

Effectiveness of Adapted COVID-19 Vaccines and Ability to Establish Herd Immunity against Omicron BA.1 and BA4-5 Variants of SARS-CoV-2


Abstract
:1. Introduction
2. Materials and Methods
2.1. Effectiveness of Adapted Vaccines in Preventing SARS-CoV-2 Infections
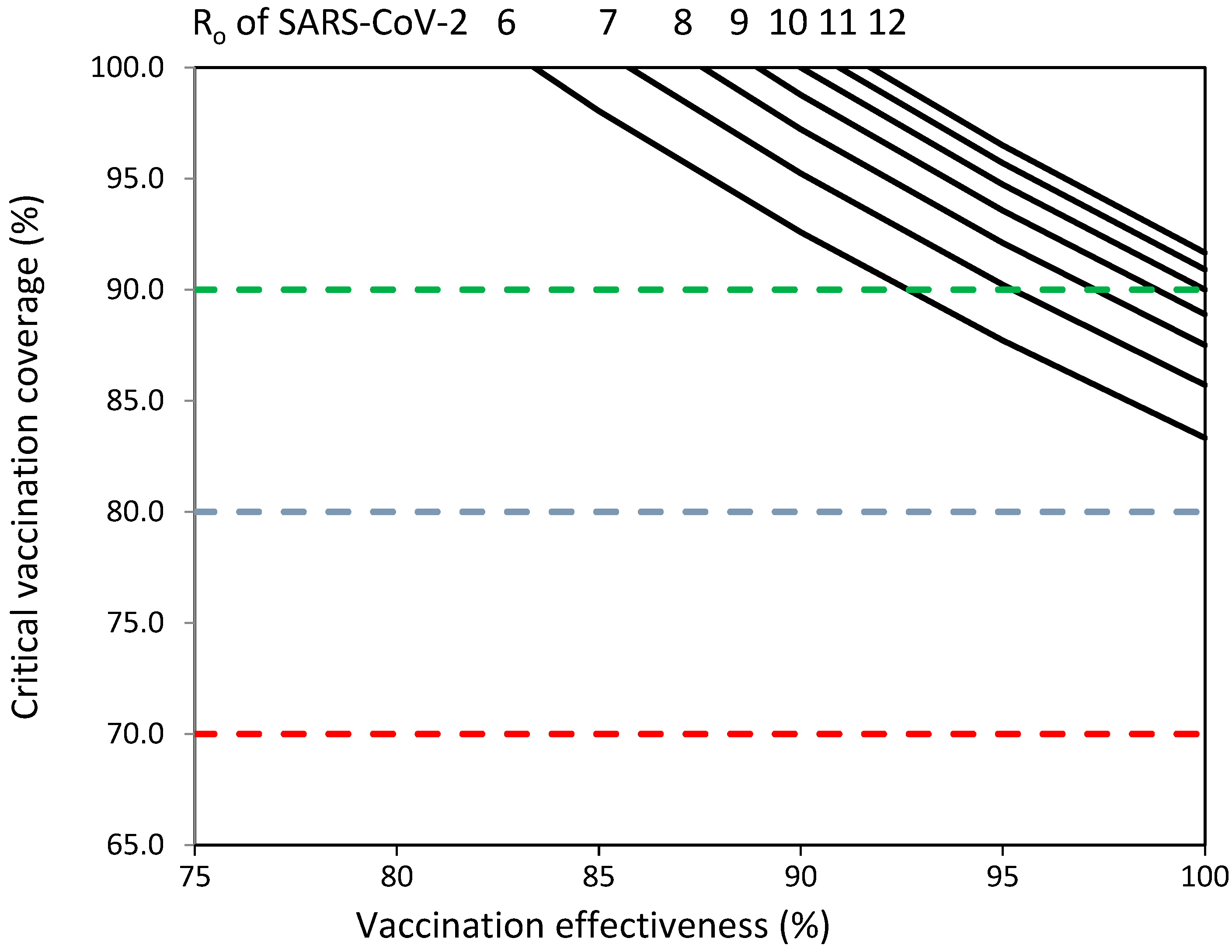
2.2. Assessment of the Ability of Adapted Vaccines to Establish Herd Immunity against Omicron Variants
2.3. Challenges That Adapted Vaccines Should Overcome to Establish Herd Immunity against Emerging SARS-CoV-2 Variants
2.4. Statistical Analysis
3. Results
3.1. Effectiveness of Adapted Vaccines in Preventing SARS-CoV-2 Infections
3.2. Assessment of the Ability of Adapted Vaccines to Establish Herd Immunity against Omicron SARS-CoV-2 Variants
3.3. Challenges That Adapted Vaccines Should Overcome to Establish Herd Immunity against Emerging SARS-CoV-2 Variants
4. Discussion
- (1)
- Detect the emergent variants.
