
Association between COVID-19 Primary Vaccination and Severe Disease Caused by SARS-CoV-2 Delta Variant among Hospitalized Patients: A Belgian Retrospective Cohort Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
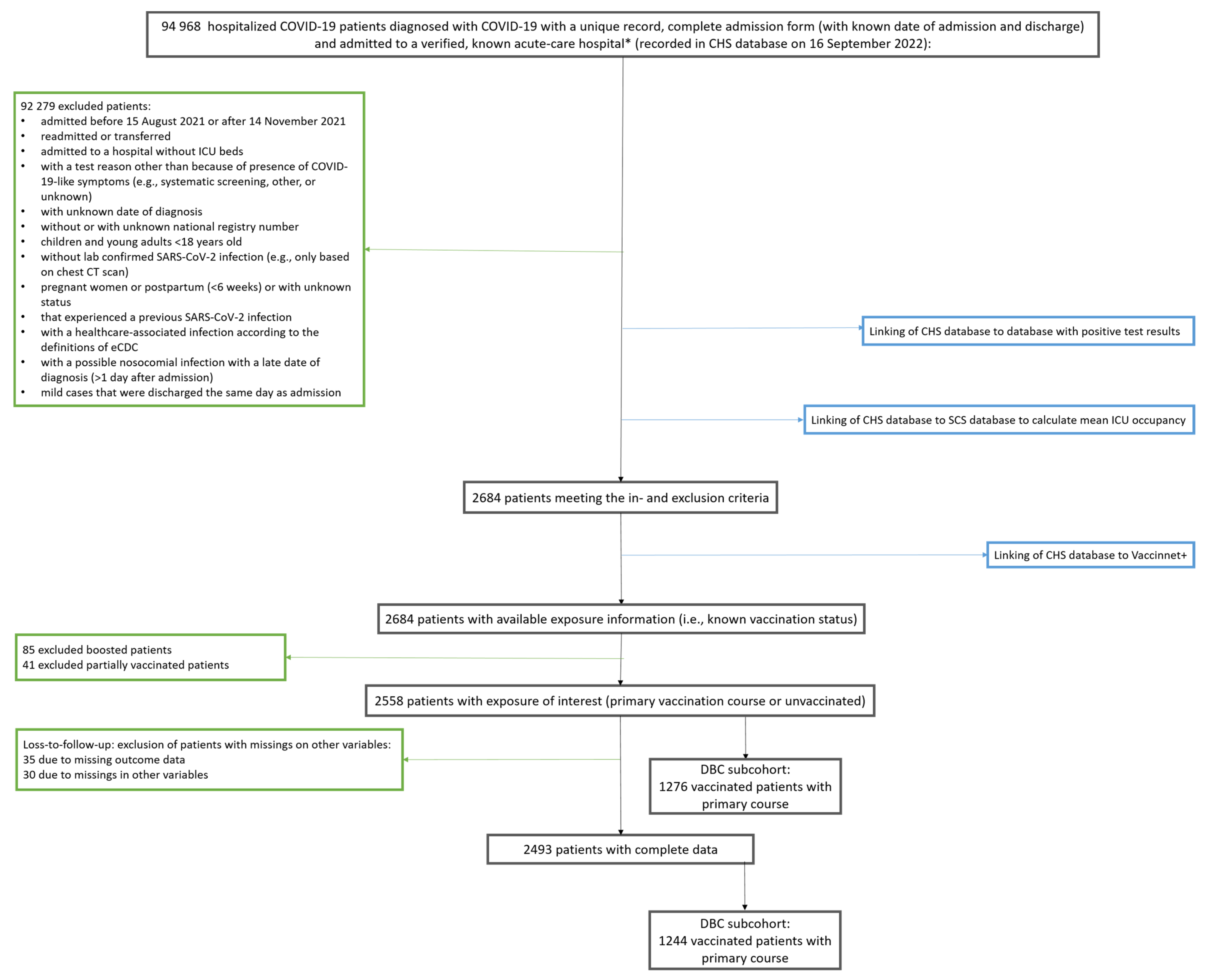
2.2. Study Population
2.3. Operationalization of Variables
2.3.1. Outcomes
2.3.2. Exposure
2.3.3. Covariates
2.4. Statistical Analyses
3. Results
3.1. Study Population
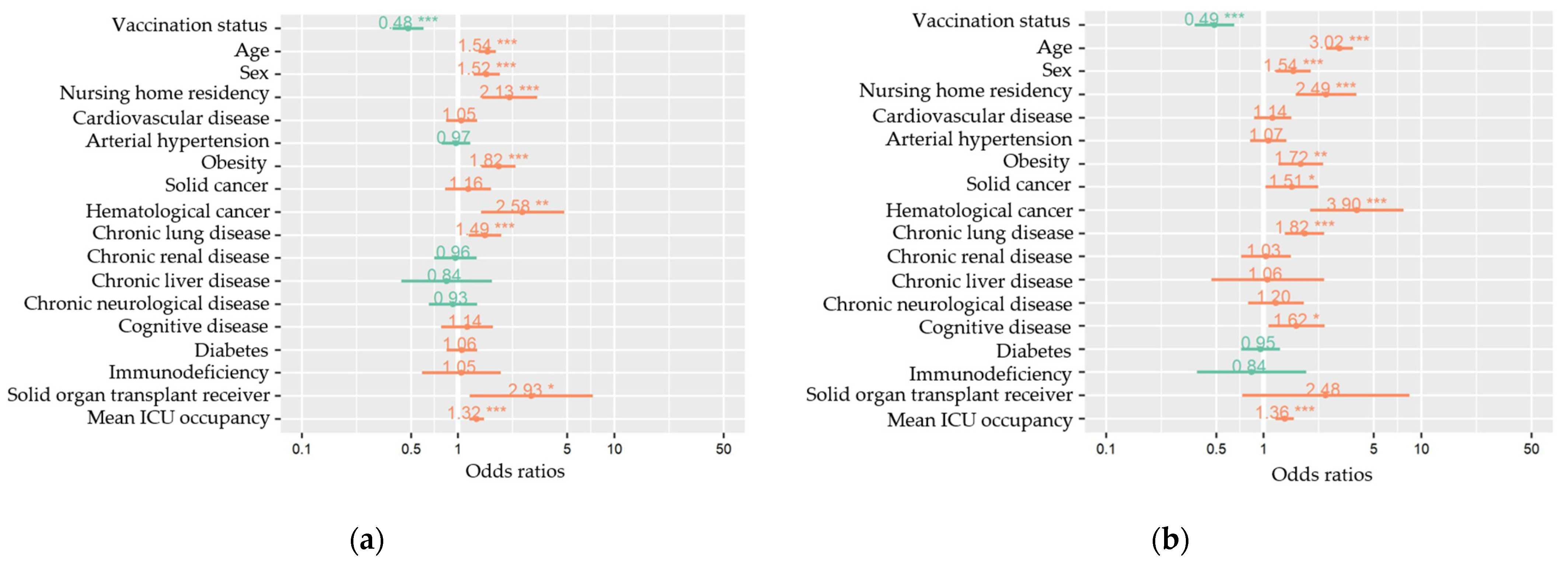
3.2. Effects of Vaccination Status on Disease Progression to Severe COVID-19 and In-Hospital Death
3.3. Exploratory Vaccine Brand Comparison among Delta Breakthrough Cases
4. Discussion
4.1. Strengths and Limitations
4.2. Generalizability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort n (%) 2558 | Primary Vaccination Course n (%) 1276 (49.9) | Unvaccinated n (%) 1282 (50.1) |
|---|---|---|---|
| Baseline characteristics | |||
| Age in years, median (IQR) [range] | 67 (53.5–80.5) [18–112] | 75 (66–84) [18–100] | 56 (43.1–68.9) [18–112] |
| Sex | |||
| Women | 1065 (41.6) | 498 (39) | 567 (44.2) |
| Men | 1493 (58.4) | 778 (61) | 715 (55.8) |
| Nursing home residency | |||
| Nursing home resident | 136 (5.3) | 113 (8.9) | 23 (1.8) |
| Living with a level of independence | 2394 (93.6) | 1145 (89.7) | 1249 (97.4) |
| Presence of comorbidities | |||
| No comorbidities | 627 (24.5) | 150 (11.8) | 477 (37.2) |
| Comorbidities | 1931 (75.5) | 1126 (88.2) | 805 (62.8) |
| Cardiovascular disease | 720 (28.1) | 519 (40.7) | 201 (15.7) |
| Arterial hypertension | 927 (36.2) | 560 (43.9) | 367 (28.6) |
| Diabetes | 575 (22.5) | 341 (26.7) | 234 (18.3) |
| Chronic renal disease | 277 (10.8) | 200 (15.7) | 77 (6) |
| Chronic liver disease | 57 (2.2) | 32 (2.5) | 25 (2) |
| Chronic neurologic or neuromuscular disease | 197 (7.7) | 139 (10.9) | 58 (4.5) |
| Cognitive impairment | 160 (6.3) | 119 (9.3) | 41 (3.2) |
| Immunocompromised disease | 82 (3.2) | 61 (4.8) | 21 (1.6) |
| Chronic lung disease | 454 (17.7) | 324 (25.4) | 130 (10.1) |
| Solid cancer | 204 (8.0) | 147 (11.5) | 57 (4.4) |
| Hematological cancer | 53 (2.1) | 39 (3.1) | 14 (1.1) |
| Solid organ transplantation | 26 (1) | 23 (1.8) | 3 (0.2) |
| Obesity | 414 (16.2) | 171 (13.4) | 243 (19) |
| Number of comorbidities, median [range] | 1 [0–8] | 2 [0–8] | 1 [0–8] |
| Determinants | |||
| Mean ICU occupancy rate in %, median (IQR) [range] | 18.5 (10.2–26.8) [0–75] | 18.5 (10.7–26.4) [0–69.2] | 18.5 (9.8–27) [0–75] |
