C. COVID-19 vaccine update: Vaccine effectiveness, SARS-CoV-2 variants, boosters, adverse effects, and immune correlates of protection. J. Biomed. Sci. 2022, 29, 82. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by COVID-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Khoury, J.; Najjar-Debbiny, R.; Hanna, A.; Jabbour, A.; Abu Ahmad, Y.; Saffuri, A.; Abu-Sinni, M.; Shkeiri, R.; Elemy, A.; Hakim, F. COVID-19 vaccine–Long term immune decline and breakthrough infections. Vaccine 2021, 39, 6984–6989. [Google Scholar] [CrossRef]
- Favresse, J.; Bayart, J.-L.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Wieers, G.; Laurent, C.; Dogné, J.-M.; et al. Antibody titres decline 3-month post-vaccination with BNT162b2. Emerg. Microbes Infect. 2021, 10, 1495–1498. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, 31. [Google Scholar] [CrossRef]
- DiaSorin LIASON SARS-CoV-2 S1/S2 IgG. The Fully Automated Serology Test for the Detection of SARS-CoV-2 IgG Antibodies. Available online: https://www.diasorin.com/sites/default/files/allegati/liaisonr_sars-cov-2_s1s2_igg_brochure.pdf (accessed on 25 January 2023).
- Bonelli, F.; Sarasini, A.; Zierold, C.; Calleri, M.; Bonetti, A.; Vismara, C.; Blocki, F.A.; Pallavicini, L.; Chinali, A.; Campisi, D.; et al. Clinical and Analytical Performance of an Automated Serological Test That Identifies S1/S2-Neutralizing IgG in COVID-19 Patients Semiquantitatively. J. Clin. Microbiol. 2020, 58, e01224-20. [Google Scholar] [CrossRef]
- Levi, R.; Azzolini, E.; Pozzi, C.; Ubaldi, L.; Lagioia, M.; Mantovani, A.; Rescigno, M. One dose of SARS-CoV-2 vaccine exponentially increases antibodies in individuals who have recovered from symptomatic COVID-19. J. Clin. Investig. 2021, 131, 1–5. [Google Scholar] [CrossRef]
- Levi, R.; Ubaldi, L.; Pozzi, C.; Angelotti, G.; Sandri, M.T.; Azzolini, E.; Salvatici, M.; Savevski, V.; Mantovani, A.; Rescigno, M. The antibody response to SARS-CoV-2 infection persists over at least 8 months in symptomatic patients. Commun. Med. 2021, 1, 32. [Google Scholar] [CrossRef]
- Morales-Núñez, J.J.; Muñoz-Valle, J.F.; Machado-Sulbarán, A.C.; Díaz-Pérez, S.A.; Torres-Hernández, P.C.; Panduro-Espinoza, B.V.; de Leon, J.A.G.-D.; Munguía-Ramirez, C.D.; Hernández-Bello, J. Comparison of three different COVID-19 vaccine platforms (CoronaVac, BTN162b2, and Ad5-nCoV) in individuals with and without prior COVID-19: Reactogenicity and neutralizing antibodies. Immunol. Lett. 2022, 251, 20–28. [Google Scholar] [CrossRef]
- Sandoval, C.; Guerrero, D.; Muñoz, J.; Godoy, K.; Souza-Mello, V.; Farías, J. Effectiveness of mRNA, protein subunit vaccine and viral vectors vaccines against SARS-CoV-2 in people over 18 years old: A systematic review. Expert Rev. Vaccines 2022, 22, 35–53. [Google Scholar] [CrossRef]
