
Communicating with Patients about COVID-19 Vaccination: A Qualitative Study on Vaccinators in Tuscany Region, Italy
 ,
,  , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting, Design and Population
2.2. Data Collection, Processing and Analysis
3. Results
3.1. Theme 1—Users’ Attitudes towards COVID-19 Vaccination
3.2. Theme 2—Factors Influencing Vaccine Confidence
3.2.1. Sub-Theme 2.1—Determinants of Vaccine Hesitancy: Individual and Group Influence; Contextual Influences; Vaccine/Vaccination Specific Issues
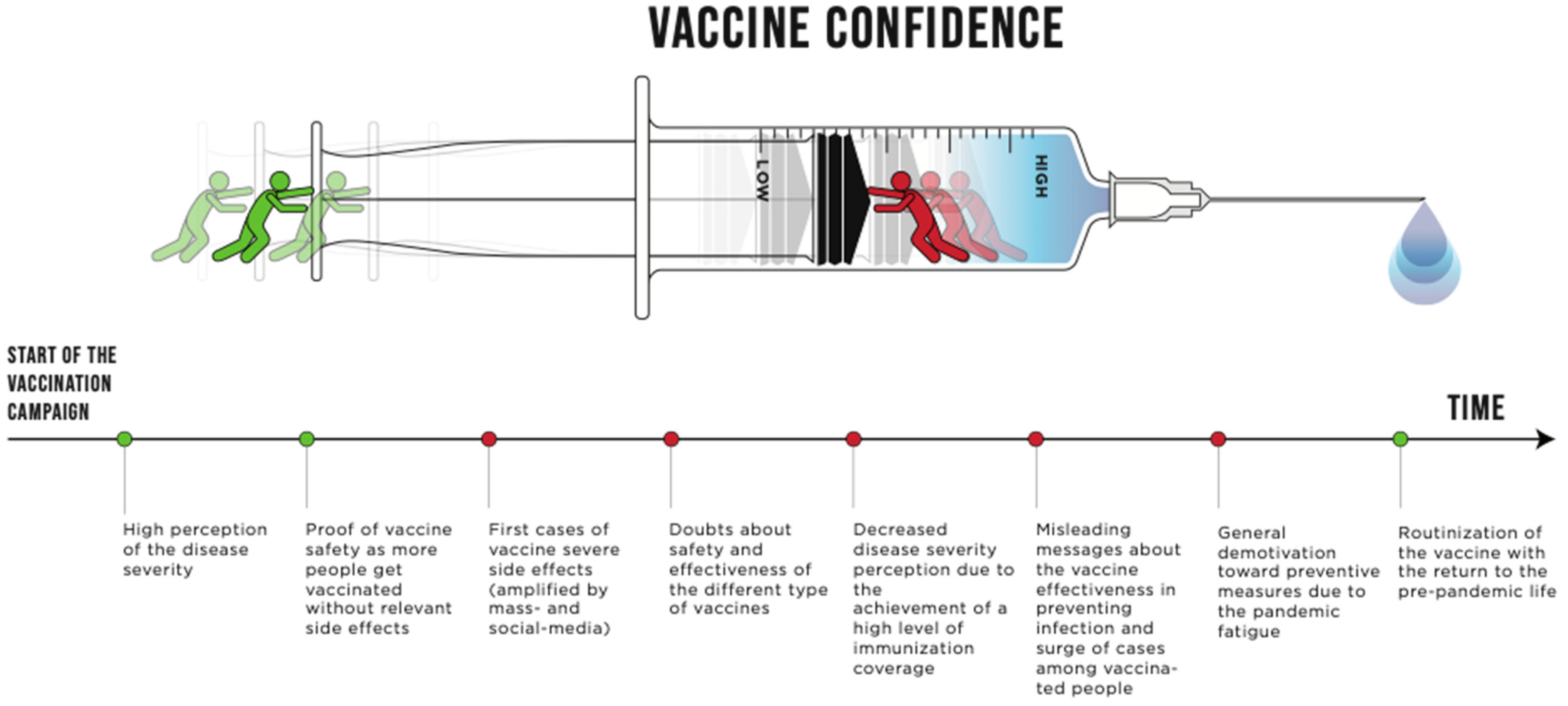
3.2.2. Sub-Theme 2.2—Changes in User Vaccine Confidence over the Course of the Vaccination Campaign
3.3. Theme 3—Information and Health Communication
3.3.1. Sub-Theme 3.1—COVID-19 Vaccine Knowledge and Information-Seeking Behaviors
3.3.2. Sub-Theme 3.2—The Impact of Institutional and Media Communication on Users’ Vaccine Perception and the Related Consequences on Vaccinators
3.4. Theme 4—Principles and Strategies for Dealing with Vaccine Hesitancy and Refusal
- Empathy: it emerged how crucial it was to have active and non-judgmental listening, to make the user feel understood, and to ask for users’ feedback about the information provided during the consultation. Furthermore, putting themselves on the same level as the user was regarded as a useful strategy by several vaccinators, with some of them saying that sharing their own experience and initial concerns about the vaccine reassured hesitant users. Lastly, another strategy reported to reassure hesitant users was to involve other users’ trusted medical health professionals so as to make them feel truly heard and understood.
- Transparency: transparency and honesty about scientific evidence was deemed essential to establishing a relationship of trust with users. Furthermore, it highlighted the importance of clearly admitting the uncertainty of evidence when they were not strong enough. This situation occurred, for example, in the case of the vaccination of pregnant women at the beginning of the vaccination campaign.