| Length of stay in days, median (IQR) [range] | 7 (2.5–11.5) [1–365] | 8 (3.5–12.5) [1–365] | 7 (3–11) [1–193] |
| ICU admission | 500 (19.5) | 194 (15.2) | 306 (23.9) |
| ARDS | 297 (11.6) | 113 (8.9) | 184 (14.4) |
| In-hospital death | 400 (15.6) | 228 (17.9) | 172 (13.4) |
| Severe COVID-19 | 767 (30) | 360 (28.2) | 407 (31.7) |
| Characteristics | mRNA n (%) 854 (66.9) | AZ n (%) 331 (25.9) | J&J n (%) 91 (7.1) |
|---|---|---|---|
| Baseline characteristics | |||
| Age in years, median (IQR) [range] | 67 (53.5–80.5) [18–112] | 75 (66–84) [18–100] | 56 (43.1–68.9) [18–112] |
| Sex | |||
| Women | 1065 (41.6) | 498 (39) | 567 (44.2) |
| Men | 1493 (58.4) | 778 (61) | 715 (55.8) |
| Nursing home residency | |||
| Nursing home resident | 136 (5.3) | 113 (8.9) | 23 (1.8) |
| Living with a level of independence | 2394 (93.6) | 1145 (89.7) | 1249 (97.4) |
| Presence of comorbidities | |||
| No comorbidities | 627 (24.5) | 150 (11.8) | 477 (37.2) |
| Comorbidities | 1931 (75.5) | 1126 (88.2) | 805 (62.8) |
| Cardiovascular disease | 720 (28.1) | 519 (40.7) | 201 (15.7) |
| Arterial hypertension | 927 (36.2) | 560 (43.9) | 367 (28.6) |
| Diabetes | 575 (22.5) | 341 (26.7) | 234 (18.3) |
| Chronic renal disease | 277 (10.8) | 200 (15.7) | 77 (6) |
| Chronic liver disease | 57 (2.2) | 32 (2.5) | 25 (2) |
| Chronic neurologic or neuromuscular disease | 197 (7.7) | 139 (10.9) | 58 (4.5) |
| Cognitive impairment | 160 (6.3) | 119 (9.3) | 41 (3.2) |
| Immunocompromised disease | 82 (3.2) | 61 (4.8) | 21 (1.6) |
| Chronic lung disease | 454 (17.7) | 324 (25.4) | 130 (10.1) |
| Solid cancer | 204 (8.0) | 147 (11.5) | 57 (4.4) |
| Hematological cancer | 53 (2.1) | 39 (3.1) | 14 (1.1) |
| Solid organ transplantation | 26 (1) | 23 (1.8) | 3 (0.2) |
| Obesity | 414 (16.2) | 171 (13.4) | 243 (19) |
| Number of comorbidities, median [range] | 1 [0–8] | 2 [0–8] | 1 [0–8] |
| Time since vaccination in days, median (IQR) [range] | 67 (53.5–80.5) [18–112] | 75 (66–84) [18–100] | 56 (43.1–68.9) [18–112] |
| Determinants | |||
| Mean ICU occupancy rate in %, median (IQR) [range] | 18.5 (10.2–26.8) [0–75] | 18.5 (10.7–26.4) [0–69.2] | 18.5 (9.8–27) [0–75] |
| Length of stay in days, median (IQR) [range] | 7 (2.5–11.5) [1–365] | 8 (3.5–12.5) [1–365] | 7 (3–11) [1–193] |
| ICU admission | 500 (19.5) | 194 (15.2) | 306 (23.9) |
| ARDS | 297 (11.6) | 113 (8.9) | 184 (14.4) |
