
Serological Responses up to 9 Months following COVID-19 mRNA Vaccination in Residents and Health-Care Workers of Long-Term Care Facilities: A Multicenter Prospective Cohort Study in Northern Italy
 ,
,  , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
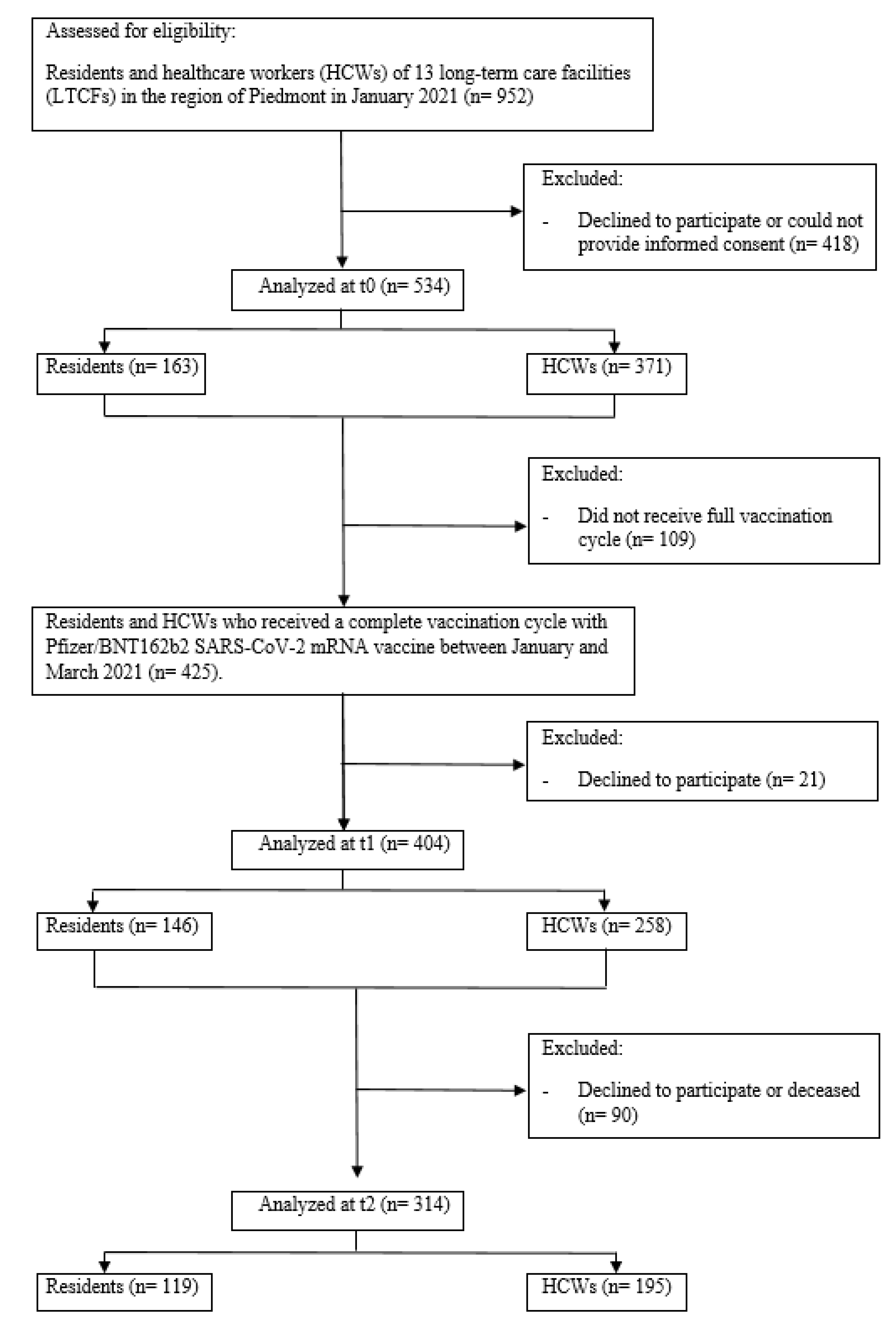
2.1. Study Design, Participants and Data Collection
2.2. Laboratory Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vicentini, C.; Bazzolo, S.; Gamba, D.; Zotti, C.M. Analysis of the Fatality Rate in Relation to Testing Capacity during the First 50 Days of the COVID-19 Epidemic in Italy. Am. J. Trop. Med. Hyg. 2020, 103, 2382–2390. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. Report esteso ISS COVID-19: Sorveglianza, impatto delle infezioni ed efficacia vaccinale. In Aggiornamento Nazionale 2/11/2022; Istituto Superiore di Sanità: Rome, Italy, 2022. [Google Scholar]
- Shrotri, M.; Krutikov, M.; Palmer, T.; Giddings, R.; Azmi, B.; Subbarao, S.; Fuller, C.; Irwin-Singer, A.; Davies, D.; Tut, G.; et al. Vaccine Effectiveness of the First Dose of ChAdOx1 NCoV-19 and BNT162b2 against SARS-CoV-2 Infection in Residents of Long-Term Care Facilities in England (VIVALDI): A Prospective Cohort Study. Lancet Infect. Dis. 2021, 21, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Amore, S.; Puppo, E.; Melara, J.; Terracciano, E.; Gentili, S.; Liotta, G. Impact of COVID-19 on Older Adults and Role of Long-Term Care Facilities during Early Stages of Epidemic in Italy. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bordino, V.; Vicentini, C.; D’Ambrosio, A.; Quattrocolo, F.; Novati, R.; Sticchi, C.; Bersani, M.; Fedeli, U.; Fabbri, L.; Brusaferro, S.; et al. Burden of Healthcare-Associated Infections in Italy: Incidence, Attributable Mortality and Disability-Adjusted Life Years (DALYs) from a Nationwide Study, 2016. J. Hosp. Infect. 2021, 113, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore di Sanità. Sorveglianza COVID-19—Sorveglianza strutture residenziali socio-sanitarie nell’emergenza COVID-19. In Report Nazionale Andamento Temporale Dell’epidemia di COVID-19 21 December 2020–18 September 2022; Istituto Superiore di Sanità: Rome, Italy, 2022. [Google Scholar]