- Highlighting the balance between risks and benefits: vaccinators found it useful to stress the high level of vaccine efficacy and safety on the one hand while highlighting the risk of getting COVID-19 on the other hand. The use of everyday life examples, such as pointing out that the COVID-19 vaccine had similar or fewer risks than other commonly used drugs, was useful in overcoming fear and hesitation. Since one of the most common fears was the unknown long-term effects of the vaccine, pointing out that COVID-19 also may have long-term effects was proven useful. Furthermore, highlighting specific aspects in terms of personal or familiar clinical risks helped to make users understand that vaccination is particularly useful for their case.
- Adopting a personalized approach: a user-centered approach was frequently mentioned in dealing with vaccine hesitancy. This required exploring reasons behind hesitancy without being judgmental and understanding the user’s belief and attitude toward health and vaccines in order to adapt the communication style. If the user shows beliefs and values in line with vaccine recommendations, reporting scientific data and evidence was reported to be persuasive; in the case of contrasting convictions, emotional stories were reported to be more effective.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Overview. Available online: https://health.ec.europa.eu/vaccination/overview_en (accessed on 28 November 2022).
- Cicchetti, A.; Ruggeri, M.; Gitto, L.; Mennini, F.S. Extending influenza vaccination to individuals aged 50–64: A budget impact analysis. Int. J. Technol. Assess. Health Care 2010, 26, 288–293. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ten Threats to Global Health in 2019. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 15 February 2022).
- Eriksson, C.O.; Stoner, R.C.; Eden, K.B.; Newgard, C.D.; Guise, J.-M. The Association Between Hospital Capacity Strain and Inpatient Outcomes in Highly Developed Countries: A Systematic Review. J. Gen. Intern. Med. 2016, 32, 686–696. [Google Scholar] [CrossRef]
- Trentini, F.; Marziano, V.; Guzzetta, G.; Tirani, M.; Cereda, D.; Poletti, P.; Piccarreta, R.; Barone, A.; Preziosi, G.; Arduini, F.; et al. Pressure on the Health-Care System and Intensive Care Utilization During the COVID-19 Outbreak in the Lombardy Region of Italy: A Retrospective Observational Study in 43,538 Hospitalized Patients. Am. J. Epidemiol. 2021, 191, 137–146. [Google Scholar] [CrossRef]
- Scherer, L.D.; Shaffer, V.A.; Patel, N.; Zikmund-Fisher, B.J. Can the vaccine adverse event reporting system be used to increase vaccine acceptance and trust? Vaccine 2016, 34, 2424–2429. [Google Scholar] [CrossRef]
- Chou, W.-Y.S.; Budenz, A. Considering Emotion in COVID-19 Vaccine Communication: Addressing Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, H.-J.; Booy, R.; Aston, R.; Van Damme, P.; Schumacher, R.F.; Campins, M.; Rodrigo, C.; Heikkinen, T.; Weil-Olivier, C.; Finn, A.; et al. How to optimise the coverage rate of infant and adult immunisations in Europe. BMC Med. 2007, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.; Schamel, J.; Fisher, A.; Frew, P.M. Influences on Immunization Decision-Making among US Parents of Young Children. Matern. Child Health J. 2017, 21, 2178–2187. [Google Scholar] [CrossRef] [PubMed]
- Gust, D.A.; Darling, N.; Kennedy, A.; Schwartz, B. Parents With Doubts About Vaccines: Which Vaccines and Reasons Why. Pediatrics 2008, 122, 718–725. [Google Scholar] [CrossRef]
- Goldstein, S.; MacDonald, N.E.; Guirguis, S. Health communication and vaccine hesitancy. Vaccine 2015, 33, 4212–4214. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Butler, R.; MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Diagnosing the determinants of vaccine hesitancy in specific subgroups: The Guide to Tailoring Immunization Programmes (TIP). Vaccine 2015, 33, 4176–4179. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control; Translating Health Communications Project Consortium. Systematic Literature Review of the Evidence for Effective National Immunisation Schedule Promotional Communications: Insights into Health Communication; Publications Office: Stockholm, Sweden, 2012. [Google Scholar]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- WHO Strategic Communications Framework for Effective Communications. Geneva: World Health Organization. 2020. Available online: https://www.who.int/docs/default-source/documents/communicating-for-health/communication-framework.pdf (accessed on 28 November 2022).
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; et al. Strategies for Addressing Vaccine Hesitancy-A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; MacDonald, N.E.; Sage Working Group on Vaccine Hesitancy. Strategies intended to address vaccine hesitancy: Review of published reviews. Vaccine 2015, 33, 4191–4203. [Google Scholar] [CrossRef]
- Cerqua, A.; Di Stefano, R. When did coronavirus arrive in Europe? Stat. Methods Appl. 2021, 31, 181–195. [Google Scholar] [CrossRef]
- Lastrucci, V.; Lorini, C.; Del Riccio, M.; Gori, E.; Chiesi, F.; Sartor, G.; Zanella, B.; Boccalini, S.; Bechini, A.; Puggelli, F.; et al. SARS-CoV-2 Seroprevalence Survey in People Involved in Different Essential Activities during the General Lock-Down Phase in the Province of Prato (Tuscany, Italy). Vaccines 2020, 8, 778. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Paoli, S.; Biamonte, M.A.; Moscadelli, A.; Baggiani, L.; Nerattini, M.; Lastrucci, V.; Zanobini, P.; Lorini, C. COVID-19 and schools: What is the risk of contagion? Results of a rapid-antigen-test-based screening campaign in Florence, Italy. Int. J. Infect. Dis. 2021, 112, 130–135. [Google Scholar] [CrossRef]
- Reno, C.; Sanmarchi, F.; Stoto, M.A.; Fantini, M.P.; Lenzi, J.; Golinelli, D. The impact of health policies and vaccine rollout on the COVID-19 pandemic waves in Italy. Health Policy Technol. 2022, 11, 100604. [Google Scholar] [CrossRef]
- Decreto Del Ministero Della Salute 12 Marzo 2021 (Approvazione Del Piano Strategico Nazionale Dei Vaccini per La Prevenzione Delle Infezioni Da SARS-CoV-2 Costituito Dal Documento Recante «Elementi Di Preparazione Della Strategia Vaccinale», Di Cui al Decreto 2 Gennaio 2021 Nonche’ Dal Documento Recante «Raccomandazioni Ad Interim Sui Gruppi Target Della Vaccinazione Anti SARS-CoV-2/COVID-19» Del 10 Marzo 2021); Istituto Poligrafico e Zecca dello Stato: Rome, Italy, 2021; Volume 21A01802.