- Romero-Ibarguengoitia, M.E.; González-Cantú, A.; Pozzi, C.; Levi, R.; Mollura, M.; Sarti, R.; Sanz-Sánchez, M.Á.; Rivera-Salinas, D.; Hernández-Ruíz, Y.G.; Armendariz-Vázquez, A.G.; et al. Analysis of immunization time, amplitude, and adverse events of seven different vaccines against SARS-CoV-2 across four different countries. Front. Immunol. 2022, 13, 894277. [Google Scholar] [CrossRef]
- van Gils, M.J.; Lavell, A.; van der Straten, K.; Appelman, B.; Bontjer, I.; Poniman, M.; Burger, J.A.; Oomen, M.; Bouhuijs, J.H.; van Vught, L.A.; et al. Antibody responses against SARS-CoV-2 variants induced by four different SARS-CoV-2 vaccines in health care workers in the Netherlands: A prospective cohort study. PLoS Med. 2022, 19, e1003991. [Google Scholar] [CrossRef]
- Glöckner, S.; Hornung, F.; Baier, M.; Weis, S.; Pletz, M.W.; Deinhardt-Emmer, S.; Löffler, B.; The CoNAN Study Group. Robust Neutralizing Antibody Levels Detected after Either SARS-CoV-2 Vaccination or One Year after Infection. Viruses 2021, 13, 2003. [Google Scholar] [CrossRef]
- Addo, I.Y.; Dadzie, F.A.; Okeke, S.R.; Boadi, C.; Boadu, E.F. Duration of immunity following full vaccination against SARS-CoV-2: A systematic review. Arch. Public Health 2022, 80, 200. [Google Scholar] [CrossRef]
- Fonseca, M.H.G.; Souza, T.D.F.G.D.; Araújo, F.M.D.C.; de Andrade, L.O.M. Dynamics of antibody response to CoronaVac vaccine. J. Med. Virol. 2022, 94, 2139–2148. [Google Scholar] [CrossRef]
- Ali, H.; Alahmad, B.; Al-Shammari, A.A.; Alterki, A.; Hammad, M.; Cherian, P.; Alkhairi, I.; Sindhu, S.; Thanaraj, T.A.; Mohammad, A.; et al. Previous COVID-19 Infection and Antibody Levels After Vaccination. Front. Public Health 2021, 9, 778243. [Google Scholar] [CrossRef]
- Frasca, D.; Reidy, L.; Cray, C.; Diaz, A.; Romero, M.; Kahl, K.; Blomberg, B.B. Influence of obesity on serum levels of SARS-CoV-2-specific antibodies in COVID-19 patients. PLoS ONE 2021, 16, e0245424. [Google Scholar] [CrossRef]
- Zeng, B.; Le Gao, L.; Zhou, Q.; Yu, K.; Sun, F. Effectiveness of COVID-19 vaccines against SARS-CoV-2 variants of concern: A systematic review and meta-analysis. BMC Med. 2022, 20, 200. [Google Scholar] [CrossRef] [PubMed]
- Chua, J.X.; Durrant, L.G.; Chok, Y.L.; Lai, O.M. Susceptibility to SARS-CoV-2 omicron following ChAdOx1 nCoV-19 and BNT162b2 versus CoronaVac vaccination. iScience 2022, 25, 105379. [Google Scholar] [CrossRef] [PubMed]