| Death | 400 (15.6) | 228 (17.9) | 172 (13.4) |
| Severe COVID-19 | 767 (30) | 360 (28.2) | 407 (31.7) |
Appendix B
| Odds Ratios and 95% Confidence Intervals for Severe COVID-19 and Death | ||||
|---|---|---|---|---|
| Model | Severe COVID-19 | Death | ||
| OR | 95% CI | OR | 95% CI | |
| Mixed effects logistic regression (only significant variables) | 0.4852 J | 0.3874; 0.6077 | 0.5026 K | 0.3769; 0.6703 |
Appendix C
| Odds Ratios and 95% Confidence Intervals for Severe COVID-19 | |||
|---|---|---|---|
| Age ≤ 75 y old L | |||
| Ref category → | J&J | AZ | mRNA |
| J&J | 1.55 (0.72; 3.37) | 0.94 (0.44; 2.00) | |
| AZ | 0.64 (0.30; 1.40) | 0.61 (0.37; 1.01) | |
| mRNA | 1.06 (0.50; 2.25) | 1.65 (0.99; 2.73) | |
| Age > 75 y old M | |||
| J&J | 2.71 (1.24; 5.90) | 2.34 (1.16; 4.72) | |
| AZ | 0.37 (0.17; 0.80) | 0.86 (0.55; 1.37) | |
| mRNA | 0.43 (0.21; 0.86) | 1.16 (0.73; 1.83) | |
| Odds Ratios and 95% Confidence Intervals for In-hospital Death | |||
|---|---|---|---|
| Age ≤ 75 y Old N | |||
| Ref category → | J&J | AZ | mRNA |
| J&J | 2.00 (0.69; 5.82) | 1.50 (0.56; 4.00) | |
| AZ | 0.50 (0.17; 1.45) | 0.75 (0.40; 1.40) | |
| mRNA | 0.67 (0.25; 1.78) | 1.33 (0.72; 2.49) | |
| Age > 75 y old O | |||
| J&J | 3.13 (1.40; 7.01) | 3.05 (1.48; 6.26) | |
| AZ | 0.32 (0.14; 0.72) | 0.97 (0.59; 1.60) | |
| mRNA | 0.32 (0.16; 0.67) | 1.03 (0.62; 1.69) | |
References
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and Safety of SARS-CoV-2 Vaccine in Real-World Studies: A Systematic Review and Meta-Analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef]
- Sciensano. COVID-19—COVID-19 Wekelijks Epidemiologisch Bulletin van 22 April 2022; Sciensano: Brussels, Belgium, 2022. [Google Scholar]
- Tan, L.Y.; Komarasamy, T.V.; Rmt Balasubramaniam, V. Hyperinflammatory Immune Response and COVID-19: A Double-Edged Sword. Front. Immunol. 2021, 12, 742941. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. MRNA Vaccines Induce Durable Immune Memory to SARS-CoV-2 and Variants of Concern. Science 2021, 374, abm0829. [Google Scholar] [CrossRef] [PubMed]
- Facon, P. Advies voor de Operationalisering van de Vaccinatiestrategie COVID-19 voor België Taskforce Operationalization of the Vaccination Strategy; Report; Regeringscommissariaat: Corona, Belgium, 2020; p. 39. Available online: https://cdn.nimbu.io/s/yba55wt/assets/Regeringscommissariaat%20Corona%20-%20Vaccinatiestrategie%20voor%20Belgi_.pdf (accessed on 18 November 2022).