- European Centre for Disease Prevention and Control. Let’s Talk about Hesitancy; ECDC: Stockholm, Sweden, 2016; Available online: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/lets-talk-about-hesitancy-vaccination-guide.pdf (accessed on 28 November 2022).
- Lastrucci, V.; Collini, F.; Forni, S.; D’Arienzo, S.; Di Fabrizio, V.; Buscemi, P.; Lorini, C.; Gemmi, F.; Bonaccorsi, G. The indirect impact of COVID-19 pandemic on the utilization of the emergency medical services during the first pandemic wave: A system-wide study of Tuscany Region, Italy. PLoS ONE 2022, 17, e0264806. [Google Scholar] [CrossRef] [PubMed]
- Lastrucci, V.; Bonaccorsi, G.; Forni, S.; D’Arienzo, S.; Bachini, L.; Paoli, S.; Lorini, C.; Gemmi, F. The indirect impact of COVID-19 large-scale containment measures on the incidence of community-acquired pneumonia in older people: A region-wide population-based study in Tuscany, Italy. Int. J. Infect. Dis. 2021, 109, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, 210–221. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348, Correction in 2021, 5, 960. [Google Scholar] [CrossRef] [PubMed]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef]
- Lee, S.K.; Sun, J.; Jang, S.; Connelly, S. Misinformation of COVID-19 vaccines and vaccine hesitancy. Sci. Rep. 2022, 12, 13681. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.-A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, e110. [Google Scholar] [CrossRef]
- Momplaisir, F.; Haynes, N.; Nkwihoreze, H.; Nelson, M.; Werner, R.M.; Jemmott, J. Understanding Drivers of COVID-19 Vaccine Hesitancy Among Blacks. Clin. Infect. Dis. 2021, 73, 1784–1789. [Google Scholar] [CrossRef]
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Jennings, W.; Stoker, G.; Bunting, H.; Valgarðsson, V.; Gaskell, J.; Devine, D.; McKay, L.; Mills, M. Lack of Trust, Conspiracy Beliefs, and Social Media Use Predict COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 593. [Google Scholar] [CrossRef] [PubMed]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.A.; Failla, G.; Puleo, V.; Melnyk, A.; Lontano, A.; Ricciardi, W. Social media and attitudes towards a COVID-19 vaccination: A systematic review of the literature. Eclinicalmedicine 2022, 48. [Google Scholar] [CrossRef] [PubMed]
- Aquino, F.; Donzelli, G.; De Franco, E.; Privitera, G.; Lopalco, P.L.; Carducci, A. The web and public confidence in MMR vaccination in Italy. Vaccine 2017, 35, 4494–4498. [Google Scholar] [CrossRef] [PubMed]
- Gahr, P.; DeVries, A.S.; Wallace, G.; Miller, C.; Kenyon, C.; Sweet, K.; Martin, K.; White, K.; Bagstad, E.; Hooker, C.; et al. An Outbreak of Measles in an Undervaccinated Community. Pediatrics 2014, 134, e220–e228. [Google Scholar] [CrossRef]
- Jama, A.; Ali, M.; Lindstrand, A.; Butler, R.; Kulane, A. Perspectives on the Measles, Mumps and Rubella Vaccination among Somali Mothers in Stockholm. Int. J. Environ. Res. Public Health 2018, 15, 2428. [Google Scholar] [CrossRef]
- Van Der Linden, S.; Roozenbeek, J.; Compton, J. Inoculating Against Fake News About COVID-19. Front. Psychol. 2020, 11, 566790. [Google Scholar] [CrossRef]
- Gilles, I.; Bangerter, A.; Clémence, A.; Green, E.G.T.; Krings, F.; Staerklé, C.; Wagner-Egger, P. Trust in medical organizations predicts pandemic (H1N1) 2009 vaccination behavior and perceived efficacy of protection measures in the Swiss public. Eur. J. Epidemiol. 2011, 26, 203–210. [Google Scholar] [CrossRef]
- Gangarosa, E.; Galazka, A.; Wolfe, C.; Phillips, L.; Miller, E.; Chen, R. Impact of anti-vaccine movements on pertussis control: The untold story. Lancet 1998, 351, 356–361. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Chanel, O.; Luchini, S.; Massoni, S.; Vergnaud, J.-C. Impact of information on intentions to vaccinate in a potential epidemic: Swine-origin Influenza A (H1N1). Soc. Sci. Med. 2011, 72, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, F.P.; Stefanizzi, P.; Brescia, N.; Lattanzio, S.; Martinelli, A.; Tafuri, S. COVID-19 vaccination hesitancy in Italian healthcare workers: A systematic review and meta-analysis. Expert Rev. Vaccines 2022, 21, 1289–1300. [Google Scholar] [CrossRef] [PubMed]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Aw, J.; Seah, S.S.Y.; Seng, B.J.J.; Low, L.L. COVID-19-Related Vaccine Hesitancy among Community Hospitals’ Healthcare Workers in Singapore. Vaccines 2022, 10, 537. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Behavioural Considerations for Acceptance and Uptake of COVID-19 Vaccines: WHO Technical Advisory Group on Behavioural Insights and Sciences for Health, Meeting Report, 15 October 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/337335/9789240016927-eng.pdf?sequence=1&isAllowed=y (accessed on 28 November 2022).