- (2)
- Assess the health impact of the emergent variants.
- (3)
- Monitor and characterize the transmissibility and immune escape of the emergent variants.
- (4)
- Assess the anti-SARS-CoV-2 immunity levels in the population.
- (5)
- Assess the percentages of COVID-19 vaccination coverage required to establish herd immunity.
- (6)
- Decide the vaccination strategy to protect vulnerable population groups and to prevent SARS-CoV-2 transmission in the population.
- (7)
- Develop COVID-19 booster vaccinations to overcome waning vaccine-induced immunity.
- (8)
- Develop updated and new vaccines against emergent variants of concern to increase COVID-19 vaccination effectiveness in preventing severe disease and SARS-CoV-2 infection.
- (9)
- Use non-pharmacological measures if they are necessary to reduce viral transmissibility among vulnerable population groups and to reduce SARS-CoV-2 transmission in the population.
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 5 December 2023).
- WHO. COVID-19 Strategic Preparedness and Response Plan (SPRP); WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/WHO-WHE-2021.02 (accessed on 14 July 2023).
- WHO. COVID-19 Vaccination−Strategic Vision for 2022. Available online: https://cdn.who.int/media/docs/default-source/immunization/sage/covid/global-COVID-19-vaccination-strategic-vision-for-2022_sage-yellow-book.pdf?sfvrsn=4827ec0d_5 (accessed on 10 June 2023).
- Huang, C.; Yang, L.; Pan, J.; Xu, X.; Peng, R. Correlation between vaccine coverage and the COVID-19 pandemic throughout the world: Based on real-world data. J. Med. Virol. 2022, 94, 2181–2187. [Google Scholar] [CrossRef]
- Plans-Rubió, P. Percentages of Vaccination Coverage Required to Establish Herd Immunity against SARS-CoV-2. Vaccines 2022, 8, 736. [Google Scholar] [CrossRef]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 5 December 2023).
- WHO. Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic, 5 May 2023. Available online: www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic (accessed on 26 November 2023).
- WHO. With the International Public Health Emergency Ending, WHO/Europe Launches Its Transition Plan for COVID-19. WHO News, 12 June 2023. Available online: https://reliefweb.int/report/world/international-public-health-emergency-ending-whoeurope-launches-its-transition-plan-covid-19?gad_source=1&gclid=Cj0KCQiAsburBhCIARIsAExmsu5PlP4lXEeC9-O_4ujO2dyycSp2DjLHF9owc-fvwLEKFSrGXH4St10aAol6EALw_wcB (accessed on 2 November 2023).
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- WHO. Achieving 70% COVID-19 Immunization Coverage by Mid-2022. Statement of the Independent Allocation of Vaccines Group (IAVG) of COVAX. 23 December 2021. Available online: https://www.who.int/news/item/23-12-2021-achieving-70-COVID-19-immunization-coverage-by-mid-2022 (accessed on 5 December 2023).
- Morens, D.M.; Folkers, G.K.; Fauci, A.S. The concept of classical herd ommunity may not apply to COVID-19. J. Infect Dis. 2022, 226, 195–198. [Google Scholar] [CrossRef]
- WHO. Traking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 26 September 2023).
- Institute for Health Metrics and Evaluation (IHME). COVID-19 Vaccine Efficacy Summary; IHME, University of Washington: Seattle, WA, USA, 2023; Available online: https://www.healthdata.org/research-analysis/diseases-injuries/covid/covid-19-vaccine-efficacy-summary (accessed on 27 November 2023).
