
Are Fear of COVID-19 and Vaccine Hesitancy Associated with COVID-19 Vaccine Uptake? A Population-Based Online Survey in Nigeria

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Instruments
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Considerations and Participant Recruitment
3. Results
3.1. Participant Sociodemographic Characteristics and COVID-19 Vaccination Status
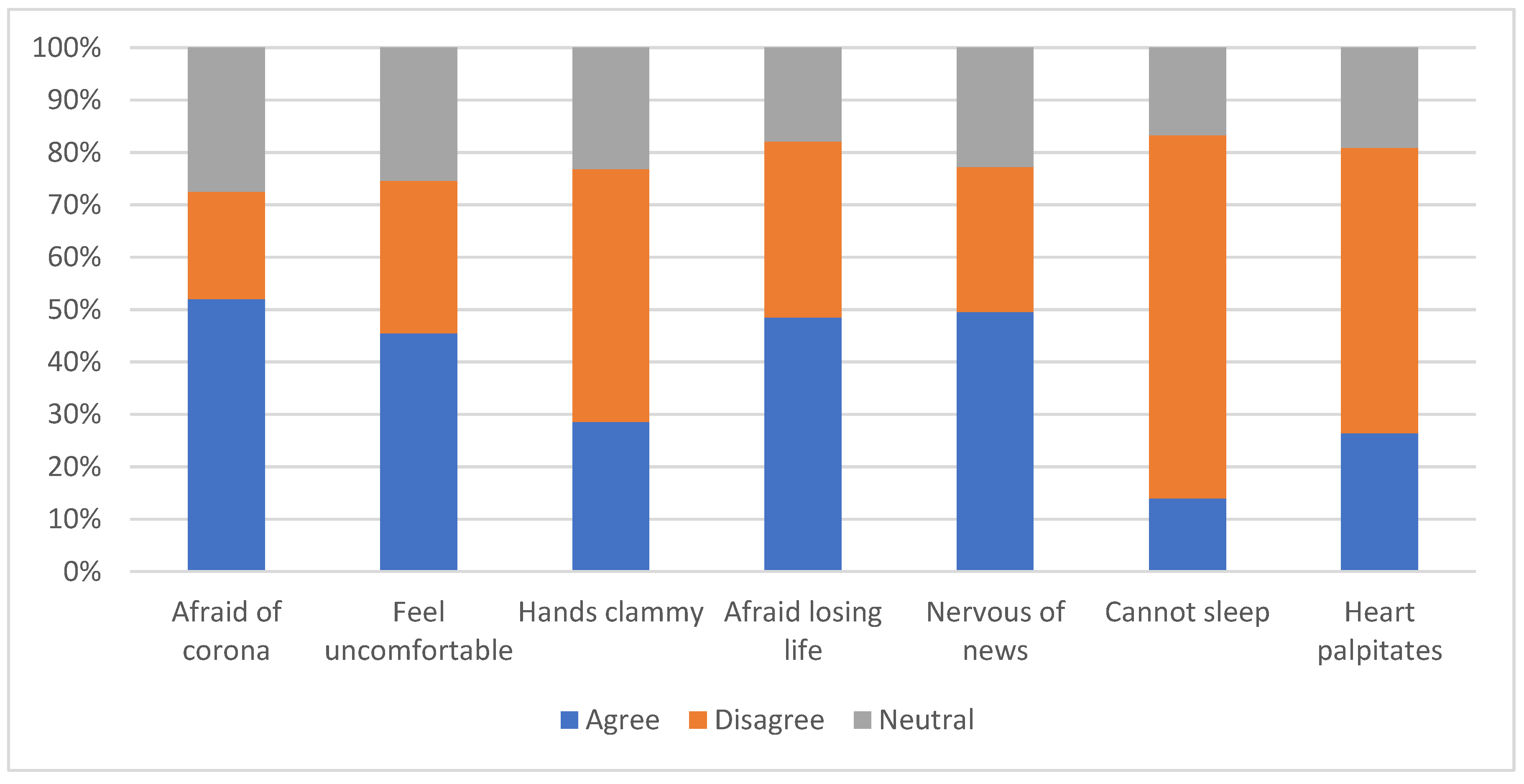