- Lastrucci, V.; Lorini, C.; Del Riccio, M.; Gori, E.; Chiesi, F.; Moscadelli, A.; Zanella, B.; Boccalini, S.; Bechini, A.; Puggelli, F.; et al. The Role of Health Literacy in COVID-19 Preventive Behaviors and Infection Risk Perception: Evidence from a Population-Based Sample of Essential Frontline Workers during the Lockdown in the Province of Prato (Tuscany, Italy). Int. J. Environ. Res. Public Health 2021, 18, 13386. [Google Scholar] [CrossRef]
- Lastrucci, V.; Lorini, C.; Stacchini, L.; Stancanelli, E.; Guida, A.; Radi, A.; Morittu, C.; Zimmitti, S.; Alderotti, G.; Del Riccio, M.; et al. Determinants of Actual COVID-19 Vaccine Uptake in a Cohort of Essential Workers: An Area-Based Longitudinal Study in the Province of Prato, Italy. Int. J. Environ. Res. Public Health 2022, 19, 13216. [Google Scholar] [CrossRef]
- Nicolo, M.; Kawaguchi, E.S.; Ghanem-Uzqueda, A.; Kim, A.E.; Soto, D.; Deva, S.; Shanker, K.; Rogers, C.; Lee, R.; Casagrande, Y.; et al. Characteristics associated with COVID-19 vaccination status among staff and faculty of a large, diverse University in Los Angeles: The Trojan Pandemic Response Initiative. Prev. Med. Rep. 2022, 27, 101802. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Sample n | 30 |
|---|---|
| Median age (interquartile range) | 37 (31–44) |
| Female sex n (%) | 14 (46.7) |
| Number of vaccinations administered n (%) | |
| 1000–2000 | 17 (56.7) |
| 2000–5000 | 6 (20) |
| 5000–10,000 | 4 (13.3) |
| >10,000 | 3 (10) |
| Number of patients * (mean ± standard deviation) | 1405 ± 253 |
| Previous experience with other vaccination campaigns n (%) | 19 (63.3) |
| Urbanization level area n (%) | |
| Urban | 10 (33.3) |
| Suburban/rural | 20 (66.7) |
| Type of vaccinators ** n (%) | |
| Vaccination HUB | 12 (40) |
| Hospital | 3 (10) |
| Special continuity care units | 6 (20) |
| General practitioners | 12 (40) |
| Theme 1. Users’ Attitudes towards COVID-19 Vaccination |
|---|
| - There are several type of user attitudes: those who are enthusiastic about the vaccine, they want to be vaccinated immediately, and they would take also an extra dose, if it were possible; then there are the passive users, who have been told that “this is the rule and it has to be done” so they do it without expressing any particular opinion about vaccine, if it has to be done it has to be done; then there are the reassurance seekers, those who are afraid that the vaccine will hurt them, but in the end they do get vaccinated; there are the opposers, who don’t want to get it for ethical or political reasons...basically, these are the categories (Vaccinator n. 18, G.P.). - (…) the majority of people trusted the doctors, the health system and the safety of the vaccine. (Vaccinator n. 3, HUB). - (People) came confident and happy to have this chance (to get vaccinated) in order to come back to social daily life in the most normal conditions as possible. For most people, the goal was this (to return to normal life) (Vaccinator n. 11, HUB). - (...) youngsters, like those in their twenties, were receptive and willing to do it. Teenagers are the ones who have made a very rational thought: “I want to get back to my life, that’s what the vaccine is for, so I am gonna do it” (Vaccinator n. 18, G.P.). - (…) some people just follow the rules as they were dictated to them; those subjects act without making any criticisms or assessment: if the rule says a thing has to be done, they just make it (Vaccinator n. 17, G.P.). - They are not contrary to the vaccine because of the information they had read on the Internet. The hesitant people are looking for answers, so if you give them the right amount of time and attention, they will eventually become users convinced of what they are doing; it takes time, but the hesitant people don’t want per se to do it...they just need an extra communicative effort (Vaccinator n. 10, HUB). - (…) there were users that were afraid; I mean, they did not distrust the health system or the health worker, but they had a lot of apprehension and doubts generated by the news (Vaccinator n. 11, HUB). - Some waited because they were afraid, they said “now let’s see how many people get vaccinated, and let’s see if they will have any issues” (Vaccinator n. 23, G.P.). - Covid-19 vaccines have been administered in a short time frame, so (they say) “Alt! before doing it myself, I will think about it”; it’s a very selfish kind of argument based on the conviction that other vaccines have been tested on people, whereas Covid-19 vaccine was not, so (they said) “why should I be the guinea pig?” (Vaccinator n. 15, HUB). - There were people who came for vaccination and told me “I only get vaccinated because I have to, otherwise I can’t work” (…) these patients were the most difficult to handle (Vaccinator n. 14, USCA). - Telling them (users ideologically opposed to the vaccine) that vaccination is beneficial for their health and can save their lives it’s not compelling; the only way is to affirm that there are norms that require the vaccination, and those laws must be obeyed; they may get vaccinated only because of that (Vaccinator n. 6, HUB). - This small percentage of users (ideologically opposed to the vaccine) is firmly convinced.. it will be almost impossible to change their minds; they are probably the ones who are still not vaccinated (Vaccinator n. 1, HUB). - The “no-vax” people wouldn’t accept any form of dialogue: they yell at you, tell you to f**k yourself, and say you bye-bye; in my opinion, there are limited activities that can be done with them (Vaccinator n. 3, HUB). - They are often people with an average level of education—neither illiterate nor graduates... they are neither very poor nor very rich, so let’s say (that they belong to) the middle class of the population (Vaccinator n. 18, G.P.). - The “no-vax” people were users with a medium-high cultural level—usually not in the medical field; they presume to have all the answers without any needing to consult you (Vaccinator n. 18, G.P.). |