- Yue, C.; Song, W.; Wang, L.; Jian, F.; Chen, X.; Gao, F.; Shen, Z.; Wang, Y.; Wang, X.; Cao, Y. ACE2 binding and antibody evasion in enhanced transmissibility of XBB.1.5. Lancet Infect Dis. 2023, 23, 278–280. [Google Scholar] [CrossRef]
- Mohammed, H.; Pham-Tran, D.D.; Yeoh, Z.Y.M.; Wang, B.; McMillan, M.; Andraweera, P.H.; Marshall, H.S. A Systematic Review and Meta-Analysis on the Real-World Effectiveness of COVID-19 Vaccines against Infection, Symptomatic and Severe COVID-19 Disease Caused by the Omicron Variant (B.1.1.529). Vaccines 2023, 11, 224. [Google Scholar] [CrossRef]
- United Kingdom Security Agency. SARS-CoV-2 Variants of Concern and Variants under Investigation in England. UK Security Agency: Technical Briefing 33. 23 December 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1043807/technical-briefing-33.pdf (accessed on 5 April 2023).
- Markov, P.V.; Ghafari, M.; Beer, M.; Lythgoe, K.; Simmonds, P.; Stilianakis, N.I.; Katzourakis, A. The evolution of SARS-CoV-2. Nat. Rev. Microbiol. 2023, 21, 361–379. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Jiang, L.; Tian, T.; Li, W.; Pan, Y.; Wang, Y. Efficacy and Safety of COVID-19 Vaccination in Older Adults: A Systematic Review and Meta-Analysis. Vaccines 2022, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Pagel, C.; Wilde, H.; Tomlinson, C.; Mateen, B.; Brown, K. A Methodological Framework for Assessing the Benefit of SARS-CoV-2 Vaccination following Previous Infection: Case Study of Five- to Eleven-Year-Olds. Vaccines 2023, 11, 988. [Google Scholar] [CrossRef] [PubMed]
- WHO. Status of COVID-19 Vaccines within WHO EUL/PQ Evaluation Process. Available online: https://extranet.who.int/pqweb/sites/default/files/documents/Status_COVID_VAX_02April2022.pdf (accessed on 4 May 2023).
- EMA. Authorized COVID-19 Vaccines. Available online: https://www.ema.europa.eu/en/human-regulatory-overview/public-health-threats/coronavirus-disease-covid-19/covid-19-medicine (accessed on 4 May 2023).
- Link-Gelles, R.; Weber, Z.A.; Reese, S.E.; Payne, A.B.; Gaglani, M.; Adams, K.; Kharbanda, A.B.; Natarajan, K.; DeSilva, M.B.; Dascomb, K.; et al. Estimates of Bivalent mRNA Vaccine Durability in Preventing COVID-19-Associated Hospitalization and Critical Illness Among Adults with and without Immunocompromising Conditions-VISION Network, September 2022-April 2023. MMWR Morb. Mortal.Wkly. Rep. 2023, 72, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Weber, Z.A.; Natarajan, K.; Klein, N.P.; Kharbanda, A.B.; Stenehjem, E.; Embi, P.J.; Reese, S.E.; Naleway, A.L.; Grannis, S.J.; et al. Early Estimates of Bivalent mRNA Vaccine Effectiveness in Preventing COVID-19-Associated Emergency Department or Urgent Care Encounters and Hospitalizations Among Immunocompetent Adults-VISION Network, Nine States, Sptember-November 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 71, 1637–1646. [Google Scholar] [CrossRef]
- Arashiro, T.; Arima, Y.; Kuramochi, J.; Muraoka, H.; Sato, A.; Chubachi, K.; Yanai, A.; Arioka, H.; Uehara, Y.; Ihara, G.; et al. Effectiveness of BA.1- and BA.4/BA. 5-Containing Bivalent COVID-19 mRNA Vaccines Against Symptomatic SARS-CoV-2 Infection During the BA.5-Dominant Period in Japan. Open Forum Infect. Dis. 2023, 10, ofad240. [Google Scholar] [CrossRef]
- Surie, D.; DeCuir, J.; Zhu, Y.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; et al. Early Estimates of Bivalent mRNA Vaccine Effectiveness in Preventing COVID-19-Associated Hospitalization Among Immunocompetent Adults Aged ≥65 Years-IVY Network, 18 States, September 8–November 30, 2022. MMWR Morb. Mortal Wkly. Rep. 2022, 71, 1625–1630. [Google Scholar] [CrossRef]