- Dadras, O.; SeyedAlinaghi, S.; Karimi, A.; Shojaei, A.; Amiri, A.; Mahdiabadi, S.; Fakhfouri, A.; Razi, A.; Mojdeganlou, H.; Mojdeganlou, P.; et al. COVID-19 Vaccines’ Protection Over Time and the Need for Booster Doses; a Systematic Review. Arch. Acad. Emerg. Med. 2022, 10, e53. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.-Y.; Xue, J.-H.; Xiao, Y.; Jia, Z.-J.; Wu, M.-J.; Liu, Y.-Y.; Li, W.-L.; Liang, X.-M.; Yang, T.-C. Response and Duration of Serum Anti-SARS-CoV-2 Antibodies After Inactivated Vaccination Within 160 Days. Front. Immunol. 2021, 12, 786554. [Google Scholar] [CrossRef]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARS-CoV-2 after COVID-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022, 386, 1207–1220. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total (n = 1132) (%) | BNT162b2 (n = 159) (%) | mRNA-1273 (n = 17) (%) | CoronaVac (n = 429) (%) | ChAdOx1-S (n = 518) (%) | Ad5-vCoV (n = 4) (%) | Ad26. COV2.S (n = 5) (%) | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Diabetes Mellitus 2 | 219 (19.4) | 6 (3.8) | 1 (5.9) | 63 (14.7) | 149 (28.8) | 0 (0) | 0 (0) | <0.001 |
| Hypertension | 356 (31.5) | 21 (13.3) | 2 (11.8) | 94 (22.0) | 237 (45.8) | 2 (50.0) | 0 (0) | <0.001 |
| Asthma | 32 (2.8) | 3 (1.9) | 1 (5.9) | 13 (3.0) | 15 (2.9) | 0 (0) | 0 (0) | 0.923 |
| Chronic Obstructive Pulmonary Disease | 8 (0.7) | 0 (0) | 0 (0) | 2 (0.5) | 6 (1.2) | 0 (0) | 0 (0) | 0.675 |
| Obesity | 383 (33.9) | 33 (20.9) | 2 (12.5) | 142 (33.2) | 205 (39.6) | 1 (25.0) | 0 (0) | <0.001 |
| Smoking | 99 (8.5) | 17 (10.8) | 4 (23.5) | 43 (10.0) | 34 (6.6) | 0 (0) | 1 (20.0) | 0.060 |
| Renal Disease | 15 (1.3) | 1 (0.6) | 0 (0) | 4 (0.9) | 10 (1.9) | 0 (0) | 0 (0) | 0.719 |
| Dyslipidemia | 210 (18.6) | 12 (7.6) | 1 (5.9) | 59 (13.8) | 137 (26.4) | 1 (25.0) | 0 (0) | <0.001 |
| Pregnancy | 2 (0.4) | 0 (0) | 0 (0) | 1 (0.2) | 0 (0) | 1 (25.0) | 0 (0) | <0.001 |
| Active Neoplasia | 12 (1.1) | 0 (0) | 0 (0) | 1 (0.2) | 11 (2.1) | 0 (0) | 0 (0) | 0.067 |
| Previous Neoplasia | 32 (2.8) | 1 (0.6) | 0 (0) | 6 (1.4) | 25 (4.8) | 0 (0) | 0 (0) | 0.015 |
| Atrial Fibrillation | 31 (2.7) | 0 (0) | 0 (0) | 4 (0.9) | 27 (5.2) | 0 (0) | 0 (0) | <0.001 |
| Cardiac Failure | 9 (0.8) | 0 (0) | 0 (0) | 0 (0) | 9 (1.7) | 0 (0) | 0 (0) | 0.057 |
| Coronary Disease | 23 (2.0) | 0 (0) | 0 (0) | 3 (0.7) | 20 (3.9) | 0 (0) | 0 (0) | 0.006 |
| Stroke | 14 (1.2) | 0 (0) | 0 (0) | 1 (0.2) | 13 (2.5) | 0 (0) | 0 (0) | 0.027 |
| Hepatic Steatosis | 50 (4.4) | 3 (1.9) | 0 (0) | 23 (5.4) | 23 (4.4) | 1 (25.0) | 0 (0) | 0.140 |
| Cirrhosis | 6 (0.5) | 0 (0) | 0 (0) | 1 (0.2) | 5 (1.0) | 0 (0) | 0 (0) | 0.616 |
| Hepatitis/Hepatic Failure | 13 (1.2) | 1 (0.6) | 0 (0) | 4 (0.9) | 8 (1.5) | 0 (0) | 0 (0) | 0.906 |
| Rheumatoid Arthritis | 58 (5.1) | 5 (3.2) | 1 (5.9) | 10 (2.3) | 42 (8.1) | 0 (0) | 0 (0) | 0.003 |