| B | P | BARRIERS | PROMOTERS | ||
|---|---|---|---|---|---|
| N. vaccinators | |||||
| SOCIO ECONOMIC GROUP | Age | 22 | 21 | - 45–60 years | - Over 70 years - Under 30 years |
| Race/ethnicity | 3 | - | - Residents and migrants from East Europe | ||
| Birthplace | 3 | - | - Hard-to-reach migrant populations | ||
| Income/SES | 1 | 5 | - Lower-middle class | - Precarious working conditions - Economic migrant | |
| Marital status/family composition | - | - | |||
| Education | 8 | 1 | - Average to good educational background/level (excluded education in the health science fields) | - Low education level | |
| Occupation | - | 2 | - Healthcare workers | ||
| Language proficiency | - | - | |||
| Family decision making | 4 | 2 | - Having a family member ideologically opposed to the vaccination (in the case of elderly and adolescent vaccination) | - Having a family member vaccine confident (in the case of elderly and adolescent vaccination) | |
| Access to health care | - | - | |||
| Health status | 9 | 2 | - Pregnancy - Allergies and taking pharmaceuticals for other illnesses - Comorbidities (cardiologic, rare and autoimmune diseases) - Frail users | - Frail users - People who live in nursing home | |
| Family size | - | - | |||
| RELIGION/CULTURE/GENDER | Religious affiliation | - | - | ||
| Cultural | 2 | - Ethical reasons | |||
| Gender | - | - | |||
| POLITICS/POLICIES | Politics | 3 | - | - Government distrust - Supporting political parties that are against policies promoting vaccination and containment measures | |
| Policies | 8 | 14 | - Conflicting directives - Work and social restrictions foreseen for the unvaccinated | - Work and social restrictions foreseen for the unvaccinated | |
| INFLUENTIAL LEADERS AND INDIVIDUALS | Influential leaders and individuals | 1 | - | - Influential religious leaders followed by some migrant communities | |
| COMMUNICATION AND MEDIA ENVIRONMENT | Access to information | - | 5 | - Easy access to information from mass-media - Institutional communication campaigns | |
| Mass Media (use and influence) | 19 | - | - Infodemia - Fake news - Misinformation/disinformation from social/mass-media - Sensationalistic type of journalism - Institutional communication campaigns | ||
| PHARMACEUTICAL INDUSTRY | Pharmaceutical Industry | 11 | - | - Conspiracy theory | |
| HISTORICAL INFLUENCES | Historical influences | - | - | ||
| GEOGRAPHIC BARRIERS | Place of residence | - | - | ||
| RISK/BENEFIT (SCIENTIFICALLY BASED) | Use of evidence | - | 4 | - Seeking medical evidence from official sources | |
| Trust in evidence | 2 | 1 | - Distrust in the scientific process | - Confidence in science | |
| VACCINATION SCHEDULE | Schedule | 2 | - | - Unclear schedule for those who had previously experienced COVID-19 (early stages of the campaign) - Not having clear whether further booster doses would be needed in the future | |
| MODE OF ADMINISTRATION | Mode of administration | 2 | - | - Agophobia | |
| MODE OF DELIVERY | Campaign | 2 | 3 | - Rigid rules for appointment scheduling in the early stages of the vaccination campaign - The possibility to book the vaccination appointment only online in the early stages of the vaccination campaign | - Easy rescheduling of vaccination appointment - Open access and evening opening of the vaccination HUBs - Cooperation between primary care services for the vaccination of the hard-to-reach populations |
| INTRODUCTION OF A NEW VACCINE OR NEW FORMULATION | Introduction of a new vaccine or a new formulation | 17 | - | - New technology in the vaccine - Rapid development of the vaccine - Absence of real world-data on vaccine side-effects | |
| RELIABILITY OF VACCINE SUPPLY | Supply | - | - | ||
| ROLE OF HEALTHCARE PROFESSIONALS | Patient communication | - | 16 | - Involving other trusted health professionals in the decision-making process - Transparent and honest communication of evidence - Empathy and active and non-judgmental listening - Sharing own experience and real stories about the vaccination | |
| Vaccination expectations | 10 | - | - The unmet expectation that the vaccine would prevent SARS-CoV-2 infection | ||
| Organizational culture | - | - | |||
| Place of work | - | - | |||
| COST | Financial | - | - | ||
| Time | - | - | |||
| Administrative | - | - | |||
| Access | - | - | |||
| TAILORING VACCINES/VACCINATION TO NEEDS | Options | 11 | - | - Concerns about the possibility of using different types of vaccines | |
| EXPERIENCE WITH PAST VACCINATION | Vaccination behavior | 2 | 1 | - Having refused other adult vaccinations | - Having received the flu vaccine |
| RISK/BENEFITS (PERCEIVED /HEURISTICS) | Susceptibility to disease | 3 | 4 | - Not believing in being at risk of contracting the infection | - Fear of the infection - COVID-19 personal experiences (or in the closest people) |
| Disease severity | 3 | 11 | - Not believing in being at risk of severe COVID-19 - Fear of the vaccine greater than fear of the disease | - High perception of the risk of the disease - Dramatic memories of COVID-19 deaths observed in 2020 - Severe COVID-19 personal experiences (or in the closest people) - Perception of the severity of the disease in the elderly and in other population subgroups at risk | |
| Vaccine safety | 25 | 4 | - Negative experience with previous doses - Fear of long-term reactions (e.g., genome modifications, cancer, fertility, etc.) - Fear of side-effects - Concerns about the composition of the vaccine (mRNA) - Safety in pregnancy and breast-feeding | - Vaccine confidence attitude | |
