
Quantitative Analysis of Anti-N and Anti-S Antibody Titers of SARS-CoV-2 Infection after the Third Dose of COVID-19 Vaccination

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sample Collection
2.2. Measurement of Anti-SARS-CoV-2 Spike (Anti-S) and Anti-SARS-CoV-2 Nucleocapsid (Anti-N) Antibodies
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Participants
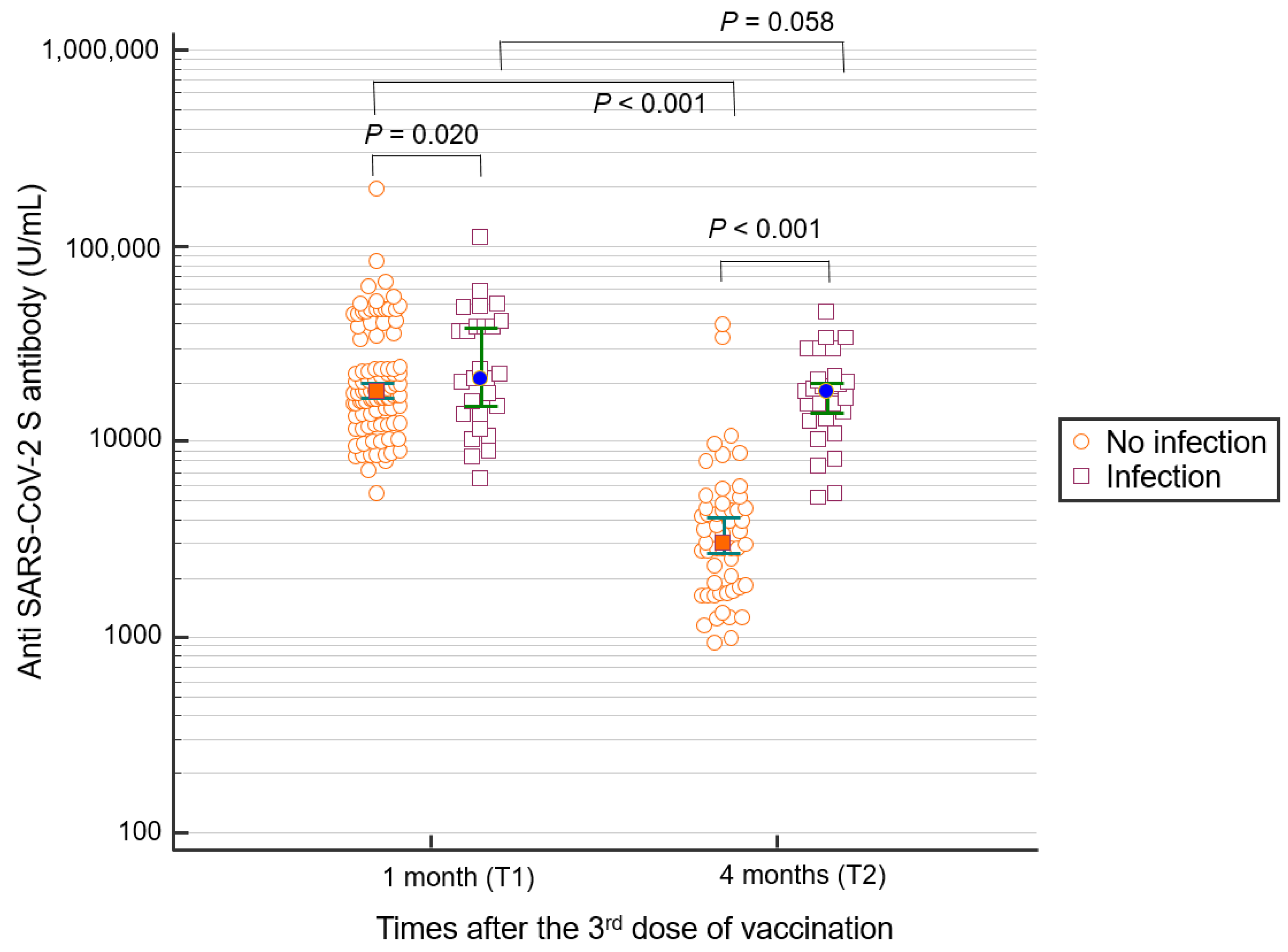
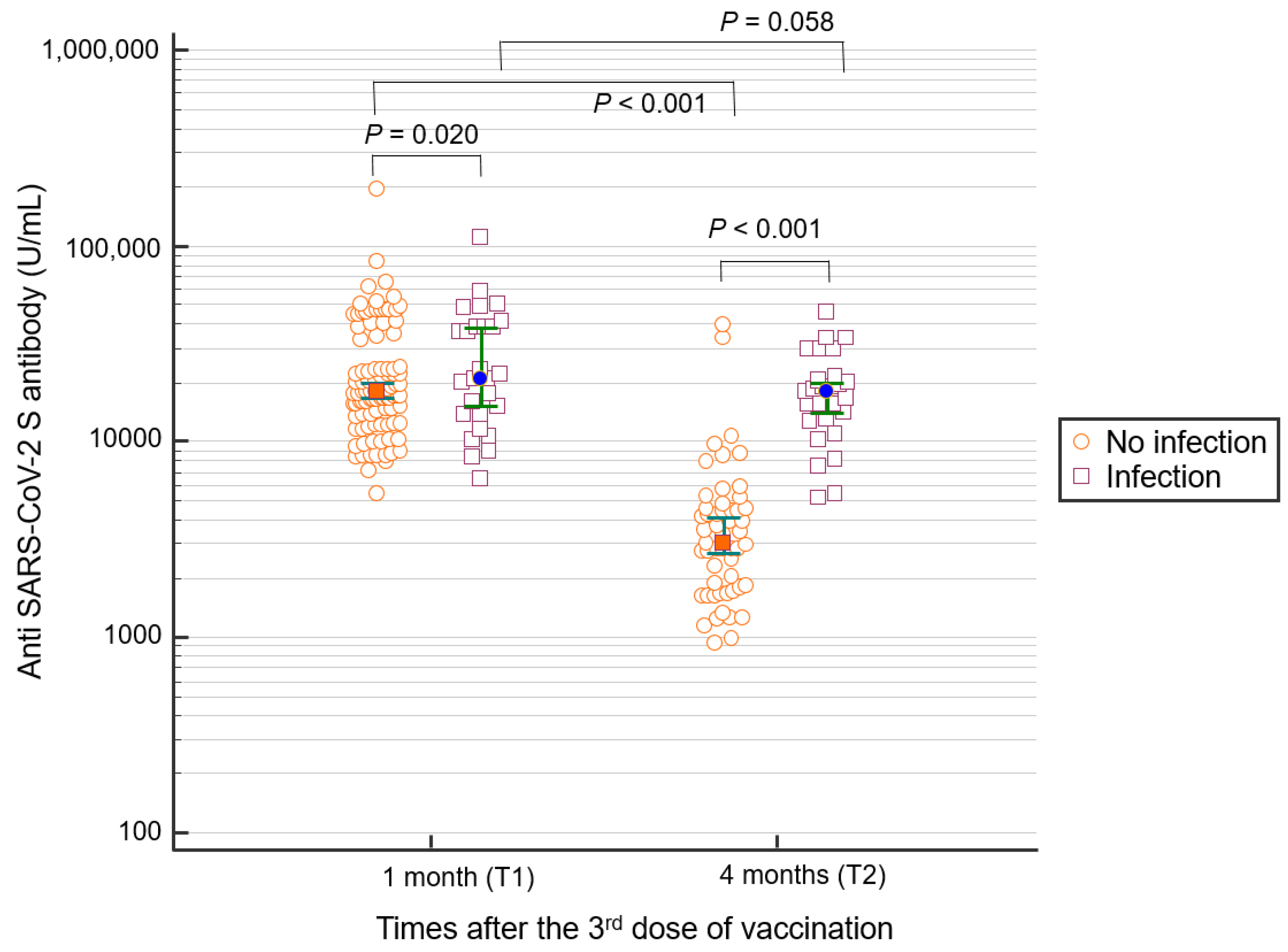
3.2. Qualitative and Quantitative Analyses of Anti-S Antibodies 1 and 4 Months after the Third Dose of COVID-19 Vaccination