- Nace, D.A.; Kip, K.E.; Mellors, J.W.; Peck Palmer, O.M.; Shurin, M.R.; Mulvey, K.; Crandall, M.; Sobolewski, M.D.; Enick, P.N.; McCormick, K.D.; et al. Antibody Responses after mRNA-Based COVID-19 Vaccination in Residential Older Adults: Implications for Reopening. J. Am. Med. Dir. Assoc. 2021, 22, 1593–1598. [Google Scholar] [CrossRef]
- Monge, S.; Olmedo, C.; Alejos, B.; Lapeña, M.F.; Sierra, M.J.; Limia, A. Direct and Indirect Effectiveness of Mrna Vaccination against Severe Acute Respiratory Syndrome Coronavirus 2 in Long-Term Care Facilities, Spain. Emerg. Infect. Dis. 2021, 27, 2595–2603. [Google Scholar] [CrossRef]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why Does COVID-19 Disproportionately Affect Older People? Aging 2020, 12, 9959–9981. [Google Scholar] [CrossRef]
- Liu, Y.; Mao, B.; Liang, S.; Yang, J.W.; Lu, H.W.; Chai, Y.H.; Wang, L.; Zhang, L.; Li, Q.H.; Zhao, L.; et al. Association between Age and Clinical Characteristics and Outcomes of COVID-19. Eur. Respir. J. 2020, 55, 2001112. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-Dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Ferrari, D.; Clementi, N.; Criscuolo, E.; Ambrosi, A.; Corea, F.; Di Resta, C.; Tomaiuolo, R.; Mancini, N.; Locatelli, M.; Plebani, M.; et al. Antibody Titer Kinetics and Sars-Cov-2 Infections Six Months after Administration with the Bnt162b2 Vaccine. Vaccines 2021, 9, 1357. [Google Scholar] [CrossRef]
- Alejo, J.L.; Mitchell, J.; Chang, A.; Chiang, T.P.Y.; Massie, A.B.; Segev, D.L.; Makary, M.A. Prevalence and Durability of SARS-CoV-2 Antibodies among Unvaccinated US Adults by History of COVID-19. JAMA—J. Am. Med. Assoc. 2022, 327, 1085–1087. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, L.; Saso, A.; Torres Ortiz, A.; Lam, T.; Hatcher, J.; Thistlethwayte, R.; Harris, M.; Best, T.; Johnson, M.; Wagstaffe, H.; et al. Long-Term Persistence of Spike Protein Antibody and Predictive Modeling of Antibody Dynamics after Infection with Severe Acute Respiratory Syndrome Coronavirus 2. Clin. Infect. Dis. 2022, 74, 1220–1229. [Google Scholar] [CrossRef]
- Bordino, V.; Marengo, N.; Garlasco, J.; Cornio, A.R.; Meddis, D.; Ditommaso, S.; Giacomuzzi, M.; Memoli, G.; Gianino, M.M.; Vicentini, C.; et al. A Cross-Sectional Study of SARS-CoV-2 Seropositivity among Healthcare Workers and Residents of Long-Term Facilities in Italy, January 2021. J. Med. Virol. 2022, 94, 3054–3062. [Google Scholar] [CrossRef]