3.2. Fear of Coronavirus Disease and Vaccine Hesitancy among Participants
3.3. Fear of Coronavirus Disease and COVID-19 Vaccine Uptake
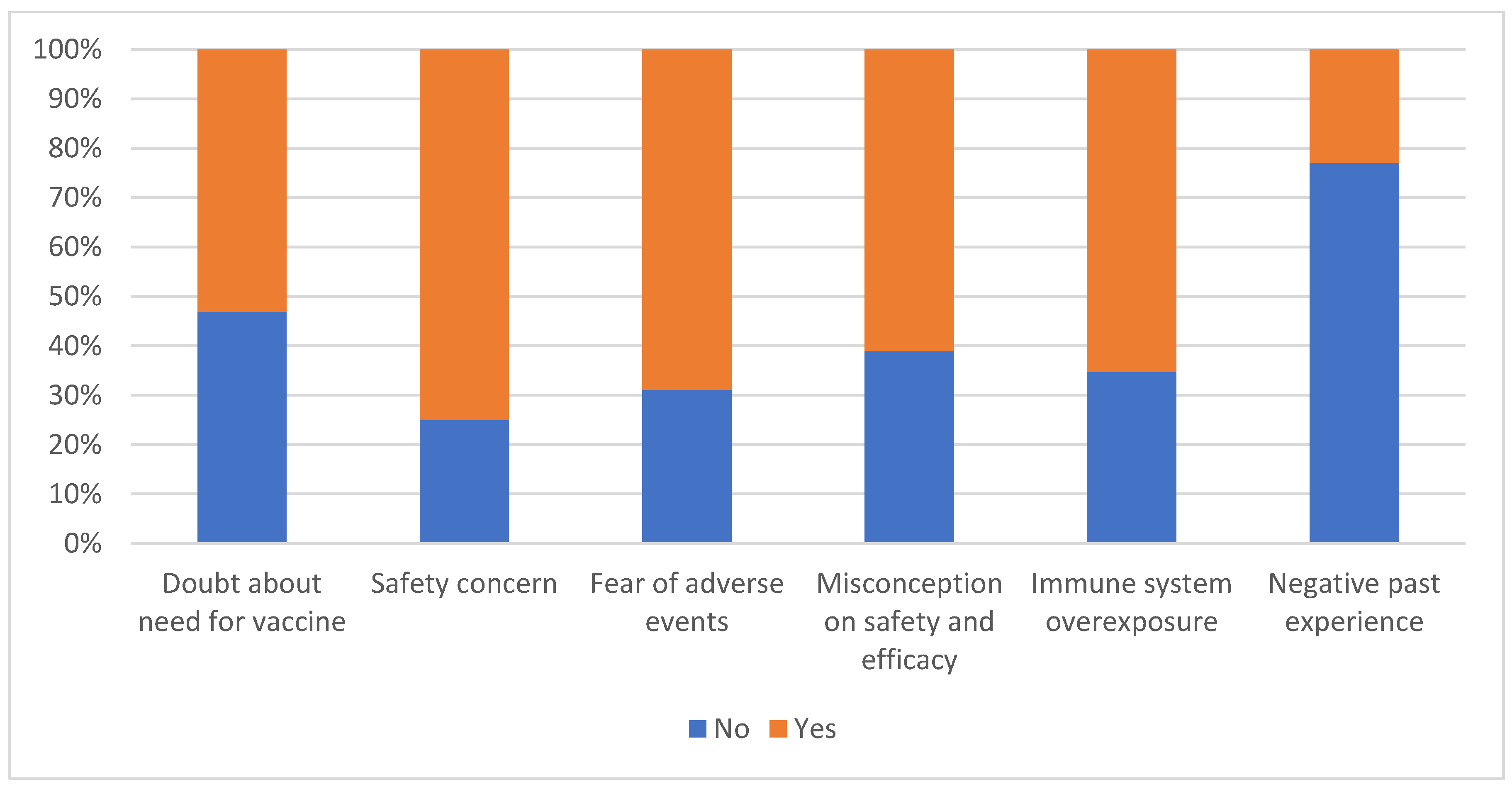
3.4. Reasons for Vaccine Refusal and COVID-19 Vaccine Uptake
4. Discussion
4.1. Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Health Organization. Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 20 May 2022).