- Arbel, R.; Peretz, A.; Sergienko, R.; Friger, M.; Beckenstein, T.; Duskin-Bitan, H.; Yaron, S.; Hammerman, A.; Bilenko, N.; Netzer, D. Effectiveness of a bivalent mRNA vaccine booster dose to prevent severe COVID-19 outcomes: A retrospective cohort study. Lancet Infect. Dis 2023, 23, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.Y.; Chiew, C.J.; Pang, D.; Lee, V.J.; Ong, B.; Wang, L.F.; Ren, E.C.; Lye, D.C.; Tan, K.B. Effectiveness of bivalent mRNA vaccines against medically attended symptomatic SARS-CoV-2 infection and COVID-19-related hospital admission among SARS-CoV-2-naive and previously infected individuals: A retrospective cohort study. Lancet Infect. Dis. 2023, 23, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Bo, Y.; Guo, C.; Lin, C.; Zeng, Y.; Li, H.B.; Zhang, Y.; Hossain, M.S.; Chan, J.W.M.; Yeung, D.W.; Kwok, K.O.; et al. Effectiveness of non-pharmaceutical interventions on COVID-19 transmission in 190 countries from 23 January to 13 April 2020. Int. J. Infect. Dis. 2021, 102, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Milne, G.J.; Carrivick, J.; Whyatt, D. Mitigating the SARS-CoV-2 Delta disease burden in Australia by non-pharmaceutical interventions and vaccinating children: A modelling analysis. BMC Med. 2022, 20, 80. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. Br. Med. J. 2016, 355, i4919. [Google Scholar] [CrossRef]
- Fontanet, A.; Cauchemez, S. COVID-19 herd immunity: Where are we? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef]
- She, J.; Hou, D.; Chen, C.; Bi, J.; Song, Y. Challenges of vaccination and herd immunity in COVID-19 and management strategies. Clin. Respir. J. 2022, 16, 708–716. [Google Scholar] [CrossRef]
- Chatterjee, S.; Bhattacharya, M.; Nag, S.; Dhama, K.; Chakraborty, C. A Detailed Overview of SARS-CoV-2 Omicron: Its Sub-Variants, Mutations and Pathophysiology, Clinical Characteristics, Immunological Landscape, Immune Escape, and Therapies. Viruses 2023, 15, 167. [Google Scholar] [CrossRef]
- Lin, Y.; Ocklöv, J. The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus. J. Travel Med. 2021, 28, 1–3. [Google Scholar] [CrossRef]
- Ito, K.; Piantham, C.; Nishiura, H. Relative instantaneous reproduction number of Omicron SARS-CoV-2 variant with respect to the Delta variant in Denmark. J. Med. Virol. 2022, 94, 2265–2268. [Google Scholar] [CrossRef]
- Tegally, H.; Wilkinson, E.; Giovanetti, M.; Iranzadeh, A.; Fonseca, V.; Giandhari, J.; Doolabh, D.; Pillay, S.; San, E.J.; Msomi, N.; et al. Detection of a SARS-CoV-2 variant of concern in South Africa. Nature 2021, 592, 438–443. [Google Scholar] [CrossRef]
- Faria, N.R.; Mellan, T.A.; Whittaker, C.; Claro, I.M.; Candido, D.D.S.; Mishra, S.; Crispim, M.A.E.; Sales, F.C.S.; Hawryluk, I.; McCrone, J.T.; et al. Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil. Science 2021, 372, 815–821. [Google Scholar] [CrossRef]
- Hui, K.P.Y.; Ho, J.C.W.; Cheung, M.C.; Ng, K.C.; Ching, R.H.H.; Lai, K.L.; Kam, T.T.; Gu, H.; Sit, K.Y.; Hsin, M.K.Y.; et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature 2022, 603, 715–720. [Google Scholar] [CrossRef]
- Bálint, G.; Vörös-Horváth, B.; Széchenyi, A. Omicron: Increased transmissibility and decreased pathogenicity. Sig. Transduct. Target Ther. 2022, 7, 151. [Google Scholar] [CrossRef]
- Epidat: Programa para Análisis Epidemiológico de Datos; Consellería de Sanidade, Xunta de Galicia: Celeiro-Viveiro, Spain; Organización Panamericana de la salud (OPS-OMS): Washington, DC, USA; Universidad CES, Colombia: Medellín, Colombia, 2014.