- Infantino, M.; Pieri, M.; Nuccetelli, M.; Grossi, V.; Lari, B.; Tomassetti, F.; Calugi, G.; Pancani, S.; Benucci, M.; Casprini, P.; et al. The WHO International Standard for COVID-19 serological tests: Towards harmonization of anti-spike assays. Int. Immunopharmacol. 2021, 100, 108095. [Google Scholar] [CrossRef]
- Van Praet, J.T.; Vandecasteele, S.; De Roo, A.; De Vriese, A.S.; Reynders, M. Humoral and Cellular Immunogenicity of the BNT162b2 Messenger RNA Coronavirus Disease 2019 Vaccine in Nursing Home Residents. Clin. Infect. Dis. 2021, 73, 2145–2147. [Google Scholar] [CrossRef]
- Blain, H.; Tuaillon, E.; Gamon, L.; Pisoni, A.; Miot, S.; Rolland, Y.; Picot, M.C.; Bousquet, J. Antibody Response after One and Two Jabs of the BNT162b2 Vaccine in Nursing Home Residents: The CONsort-19 Study. Allergy Eur. J. Allergy Clin. Immunol. 2021, 77, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Lukaszuk, K.; Kiewisz, J.; Rozanska, K.; Dabrowska, M.; Podolak, A.; Jakiel, G.; Woclawek-Potocka, I.; Lukaszuk, A.; Rabalski, L. Usefulness of Ivd Kits for the Assessment of Sars-Cov-2 Antibodies to Evaluate the Humoral Response to Vaccination. Vaccines 2021, 9, 840. [Google Scholar] [CrossRef]
- Lavezzo, E.; Pacenti, M.; Manuto, L.; Boldrin, C.; Cattai, M.; Grazioli, M.; Bianca, F.; Sartori, M.; Caldart, F.; Castelli, G.; et al. Neutralising Reactivity against SARS-CoV-2 Delta and Omicron Variants by Vaccination and Infection History. Genome Med. 2022, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Lumley, S.F.; Wei, J.; Cox, S.; James, T.; Justice, A.; Jesuthasan, G.; O’Donnell, D.; Howarth, A.; Hatch, S.B.; et al. Quantitative SARS-CoV-2 Anti-Spike Responses to Pfizer–BioNTech and Oxford–AstraZeneca Vaccines by Previous Infection Status. Clin. Microbiol. Infect. 2021, 27, e7–e1516. [Google Scholar] [CrossRef]
- Swadźba, J.; Anyszek, T.; Panek, A.; Martin, E. Anti-Spike SARS-CoV-2 IgG Assessment with a Commercial Assay during a 4-Month Course after COVID-19 Vaccination. Vaccines 2021, 9, 1367. [Google Scholar] [CrossRef]
- Gallais, F.; Gantner, P.; Bruel, T.; Velay, A.; Planas, D.; Wendling, M.J.; Bayer, S.; Solis, M.; Laugel, E.; Reix, N.; et al. Evolution of Antibody Responses up to 13 Months after SARS-CoV-2 Infection and Risk of Reinfection. EBioMedicine 2021, 71, 103561. [Google Scholar] [CrossRef] [PubMed]
