
Flu Shots Unveiled: A Global Systematic Review of Healthcare Providers’ Uptake of, Perceptions, and Attitudes toward Influenza Vaccination

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
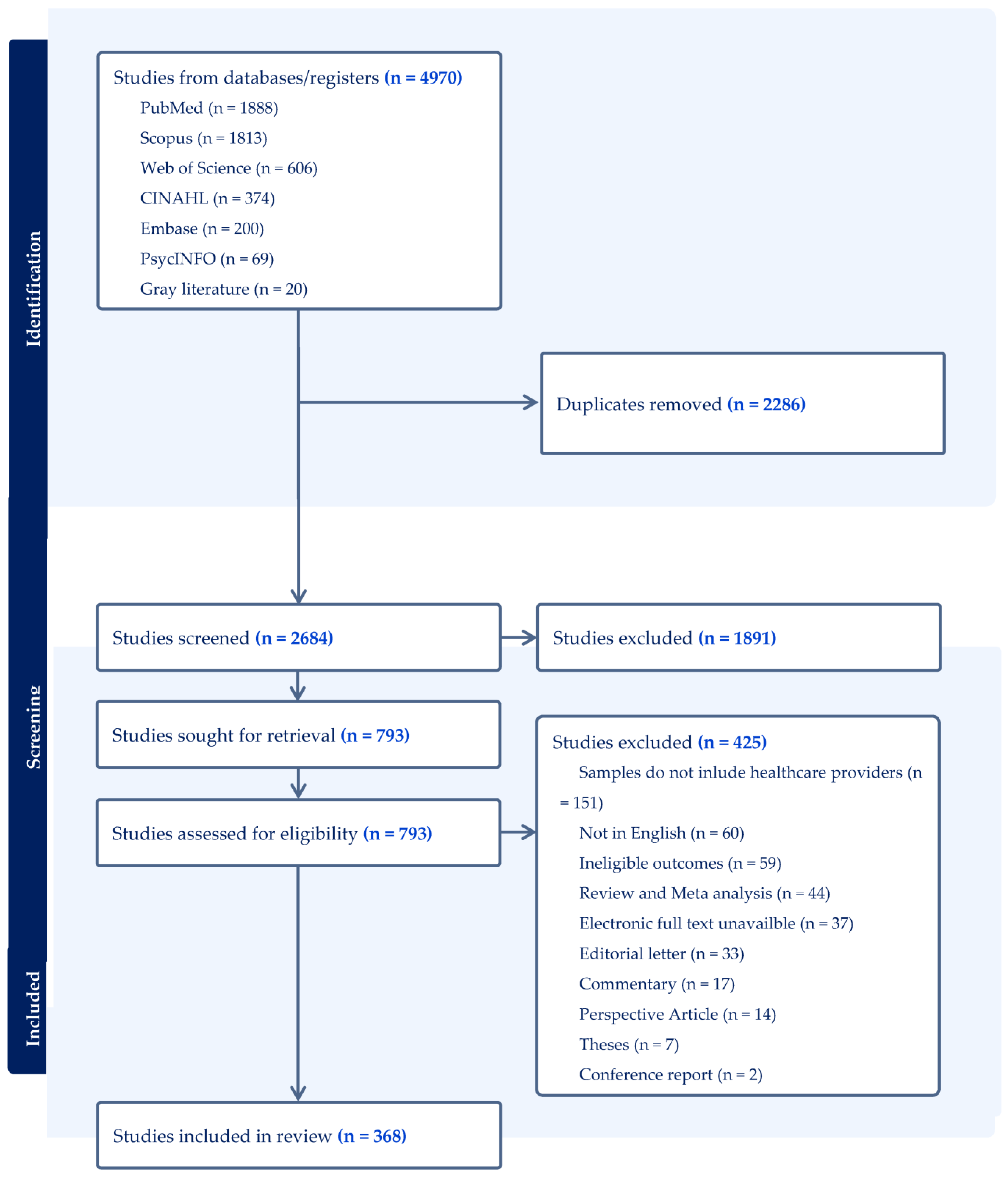
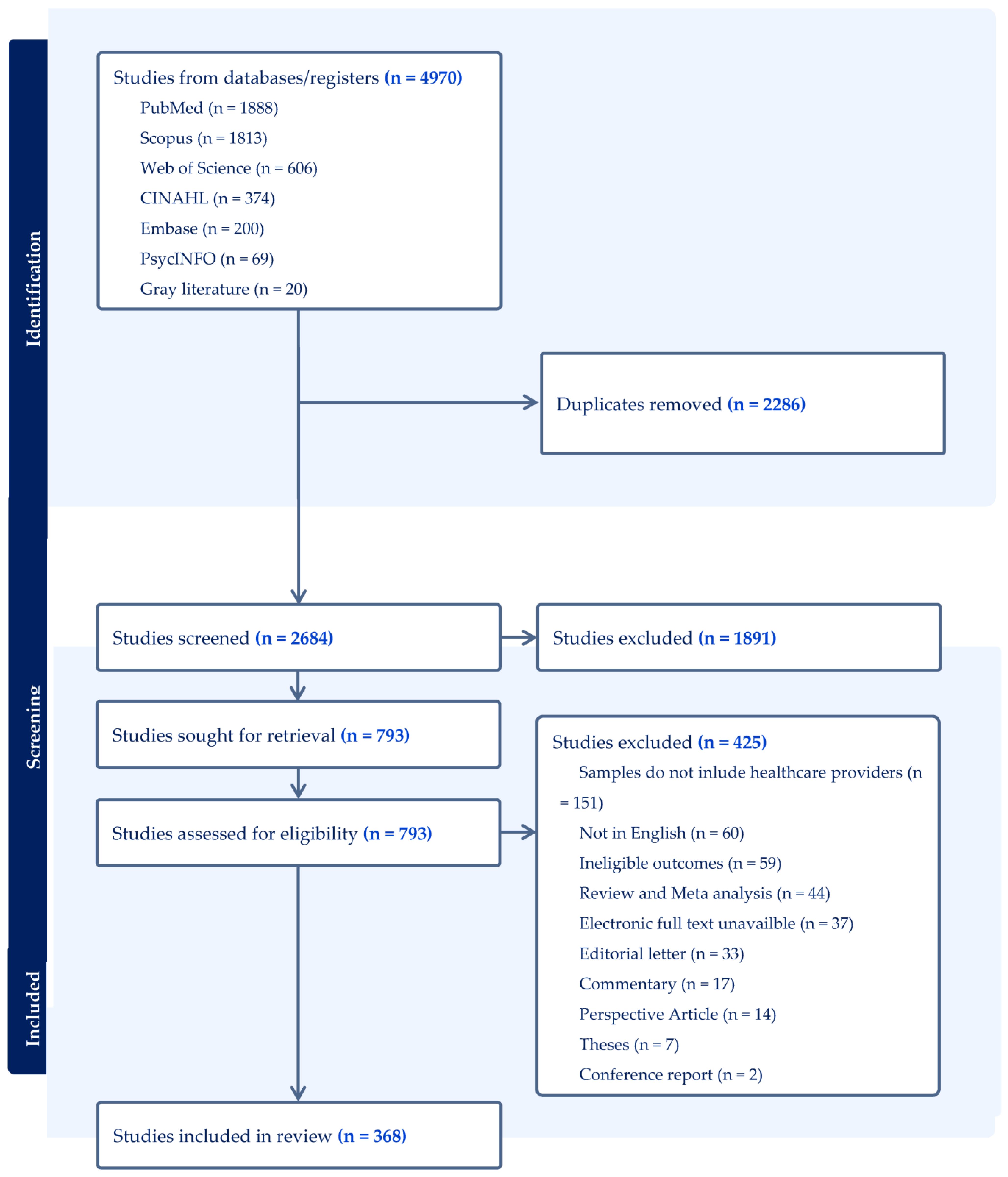
2.1. Literature Search
2.2. Study Extraction
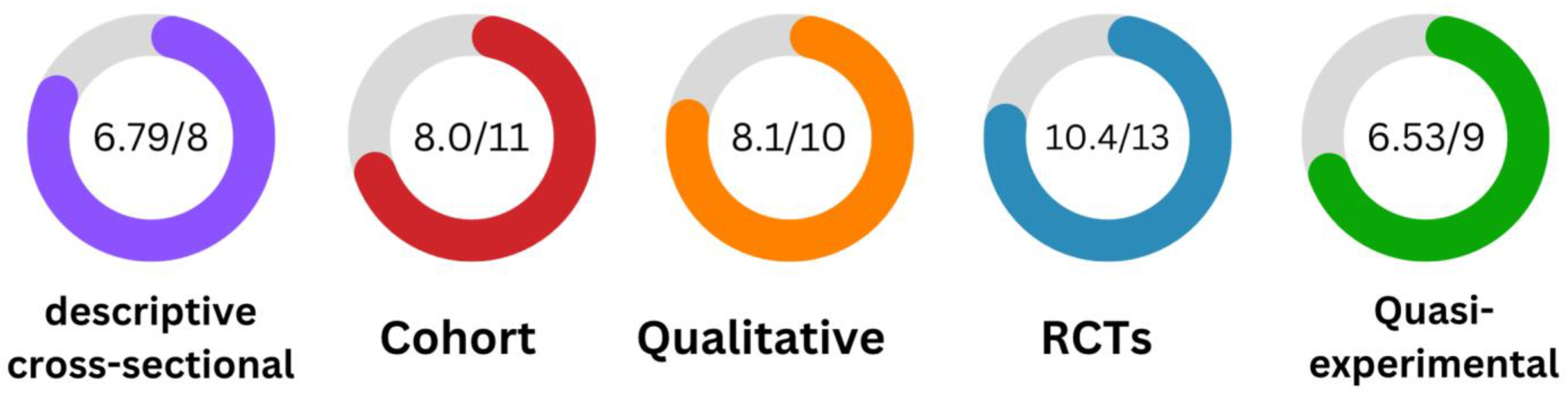
2.3. Quality Assessment
2.4. Narrative Synthesis
3. Results
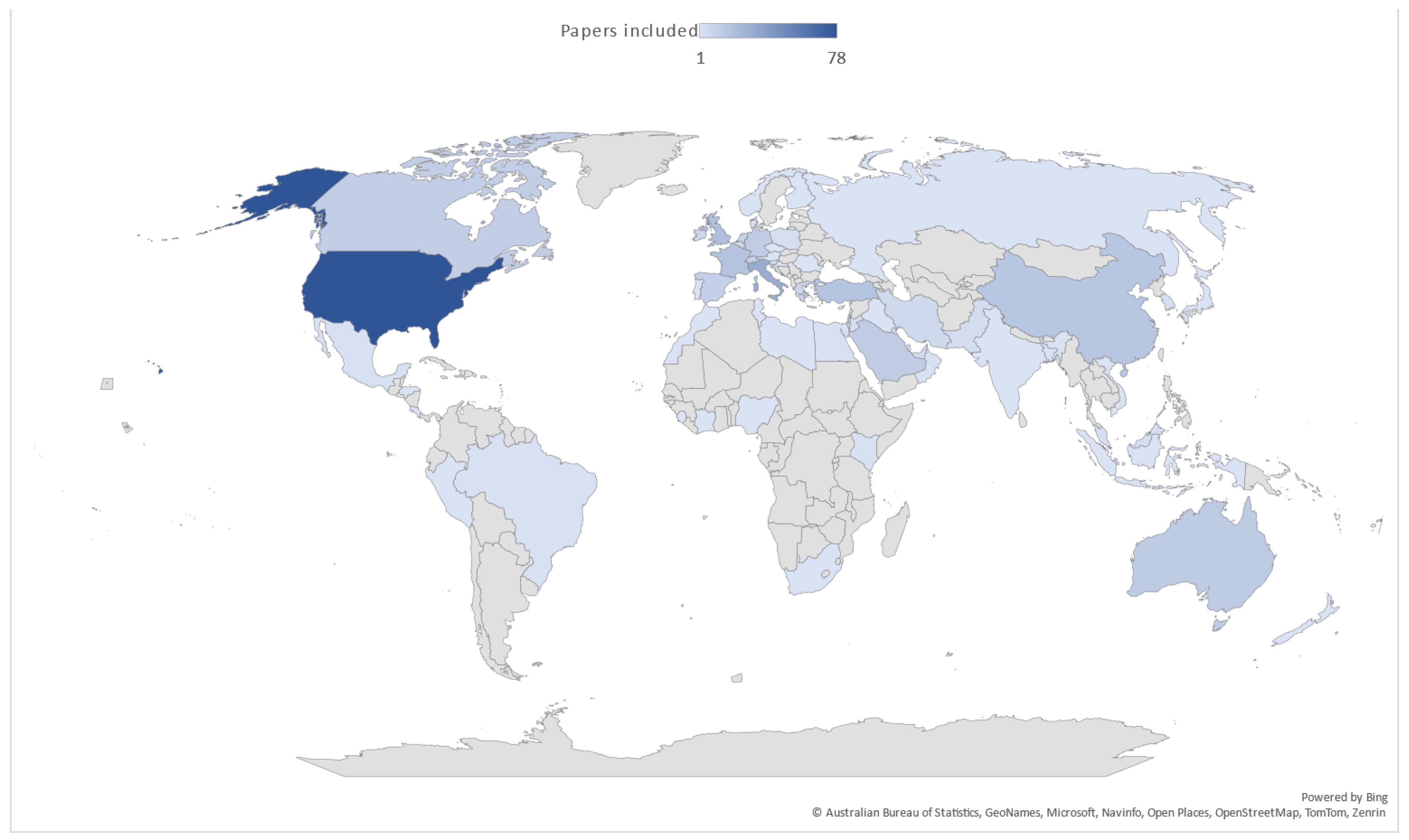
3.1. Study Characteristics
3.2. Exploring Key Themes: HCPs’ Attitudes toward Influenza Vaccination
3.2.1. Fostering Positive Views: Factors Promoting Attitudes toward Influenza Vaccines
3.2.2. Navigating Hesitancy: Barriers and Challenges to Attitudes on Influenza Vaccines
3.2.3. Empowering Change: Interventions and Their Impact on HCPs’ Attitudes
3.2.4. Pandemic Overlap: Intersecting Attitudes toward Influenza and COVID-19 Vaccines