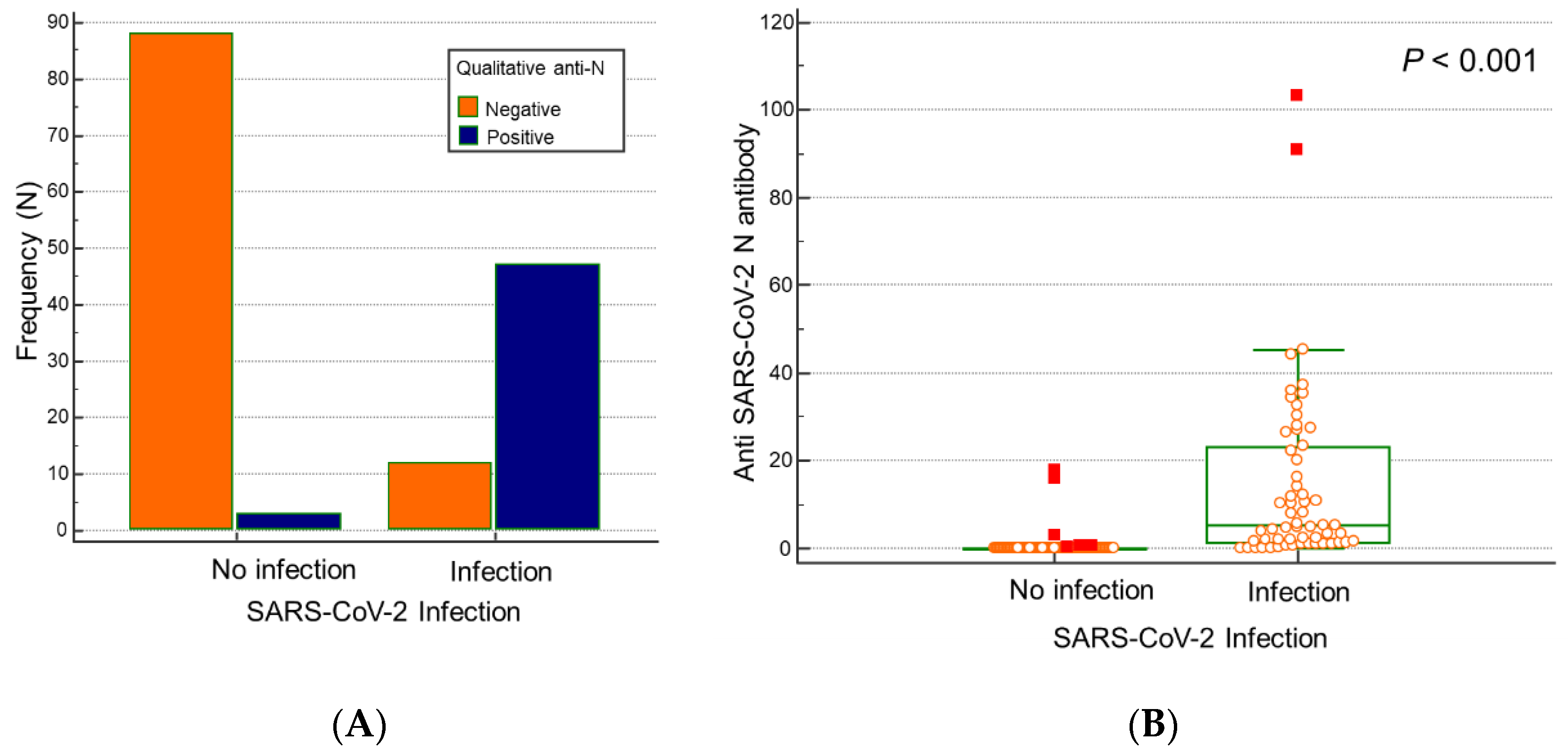
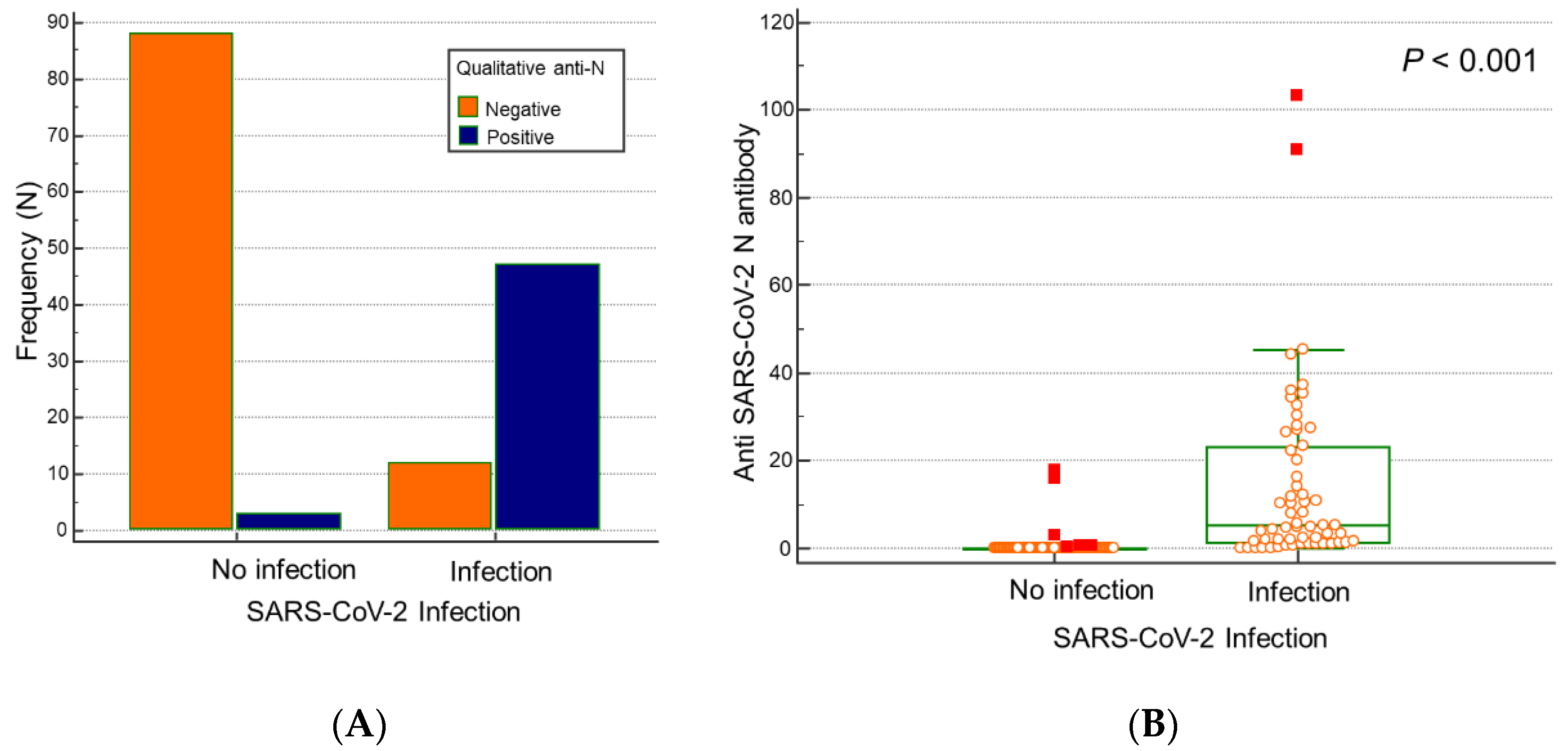
3.3. Qualitative and Quantitative Analyses of Anti-N Antibodies 4 Months after Third Dose of COVID-19 Vaccination