- Carrat, F.; Villarroel, P.M.S.; Lapidus, N.; Fourié, T.; Blanché, H.; Dorival, C.; Nicol, J.; Deleuze, J.F.; Robineau, O.; Carrat, F.; et al. Heterogeneous SARS-CoV-2 Humoral Response after COVID-19 Vaccination and/or Infection in the General Population. Sci. Rep. 2022, 12, 1–10. [Google Scholar] [CrossRef]
- Flisiak, R.; Pawłowska, M.; Rogalska-Płońska, M.; Bociąga-Jasik, M.; Kłos, K.; Piekarska, A.; Zarębska-Michaluk, D. Effect of Covid-19 on Anti-s Antibody Response in Healthcare Workers Six Months Post-Vaccination. Vaccines 2021, 9, 1325. [Google Scholar] [CrossRef]
- Ogrič, M.; Žigon, P.; Podovšovnik, E.; Lakota, K.; Sodin-Semrl, S.; Rotar, Ž.; Čučnik, S. Differences in SARS-CoV-2-Specific Antibody Responses After the First, Second, and Third Doses of BNT162b2 in Naïve and Previously Infected Individuals: A 1-Year Observational Study in Healthcare Professionals. Front. Immunol. 2022, 13, 876533. [Google Scholar] [CrossRef] [PubMed]
- Shenai, M.B.; Rahme, R.; Noorchashm, H. Equivalency of Protection from Natural Immunity in COVID-19 Recovered Versus Fully Vaccinated Persons: A Systematic Review and Pooled Analysis. Cureus 2021, 13, e19102. [Google Scholar] [CrossRef]
- Milne, G.; Hames, T.; Scotton, C.; Gent, N.; Johnsen, A.; Anderson, R.M.; Ward, T. Does Infection with or Vaccination against SARS-CoV-2 Lead to Lasting Immunity? Lancet Respir. Med. 2021, 9, 1450–1466. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore di Sanità. Report esteso ISS COVID-19: Sorveglianza, impatto delle infezioni ed efficacia vaccinale. In Aggiornamento Nazionale 02/09/2022; Istituto Superiore di Sanità: Rome, Italy, 2022. [Google Scholar]
- Istituto Superiore di Sanità. Prevalenza e distribuzione delle varianti di SARS-CoV-2 di interesse per la sanità pubblica in Italia. In Rapporto n. 15 del 10 Dicembre 2021; Istituto Superiore di Sanità: Rome, Italy, 2021. [Google Scholar]
- Meyer, M.; Constancias, F.; Worth, C.; Meyer, A.; Muller, M.; Boussuge, A.; Kaltenbach, G.; Schmitt, E.; Chayer, S.; Velay, A.; et al. Humoral Immune Response after COVID-19 Infection or BNT162b2 Vaccine among Older Adults: Evolution over Time and Protective Thresholds. GeroScience 2022, 44, 1229–1240. [Google Scholar] [CrossRef]