- Moulana, A.; Dupic, T.; Phillips, A.M.; Chang, J.; Roffler, A.A.; Greaney, A.J.; Starr, T.N.; Bloom, J.D.; Desai, M.M. The landscape of antibody binding affinity in SARS-CoV-2 Omicron BA.1 evolution. Elife 2023, 12, e83442. [Google Scholar] [CrossRef] [PubMed]
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Vir. 2022, 94, 1825–1832. [Google Scholar] [CrossRef]
- Huo, J.; Dijokaite-Guraliuc, A.; Liu, C.; Zhou, D.; Ginn, H.M.; Das, R.; Supasa, P.; Selvaraj, M.; Nutalai, R.; Tuekprakhon, A.; et al. A delicate balance between antibody evasion and ACE2 affinity for Omicron BA.2.75. Cell Rep. 2023, 42, 111903. [Google Scholar] [CrossRef]
- Rees-Spear, C.; Muir, L.; Griffith, S.A.; Heaney, J.; Aldon, Y.; Snitselaar, J.L.; Thomas, P.; Graham, C.; Seow, J.; Lee, N.; et al. The effect of spike mutations on SARS-CoV-2 neutralization. Cell Rep. 2021, 34, 108890. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Forecasting Team. Past SARS-CoV-2 infection protection against re-infection: A systematic review and meta-analysis. Lancet 2023, 401, 833–842. [Google Scholar] [CrossRef]
- Pulliam, J.R.C.; Schalkwyk, C.; Govender, N.; Gottberg, A.; Cohen, C.; Groome, M.J. Increased risk of SARS-CoV-2 reinfection associated with emergence of the Omicron variant in South Africa. Science 2022, 376, eabn4947. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Wheatley, A.K.; Ramuta, M.D.; Reynaldi, A.; Cromer, D.; Subbarao, K.; O’Connor, D.H.; Kent, S.J.; Davenport, M.P. Measuring immunity to SARS-CoV-2 infection: Comparing assays and animal models. Nat. Rev. Immunol. 2020, 20, 727–738. [Google Scholar] [CrossRef]
- Springer, D.N.; Bauer, M.; Medits, I.; Camp, J.V.; Aberle, S.W.; Burtscher, C.; Höltl, E.; Weseslindtner, L.; Stiasny, K.; Aberle, J.H. Bivalent COVID-19 mRNA booster vaccination (BA.1 or BA.4/BA.5) increases neutralization of matched Omicron variants. NPJ Vaccines 2023, 8, 110. [Google Scholar] [CrossRef] [PubMed]
- Mazanec, M.B.; Coudret, C.L.; Fletcher, D.R. Intracellular neutralization of influenza virus by immunoglobulin A anti-hemagglutinin monoclonal antibodies. J. Virol. 1995, 69, 1339–1343. [Google Scholar] [CrossRef]
- Sterlin, D.; Mathian, A.; Miyara, M.; Mohr, A.; Anna, F.; Claër, L.; Quentric, P.; Fadlallah, J.; Devilliers, H.; Ghillani, P.; et al. IgA dominates the early neutralizing antibody response to SARS-CoV-2. Sci. Transl. Med. 2021, 13, eabd2223. [Google Scholar] [CrossRef]
- Arora, P.; Sidarovich, A.; Krüger, N.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.S.; Winkler, M.S.; Schulz, S.; Jäck, H.M.; et al. B.1.617.2 enters and fuses lung cells with increased efficiency and evades antibodies induced by infection and vaccination. Cell Rep. 2021, 37, 109825. [Google Scholar] [CrossRef]
- Kodera, S.; Ueta, H.; Unemi, T.; Nakata, T.; Hirata, A. Population-level immunity for transient suppression of COVID-19 waves in Japan from April 2021 to September 2022. Vaccines 2023, 11, 1457. [Google Scholar] [CrossRef]
- European Medicines Agency. EMA Considerations on COVID-19 Vaccine Approval. EMA/592928/2020. Available online: https://www.ema.europa.eu/en/documents/other/ema-considerations-covid-19-vaccine-approval_en.pdf (accessed on 28 April 2022).