- Koffman, J.; Gross, J.; Etkind, S.N.; Selman, L. Uncertainty and COVID-19: How are we to respond? J. R. Soc. Med. 2020, 113, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Centre for Disease Control (CDC). SARS-CoV-2 Variant Classifications and Definition. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html (accessed on 15 May 2022).
- Robinson, J.; Banerjee, I.; Leclézio, A.; Sathian, B. COVID-19 and mutations a threat level assessment. Nepal J. Epidemiol. 2021, 11, 983–987. [Google Scholar] [CrossRef] [PubMed]
- Arora, M.; Lakshmi, R. Vaccines-safety in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 76, 23–40. [Google Scholar] [CrossRef]
- Belongia, E.A.; Naleway, A.L. Smallpox vaccine: The good, the bad, and the ugly. Clin. Med. Res. 2003, 1, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Centre for Disease Control (CDC). Disease You Almost Forgot about (Thanks to Vaccines). 2020. Available online: https://blog.byjus.com/knowledge-vine/diseases-you-almost-forgot-about-thanks-to-vaccines/ (accessed on 25 December 2021).
- Edwards, K.M.; Orenstein., W.A. COVID-19: Vaccines. Up to Date. 2022. Available online: https://www.uptodate.com/contents/covid-19-vaccines (accessed on 3 April 2022).
- World Health Organization. Weekly Epidemiological Update on COVID-19—29 March 2022. 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---29-march-2022 (accessed on 3 April 2022).
- Afolabi, A.A.; Ilesanmi, O.S. Dealing with vaccine hesitancy in Africa: The prospective COVID-19 vaccine context. Pan Afr. Med. J. 2021, 38, 3. [Google Scholar] [CrossRef] [PubMed]
- Michael, C.A.; Waziri, N.; Gunnala, R.; Biya, O.; Kretsinger, K.; Wiesen, E.; Goodson, J.L.; Esapa, L.; Gidado, S.; Uba, B.; et al. Polio Legacy in Action: Using the Polio Eradication Infrastructure for Measles Elimination in Nigeria—The National Stop Transmission of Polio Program. J. Infect. Dis. 2017, 215, S373–S379. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 20, 1537–1545. [Google Scholar] [CrossRef] [Green Version]
- Kayode, O.; Babatunde, O.; Adekunle, O.; Igbalajobi, M.; Abiodun, A. COVID-19 Vac-cine Hesitancy: Maximising the Extending Roles of Community Pharmacists in Nigeria in Driving Be-havioural Changes in Public Health Interventions. J. Infect. Dis. Epidemiol. 2021, 7, 205. [Google Scholar]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Al-Jayyousi, G.F.; Sherbash, M.A.M.; Ali, L.A.M.; El-Heneidy, A.; Alhussaini, N.W.Z.; Elhassan, M.E.A.; Nazzal, M.A. Factors influencing public attitudes towards COVID-19 vaccination: A scoping review informed by the socio-ecological model. Vaccines 2021, 9, 548. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and receptivity for COVID-19 vaccines: A rapid systematic review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- McCaffery, K.J.; Dodd, R.H.; Cvejic, E.; Ayrek, J.; Batcup, C.; Isautier, J.M.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; et al. Health literacy and disparities in COVID-19-related knowledge, attitudes, beliefs and behaviours in Australia. Public Health Res. Pract. 2020, 30, e30342012. [Google Scholar] [CrossRef] [PubMed]