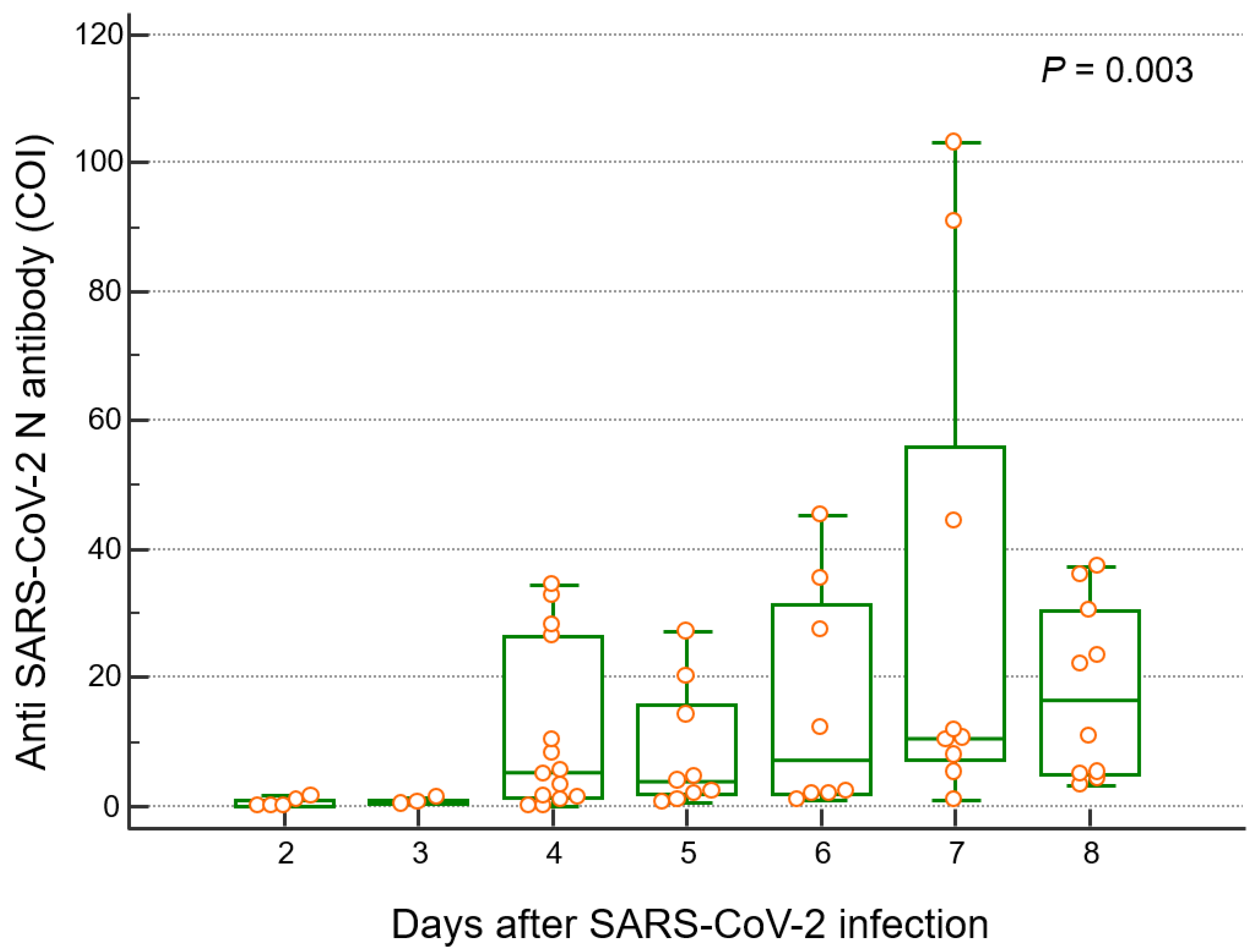
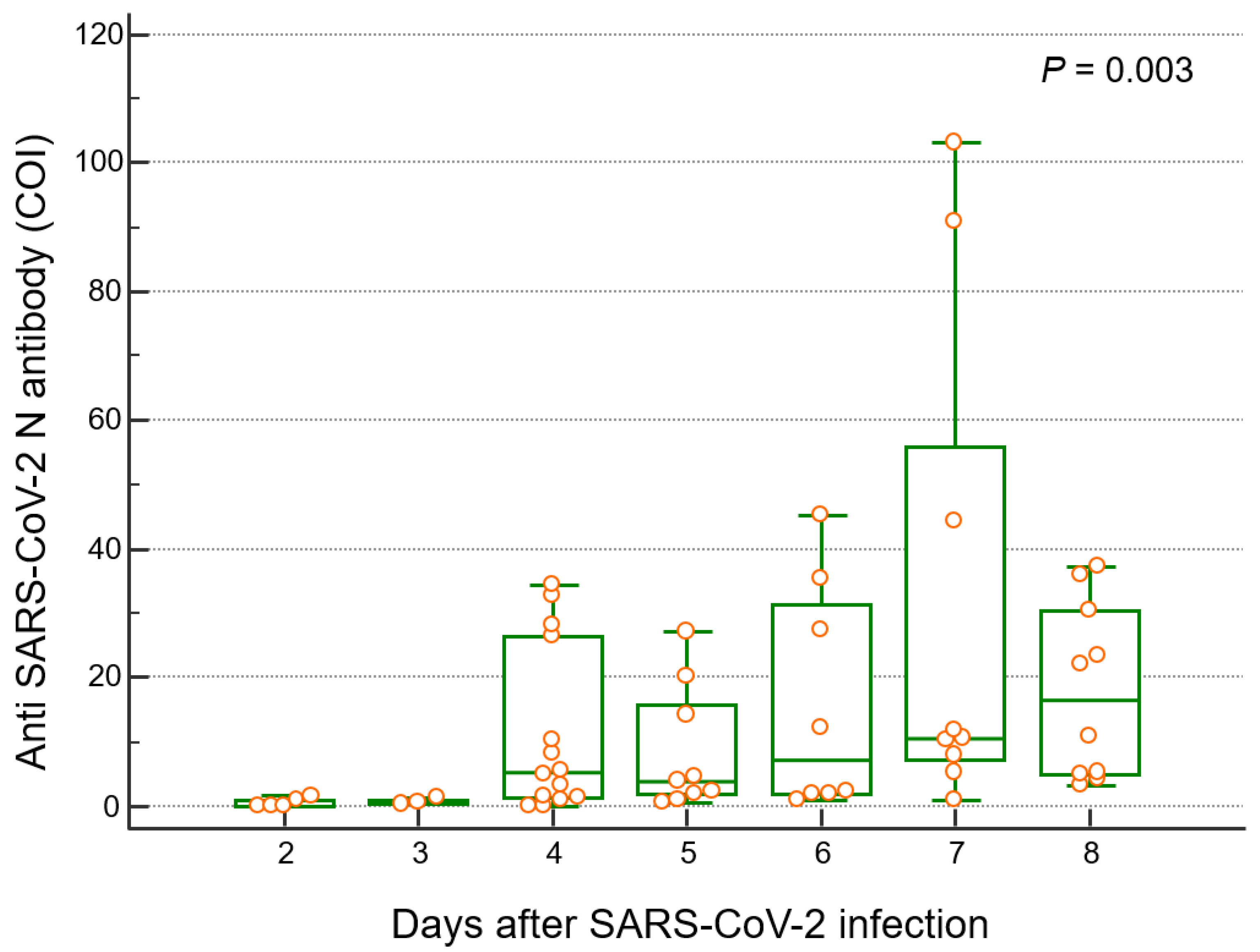
3.4. Quantitative Analysis of Anti-N and Anti-S SARS-CoV-2 Antibodies Based on Duration of SARS-CoV-2 Infection