- Sciensano. Belgium COVID-19 Epidemiological Situation: Vaccination 2021. Available online: https://Datastudio.Google.Com/Embed/Reporting/C14a5cfc-Cab7-4812-848c-0369173148ab/Page/P_j1f02pfnpc (accessed on 18 November 2022).
- Harder, T.; Külper-Schiek, W.; Reda, S.; Treskova-Schwarzbach, M.; Koch, J.; Vygen-Bonnet, S.; Wichmann, O. Effectiveness of COVID-19 Vaccines against SARS-CoV-2 Infection with the Delta (B.1.617.2) Variant: Second Interim Results of a Living Systematic Review and Meta-Analysis, 1 January to 25 August 2021. Eurosurveillance 2021, 26, 2100920. [Google Scholar] [CrossRef]
- Sciensano. COVID-19 Surveillance: Frequently Asked Questions; 2.3. What Dates Define the Waves of the COVID-19 Epidemic in Belgium? 24 November 2021. Available online: https://Covid-19.Sciensano.Be/Sites/Default/Files/Covid19/COVID-19_FAQ_ENG_final.Pdf (accessed on 18 November 2022).
- Tian, D.; Sun, Y.; Zhou, J.; Ye, Q. The Global Epidemic of the SARS-CoV-2 Delta Variant, Key Spike Mutations and Immune Escape. Front. Immunol. 2021, 12, 751778. [Google Scholar] [CrossRef] [PubMed]
- Chia, P.; Xiang Ong, S.; Chiew, C.; Ang, L.; Chavatte, J.; Mak, T. Virological and Serological Kinetics of SARS-CoV-2 Delta Variant Vaccine Breakthrough Infections: A Multicentre Cohort Study. Clin. Microbiol. Infect. 2022, 28, 612.e1–612.e7. [Google Scholar] [CrossRef]
- Kissler, S.M.; Fauver, J.R.; Mack, C.; Tai, C.G.; Breban, M.I.; Watkins, A.E.; Samant, R.M.; Anderson, D.J.; Metti, J.; Khullar, G.; et al. Viral Dynamics of SARS-CoV-2 Variants in Vaccinated and Unvaccinated Persons. N. Engl. J. Med. 2021, 385, 2489–2491. [Google Scholar] [CrossRef]
- de Michelena, P.; Torres, I.; Albert, E.; Bracho, A.; González-Candelas, F.; Navarro, D. Impact of Time Elapsed since Full Vaccination on SARS-CoV-2 RNA Load in Delta-Variant Breakthrough COVID-19. J. Infect. 2022, 84, 579–613. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.; Grüne, B.; Buess, M.; Joisten, C.; Klobucnik, J.; Nießen, J.; Patten, D.; Wolff, A.; Wiesmüller, G.A.; Kossow, A.; et al. COVID-19 Breakthrough Infections and Transmission Risk: Real-World Data Analyses from Germany’s Largest Public Health Department (Cologne). Vaccines 2021, 9, 1267. [Google Scholar] [CrossRef]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community Transmission and Viral Load Kinetics of the SARS-CoV-2 Delta (B.1.617.2) Variant in Vaccinated and Unvaccinated Individuals in the UK: A Prospective, Longitudinal, Cohort Study. Lancet Infect. Dis. 2022, 22, 183–195. [Google Scholar] [CrossRef]
- Siedner, M.J.; Boucau, J.; Gilbert, R.F.; Uddin, R.; Luu, J.; Haneuse, S.; Vyas, T.; Reynolds, Z.; Iyer, S.; Chamberlin, G.C.; et al. Duration of Viral Shedding and Culture Positivity with Postvaccination SARS-CoV-2 Delta Variant Infections. JCI Insight 2022, 7, 155483. [Google Scholar] [CrossRef]
- Levine-Tiefenbrun, M.; Yelin, I.; Alapi, H.; Katz, R.; Herzel, E.; Kuint, J.; Chodick, G.; Gazit, S.; Patalon, T.; Kishony, R. Viral Loads of Delta-Variant SARS-CoV-2 Breakthrough Infections after Vaccination and Booster with BNT162b2. Nat. Med. 2021, 27, 2108–2110. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A. Severity of Disease Among Adults Hospitalized with Laboratory-Confirmed COVID-19 Before and During the Period of SARS-CoV-2 B.1.617.2 (Delta) Predominance—COVID-NET, 14 States, January–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1513–1519. [Google Scholar] [CrossRef]
- Fisman, D.N.; Tuite, A.R. Evaluation of the Relative Virulence of Novel SARS-CoV-2 Variants: A Retrospective Cohort Study in Ontario, Canada. CMAJ 2021, 193, E1619–E1625. [Google Scholar] [CrossRef]