- Vinh, D.C.; Gouin, J.P.; Cruz-Santiago, D.; Canac-Marquis, M.; Bernier, S.; Bobeuf, F.; Sengupta, A.; Brassard, J.P.; Guerra, A.; Dziarmaga, R.; et al. Real-world serological responses to extended-interval and heterologous COVID-19 mRNA vaccination in frail, older people (UNCoVER): An interim report from a prospective observational cohort study. Lancet Healthy Longev. 2022, 3, e166–e175. [Google Scholar] [CrossRef]
- Sariol, C.A.; Pantoja, P.; Serrano-collazo, C.; Rosa-arocho, T.; Armina-rodríguez, A.; Cruz, L.; Stone, E.T.; Arana, T.; Climent, C.; Latoni, G.; et al. Function Is More Reliable than Quantity to Follow up the Humoral Response to the Receptor-binding Domain of Sars-cov-2-spike Protein after Natural Infection or COVID-19 Vaccination. Viruses 2021, 13, 1972. [Google Scholar] [CrossRef]
- Dimeglio, C.; Herin, F.; Martin-Blondel, G.; Miedougé, M.; Izopet, J. Antibody Titers and Protection against a SARS-CoV-2 Infection. J. Infect. 2022, 84, 248–288. [Google Scholar] [CrossRef]
- Su, Y.; Chen, D.; Yuan, D.; Lausted, C.; Choi, J.; Dai, C.L.; Voillet, V.; Duvvuri, V.R.; Scherler, K.; Troisch, P.; et al. Multi-Omics Resolves a Sharp Disease-State Shift between Mild and Moderate COVID-19. Cell 2020, 183, 1479–1495.e20. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Su, Y.; Baloni, P.; Chen, D.; Pavlovitch-Bedzyk, A.J.; Yuan, D.; Duvvuri, V.R.; Ng, R.H.; Choi, J.; Xie, J.; et al. Integrated analysis of plasma and single immune cells uncovers metabolic changes in individuals with COVID-19. Nat. Biotechnol. 2022, 40, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895.e20. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zaslavsky, M.; Su, Y.; Guo, J.; Sikora, M.J.; van Unen, V.; Christophersen, A.; Chiou, S.H.; Chen, L.; Li, J.; et al. KIR+CD8+ T cells suppress pathogenic T cells and are active in autoimmune diseases and COVID-19. Science 2022, 376, eabi9591. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Feng, S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; et al. Safety, immunogenicity, and reactogenicity of BNT162b2 and mRNA-1273 COVID-19 vaccines given as fourth-dose boosters following two doses of ChAdOx1 nCoV-19 or BNT162b2 and a third dose of BNT162b2 (COV-BOOST): A multicentre, blinded, phase 2, randomised trial. Lancet Infect. Dis. 2022, 22, 1131–1141. [Google Scholar] [CrossRef]