| Vaccine efficacy | 4 | 9 | - Lack of protection against the infection | - Awareness of vaccine efficacy in preventing severe COVID-19 | |
| PERSONAL EXPERIENCE WITH AND TRUST IN HEALTH SYSTEM AND PROVIDER | Distrust/fear of vaccine due to | 7 | - | - Distrust in the healthcare system - Distrust of the G.P.s’ ability to identify a conspiracy | |
| Satisfaction with public health system | - | 4 | - Trust and reliance on the doctor’s recommendation - Confidence in the healthcare system | ||
| KNOWLEDGE/AWARENESS OF WHY/WHERE /WHAT/WHEN VACCINES ARE NEDEED | Knowledge—Vaccination | 2 | 2 | - Lack of awareness of the steps and requirements necessary to have a commercially approved vaccine - Lack of vaccine literacy skills | - Parents well informed about their children’s vaccination - Being aware of vaccine’s benefits |
| Knowledge—General Health | 2 | - | - Low health literacy level | ||
| BELIEFS, ATTITUDES AND MOTIVATION ABOUT HEALTH AND PREVENTION | Attitude | 4 | 2 | - Risk-taking inclination - Ideologically opposed to conventional medicine | - Trust in science and in the scientific method |
| Beliefs | 4 | - | - Belief in complementary and alternative therapies - Belief that drugs and conventional medicine are harmful | ||
| Motivation/Practices | 1 | - | - Use of alternative therapies for preventing/treating COVID-19 | ||
| IMMUNISATION IS A SOCIAL NORM VS. IMMUNIZATION IS NOT NEEDED/ HARMFUL | Need for vaccine | 2 | 2 | - Considering the vaccine unnecessary | - Being aware that the vaccine protects one’s own inner circle - Awareness of community immunity mechanism and why it is needed to end the pandemic crisis - Attitude to respect the recommendation from the institution |
| Theme 2. Factors Influencing Vaccine Confidence |
|---|
| 2.1.—Determinants of Vaccine Hesitancy: Individual and Group Influence; Contextual Influences; Vaccine/Vaccination Specific Issues |
| - Long-term fears were due to the fact that the vaccine was new and the belief that it was not tested enough (people said) “I am still fertile, who knows what kind of children I may have”, “I am worried about the possible changes in my DNA”, “who knows what will happen in thirty years when my children will be grown up”(Vaccinator n. 14, USCA). - It was a new vaccine, so people were really, really worried (Vaccinator n. 10, HUB). - I remember people saying “Uhm, but the vaccine is still experimental” (Vaccinator n. 11, HUB). - Some people asked themselves “What’s the point of getting vaccinated if I will get COVID-19 anyway” (Vaccinator n. 9, Hospital and HUB). - In my opinion, there has been an excess of information, which created confusion among people. From an institutional and a regulatory point of view, they have not been capable of giving the required few clear rules…also from a media point of view, the virologists in TV shows who said everything and more…for example, until the day before, it was said that the surgical mask is effective and then, the day after, it was no longer protective, many people thought “how is it possible that on 23 July the surgical mask is fine and on the 24th it is not adequate anymore? There must be something wrong here”; and this mechanism arouse suspicions, especially in people with a lower level of trust (Vaccinator n. 17, G.P.). - News about vaccines were continually and literally thrown at people, but they were not able to digest them; too many voices wanted to take part in this discussion; all this led to debates that fuelled insecurity in people’s minds (Vaccinator n. 1, HUB). - Some users said “I only get vaccinated because I have to, otherwise I can’t go to work” (Vaccinator n. 15, HUB). - At the beginning (of the vaccination campaign), we had a great adherence and the users we vaccinated were eager to get the vaccine, they had no hesitation... they perceived a high risk of COVID-19 (Vaccinator n. 4, HUB). - The vaccination campaign was well organized as it attempted to reach as many people as possible by opening the HUBs in the evening and allowing users to get vaccinated without prior booking...all this worked well (Vaccinator n. 11, HUB). |
| 2.2.—Changes in user vaccine confidence over the course of the vaccination campaign |
| - (Vaccine confidence) changed in relation to COVID-19 risk perception: when the risk perception was high, vaccination was almost seen as it was the only way of salvation..everyone competed to get vaccinated first. Then, as time went by and risk perception declined, the vaccine almost became a hassle (Vaccinator n. 2, HUB). - (Vaccine confidence) has changed over the time...as the vaccine was given to more and more people, people realized that the vaccine doesn’t cause side effects and prevents people from getting sick or getting the severe forms (Vaccinator n. 3, HUB). - As the time went by and we went on with the third and the fourth doses, the proportion of sceptics increased..it seems that users had a higher perception of the risks of the vaccine rather than of those related to the disease...users were more hesitant (Vaccinator n. 4, HUB). - The negative news were amplified by the press; for example, the case of the side effects of AstraZeneca vaccine...this created huge concern in users (Vaccinator n. 8, HUB). - (…) a man, who previously received two doses of Pfizer vaccine, refused to receive the Moderna vaccine for the 3rd dose because he was afraid of possible side effects, he insisted to get the Pfizer vaccine (Vaccinator n. 5, HUB). - People were not well informed about the reasons why get the vaccine, it was not clearly explained the difference between preventing the infection and preventing the severe consequences...especially during the omicron wave it has been observed that (the vaccine) does not prevent the infection (Vaccinator n. 9, Hospital and HUB). |