- McKeigue, P.M.; McAllister, D.A.; Hutchinson, S.J.; Robertson, C.; Stockton, D.; Colhoun, H.M. Vaccine Efficacy against Severe COVID-19 in Relation to Delta Variant (B.1.617.2) and Time since Second Dose in Patients in Scotland (REACT-SCOT): A Case-Control Study. Lancet Respir. Med. 2022, 10, 566–572. [Google Scholar] [CrossRef]
- Stupica, D.; Collinet-Adler, S.; Kejžar, N.; Jagodic, Z.; Poljak, M.; Nahtigal Klevišar, M. The Impact of SARS-CoV-2 Primary Vaccination in a Cohort of Patients Hospitalized for Acute COVID-19 during Delta Variant Predominance. J. Clin. Med. 2022, 11, 1191. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Leibner, E.S.; Hackett, A.; Maguire, K.; Mashriqi, N.; Kohli-Seth, R. The Third Wave: Comparing Seasonal Trends in COVID-19 Patient Data at a Large Hospital System in New York City. Crit. Care Explor. 2022, 4, e0653. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between MRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Self, W.H.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; McNeal, T.; et al. Effectiveness of MRNA Vaccination in Preventing COVID-19-Associated Invasive Mechanical Ventilation and Death—United States, March 2021-January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Toker, İ.; Kılınç Toker, A.; Turunç Özdemir, A.; Çelik, İ.; Bol, O.; Bülbül, E. Vaccination Status among Patients with the Need for Emergency Hospitalizations Related to COVID-19. Am. J. Emerg. Med. 2022, 54, 102–106. [Google Scholar] [CrossRef]
- Van Goethem, N.; Vilain, A.; Wyndham-Thomas, C.; Deblonde, J.; Bossuyt, N.; Lernout, T.; Rebolledo Gonzalez, J.; Quoilin, S.; Melis, V.; Van Beckhoven, D. Rapid Establishment of a National Surveillance of COVID-19 Hospitalizations in Belgium. Arch. Public Health 2020, 78, 121. [Google Scholar] [CrossRef]
- Van Goethem, N.; Serrien, B.; Vandromme, M.; Wyndham-Thomas, C.; Catteau, L.; Brondeel, R.; Klamer, S.; Meurisse, M.; Cuypers, L.; André, E.; et al. Conceptual Causal Framework to Assess the Effect of SARS-CoV-2 Variants on COVID-19 Disease Severity among Hospitalized Patients. Arch. Public Health 2021, 79, 185. [Google Scholar] [CrossRef] [PubMed]
- Cuypers, L.; Maes, P.; Janssenswillen, S.; Keyaerts, E.; Baele, G.; Dellicour, S.; Wenseleers, T.; Potter, B.; Wollants, E.; Van Ranst, M.; et al. Genomic Surveillance of SARS-CoV-2 in Belgium—Situation Update 10th of August 2021; Report; National Reference Laboratory (UZ Leuven & KU Leuven): Leuven, Belgium, 2021. [Google Scholar]
- Cuypers, L.; Maes, P.; Janssenswillen, S.; Keyaerts, E.; Baele, G.; Dellicour, S.; Wenseleers, T.; Potter, B.; Wollants, E.; Van Ranst, M.; et al. Genomic Surveillance of SARS-CoV-2 in Belgium—Situation Update 17th of August 2021; Report; National Reference Laboratory (UZ Leuven & KU Leuven): Leuven, Belgium, 2021. [Google Scholar]
- Cuypers, L.; Maes, P.; Keyaerts, E.; Baele, G.; Dellicour, S.; Wenseleers, T.; Potter, B.; Janssenswillen, S.; Wollants, E.; Van Ranst, M.; et al. Genomic Surveillance of SARS-CoV-2 in Belgium—Situation Update 16th of November 2021; Report; National Reference Laboratory (UZ Leuven & KU Leuven): Leuven, Belgium, 2021. [Google Scholar]
- Cuypers, L.; Maes, P.; Dellicour, S.; Van Weyenbergh, J.; Keyaerts, E.; Baele, G.; Raymenants, J.; Wenseleers, T.; Potter, B.; Janssenswillen, S.; et al. Genomic Surveillance of SARS-CoV-2 in Belgium—Situation Update 30th of November 2021; Report; National Reference Laboratory (UZ Leuven & KU Leuven): Leuven, Belgium, 2021. [Google Scholar]
- Sciensano. Belgium COVID-19 Epidemiological Situation: Variants. 2021. Available online: Https://Datastudio.Google.Com/Embed/Reporting/C14a5cfc-Cab7-4812-848c-0369173148ab/Page/UrrUC (accessed on 18 November 2022).