- European Medicines Agency First Adapted COVID-19 Booster Vaccines Recommended for Approval in the EU. Available online: https://www.ema.europa.eu/en/news/first-adapted-covid-19-booster-vaccines-recommended-approval-eu (accessed on 27 October 2023).
- European Medicines Agency. Adapted Vaccine Targeting BA.4 and BA.5 Omicron Variants and Original SARS-CoV-2 Recommended for Approval. Available online: https://www.ema.europa.eu/en/news/adapted-vaccine-targeting-ba4-ba5-omicron-variants-original-sars-cov-2-recommended-approval (accessed on 27 October 2023).
- Dong, Y.; Dai, T.; Wang, B.; Zhang, L.; Zeng, L.-H.; Huang, J.; Yan, H.; Zhang, L.; Zhou, F. The way of SARS-CoV-2 vaccine development: Success and challenges. Sig. Transduct. Target Ther. 2021, 6, 387. [Google Scholar] [CrossRef]
- Piccoli, L.; Park, Y.J.; Tortorici, M.A.; Czudnochowski, N.; Walls, A.C.; Beltramello, M.; Silacci-Fregni, C.; Pinto, D.; Rosen, L.E.; Bowen, J.E.; et al. Mapping Neutralizing and Immunodominant Sites on the SARS-CoV-2 Spike Receptor-Binding Domain by Structure-Guided High-Resolution Serology. Cell 2020, 183, 1024–1042.e21. [Google Scholar] [CrossRef] [PubMed]
- Vilibic-Cavlek, T.; Bogdanic, M.; Borko, E.; Hruskar, Z.; Zilic, D.; Ferenc, T.; Tabain, I.; Barbic, L.; Vujica Ferenc, M.; Ferencak, I.; et al. Detection of SARS-CoV-2 Antibodies: Comparison of Enzyme Immunoassay, Surrogate Neutralization and Virus Neutralization Test. Antibodies 2023, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.; Alisoltani, A.; Bratt, D.; Cohen-Lavi, L.; Dearlove, B.L.; Drosten, C.; Fischer, W.M.; Fouchier, R.A.M.; Gonzalez-Reiche, A.S.; Jaroszewski, L.; et al. US National Institutes of Health Prioritization of SARS-CoV-2 Variants. Emerg. Infect. Dis. 2023, 29, e221646. [Google Scholar] [CrossRef]
- Velavan, T.P.; Pollard, A.J.; Kremsner, P.C. Herd immunity and vaccination of children for COVID-19. Int. J. Infect. Dis. 2020, 98, 14–15. [Google Scholar] [CrossRef]

{kind=link}
| Vaccine | Study Population, Country | Outcome | No. Positive/No. Negative | aVE % (95% CI) |
|---|---|---|---|---|
| Link-Gelles et al. [22] | ||||
| Bivalent vaccine | Adults USA | Hospitalization 7–59 days after vaccination | unV: 1791/13723 V: 327/4530 | 62 (57–67) |
| Hospitalization 60–115 days after vaccination | unV: 1791/13723 V:486/4705 | 47 (41–53) | ||
| Critical care 7–59 days after vaccination | unV: 367/13723 V: 49/4530 | 69 (57–77) | ||
| Critical care 60–115 days after vaccination | unV: 367/13723 V: 85/4705 | 46 (30–58) | ||
| Critical care 120–179 days after vaccination | unV: 367/13723 V: 33/2995 | 50 (26–66) | ||
| Tendorde et al. [23] | ||||
| Bivalent vaccine | Adults USA | Hospitalization ≥7 days after vaccination | unV: 434/3658V: 56/828 | 59 (44–70) |
| Arashiro et al. [24] | ||||
| BA.1 vaccine | Adults Japan | Hospitalization ≥14 days after vaccination | unV: 442/226 V: 95/76 | 65 (47–77) |