- Popa, G.L.; Muntean, A.-A.; Muntean, M.-M.; Popa, M.I. Knowledge and attitudes on vaccination in southern romanians: A cross-sectional questionnaire. Vaccines 2020, 8, 774. [Google Scholar] [CrossRef]
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Brown Nicholls, L.A.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: Outlining evidence-based and theoretically informed future intervention content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of covid-19 vaccination during the covid-19 pandemic in china. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Predictors of COVID-19 vaccination uptake and reasons for decline of vaccination: A systematic review. medRxiv 2021. [Google Scholar] [CrossRef]
- Al Janabi, T.; Pino, M. Predictors for Actual COVID-19 Vaccine Uptake and Intended Booster Dosage among Medical Students of an Osteopathic Medical School in New York. Epidemiologia 2021, 2, 553–563. [Google Scholar] [CrossRef]
- Dubé, E.; MacDonald, N.E. How can a global pandemic affect vaccine hesitancy? Expert Rev. Vaccines 2020, 19, 899–901. [Google Scholar] [CrossRef]
- Pertwee, E.; Simas, C.; Larson, H.J. An epidemic of uncertainty: Rumors, conspiracy theories and vaccine hesitancy. Nat. Med. 2022, 28, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Paul, K.; Zimmerman, B.; Corsico, P.; Fiske, A.; Geiger, S.; Johnson, S.; Kuiper, J.; Lievevrouw, E.; Marelli, L.; Prainsack, B.; et al. Anticipating hopes, fears and expectations towards COVID-19 vaccines: A qualitative interview study in seven European countries. SSM-Qual. Res. Health 2022, 2, 100035. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Personal. Individ. Differ. 2021, 172, 110590. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of U.S. adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.-H.M.; Sarkar, T.; Khan, M.M.; Roy, S.K.; Khan, S.H.; Hasan, S.M.M.; Hossain, M.S.; Dell, C.A.; Seale, H.; Islam, M.S. Factors Affecting Willingness to Receive COVID-19 Vaccine Among Adults: A Cross-sectional Study in Bangladesh. J. Health Manag. 2021, 97359842110506. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations: Modifications of a model for telecommunications. In Die Diffusion von Innovationen in der Telekommunikation; Springer: Cham, Switzerland, 1995; pp. 25–38. [Google Scholar]
- Snell Jr, W.E.; Wooldridge, D.G. Sexual awareness: Contraception, sexual behaviors and sexual attitudes. Sex. Marital Ther. 1998, 13, 191–199. [Google Scholar] [CrossRef]
- Danchin, M.; Biezen, R.; Manski-Nankervis, J.-A.; Kaufman, J.; Leask, J. Preparing the public for COVID-19 vaccines: How can general practitioners build vaccine confidence and optimise uptake for themselves and their patients? Aust. J. Gen. Pract. 2020, 49, 625–629. [Google Scholar] [CrossRef]
- Coustasse, A.; Kimble, C.; Maxik, K. COVID-19 and Vaccine Hesitancy: A Challenge the United States Must Overcome. J Ambul Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef]
- Prasad, M.; Lin, J.L.; Gu, Y.; Gupta, R.; Macary, P.; Schwarz, H. No crossreactivity of anti-SARS-CoV-2 spike protein antibodies with Syncytin-1. Cell. Mol. Immunol. 2021, 18, 2566–2568. [Google Scholar] [CrossRef]