3.2.5. Twin Challenges: Mandatory Policy Impact on Attitudes and Influenza Vaccination
4. Discussion
4.1. Prospects for Future Research
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Influenza (Seasonal). World Health Organization. 3 October 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 2 September 2023).
- Centers for Disease Control and Prevention. Disease Burden of Flu. Centers for Disease Control and Prevention. 4 October 2022. Available online: https://www.cdc.gov/flu/about/burden/index.html (accessed on 2 September 2023).
- Grohskopf, L.A.; Sokolow, L.Z.; Olsen, S.J. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2021–2022 Influenza Season. MMWR Recomm. Rep. 2021, 70, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Dormitzer, P.R.; Suphaphiphat, P.; Gibson, D.G.; Wentworth, D.E.; Stockwell, T.B.; Algire, M.A.; Alperovich, N.; Barro, M.; Brown, D.M.; Craig, S.; et al. Synthetic Generation of Influenza Vaccine Viruses for Rapid Response to Pandemics. Sci. Transl. Med. 2013, 5, 185ra68. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F. The human antibody response to influenza A virus infection and vaccination. Nat. Rev. Immunol. 2019, 19, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Skowronski, D.M.; Janjua, N.Z.; De Serres, G.; Sabaiduc, S.; Eshaghi, A.; Dickinson, J.A.; Fonseca, K.; Winter, A.-L.; Gubbay, J.B.; Krajden, M.; et al. Low 2012–13 Influenza Vaccine Effectiveness Associated with Mutation in the Egg-Adapted H3N2 Vaccine Strain Not Antigenic Drift in Circulating Viruses. PLoS ONE 2014, 9, e92153. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.G.; Tay, E.L.; Kelly, H. Variable Definitions of the Influenza Season and Their Impact on Vaccine Effectiveness Estimates. Vaccine 2013, 31, 4280–4283. [Google Scholar] [CrossRef]
- Jit, M.; Newall, A.T.; Beutels, P. Key issues for estimating the impact and cost-effectiveness of seasonal influenza vaccination strategies. Hum. Vaccines Immunother. 2013, 9, 834–840. [Google Scholar] [CrossRef]
- Ferdinands, J.M.; Olsho, L.E.W.; Agan, A.A.; Bhat, N.; Sullivan, R.M.; Hall, M.; Mourani, P.M.; Thompson, M.; Randolph, A.G. Effectiveness of influenza vaccine against life-threatening RT-PCR-confirmed influenza illness in US children, 2010–2012. J. Infect. Dis. 2014, 210, 674–683. [Google Scholar] [CrossRef]
- Ozawa, S.; Portnoy, A.; Getaneh, H.; Clark, S.; Knoll, M.; Bishai, D.; Yang, H.K.; Patwardhan, P.D. Modeling the economic burden of adult vaccine-preventable diseases in the United States. Health Aff. 2016, 35, 2124–2132. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Estimating Seasonal Influenza-Associated Deaths in the United States: CDC Study Confirms Variability of Flu. Available online: https://www.cdc.gov/flu/about/burden/faq.htm#deaths (accessed on 15 September 2023).