| BA.4-5 vaccine | unV: 442/226 V: 112/116 | 76 (65–83) | ||
| Overall aVE in preventing severe disease obtained via meta-analysis | ||||
| Range of values from selected studies: 46–76% | ||||
| Fixed-effects meta-analysis: 56% (95% CI: 53–59%) Random-effects meta-analysis: 60% (95% CI: 51–66%) | ||||
| aVE in preventing SARS-CoV-2 infection (35% lower than that for severe disease [13]) | ||||
| Range of values from selected studies: 30–49% | ||||
| Estimated from the fixed-effects meta-analysis results: 36% (95% CI: 34–38%) Estimated from the random-effects meta-analysis results: 39% (95% CI: 33–43%) | ||||
| Effectiveness of Adapted Vaccines (%) | Ro Values of SARS-CoV-2 that Adapted Vaccines Could Block | |||||
|---|---|---|---|---|---|---|
| Vaccination Coverage | ||||||
| 60% | 70% | 80% | 90% | 95% | 100% | |
| (1) Without using NPIs and 0% prevalence of protected individuals in the population (0P) | ||||||
| 30 | 1.22 | 1.27 | 1.32 | 1.37 | 1.40 | 1.43 |
| 39 | 1.31 | 1.38 | 1.45 | 1.54 | 1.59 | 1.64 |
| z | 1.42 | 1.52 | 1.64 | 1.79 | 1.87 | 1.96 |
| (2) Using face masks and 0P | ||||||
| 30 | 1.44 | 1.49 | 1.55 | 1.61 | 1.65 | 1.68 |
| 39 | 1.54 | 1.62 | 1.71 | 1.81 | 1.87 | 1.93 |
| 49 | 1.67 | 1.79 | 1.94 | 2.11 | 2.20 | 2.31 |
| Using face masks and social distancing and 0P | ||||||
| 30 | 1.99 | 2.06 | 2.14 | 2.23 | 2.28 | 2.33 |
| 39 | 2.13 | 2.24 | 2.37 | 2.51 | 2.59 | 2.67 |
| 49 | 2.31 | 2.48 | 2.68 | 2.91 | 3.05 | 3.19 |
| Using face masks, social distancing, travel restrictions and 0P | ||||||
| 30 | 2.67 | 2.77 | 2.88 | 3.00 | 3.06 | 3.13 |
| 39 | 2.86 | 3.01 | 3.18 | 3.37 | 3.48 | 3.59 |
| 49 | 3.10 | 3.33 | 3.60 | 3.91 | 4.09 | 4.29 |
| Using face masks, social distancing, travel restrictions, quarantine (MDTQ) and 0P | ||||||
| 30 | 3.28 | 3.40 | 3.54 | 3.68 | 3.76 | 3.84 |
| 39 | 3.51 | 3.70 | 3.91 | 4.14 | 4.27 | 4.41 |
| 49 | 3.81 | 4.09 | 4.42 | 4.81 | 5.03 | 5.27 |
| (3) Using NPIs (MDTQ) and 10% prevalence of protected individuals in the population | ||||||
| 30 | 3.73 | 3.90 | 4.07 | 4.27 | 4.37 | 4.48 |
| 39 | 4.04 | 4.29 | 4.57 | 4.90 | 5.08 | 5.27 |
| 49 | 4.44 | 4.83 | 5.29 | 5.86 | 6.19 | 6.56 |
| Using MDTQ and 20% prevalence of protected individuals in the population | ||||||
| 30 | 4.34 | 4.56 | 4.80 | 5.07 | 5.22 | 5.38 |
| 39 | 4.75 | 5.10 | 5.51 | 5.99 | 6.26 | 6.56 |
| 49 | 5.31 | 5.88 | 6.59 | 7.49 | 8.04 | 8.67 |
| Using MDTQ and 30% prevalence of protected individuals in the population | ||||||
| 30 | 5.17 | 5.49 | 5.84 | 6.25 | 6.48 | 6.72 |
| 39 | 5.77 | 6.30 | 6.93 | 7.70 | 8.16 | 8.67 |
| 49 | 6.62 | 7.53 | 8.73 | 10.38 | 11.46 | 12.80 |