- Singh, K.; Lima, G.; Cha, M.; Cha, C.; Kulshrestha, J.; Ahn, Y.-Y.; Varol, O. Misinformation, believability, and vaccine acceptance over 40 countries: Takeaways from the initial phase of the COVID-19 infodemic. PLoS ONE 2022, 17, e0263381. [Google Scholar] [CrossRef] [PubMed]
- Carrieri, V.; Madio, L.; Principe, F. Vaccine hesitancy and (fake) news: Quasi?experimental evidence from Italy. Health Econ. 2019, 28, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Bono, S.A.; Villela, E.F.d.M.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors affecting COVID-19 vaccine acceptance: An international survey among low-and middle-income countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef] [PubMed]
- Draulans, D. ‘Finally, a virus got me.’ Scientist who fought Ebola and HIV reflects on facing death from COVID-19. Science 2020. [Google Scholar] [CrossRef]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 19, 1875–1888. [Google Scholar] [CrossRef]
- Adams, J.; MacKenzie, M.J.; Amegah, A.K.; Ezeh, A.; Gadanya, M.A.; Omigbodun, A.; Sarki, A.M.; Thistle, P.; Ziraba, A.K.; Stranges, S.; et al. The conundrum of low covid-19 mortality burden in sub-saharan africa: Myth or reality? Glob. Health Sci. Pract. 2021, 9, 433–443. [Google Scholar] [CrossRef]
- Schmidt, T.; Cloete, A.; Davids, A.; Makola, L.; Zondi, N.; Jantjies, M. Myths, misconceptions, othering and stigmatizing responses to Covid-19 in South Africa: A rapid qualitative assessment. PLoS ONE 2020, 15, e0244420. [Google Scholar] [CrossRef]
- Osei, S.A.; Biney, R.P.; Anning, A.S.; Nortey, L.N.; Ghartey-Kwansah, G. Low incidence of COVID-19 case severity and mortality in Africa; Could malaria co-infection provide the missing link? BMC Infect. Dis. 2022, 22, 78. [Google Scholar] [CrossRef]
- Mertens, G.; Lodder, P.; Smeets, T.; Duijndam, S. Fear of COVID-19 predicts vaccination willingness 14 months later. J. Anxiety Disord. 2022, 102574. [Google Scholar] [CrossRef]
- Akarsu, B.; Canbay Özdemir, D.; Ayhan Baser, D.; Aksoy, H.; Fidancı, İ.; Cankurtaran, M. While studies on COVID-19 vaccine is ongoing, the public’s thoughts and attitudes to the future COVID-19 vaccine. Int. J. Clin. Pract. 2021, 75, e13891. [Google Scholar] [CrossRef]
- Mărcău, F.-C.; Purec, S.; Niculescu, G. Study on the Refusal of Vaccination against COVID-19 in Romania. Vaccines 2022, 10, 261. [Google Scholar] [CrossRef] [PubMed]
- Kourlaba, G.; Kourkouni, E.; Maistreli, S.; Tsopela, C.-G.; Molocha, N.-M.; Triantafyllou, C.; Koniordou, M.; Kopsidas, I.; Chorianopoulou, E.; Maroudi-Manta, S. Willingness of Greek general population to get a COVID-19 vaccine. Glob. Health Res. Policy 2021, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Maglione, M.A.D.; Raaen, L.; Smith, A.; Chari, R.; Newberry, S.; Shanman, R.; Perry, T.; Goetz, M.B.; Gidengil, C. New Vaccines Study Findings Recently Were Reported by Researchers at Children’s Hospital (Safety of Vaccines Used for Routine Immunization of US Children: A Systematic Review). Vaccine Wkly. 2014, 39. Available online: https://go.gale.com/ps/i.do?id=GALE%7CA385153339&sid=sitemap&v=2.1&it=r&p=AONE&sw=w&userGroupName=anon%7Ec5749dfa (accessed on 1 August 2022).