| Theme 3. Information and Health Communication |
|---|
| 3.1.—COVID-19 Vaccine Knowledge and Information Seeking Behaviors |
| - The main sources of information were social media and television (Vaccinator n. 8, HUB). - In my opinion, TV was the main source of information…surely this medium reached the majority of people as it was switched on every day, at any time; moreover, it reached also those who did not use the web. Other sources of information were: the web, newspapers, radio, and at the very end the direct contact with the family doctor (Vaccinator n. 2, HUB). - Without any doubts, users mostly get their information from unofficial sources (Vaccinator n. 1, HUB). - Mostly they get information from Internet and television; I believe that older people and foreigners also get information from relatives and friends (Vaccinator n. 5, HUB). - (people seek information) only on Google…older people get informed from the TV. Youngsters, but also the not-so-young, “googled” everything…with “Google” I mean the use of Internet in general, including social-media. Government and institutions should push more and more on establishing a relationship (with users) through social media (Vaccinator n. 12, USCA). - (…) in the end, people look for what they are interested in and the answers they want to hear (Vaccinator n. 15, HUB). - The “no-vax” people seek information on the Internet by searching for facts they like to read…we all like to read things that confirm our own thoughts (Vaccinator n. 6, HUB). - The “no-vaxxers” are hyper-informed by sources that are selected by them...and they know very well that (these sources) are unreliable; they speak their own language, they “ring their bells”...they like that sound, they don’t want to hear another one (Vaccinator n. 12, USCA). - The weakest element has been the lack of integration with general practitioners and primary care services; the general practitioners represent the capillarity of the health system, so as to reach individuals with a trusted face (Vaccinator n. 1, HUB). |
| 3.2.—The Impact of Institutional and Media Communication on Users’ Vaccine Perception and the Related Consequences on Vaccinators |
| - The several fake news spread on Telegram and Facebook were terrible. Especially users in their fifties were the more vulnerable to fake news, they were not able to discern a trusted source of information, and they believe in everything they read…they were those who mainly believe in conspiracy theories (Vaccinator n. 9, Hospital and HUB). - We’ve seen a huge amount of information, an infodemia. People’ve been intoxicated with information (Vaccinators n. 1, HUB). - (…) patients told me “we no longer know what to believe anymore”, there are too much information, both good and bad, obviously the bad is more problematic, but the good is also excessive; many people told me “I just don’t listen to the news anymore because it makes me anxious and it’s not clear what is necessary to do”, this has certainly created a lot of confusion in people (Vaccinator n. 19, G.P. and USCA). - During the vaccination campaign, everybody talked about that, everybody had to have an opinion about the vaccine and had to talk about it…more or less everybody had an idea, whether this idea was correct or not (Vaccinator n. 10, HUB). - Contrasting institutional messages generates confusion in users as well as in the health operators who had to deal with them and explain the reasons of the frequent change of directions…the users may think “you all are crazy!” (Vaccinator n. 11, HUB). - Most of the people don’t understand the scientific process and institutions were not able to make people understand why it was necessary to backtrack on some of the decisions made (Vaccinator n. 2, HUB). - The awareness-raising campaign was not done on a specific target group but on the entire population..it is difficult to involve all the age groups at the same time, they are receptive to different communication mechanisms (Vaccinator n. 1, HUB). |
| Theme 4—Principles and Strategies for Dealing with Vaccine Hesitancy and Refusal |
|---|
| - (with hesitant user) I try to establish a relationship of trust that can make them feeling safe (Vaccinator n. 2, HUB). - I tried to empathize with their fears, telling them that I have been afraid too, and that fear is a human reaction that must not be criticized but accepted (…) I mainly try to establish a close relationship (with the users) putting myself on the same level and provide accurate and transparent information whenever they had doubts (Vaccinator n. 1, HUB). - I told them (to the users): “I got vaccinated in January, I actually was among the first operators getting vaccinated, and thus I certainly had some fears and apprehensions, as it happens every time you try something new, but there were solid data (about COVID-19 vaccination) reliability and security. Even though I had some fear of getting vaccinated, I certainly had a greater fear of getting the disease”. This was something everyone agreed on (Vaccinator n. 3, HUB). - I tried to understand their main doubts and concerns, I tried to be as clear and understandable as possible, and surely I asked their feedbacks…I mean, when I was explaining something I checked that everything was comprehended. I used simple examples to describe the virus structure and how the vaccine works...I tried to simplify as much as possible (Vaccinator n. 10, HUB). - It is important to make them (hesitant users) understand that things are transparent, that the information is open for everyone, and that there are no hidden facts (Vaccinator