| Psoriasis/Thyroiditis and Other Immune Diseases | 77 (6.8) | 6 (3.8) | 0 (0) | 21 (4.9) | 50 (9.7) | 0 (0) | 0 (0) | 0.022 |
| Usage of Immunosuppressive Drugs | 16 (1.4) | 2 (1.3) | 0 (0) | 5 (1.2) | 9 (1.7) | 0 (0) | 0 (0) | 0.965 |
| Gout | 39 (3.5) | 2 (1.3) | 0 (0) | 11 (2.6) | 26 (5.0) | 0 (0) | 0 (0) | 0.158 |
| Surgical Procedure with General Anesthesia | 64 (5.7) | 4 (2.5) | 0 (0) | 19 (4.4) | 39 (7.5) | 2 (50.0) | 0 (0) | <0.001 |
| Organ Transplant | 5 (0.4) | 0 (0) | 0 (0) | 1 (0.2) | 4 (0.8) | 0 (0) | 0 (0) | 0.773 |
| SARS-CoV-2 Infection History | Total (n = 1132) | BNT162b2 (n = 159) (IQR) AU/mL | mRNA-1273 (n = 17) (IQR) AU/mL | CoronaVac (n = 429) (IQR) AU/mL | ChAdOx1-S (n = 518) (IQR) AU/mL | Ad5-vCoV (n = 4) (IQR) AU/mL | Ad26.COV2.S (n = 5) (IQR) AU/mL | p-Value |
|---|---|---|---|---|---|---|---|---|
| Before vaccination | ||||||||
| Negative | 3.8 (0) (n = 884) | 3.8 (3.7) (n = 110) | 3.8 (29.1) (n = 13) | 3.8 (1.2) (n = 303) | 3.8 (0) (n = 454) | 3.8 (0) (n = 2) | 3.8 (0) (n = 2) | 0.009 |
| Positive | 96.8 (173.7) (n = 247) | 99.6 (178.5) (n = 48) | 77.5 (196.6) (n = 4) | 91.0 (137.0) (n = 126) | 90.7 (267.0) (n = 64) | 198.0 (-) (n = 2) | 56.9 (-) (n = 3) | 0.908 |
| p-value | <0.001 | <0.001 | 0.032 | <0.001 | <0.001 | 0.333 | 0.200 | |
| After first dose | ||||||||
| Negative | 20.3 (69.6) (n = 866) | 89.4 (97.1) (n = 107) | 163.5 (5426.2) (n = 12) | 6.56 (22.1) (n = 249) | 21.6 (45.9) (n = 453) | - | - | <0.001 |
| Positive before vaccination | 584.0 (2409.0) (n = 235) | 3295 (3725.0) (n = 48) | 4970 (14,072.5) (n = 4) | 320.0 (447.0) (n = 119) | 1495.0 (3141.7) (n = 64) | - | - | <0.001 |
| New cases | 211 (-) (n = 3) | 211 (-) (n = 1) | (n = 0) | 245 (-) (n = 2) | (n = 0) | - | - | 1.000 |
| p-value | <0.001 | <0.001 | 0.078 | <0.001 | <0.001 | - | - | |
| 21–28 days after completion of scheme | ||||||||
| Negative | 160 (259.2) (n = 803) | 1080 (1855.5) (n = 94) | 2370 (3300) (n = 11) | 119 (112.9) (n = 269) | 155.0 (212.8) (n = 425) | 37.25 (-) (n = 2) | 60.7 (-) (n = 2) | <0.001 |
| Positive before vaccination | 608.5 (2156.0) (n = 228) | 3085.0 (3292.5) (n = 42) | 5585.0 (6580.0) (n = 4) | 303.0 (376.5) (n = 117) | 1430.0 (3174.7) (n = 60) | 3915 (-) (n = 2) | 2740 (-) (n = 3) | <0.001 |
| New cases | 1555 (1342.7) (n = 12) | 1960 (-) (n = 3) | (n = 0) | 905.5 (1363.5) (n = 8) | 2620.0 (-) (n = 1) | (n = 0) | (n = 0) | 0.081 |
| p-value | <0.001 | <0.001 | 0.056 | <0.001 | <0.001 | 0.333 | 0.200 | |
| Six months after completion of scheme | ||||||||
| Negative | 48.8 (152.2) (n = 730) | 271.0 (649.7) (n = 92) | 336.0 (827.0) (n = 11) | 33.7 (131.4) (n = 203) | 38.5 (72.9) (n = 421) | 27.9 (-) (n = 1) | 49.2 (-) (n = 2) | <0.001 |