- Surveillance Definitions for COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/surveillance-definitions (accessed on 22 April 2022).
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C.; Murthy, S.; Diaz, J.; Adhikari, N.K.; Angus, D.C.; Arabi, Y.M.; Baillie, K.; Bauer, M.; Berry, S.; Blackwood, B.; et al. A Minimal Common Outcome Measure Set for COVID-19 Clinical Research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Sciensano. COVID-19 Surveillance: Frequently Asked Questions; 10. Data for the Surveillance of Vaccination. Available online: Https://Covid-19.Sciensano.Be/Sites/Default/Files/Covid19/COVID-19_FAQ_ENG_final.Pdf (accessed on 18 November 2022).
- Asai, Y.; Nomoto, H.; Hayakawa, K.; Matsunaga, N.; Tsuzuki, S.; Terada, M.; Ohtsu, H.; Kitajima, K.; Suzuki, K.; Suzuki, T.; et al. Comorbidities as Risk Factors for Severe Disease in Hospitalized Elderly COVID-19 Patients by Different Age-Groups in Japan. Gerontology 2022, 68, 1027–1037. [Google Scholar] [CrossRef]
- Taccone, F.S.; Goethem, N.V.; Pauw, R.D.; Wittebole, X.; Blot, K.; Oyen, H.V.; Lernout, T.; Montourcy, M.; Meyfroidt, G.; Beckhoven, D.V. The Role of Organizational Characteristics on the Outcome of COVID-19 Patients Admitted to the ICU in Belgium. Lancet Reg. Health–Eur. 2021, 2, 100019. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.A.; Satti, L.; Bizanjo, M.; Ather, N.A. Comparison of Clinical Characteristics and Outcome Between Vaccinated and Non-Vaccinated Patients of COVID-19 During the Delta Variant-Dominated Fourth Wave in a Tertiary Care Hospital in Karachi, Pakistan. Cureus 2022, 14, e23726. [Google Scholar] [CrossRef] [PubMed]
- Fournier, P.-E.; Houhamdi, L.; Colson, P.; Cortaredona, S.; Delorme, L.; Cassagne, C.; Lagier, J.-C.; Chaudet, H.; Tissot-Dupont, H.; Giraud-Gatineau, A.; et al. SARS-CoV-2 Vaccination and Protection Against Clinical Disease: A Retrospective Study, Bouches-Du-Rhône District, Southern France, 2021. Front. Microbiol. 2022, 12, 796807. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Quadri, S.; AlAwadhi, A.I.; AlQahtani, M. COVID-19 Recovery Patterns Across Alpha (B.1.1.7) and Delta (B.1.617.2) Variants of SARS-CoV-2. Front. Immunol. 2022, 13, 812606. [Google Scholar] [CrossRef]
- Witkowski, J.M.; Fulop, T.; Bryl, E. Immunosenescence and COVID-19. Mech. Ageing Dev. 2022, 204, 111672. [Google Scholar] [CrossRef]
- French, G.; Hulse, M.; Nguyen, D.; Sobotka, K.; Webster, K.; Corman, J.; Aboagye-Nyame, B.; Dion, M.; Johnson, M.; Zalinger, B.; et al. Impact of Hospital Strain on Excess Deaths During the COVID-19 Pandemic—United States, July 2020–July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1613–1616. [Google Scholar] [CrossRef] [PubMed]
- Cavillot, L.; Van Loenhout, J.; Catteau, L.; Van den Borre, L.; De Pauw, R.; Blot, K.; Speybroeck, N.; Devleesschauwer, B.; Hubin, P. COVID-19 Vaccination Uptake in Belgium: Socioeconomic and Sociodemographic Disparities. Eur. J. Public Health 2022, 32, ckac129.046. [Google Scholar] [CrossRef]
- Fillmore, N.R.; La, J.; Zheng, C.; Doron, S.; Do, N.V.; Monach, P.A.; Branch-Elliman, W. The COVID-19 Hospitalization Metric in the Pre- and Postvaccination Eras as a Measure of Pandemic Severity: A Retrospective, Nationwide Cohort Study. Infect. Control Hosp. Epidemiol. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Griffith, G.J.; Morris, T.T.; Tudball, M.J.; Herbert, A.; Mancano, G.; Pike, L.; Sharp, G.C.; Sterne, J.; Palmer, T.M.; Davey Smith, G.; et al. Collider Bias Undermines Our Understanding of COVID-19 Disease Risk and Severity. Nat. Commun. 2020, 11, 5749. [Google Scholar] [CrossRef] [PubMed]