- Betsch, C.; Sachse, K. Debunking Vaccination Myths: Strong Risk Negations Can Increase Perceived Vaccination Risks. Health Psychol. 2013, 32, 146–155. [Google Scholar] [CrossRef]
- Akther, T.; Nur, T. A model of factors influencing COVID-19 vaccine acceptance: A synthesis of the theory of reasoned action, conspiracy theory belief, awareness, perceived usefulness, and perceived ease of use. PLoS ONE 2022, 17, e0261869. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley Pub. Co.: Reading, MA, USA, 1975. [Google Scholar]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Groenewoud, R.; Rachor, G.S.; Asmundson, G.J. A proactive approach for managing COVID-19: The importance of understanding the motivational roots of vaccination hesitancy for SARS-CoV2. Front. Psychol. 2020, 11, 575950. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Categories | Responses | Percentage |
|---|---|---|---|
| Age, y (Mean ± SD) | – | 31.86 ± 9.10 | – |
| Sex | Female | 180 | 31.3 |
| Male | 395 | 68.7 | |
| Geopolitical zone | North-east | 356 | 62.1 |
| North-west | 123 | 21.5 | |
| North-central | 42 | 7.3 | |
| South-east | 11 | 1.9 | |
| South-south | 20 | 3.5 | |
| South-west | 21 | 3.7 | |
| COVID-19 vaccination status | Vaccinated | 158 | 27.7 |
| Unvaccinated | 413 | 72.3 |
| Variables | Categories | Crude OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|---|
| I am most afraid of corona | Agree | 1.70 (1.06–2.63) * | 1.34 (0.72–2.51) |
| Disagree | 1.40 (0.90–2.45) | 1.36 (0.70–2.63) | |
| Neutral | 1 | 1 | |
| It makes me uncomfortable to think about corona | Agree | 1.53 (0.96–2.44) | 1.48 (0.78–2.78) |
| Disagree | 1.03 (0.61–1.73) | 0.84 (0.43–1.63) | |
| Neutral | 1 | 1 | |
| My hands become clammy when I think of corona | Agree | 1.14 (0.68–1.92) | 0.73 (0.38–1.42) |
| Disagree | 1.12 (0.70–1.79) | 1.42 (0.77–2.61) | |
| Neutral | 1 | 1 | |
| I am afraid of losing my life because of corona | Agree | 1.24 (0.75–2.07) | 1.17 (0.59–2.32) |
| Disagree | 0.86 (0.49–1.49) | 0.98 (0.50–1.96) | |
| Neutral | 1 | 1 | |
| When I watch news about corona on social media, I become nervous | Agree | 1.26 (0.78–2.03) | 0.95 (0.52–1.75) |
| Disagree | 1.17 (0.69–1.98) | 1.42 (0.75–2.69) | |
| Neutral | 1 | ||
| I can’t sleep because I am worried about getting corona | Agree | 1.17 (0.62–2.24) | 0.96 (0.42–2.22) |
| Disagree | 0.86 (0.52–1.41) | 0.99 (0.51–1.90) | |
| Neutral | 1 | 1 | |
| My heart palpitates when I think about getting corona | Agree | 0.98 (0.58–1.68) | 0.85 (0.42–1.69) |
| Disagree | 0.63 (0.40–1.04) | 0.47 (0.25–0.90) | |
| Neutral | 1 | 1 | |
| Sex | Male | 0.79 (0.53–1.16) | 0.88 (0.55–1.40) |
| Female | 1 | 1 | |
| Geopolitical zone | North-east | 1.00 (0.38–2.65) | 0.79 (0.27–2.30) |
| North-west | 0.77 (0.27–2.17) | 0.75 (0.24–2.31) | |
| North-central | 0.78 (0.24–2.55) | 0.50 (0.14–1.82) | |