| Positive before vaccination | 387.0 (834.0) (n = 247) | 886.5 (1079.0) (n = 48) | 948.5 (1793.9) (n = 4) | 262 (441.8) (n = 126) | 736.0 (1328.5) (n = 64) | 765 (-) (n = 2) | 1330.0 (-) (n = 3) | <0.001 |
| New cases | 926 (2353.0) (n = 155) | 1850 (1596.0) (n = 19) | 1305.5 (-) (n = 2) | 372.5 (2886.6) (n = 100) | 1190 (1901.5) (n = 33) | 3.8 (-) (n = 1) | (n = 0) | 0.082 |
| p-value | <0.001 | <0.001 | 0.599 | <0.001 | <0.001 | 0.259 | 0.200 | |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.022 | 0.015 | |
| Coefficient | p-Value | |
|---|---|---|
| Intercept | 0.21 (−0.06, 0.49) | 0.13 |
| ChAdOx1-SARS-CoV-2 | −0.56 (−0.85, −0.26) | <0.001 |
| CoronaVac | −0.45 (−0.74, −0.16) | 0.002 |
| mRNA−1273 | −0.52 (−1.8, 0.77) | 0.43 |
| Male sex | 0.03 (−0.07, 0.13) | 0.58 |
| Age b | −0.04 (−0.12, 0.03) | 0.25 |
| BMI c | −0.07 (−0.13, −0.02) | 0.012 |
| Antibodies d | 0.12 (−0.15, 0.38) | 0.39 |
| Antibodies*ChAdOx1-SARS-CoV-2 d | 0.67 (0.4, 0.95) | <0.001 |
| Antibodies*CoronaVac d | 0.48 (0.19, 0.76) | 0.001 |
| Antibodies*mRNA-1273 d | 0.29 (−0.81, 1.39) | 0.60 |
| Previous COVID infection e | 0.24 (0.11, 0.37) | <0.001 |
| COVID infection after 2nd dose | 1.17 (1.01, 1.33) | <0.001 |
| SARS-CoV-2 Infection | Total (n = 1132) (%) | BNT162b2 (n = 159) (%) | mRNA-1273 (n = 17) (%) | CoronaVac (n = 429) (%) | ChAdOx1 (n = 518) (%) | Ad5-vCoV (n = 4) (%) | Ad26.COV2.S (n = 5) (%) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Before vaccination | 247 (21.8) | 48 (30.4) | 4 (23.5) | 126 (29.4) | 64 (12.4) | 2 (50.0) | 3 (60.0) | <0.001 |
| After first dose | 4 (0.4) | 1 (0.6) | 0 (0) | 2 (0.5) | 1 (0.2) | - | - | 0.818 |
| After second dose | 183 (16.2) | 25 (15.7) | 2 (11.8) | 120 (28.0) | 34 (6.6) | 1 (25.0) | 1 (20.0) | <0.001 |
| SARS-CoV-2 Infection before vaccination | ||||||||
| Symptoms | ||||||||
| Fever | 87 (39.0) | 17 (40.5) | 3 (75.0) | 46 (41.1) | 18 (30.0) | 2 (100) | 1 (33.3) | 0.178 |
| Feverish | 55 (24.7) | 10 (23.8) | 2 (50.0) | 33 (29.5) | 10 (16.7) | 0 (0) | 0 (0) | 0.261 |
| Cough | 111 (49.8) | 20 (47.6) | 3 (75.0) | 56 (50.0) | 29 (48.3) | 1 (50.0) | 2 (66.7) | 0.914 |
| Headache | 128 (57.4) | 22 (52.4) | 2 (50.0) | 69 (61.6) | 32 (53.3) | 1 (50.0) | 2 (66.7) | 0.864 |
| Dyspnea | 70 (31.4) | 13 (31.0) | 0 (0) | 34 (30.4) | 22 (36.7) | 1 (50.0) | 0 (0) | 0.499 |
| Conjunctivitis | 9 (4.0) | 1 (2.4) | 0 (0) | 5 (4.5) | 3 (5.0) | 0 (0) | 0 (0) | 0.972 |
| Palpitations | 29 (13.0) | 8 (19.0) | 1 (25.0) | 11 (9.8) | 9 (15.0) | 0 (0) | 0 (0) | 0.575 |
| Thoracic pain | 47 (21.1) | 10 (23.8) | 0 (0) | 28 (25.0) | 8 (13.3) | 1 (50.0) | 0 (0) | 0.281 |
| Odynophagia | 81 (36.3) | 17 (40.5) | 2 (50.0) | 37 (33.0) | 22 (36.7) | 1 (50.0) | 2 (66.7) | 0.774 |