n. 4, HUB). - In the case when I actually had no certainties and therefore I could not give any certainties (to the users), I spoke with honesty about the situation with complete honesty…this was helpful (Vaccinator n. 21, G.P.). - I always try to compare risks and benefits, let’s say they are concerned about the long-term consequences of the vaccine, I explained that there is no scientific evidence to fear the long-term consequences of the vaccine, whereas long-term consequences from the virus have to be feared (Vaccinator n. 2, HUB). - (I focused) on the benefits of vaccination compared with its side effects (such as fever), such as how important the vaccination is to protect from severe forms of the disease; I tried to make people understand that getting COVID-19 could result in severe consequences for their health (Vaccinator n. 15, HUB). - We try to make people understand that it is a balance between the expected benefit of protection and the consequences of the disease, including the long-term ones...stressing the fact that we don’t know exactly the long term consequences of the disease (…) there were always concerns about the long-term consequences of the vaccine, but we still don’t know what the long-term consequences of COVID-19 are (Vaccinator n. 11, HUB). - Sometimes an effective strategy for convincing a person to go ahead [with vaccination] is to involve other trusted professionals (…) there have been times when I have contacted their doctors just to give them a reassurance (Vaccinator n. 1, HUB). - In some cases I showed and compared the aspirin leaflet with that of the vaccine (Vaccinator n. 6, HUB). - Comparisons with other drugs considered harmless were also useful, highlighting the fact that in case they had taken these drugs in the past they had been exposed to similar risks of the vaccination (Vaccinator n. 21, G.P.). - With hesitant users the counselling was quite demanding, I assessed their risk both in terms of social interaction and clinical history, trying to highlight their personal risk. I remember a case of a hesitant couple, where one of the two had more indications to get the vaccine (…) in this case I remember telling to the husband “let’s say your wife might even wait for the moment as she’s a housewife and almost never leaves the house, but you have heart issues, you are diabetic, you work in a school, your situation cannot wait”...it is very useful to make them understand their own personal risks…I really have a personalised approach to the vaccine consultation (Vaccinator n. 19, G.P. and USCA). - In my opinion, people mostly don’t care about collective health, they mainly look at their own, they don’t care if vaccination reduces virus transmission, they just care about their well-being. From this point of view, the average person who comes to get vaccinated is very selfish (Vaccinator n. 9, Hospital and HUB). - (referring to the use of communication support materials) during consultation is much more important the face-to-face dialogue, people need to feel that they are talking to a reliable person who gives them a sense of security (Vaccinator n. 2, HUB). - (referring to the users ideologically opposed to the vaccine) there are no effective approaches, it’s like playing chess with a pigeon, they don’t care, you can tell them anything and they won’t change their opinion. It is a waste of breath (…) there is nothing that can convince them (Vaccinator n. 9, Hospital and HUB). - (referring to the users ideologically opposed to the vaccine) I tried as I did with the other users (…) but for them it is as if the earth was flat (Vaccinator n. 2, HUB). - They were convinced that on this particular issue (the vaccine) we (the doctors) have been fooled...in the sense that we were deceived too so we were doing things in good faiths. According to one of these theories, I was also manipulated, so they were not angry with me (Vaccinator n. 18, G.P.). - In my experience, there are no proper communicative approaches with the “no-vax” users…sometimes it seems they just want to provoke or to threaten us. Therefore, I think the best way for dealing with such users is avoiding any dismissal or direct confrontation, while at the same time try to provide concise recommendations...hoping that this may build some sort of trust for future occasions (Vaccinator n. 11, HUB). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alderotti, G.; Corvo, M.F.; Buscemi, P.; Stacchini, L.; Giorgetti, D.; Lorini, C.; Bonaccorsi, G.; Pinilla, M.J.C.; Lastrucci, V. Communicating with Patients about COVID-19 Vaccination: A Qualitative Study on Vaccinators in Tuscany Region, Italy. Vaccines 2023, 11, 223. https://doi.org/10.3390/vaccines11020223
Alderotti G, Corvo MF, Buscemi P, Stacchini L, Giorgetti D, Lorini C, Bonaccorsi G, Pinilla MJC, Lastrucci V. Communicating with Patients about COVID-19 Vaccination: A Qualitative Study on Vaccinators in Tuscany Region, Italy. Vaccines. 2023; 11(2):223. https://doi.org/10.3390/vaccines11020223
Chicago/Turabian StyleAlderotti, Giorgia, Martina Felicia Corvo, Primo Buscemi, Lorenzo Stacchini, Duccio Giorgetti, Chiara Lorini, Guglielmo Bonaccorsi, Maria José Caldés Pinilla, and Vieri Lastrucci. 2023. "Communicating with Patients about COVID-19 Vaccination: A Qualitative Study on Vaccinators in Tuscany Region, Italy" Vaccines 11, no. 2: 223. https://doi.org/10.3390/vaccines11020223
APA StyleAlderotti, G., Corvo, M. F., Buscemi, P., Stacchini, L., Giorgetti, D., Lorini, C., Bonaccorsi, G., Pinilla, M. J. C., & Lastrucci, V. (2023). Communicating with Patients about COVID-19 Vaccination: A Qualitative Study on Vaccinators in Tuscany Region, Italy. Vaccines, 11(2), 223. https://doi.org/10.3390/vaccines11020223