| South-east | 1.43 (0.30–6.74) | 0.82 (0.13–5.12) | |
| South-south | 1.68 (0.45–6.13) | 1.02 (0.99–1.04) | |
| South-west | 1 | 1 | |
| Age | – | 1.02 (1.00–1.04) | 1.02 (0.99–1.04) |
| Variables | Categories | Crude OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|---|
| Doubt about vaccination | No | 2.79 (1.90–4.09) | 2.56 (1.57–4.17) *** |
| Yes | 1 | 1 | |
| Concerns about vaccine safety | No | 1.26 (0.83–1.91) | 0.72 (0.43–1.24) |
| Yes | 1 | 1 | |
| Fear of adverse events | No | 2.14 (1.46–3.15) *** | 0.94 (0.53–1.68) |
| Yes | 1 | 1 | |
| Misconceptions about safety and efficacy | No | 2.92 (2.00–4.26) *** | 2.15 (1.24–3.71) ** |
| Yes | 1 | 1 | |
| Concerns about immune system exposure | No | 2.25 (1.54–3.29) *** | 1.79 (1.06–3.01) * |
| Yes | 1 | 1 | |
| Negative past experience with vaccine | No | 0.62 (0.41–0.95) * | 0.54 (0.33–0.89) * |
| Yes | 1 | 1 | |
| Sex | Male | 0.79 (0.53–1.16) | 0.71 (0.44–1.16) |
| Female | 1 | 1 | |
| Geopolitical zone | North-east | 1.00 (0.38–2.65) | 1.14 (0.38–3.38) |
| North-west | 0.77 (0.27–2.17) | 0.80 (0.26–2.51) | |
| North-central | 0.78 (0.24–2.55) | 0.72 (0.20–2.67) | |
| South-east | 1.43 (0.30–6.74) | 1.14 (0.17–7.72) | |
| South-south | 1.68 (0.45–6.13) | 0.91 (0.19–4.28) | |
| South-west | 1 | 1 | |
| Age | – | 1.02 (1.00–1.04) | 1.03 (1.00–1.05)* |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chutiyami, M.; Salihu, D.; Bello, U.M.; Winser, S.J.; Gambo, A.A.; Sabo, H.; Kolo, A.M.; Jalo, H.A.; Muhammad, A.S.; Mahmud, F.A.; et al. Are Fear of COVID-19 and Vaccine Hesitancy Associated with COVID-19 Vaccine Uptake? A Population-Based Online Survey in Nigeria. Vaccines 2022, 10, 1271. https://doi.org/10.3390/vaccines10081271
Chutiyami M, Salihu D, Bello UM, Winser SJ, Gambo AA, Sabo H, Kolo AM, Jalo HA, Muhammad AS, Mahmud FA, et al. Are Fear of COVID-19 and Vaccine Hesitancy Associated with COVID-19 Vaccine Uptake? A Population-Based Online Survey in Nigeria. Vaccines. 2022; 10(8):1271. https://doi.org/10.3390/vaccines10081271
Chicago/Turabian StyleChutiyami, Muhammad, Dauda Salihu, Umar Muhammad Bello, Stanley John Winser, Amina Abdullahi Gambo, Hadiza Sabo, Adam Mustapha Kolo, Hussaina Abubakar Jalo, Abdullahi Salisu Muhammad, Fatima Ado Mahmud, and et al. 2022. "Are Fear of COVID-19 and Vaccine Hesitancy Associated with COVID-19 Vaccine Uptake? A Population-Based Online Survey in Nigeria" Vaccines 10, no. 8: 1271. https://doi.org/10.3390/vaccines10081271
APA StyleChutiyami, M., Salihu, D., Bello, U. M., Winser, S. J., Gambo, A. A., Sabo, H., Kolo, A. M., Jalo, H. A., Muhammad, A. S., Mahmud, F. A., Adeleye, K. K., Azubuike, O. M., Bukola, I. M., & Kannan, P. (2022). Are Fear of COVID-19 and Vaccine Hesitancy Associated with COVID-19 Vaccine Uptake? A Population-Based Online Survey in Nigeria. Vaccines, 10(8), 1271. https://doi.org/10.3390/vaccines10081271