| Myalgias | 124 (55.6) | 25 (59.5) | 3 (75.0) | 62 (55.4) | 32 (53.3) | 1 (50.0) | 1 (33.3) | 0.898 |
| Arthralgias | 84 (37.7) | 15 (31.3) | 2 (50.0) | 43 (38.4) | 22 (36.7) | 1 (50.0) | 1 (33.3) | 0.991 |
| Anosmia | 112 (50.2) | 20 (47.6) | 1 (25.0) | 59 (42.7) | 29 (48.3) | 1 (50.0) | 2 (66.7) | 0.874 |
| Tiredness | 61 (27.4) | 14 (33.3) | 2 (50.0) | 23 (20.5) | 21 (35.0) | 1 (50.0) | 0 (0) | 0.166 |
| Diarrhea | 42 (18.8) | 10 (23.8) | 0 (0) | 17 (15.2) | 15 (25.0) | 0 (0) | 0 (0) | 0.387 |
| Vomiting | 23 (10.3) | 5 (11.9) | 1 (25.0) | 8 (7.1) | 9 (15.0) | 0 (0) | 0 (0) | 0.512 |
| Nausea | 11 (4.9) | 1 (2.4) | 0 (0) | 2 (1.8) | 8 (13.3) | 0 (0) | 0 (0) | 0.029 |
| Treatment | ||||||||
| Ambulatory | 219 (91.3) | 43 (91.5) | 3 (75.0) | 112 (93.3) | 56 (87.5) | 2 (100) | 3 (100) | 0.707 |
| Hospitalization | 19 (7.9) | 4 (2.5) | 1 (25.0) | 6 (5) | 8 (12.5) | 0 (0) | 0 (0) | |
| Intensive Care Unit | 2 (0.8) | 0 (0) | 0 (0) | 2 (1.7) | 0 (0) | 0 (0) | 0 (0) | |
| Need of supplementary oxygen | 0.936 | |||||||
| Total | 17 (7) | 3 (6.4) | 0 (0) | 8 (6.6) | 6 (9.4) | 0 (0) | 0 (0) | |
| Nasal cannula | 11 (64.7) | 2 (66.7) | 0 (0) | 4 (50.0) | 5 (83.3) | 0 (0) | 0 (0) | |
| Non-rebreather mask | 2 (11.8) | 0 (0) | 0 (0) | 1 (12.5) | 1 (16.7) | 0 (0) | 0 (0) | 0.684 |
| High flow equipment | 3 (17.6) | 1 (33.3) | 0 (0) | 2 (25.0) | 0 (0) | 0 (0) | 0 (0) | |
| Orotracheal intubation | 1 (5.9) | 0 (0) | 0 (0) | 1 (12.5) | 0 (0) | 0 (0) | 0 (0) | |
| SARS-CoV-2 Infection after first dose | ||||||||
| Symptoms | ||||||||
| Fever | 2 (50.0) | 1 (100) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.368 |
| Feverish | 2 (50.0) | 0 (0) | 0 (0) | 2 (100) | 0 (0) | - | - | 0.135 |
| Cough | 2 (50.0) | 0 (0) | 0 (0) | 2 (100) | 0 (0) | - | - | 0.135 |
| Headache | 3 (75.0) | 1 (100) | 0 (0) | 1 (50.0) | 1 (100) | - | - | 0.513 |
| Dyspnea | 1 (25.0) | 1 (100) | 0 (0) | 0 (0) | 0 (0) | - | - | 0.135 |
| Irritability | 1 (25.0) | 1 (100) | 0 (0) | 0 (0) | 0 (0) | - | - | 0.135 |
| Palpitations | 1 (25.0) | 0 (0) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.513 |
| Chills | 2 (50.0) | 0 (0) | 0 (0) | 2 (100) | 0 (0) | - | - | 0.135 |
| Odynophagia | 2 (50.0) | 1 (100) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.368 |
| Arthralgias | 2 (50.0) | 0 (0) | 0 (0) | 1 (50.0) | 1 (100) | - | - | 0.368 |
| Anosmia | 1 (25.0) | 0 (0) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.513 |
| Tiredness | 1 (25.0) | 0 (0) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.513 |
| Diarrhea | 1 (25.0) | 0 (0) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.513 |
| Vomiting | 1 (25.0) | 0 (0) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.513 |
| Nausea | 1 (25.0) | 0 (0) | 0 (0) | 0 (0) | 1 (100) | - | - | 0.135 |