- Baguelin, M.; Flasche, S.; Camacho, A.; Demiris, N.; Miller, E.; Edmunds, W.J. Assessing optimal target populations for influenza vaccination programmes: An evidence synthesis and modelling study. PLoS Med. 2013, 10, e1001527. [Google Scholar] [CrossRef]
- Uyeki, T.M. High-risk groups for influenza complications. JAMA 2020, 324, 2334. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Information for Health Professionals. Available online: https://www.cdc.gov/flu/professionals/index.htm (accessed on 2 September 2023).
- Vorsters, A.; Bonanni, P.; Maltezou, H.C.; Yarwood, J.; Brewer, N.T.; Bosch, F.X.; Hanley, S.; Cameron, R.; Franco, E.L.; Arbyn, M.; et al. The role of healthcare providers in HPV vaccination programs–A meeting report. Papillomavirus Res. 2019, 8, 100183. [Google Scholar] [CrossRef] [PubMed]
- Stöcker, A.; Hoffmann, J.; Mause, L.; Neufeind, J.; Ohnhäuser, T.; Scholten, N. What impact does the attitude toward COVID-19 vaccination have on physicians as vaccine providers? A cross sectional study from the German outpatient sector. Vaccine 2023, 41, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza vaccination in healthcare workers: A comprehensive critical appraisal of the literature. Hum. Vaccines Immunother. 2018, 14, 772–789. [Google Scholar] [CrossRef] [PubMed]
- Tanner, A.R.; Dorey, R.B.; Brendish, N.J.; Clark, T.W. Influenza vaccination: Protecting the most vulnerable. Eur. Respir. Rev. 2021, 30, 200258. [Google Scholar] [CrossRef] [PubMed]
- Guillari, A.; Polito, F.; Pucciarelli, G.; Serra, N.; Gargiulo, G.; Esposito, M.R.; Botti, S.; Rea, T.; Simeone, S. Influenza vaccination and healthcare workers: Barriers and predisposing factors. A literature review. Acta Biomed. 2021, 92 (Suppl. 2), e2021004. [Google Scholar]
- Corace, K.M.; Srigley, J.A.; Hargadon, D.P.; Yu, D.; MacDonald, T.K.; Fabrigar, L.R.; Garber, G.E. Using behavior change frameworks to improve healthcare worker influenza vaccination rates: A systematic review. Vaccine 2016, 34, 3235–3242. [Google Scholar] [CrossRef]
- Siani, A. Vaccine hesitancy and refusal: History, causes, mitigation strategies. In Integrated Science of Global Epidemics; Springer International Publishing: Cham, Switzerland, 2023; pp. 503–517. [Google Scholar]
- Brügger, N. Tracing a historical development of conspiracy theory networks on the web: The hyperlink network of vaccine hesitancy on the Danish web 2006–2015. Convergence 2022, 28, 962–982. [Google Scholar] [CrossRef]
- Alamoodi, A.; Zaidan, B.; Al-Masawa, M.; Taresh, S.M.; Noman, S.; Ahmaro, I.Y.; Garfan, S.; Chen, J.; Ahmed, M.; Zaidan, A.; et al. Multi-perspectives systematic review on the applications of sentiment analysis for vaccine hesitancy. Comput. Biol. Med. 2021, 139, 104957. [Google Scholar] [CrossRef]
- Goldenberg Maya, J. Public misunderstanding of science? Reframing the problem of vaccine hesitancy. Perspect. Sci. 2016, 24, 552–581. [Google Scholar] [CrossRef]
- Rashid, H.; Yin, J.K.; Ward, K.; King, C.; Seale, H.; Booy, R. Assessing interventions to improve influenza vaccine uptake among health care workers. Health Aff. 2016, 35, 284–292. [Google Scholar] [CrossRef]
- To, K.W.; Lai, A.; Lee, K.C.; Koh, D.; Lee, S.S. Increasing the coverage of influenza vaccination in healthcare workers: Review of challenges and solutions. J. Hosp. Infect. 2016, 94, 133–142. [Google Scholar] [CrossRef]
- Schumacher, S.; Salmanton-García, J.; Cornely, O.A.; Mellinghoff, S.C. Increasing influenza vaccination coverage in healthcare workers: A review on campaign strategies and their effect. Infection 2021, 49, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Qi, X.; Li, Q.; Tang, W.; Su, K.; Jia, M.; Yang, W.; Xia, Y.; Xiong, Y.; Qi, L.; et al. A Systematic Review and Meta-Analysis of Seasonal Influenza Vaccination of Health Workers. Vaccines 2021, 9, 1104. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Corradi, A.; Voglino, G.; Catozzi, D.; Olivero, E.; Corezzi, M.; Bert, F.; Siliquini, R. Healthcare Workers’ (HCWs) attitudes towards mandatory influenza vaccination: A systematic review and meta-analysis. Vaccine 2021, 39, 901–914. [Google Scholar] [CrossRef] [PubMed]
- Kong, G.; Lim, N.A.; Chin, Y.H.; Ng, Y.P.M.; Amin, Z. Effect of COVID-19 Pandemic on Influenza Vaccination Intention: A Meta-Analysis and Systematic Review. Vaccines 2022, 10, 606. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Covidence. Covidence: Better Systematic Review Management. 2023. Available online: https://www.covidence.org/ (accessed on 2 September 2023).