- Grewal, R.; Kitchen, S.A.; Nguyen, L.; Buchan, S.A.; Wilson, S.E.; Costa, A.P.; Kwong, J.C. Effectiveness of a fourth dose of covid-19 mRNA vaccine against the omicron variant among long term care residents in Ontario, Canada: Test negative design study. BMJ 2022, 378, e071502. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age at enrollment, median (IQR) | 53 (43–78) |
| Female gender, N (%) a | 422 (79.03) |
| SARS-CoV-2 infection prior to t0, N (%) a | 277 (51.87) |
| Days between positive RT-PCR and t0, median (IQR) t1, median (IQR) t2, median (IQR) | 70.5 (47.5–262) 112 (80.5–302) 355 (331–531) |
| Seropositivity for IgG anti-SARS-CoV-2, N (%) b t0 t1 t2 | 202 (37.83) 402 (99.5) 297 (94.59) |
| IgG response over threshold, N (%) b t0 t1 t2 | 135 (25.28) 396 (98) 85 (27.07) |
| Days between second vaccine dose and t1, median (IQR) t2, median (IQR) | 14 (14–19) 250 (250–279) |
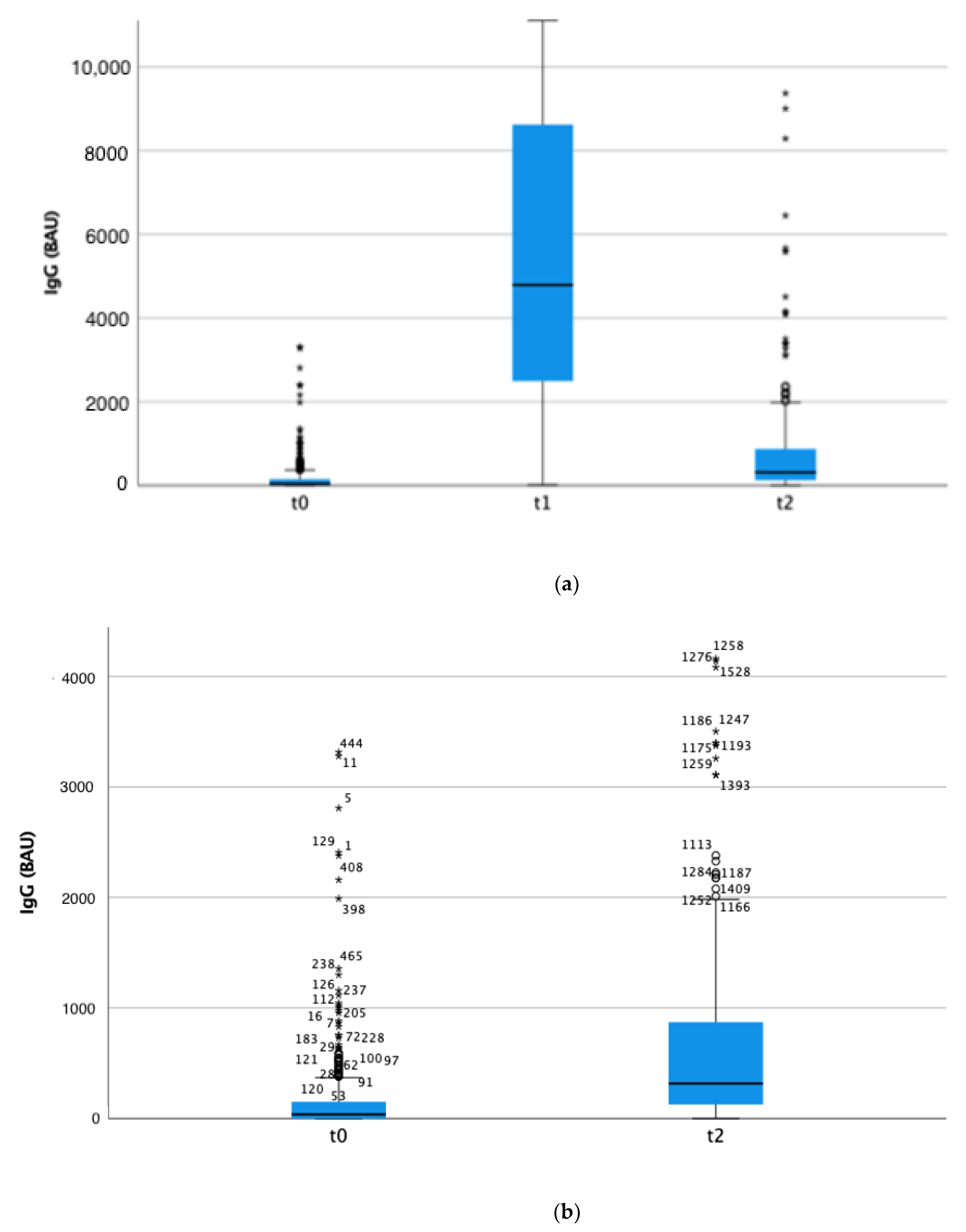
| Groups | t0 Titre, Median (IQR) [N534] | t1 Titre, Median (IQR) [N 404] | t2 Titre, Median (IQR) [N 314] |
|---|---|---|---|
| Participant category: HCWs Residents p-value a | 19.9 (0–109.7) [N 369] 73.5 (16.5–252.3) [N 165] <0.001 | 4266.8 (2328.7–7435.5) [N 258] 6377.5 (3177.3–12,806.4) [N 146] <0.001 | 230.3 (113.3–570.4) [N 195] 677.1 (264–1339) [N 119] <0.001 |
| Gender: Female Male p-value a | 38 (0–136.4) [N 422] 38.8 (0–181.7) [N 112] 0.488 | 5061.3 (2528.8–8713.2) [N 315] 3690 (2128.9–8272.3) [N 89] 0.116 | 336.7 (149.7–856.3) [N 252] 293.7 (66.1–874.5) [N 62] 0.150 |
| Age: <75 years ≥75 years p-value a | 30.3 (0–124.8) [N 389] 64 (15.4–233.5) [N 145] <0.001 | 4250.6 (2380.8–7515.8) [N 275] 7101.7 (3356–12,806.4) [N 129] <0.001 | 267.4 (117.2–637.1) [N 208] 709.1 (237.5–1208.2) [N 106] <0.001 |
| Previous SARS-CoV-2 infection: No previous infection; Previous infection, >3 months from positive RT-PCR to vaccination; Previous infection, ≤3 months from positive RT-PCR to vaccination p-value (no previous infection vs. previous infection) a | 0 (0–32.9) [N 313] 53.2 (20.6–166.4) [N 92] 136.4 (53.3–384) [N 129] <0.001 | 3568.1 (2006.8–6522.1) [N 199] 7297 (3658.2–11,379.5) [N 86] 6267.5 (3345.3–9852.4) [N 119] <0.001 | 177.8 (66.4–422.7) [N 166] 1079.2 (438.8–2176.4) [N 49] 502.7 (271.6–897.7) [N 99] <0.001 |
| All participants | 36.8 (0–151.8) | 4791.3 (2494.6–8634.4) | 316.4 (127.7–872.1) |
| OR (95% CI) | p-Value | |
|---|---|---|
| Residents HCWs | Ref 0.73 (0.02–23.68) | 0.859 |