| Dysgeusia | 1 (25.0) | 0 (0) | 0 (0) | 1 (50.0) | 0 (0) | - | - | 0.513 |
| Rhinorrhea | 1 (25.0) | 1 (100) | 0 (0) | 0 (0) | 0 (0) | - | - | 0.135 |
| Polypnea | 1 (25.0) | 1 (100) | 0 (0) | 0 (0) | 0 (0) | - | - | 0.135 |
| Treatment | ||||||||
| Ambulatory | 3 (75.0) | 1 (100) | 0 (0) | 1 (50.0) | 1 (100) | - | - | 0.513 |
| Hospitalization | 1 (25.0) | 0 (0) | 0 (0) | 1 (50.0) | 0 (0) | - | - | |
| Intensive Care Unit | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - | - | |
| Need of supplementary oxygen | ||||||||
| Total | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - | - | - |
| SARS-CoV-2 Infection after complete vaccination scheme | ||||||||
| Symptoms | ||||||||
| Fever | 54 (30.3) | 8 (33.3) | 1 (50) | 37 (31.9) | 8 (23.5) | 0 (0) | 0 (0) | 0.818 |
| Feverish | 25 (14.0) | 4 (16.7) | 0 (0) | 16 (13.8) | 5 (14.7) | 0 (0) | 0 (0) | 0.976 |
| Cough | 109 (61.2) | 9 (37.5) | 1 (50) | 78 (67.2) | 20 (58.8) | 1 (100) | 0 (0) | 0.079 |
| Headache | 79 (44.4) | 13 (54.2) | 1 (50.0) | 50 (43.1) | 13 (38.2) | 1 (100) | 1 (100) | 0.541 |
| Dyspnea | 11 (6.2) | 1 (4.2) | 0 (0) | 6 (5.2) | 4 (11.8) | 0 (0) | 0 (0) | 0.782 |
| Irritability | 6 (3.4) | 1 (4.2) | 0 (0) | 3 (2.6) | 2 (5.9) | 0 (0) | 0 (0) | 0.957 |
| Conjunctivitis | 8 (4.5) | 0 (0) | 0 (0) | 3 (2.6) | 4 (11.8) | 1 (100) | 0 (0) | <0.001 |
| Palpitations | 5 (2.8) | 1 (4.2) | 0 (0) | 3 (2.6) | 1 (2.9) | 0 (0) | 0 (0) | 0.998 |
| Thoracic pain | 13 (7.3) | 1 (4.2) | 0 (0) | 8 (6.9) | 3 (8.8) | 1 (100) | 0 (0) | 0.020 |
| Chills | 42 (23.6) | 3 (12.5) | 0 (0) | 33 (28.4) | 6 (17.6) | 0 (0) | 0 (0) | 0.409 |
| Odynophagia | 92 (51.7) | 14 (58.3) | 2 (100) | 60 (51.7) | 14 (41.2) | 1 (100) | 1 (100) | 0.340 |
| Myalgias | 77 (43.3) | 7 (29.2) | 1 (50) | 52 (44.8) | 17 (50.0) | 0 (0) | 0 (0) | 0.514 |
| Arthralgias | 53 (29.8) | 5 (20.8) | 0 (0) | 34 (29.3) | 13 (38.2) | 1 (100) | 0 (0) | 0.334 |
| Anosmia | 37 (20.8) | 4 (16.7) | 0 (0) | 20 (17.2) | 12 (35.3) | 0 (0) | 0 (0) | 0.716 |
| Tiredness | 58 (32.6) | 11 (45.8) | 1 (50.0) | 34 (29.3) | 11 (32.4) | 1 (100) | 0 (0) | 0.379 |
| Diarrhea | 16 (9.0) | 2 (8.3) | 0 (0) | 9 (7.8) | 5 (14.7) | 0 (0) | 0 (0) | 0.852 |
| Vomiting | 3 (1.7) | 0 (0) | 0 (0) | 2 (1.7) | 1 (2.9) | 0 (0) | 0 (0) | 0.977 |
| Dysgeusia | 22 (12.4) | 1 (4.2) | 0 (0) | 13 (11.2) | 7 (20.6) | 0 (0) | 1 (100) | 0.046 |
| Rhinorrhea | 75 (42.1) | 9 (37.5) | 2 (100) | 48 (41.4) | 15 (44.1) | 1 (100) | 0 (0) | 0.399 |
| Polypnea | 3 (1.7) | 1 (4.2) | 0 (0) | 2 (1.7) | 0 (0) | 0 (0) | 0 (0) | 0.908 |
| Abdominal pain | 4 (2.2) | 0 (0) | 0 (0) | 1 (0.9) | 2 (5.9) | 1 (100) | 0 (0) | <0.001 |
| Treatment | ||||||||