- Rodgers, M.; Sowden, A.; Petticrew, M.; Arai, L.; Roberts, H.; Britten, N.; Popay, J. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. A Product from the ESRC Methods Programme (Version 1); Lancaster University: Lancashire, UK, 2006. [Google Scholar]
- Maltezou, H.C.; Theodoridou, K.; Ledda, C.; Rapisarda, V.; Theodoridou, M. Vaccination of healthcare workers: Is mandatory vaccination needed? Expert Rev. Vaccines 2019, 18, 5–13. [Google Scholar] [CrossRef]
- Informal Working Group. Final Report from the Informal Working Group on Strategic Objective 2 (SO2) of the Global Vaccine Action Plan (GVAP) to the Strategic Advisory Group of Experts (SAGE) of the World Health Organization GVAP Working Group. 2017. Available online: https://www.unicef.org/immunization/files/GVAP_SO2_Report.pdf (accessed on 16 August 2019).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Theme | Meaning |
|---|---|
| (1) Fostering Positive Views: Factors Promoting Attitudes toward Influenza Vaccination |
|
| (2) Navigating Hesitancy: Barriers and Challenges to Attitudes on Influenza Vaccination |
|
| (3) Empowering Change: Interventions and Their Impact on HCPs’ Attitudes |
|
| (4) Pandemic Overlap: Intersecting Attitudes toward Influenza and COVID-19 Vaccination |
|
| (5) Twin Challenges: Mandatory Policy Impact on Attitudes and Influenza Vaccination |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dardas, L.A.; Al-leimon, O.; Jaber, A.R.; Saadeh, M.; Al-leimon, A.; Al-Hurani, A.; Jaber, A.-R.; Aziziye, O.; Al-salieby, F.; Aljahalin, M.; et al. Flu Shots Unveiled: A Global Systematic Review of Healthcare Providers’ Uptake of, Perceptions, and Attitudes toward Influenza Vaccination. Vaccines 2023, 11, 1760. https://doi.org/10.3390/vaccines11121760
Dardas LA, Al-leimon O, Jaber AR, Saadeh M, Al-leimon A, Al-Hurani A, Jaber A-R, Aziziye O, Al-salieby F, Aljahalin M, et al. Flu Shots Unveiled: A Global Systematic Review of Healthcare Providers’ Uptake of, Perceptions, and Attitudes toward Influenza Vaccination. Vaccines. 2023; 11(12):1760. https://doi.org/10.3390/vaccines11121760
Chicago/Turabian StyleDardas, Latefa Ali, Obada Al-leimon, Abdel Rahman Jaber, Mohammed Saadeh, Ahmad Al-leimon, Ahmad Al-Hurani, Abdul-Raheem Jaber, Omer Aziziye, Fadi Al-salieby, Mohammad Aljahalin, and et al. 2023. "Flu Shots Unveiled: A Global Systematic Review of Healthcare Providers’ Uptake of, Perceptions, and Attitudes toward Influenza Vaccination" Vaccines 11, no. 12: 1760. https://doi.org/10.3390/vaccines11121760
APA StyleDardas, L. A., Al-leimon, O., Jaber, A. R., Saadeh, M., Al-leimon, A., Al-Hurani, A., Jaber, A.-R., Aziziye, O., Al-salieby, F., Aljahalin, M., & Van de Water, B. (2023). Flu Shots Unveiled: A Global Systematic Review of Healthcare Providers’ Uptake of, Perceptions, and Attitudes toward Influenza Vaccination. Vaccines, 11(12), 1760. https://doi.org/10.3390/vaccines11121760