| Age | 0.84 (0.86–1.04) | 0.218 |
| Male gender Female gender | Ref 2.64 (0.54–12.85) | 0.228 |
| No prior SARS-CoV-2 infection Previous SARS-CoV-2 infection confirmed by RT-PCR | Ref 9.3 (1.07–18.13) | 0.044 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Residents HCWs | Ref 0.47 (0.09–2.36) | 0.358 |
| Age | 0.97 (0.94–1.01) | 0.105 |
| Male gender Female gender | Ref 1.01 (0.42–2.41) | 0.991 |
| No prior SARS-CoV-2 infection Previous SARS-CoV-2 infection confirmed by RT-PCR | Ref 18.1 (7.1–46) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicentini, C.; Zotti, C.M.; Cornio, A.R.; Garlasco, J.; Marengo, N.; Meddis, D.; Ditommaso, S.; Giacomuzzi, M.; Memoli, G.; Bordino, V.; et al. Serological Responses up to 9 Months following COVID-19 mRNA Vaccination in Residents and Health-Care Workers of Long-Term Care Facilities: A Multicenter Prospective Cohort Study in Northern Italy. Vaccines 2022, 10, 2183. https://doi.org/10.3390/vaccines10122183
Vicentini C, Zotti CM, Cornio AR, Garlasco J, Marengo N, Meddis D, Ditommaso S, Giacomuzzi M, Memoli G, Bordino V, et al. Serological Responses up to 9 Months following COVID-19 mRNA Vaccination in Residents and Health-Care Workers of Long-Term Care Facilities: A Multicenter Prospective Cohort Study in Northern Italy. Vaccines. 2022; 10(12):2183. https://doi.org/10.3390/vaccines10122183
Chicago/Turabian StyleVicentini, Costanza, Carla Maria Zotti, Alessandro Roberto Cornio, Jacopo Garlasco, Noemi Marengo, Davide Meddis, Savina Ditommaso, Monica Giacomuzzi, Gabriele Memoli, Valerio Bordino, and et al. 2022. "Serological Responses up to 9 Months following COVID-19 mRNA Vaccination in Residents and Health-Care Workers of Long-Term Care Facilities: A Multicenter Prospective Cohort Study in Northern Italy" Vaccines 10, no. 12: 2183. https://doi.org/10.3390/vaccines10122183
APA StyleVicentini, C., Zotti, C. M., Cornio, A. R., Garlasco, J., Marengo, N., Meddis, D., Ditommaso, S., Giacomuzzi, M., Memoli, G., Bordino, V., Gianino, M. M., & on behalf of the Collaborating Group. (2022). Serological Responses up to 9 Months following COVID-19 mRNA Vaccination in Residents and Health-Care Workers of Long-Term Care Facilities: A Multicenter Prospective Cohort Study in Northern Italy. Vaccines, 10(12), 2183. https://doi.org/10.3390/vaccines10122183