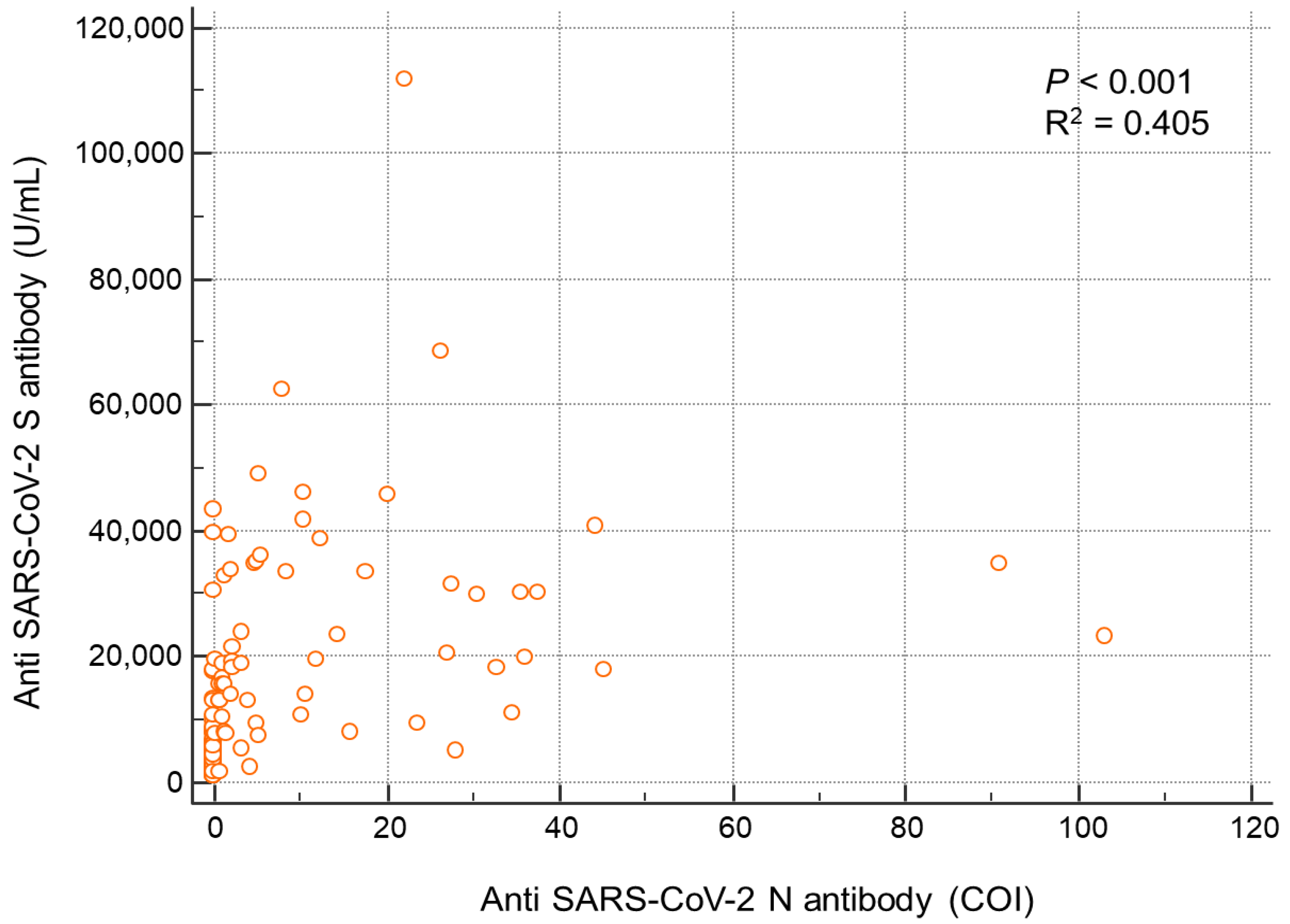
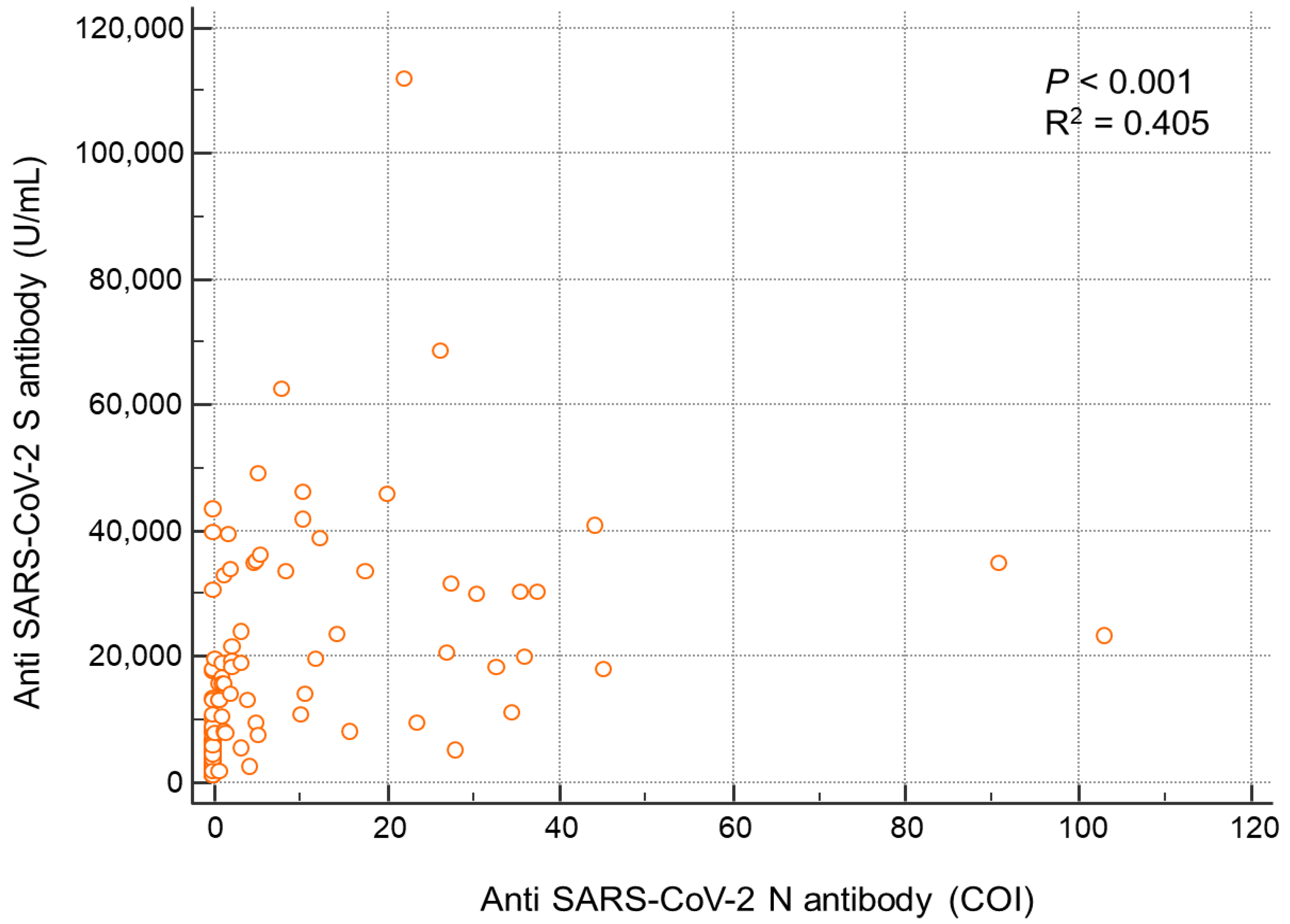
3.5. Correlation between Anti-N and Anti-S Antibody Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Korea Disease Control and Prevention Agency. Coronavirus Disease-19, Republic of Korea. 2022. Available online: http://ncov.mohw.go.kr/ (accessed on 1 June 2022).