| Characteristics | Total Cohort n (%) 2493 | Primary Vaccination Course n (%) 1244 (49.9) | Unvaccinated n (%) 1249 (50.1) |
|---|---|---|---|
| Baseline characteristics | |||
| Age in years, median (IQR) [range] | 67 (52–67) [18–112] | 75 (65–75) [18–100] | 56 (43–56) [18–112] |
| Sex | |||
| Women | 1043 (41.8) | 486 (39.1) | 557 (44.6) |
| Men | 1450 (58.2) | 758 (60.9) | 692 (55.4) |
| Nursing home residency | |||
| Nursing home resident | 131 (5.3) | 109 (8.8) | 22 (1.8) |
| Living with a level of independence | 2362 (94.7) | 1135 (91.2) | 1227 (98.2) |
| Presence of comorbidities | |||
| No comorbidities | 611 (24.5) | 147 (11.8) | 464 (37.1) |
| Comorbidities | 1882 (75.5) | 1197 (88.2) | 785 (62.9) |
| Cardiovascular disease | 700 (28.1) | 508 (40.8) | 192 (15.4) |
| Arterial hypertension | 903 (36.2) | 543 (43.6) | 360 (28.8) |
| Diabetes | 556 (22.3) | 327 (26.3) | 229 (18.3) |
| Chronic renal disease | 270 (10.8) | 194 (15.6) | 76 (6.1) |
| Chronic liver disease | 51 (2) | 30 (2.4) | 21 (1.7) |
| Chronic neurologic or neuromuscular disease | 191 (7.7) | 134 (10.8) | 57 (4.6) |
| Cognitive impairment | 157 (6.3) | 116 (9.3) | 41 (3.3) |
| Immunocompromised disease | 80 (3.2) | 59 (4.7) | 21 (1.7) |
| Chronic lung disease | 439 (17.6) | 313 (25.2) | 126 (10.1) |
| Solid cancer | 201 (8.1) | 144 (11.6) | 57 (4.6) |
| Hematological cancer | 52 (2.1) | 38 (3.1) | 14 (1.1) |
| Solid organ transplantation | 26 (1) | 23 (1.8) | 3 (0.2) |
| Obesity | 406 (16.3) | 166 (13.3) | 240 (19.2) |
| Number of comorbidities, median [range] | 1 [0–8] | 2 [0–7] | 1 [0–8] |
| Determinants | |||
| Mean ICU occupancy rate in %, median (IQR) [range] | 18.7 (10.8–18.7) [0–75] | 18.7 (10.9–18.7) [0–69.2] | 18.8 (10.7–18.8) [0–75] |
| Length of stay in days, median (IQR) [range] | 7 (4–7) [1–193] | 8 (5–8) [1–147] | 7 (4–7) [1–193] |
| ICU admission | 487 (19.5) | 189 (15.2) | 298 (23.9) |
| ARDS | 277 (11.1) | 108 (8.7) | 169 (13.5) |
| In-hospital death | 385 (15.4) | 222 (17.8) | 163 (13.1) |
| Severe COVID-19 | 736 (29.5) | 350 (28.1) | 386 (30.9) |
| Characteristics | mRNA n (%) 833 (67) | AZ n (%) 321 (25.8) | J&J n (%) 90 (7.2) |
|---|---|---|---|
| Baseline characteristics | |||
| Age in years, median (IQR) [range] | 77 (69–77) [18–98] | 73 (63–73) [22–100] | 70.5 (54–70.5) [29–99] |
| Sex | |||
| Women | 327 (39.2) | 127 (39.1) | 32 (35.6) |
| Men | 506 (60.7) | 194 (60.4) | 58 (64.4) |
| Nursing home residency | |||
| Nursing home resident | 97 (11.6) | 9 (2.8) | 3 (3.3) |
| Living with a level of independence | 736 (88.4) | 312 (97.2) | 87 (96.7) |
| Presence of comorbidities | |||
| No comorbidities | 83 (10) | 40 (12.5) | 24 (26.7) |
| Comorbidities | 750 (90) | 281 (87.5) | 66 (73.3) |
| Cardiovascular disease | 343 (41.2) | 134 (41.7) | 31 (34.4) |
| Arterial hypertension | 381 (45.7) | 134 (41.7) | 28 (31.1) |
| Diabetes | 216 (25.9) | 91 (28.3) | 20 (22.2) |
| Chronic renal disease | 135 (16.2) | 50 (15.6) | 9 (10) |
| Chronic liver disease | 19 (2.3) | 8 (2.5) | 3 (3.3) |
| Chronic neurologic or neuromuscular disease | 96 (11.5) | 32 (10) | 6 (6.7) |
| Cognitive impairment | 82 (9.8) | 25 (7.8) | 9 (10) |
| Immunocompromised disease | 40 (4.8) | 18 (5.6) | 1 (1.1) |
| Chronic lung disease | 213 (25.6) | 78 (24.3) | 22 (24.4) |
| Solid cancer | 94 (11.3) | 41 (12.8) | 9 (10) |
| Hematological cancer | 32 (3.8) | 6 (1.9) | 0 |
| Solid organ transplantation | 10 (1.2) | 12 (3.7) | 1 (1.1) |
| Obesity | 114 (13.7) | 41 (12.8) | 11 (12.2) |
| Number of comorbidities, median [range] | 2 [0–7] | 2 [0–7] | 1 [0–6] |
| Time since vaccination in days, median (IQR) [range] | 168 (144–168) [14–286] | 116 (95–116) [24–171] | 115 (84–115) [14–182] |