| Ambulatory | 176 (98.9) | 25 (100) | 2 (100) | 115 (99.1) | 32 (97.0) | 1 (100) | 1 (100) | 0.915 |
| Hospitalization | 2 (1.1) | 0 (0) | 0 (0) | 1 (0.9) | 1 (3.0) | 0 (0) | 0 (0) | |
| Intensive Care Unit | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Need of supplementary oxygen | ||||||||
| Total | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (3.0) | 0 (0) | 0 (0) | 0.495 |
| Nasal cannula | 1 (100) | 0 (0) | 0 (0) | 0 (0) | 1 (100) | 0 (0) | 0 (0) | - |
| HR (95% CI) | p-Value | |
|---|---|---|
| BMI a | 0.97 (0.86–1.09) | 0.56 |
| Previous COVID infections b | 0.45 (0.27–0.74) | 0.002 |
| Age c | 0.77 (0.60–0.99) | 0.04 |
| Male sex | 1.19 (0.83–1.72) | 0.35 |
| Antibody level after second dose d | 1.01 (0.81–1.25) | 0.94 |
| BNT162b2 | 1.73 (0.73–4.08) | 0.21 |
| CoronaVac | 1.93 (0.99–3.74) | 0.05 |
| Comorbidities e | 3.51 (1.66–7.43) | 0.001 |
| BNT162b2*comorbidities | 0.30 (0.06–1.56) | 0.15 |
| CoronaVac*comorbidities | 0.33 (0.13–0.81) | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Ibarguengoitia, M.E.; Rivera-Salinas, D.; Sarti, R.; Levi, R.; Mollura, M.; Garza-Silva, A.; Rivera-Cavazos, A.; Hernández-Ruíz, Y.G.; Barco-Flores, I.A.; González-Cantú, A.; et al. Efficacy of Six Different SARS-CoV-2 Vaccines during a Six-Month Follow-Up and Five COVID-19 Waves in Brazil and Mexico. Vaccines 2023, 11, 842. https://doi.org/10.3390/vaccines11040842
Romero-Ibarguengoitia ME, Rivera-Salinas D, Sarti R, Levi R, Mollura M, Garza-Silva A, Rivera-Cavazos A, Hernández-Ruíz YG, Barco-Flores IA, González-Cantú A, et al. Efficacy of Six Different SARS-CoV-2 Vaccines during a Six-Month Follow-Up and Five COVID-19 Waves in Brazil and Mexico. Vaccines. 2023; 11(4):842. https://doi.org/10.3390/vaccines11040842
Chicago/Turabian StyleRomero-Ibarguengoitia, Maria Elena, Diego Rivera-Salinas, Riccardo Sarti, Riccardo Levi, Maximiliano Mollura, Arnulfo Garza-Silva, Andrea Rivera-Cavazos, Yodira Guadalupe Hernández-Ruíz, Irene Antonieta Barco-Flores, Arnulfo González-Cantú, and et al. 2023. "Efficacy of Six Different SARS-CoV-2 Vaccines during a Six-Month Follow-Up and Five COVID-19 Waves in Brazil and Mexico" Vaccines 11, no. 4: 842. https://doi.org/10.3390/vaccines11040842
APA StyleRomero-Ibarguengoitia, M. E., Rivera-Salinas, D., Sarti, R., Levi, R., Mollura, M., Garza-Silva, A., Rivera-Cavazos, A., Hernández-Ruíz, Y. G., Barco-Flores, I. A., González-Cantú, A., Sanz-Sánchez, M. Á., Guimarães Júnior, M. H., Pozzi, C., Barbieri, R., Morales-Rodriguez, D. P., Texeira, M. M., & Rescigno, M. (2023). Efficacy of Six Different SARS-CoV-2 Vaccines during a Six-Month Follow-Up and Five COVID-19 Waves in Brazil and Mexico. Vaccines, 11(4), 842. https://doi.org/10.3390/vaccines11040842