| Ro Value for SARS-CoV-2 | Vaccine Effectiveness (%) a in Preventing SARS-CoV-2 Infection Required to Establish Herd Immunity Against Emerging SARS-CoV-2 Variants with Ro from 6 to 12 with Percentages of Vaccination Coverage from 70% to 95% | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Without Using NPIs b | Using Face Masks b | Using Face Masks and Social Distancing b | Using Face Masks, Social Distancing and Travel Restrictions | Using Face Masks, Social Distancing, Travel Restrictions and Quarantine | ||||||||||||
| 90% | 95% | 90% | 95% | 70% | 80% | 90% | 95% | 70% | 80% | 90% | 95% | 70% | 80% | 90% | 95% | |
| 6 | 92.6 | 87.7 | 89.3 | 84.6 | – | 91.1 | 81.0 | 76.7 | 90.8 | 79.4 | 70.6 | 66.9 | 78.9 | 69.0 | 61.3 | 58.1 |
| 6.5 | 94.0 | 89.1 | 91.0 | 86.2 | – | 93.7 | 83.3 | 78.9 | 94.8 | 82.9 | 73.7 | 69.8 | 83.8 | 73.3 | 65.2 | 61.7 |
| 7 | 95.2 | 90.2 | 92.4 | 87.6 | – | 95.9 | 85.3 | 80.8 | 98.2 | 85.9 | 76.4 | 72.4 | 88.0 | 77.0 | 68.4 | 64.8 |
| 7.5 | 96.3 | 91.2 | 93.7 | 88.7 | – | 97.9 | 87.0 | 82.4 | – | 88.5 | 78.7 | 74.6 | 91.7 | 80.2 | 71.3 | 67.5 |
| 8 | 97.2 | 92.1 | 94.8 | 89.8 | – | 99.6 | 88.5 | 83.8 | – | 90.8 | 80.7 | 76.5 | 94.9 | 83.0 | 73.8 | 69.9 |
| 8.5 | 98.0 | 92.9 | 95.7 | 90.7 | – | – | 89.8 | 85.1 | – | 92.8 | 82.5 | 78.2 | 97.7 | 85.5 | 76.0 | 72.0 |
| 9 | 98.8 | 93.6 | 96.6 | 91.5 | – | – | 91.0 | 86.2 | – | 94.6 | 84.1 | 79.7 | 87.7 | 77.9 | 73.8 | |
| 9.5 | 99.4 | 94.2 | 97.3 | 92.2 | – | – | 92.1 | 87.2 | – | 96.2 | 85.5 | 81.0 | – | 89.6 | 79.7 | 75.5 |
| 10 | 100.0 | 94.7 | 98.0 | 92.9 | – | – | 93.0 | 88.1 | – | 97.6 | 86.8 | 82.2 | – | 91.4 | 81.2 | 77.0 |
| 10.5 | – | 95.2 | 98.6 | 93.5 | – | – | 93.9 | 88.9 | – | 99.0 | 88.0 | 83.3 | – | 93.0 | 82.7 | 78.3 |
| 11 | – | 95.7 | 99.2 | 94.0 | – | – | 94.7 | 89.7 | – | – | 89.0 | 84.3 | – | 94.5 | 84.0 | 79.5 |
| 11.5 | – | 96.1 | 99.7 | 94.5 | – | – | 95.4 | 90.4 | – | – | 90.0 | 85.2 | – | 95.8 | 85.1 | 80.7 |
| 12 | – | 96.5 | – | 94.9 | – | – | 96.0 | 91.0 | – | – | 90.9 | 86.1 | – | 97.0 | 86.2 | 81.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plans-Rubió, P. Effectiveness of Adapted COVID-19 Vaccines and Ability to Establish Herd Immunity against Omicron BA.1 and BA4-5 Variants of SARS-CoV-2. Vaccines 2023, 11, 1836. https://doi.org/10.3390/vaccines11121836
Plans-Rubió P. Effectiveness of Adapted COVID-19 Vaccines and Ability to Establish Herd Immunity against Omicron BA.1 and BA4-5 Variants of SARS-CoV-2. Vaccines. 2023; 11(12):1836. https://doi.org/10.3390/vaccines11121836
Chicago/Turabian StylePlans-Rubió, Pedro. 2023. "Effectiveness of Adapted COVID-19 Vaccines and Ability to Establish Herd Immunity against Omicron BA.1 and BA4-5 Variants of SARS-CoV-2" Vaccines 11, no. 12: 1836. https://doi.org/10.3390/vaccines11121836
APA StylePlans-Rubió, P. (2023). Effectiveness of Adapted COVID-19 Vaccines and Ability to Establish Herd Immunity against Omicron BA.1 and BA4-5 Variants of SARS-CoV-2. Vaccines, 11(12), 1836. https://doi.org/10.3390/vaccines11121836