| Determinants | |||
| Mean ICU occupancy rate in %, median (IQR) [range] | 18.6 (11.3–18.6) [0–69.1] | 18.3 (10.5–18.3) [0–69.2] | 19.2 (10–19.2) [0–63] |
| Length of stay in days, median (IQR) [range] | 8 (5–8) [1–141] | 7 (4–7) [1–147] | 8 (4–8) [1–95] |
| ICU admission | 134 (16.1) | 45 (14) | 10 (11.1) |
| ARDS | 76 (9.1) | 26 (8.1) | 6 (6.7) |
| Death | 155 (18.6) | 44 (13.7) | 23 (25.6) |
| Severe COVID-19 | 244 (29.3) | 76 (23.7) | 30 (33.3) |
| Odds Ratios and 95% Confidence Intervals for Severe COVID-19 and Death | ||||
|---|---|---|---|---|
| Model | Severe COVID-19 | Death | ||
| OR | 95% CI | OR | 95% CI | |
| Only age-adjusted mixed effects logistic regression | 0.5973 A | 0.4842; 0.7368 | 0.6678 B | 0.5082; 0.8776 |
| Full mixed effects logistic regression | 0.4793 C | 0.3817; 0.6018 | 0.4876 D | 0.3646; 0.6520 |
| Odds Ratios and 95% Confidence Intervals for Severe COVID-19 | |||
|---|---|---|---|
| Age ≤ 75 y Old F | |||
| Ref category → | J&J | AZ | mRNA |
| J&J | 1.59 (0.72; 3.50) | 1.05 (0.48; 2.28) | |
| AZ | 0.63 (0.29; 1.39) | 0.66 (0.39; 1.11) | |
| mRNA | 0.95 (0.44; 2.07) | 1.51 (0.90; 2.53) | |
| Age > 75 y old G | |||
| J&J | 2.61 (1.17; 5.78) | 2.08 (0.93; 4.68) | |
| AZ | 0.38 (0.17; 0.85) | 0.80 (0.45; 1.4) | |
| mRNA | 0.44 (0.19; 1.04) | 1.25 (0.70; 2.23) | |
| Odds Ratios and 95% Confidence Intervals for In-hospital Death | |||
|---|---|---|---|
| Age ≤ 75 y Old H | |||
| Ref category → | J&J | AZ | mRNA |
| J&J | 2.37 (0.78; 7.20) | 1.37 (0.46; 4.13) | |
| AZ | 0.42 (0.14; 1.28) | 0.58 (0.27; 1.24) | |
| mRNA | 0.73 (0.24; 2.19) | 1.73 (0.81; 3.70) | |
| Age > 75 y old I | |||
| J&J | 2.82 (1.24; 6.42) | 2.28 (1.03; 5.50) | |
| AZ | 0.35 (0.16; 0.81) | 0.84 (0.45; 1.58) | |
| mRNA | 0.42 (0.18; 0.97) | 1.19 (0.63; 2.21) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robalo, Q.; De Mot, L.; Vandromme, M.; Van Goethem, N.; Gabrio, A.; Chung, P.Y.J.; Meurisse, M.; Belgian Collaborative Group on COVID-19 Hospital Surveillance; Catteau, L.; Thijs, C.; et al. Association between COVID-19 Primary Vaccination and Severe Disease Caused by SARS-CoV-2 Delta Variant among Hospitalized Patients: A Belgian Retrospective Cohort Study. Vaccines 2023, 11, 14. https://doi.org/10.3390/vaccines11010014
Robalo Q, De Mot L, Vandromme M, Van Goethem N, Gabrio A, Chung PYJ, Meurisse M, Belgian Collaborative Group on COVID-19 Hospital Surveillance, Catteau L, Thijs C, et al. Association between COVID-19 Primary Vaccination and Severe Disease Caused by SARS-CoV-2 Delta Variant among Hospitalized Patients: A Belgian Retrospective Cohort Study. Vaccines. 2023; 11(1):14. https://doi.org/10.3390/vaccines11010014
Chicago/Turabian StyleRobalo, Queeny, Laurane De Mot, Mathil Vandromme, Nina Van Goethem, Andrea Gabrio, Pui Yan Jenny Chung, Marjan Meurisse, Belgian Collaborative Group on COVID-19 Hospital Surveillance, Lucy Catteau, Carel Thijs, and et al. 2023. "Association between COVID-19 Primary Vaccination and Severe Disease Caused by SARS-CoV-2 Delta Variant among Hospitalized Patients: A Belgian Retrospective Cohort Study" Vaccines 11, no. 1: 14. https://doi.org/10.3390/vaccines11010014
APA StyleRobalo, Q., De Mot, L., Vandromme, M., Van Goethem, N., Gabrio, A., Chung, P. Y. J., Meurisse, M., Belgian Collaborative Group on COVID-19 Hospital Surveillance, Catteau, L., Thijs, C., & Blot, K. (2023). Association between COVID-19 Primary Vaccination and Severe Disease Caused by SARS-CoV-2 Delta Variant among Hospitalized Patients: A Belgian Retrospective Cohort Study. Vaccines, 11(1), 14. https://doi.org/10.3390/vaccines11010014