- Wise, J. Covid-19: People who have had infection might only need one dose of mRNA vaccine. BMJ 2021, 372, n308. [Google Scholar] [CrossRef]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, Á.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021, 397, 1057–1058. [Google Scholar] [CrossRef]
- Saadat, S.; Rikhtegaran Tehrani, Z.; Logue, J.; Newman, M.; Frieman, M.B.; Harris, A.D.; Sajadi, M.M. Binding and neutralization antibody titers after a single vaccine dose in health care workers previously infected with SARS-CoV-2. JAMA 2021, 325, 1467–1469. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody responses in seropositive persons after a single dose of SARS-CoV-2 mRNA vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Anichini, G.; Terrosi, C.; Gandolfo, C.; Gori Savellini, G.; Fabrizi, S.; Miceli, G.B.; Cusi, M.G. SARS-CoV-2 Antibody Response in Persons with Past Natural Infection. N. Engl. J. Med. 2021, 385, 90–92. [Google Scholar] [CrossRef]
- Rezaei, M.; Sadeghi, M.; Korourian, A.; Tabarsi, P.; Porabdollah, M.; Askari, E.; Mortaz, E.; Mahmoudi, S.; Marjani, M.; Velayati, A.A. Comparative evaluation of SARS-CoV-2 IgG assays against nucleocapsid and spike antigens. Hum. Antibodies 2021, 29, 109–113. [Google Scholar] [CrossRef]
- Azak, E.; Karadenizli, A.; Uzuner, H.; Karakaya, N.; Canturk, N.Z.; Hulagu, S. Comparison of an inactivated Covid19 vaccine-induced antibody response with concurrent natural Covid19 infection. Int. J. Infect. Dis. 2021, 113, 58–64. [Google Scholar] [CrossRef]
- Jeong, S.; Lee, N.; Lee, S.K.; Cho, E.J.; Hyun, J.; Park, M.J.; Song, W.; Jung, E.J.; Woo, H.; Seo, Y.B.; et al. Comparing five SARS-CoV-2 antibody assay results before and after the first and second ChAdOx1 nCoV-19 vaccination among health care workers: A prospective multicenter study. J. Clin. Microbiol. 2021, 59, e0178821. [Google Scholar] [CrossRef]
- Van Elslande, J.; Decru, B.; Jonckheere, S.; Van Wijngaerden, E.; Houben, E.; Vandecandelaere, P.; Indevuyst, C.; Depypere, M.; Desmet, S.; André, E.; et al. Antibody response against SARS-CoV-2 spike protein and nucleoprotein evaluated by four automated immunoassays and three ELISAs. Clin. Microbiol. Infect. 2020, 26, 1557.e1551–1557.e1557. [Google Scholar] [CrossRef]
- McBride, R.; van Zyl, M.; Fielding, B.C. The coronavirus nucleocapsid is a multifunctional protein. Viruses 2014, 6, 2991–3018. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.; Feng, Y.; Mo, X.; Zheng, P.; Wang, Q.; Li, P.; Peng, P.; Liu, X.; Chen, Z.; Huang, H.; et al. Kinetics of SARS-CoV-2 specific IgM and IgG responses in COVID-19 patients. Emerg. Microbes. Infect. 2020, 9, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Jochum, S.; Kirste, I.; Hortsch, S.; Grunert, V.P.; Legault, H.; Eichenlaub, U.; Kashlan, B.; Pajon, R. Clinical utility of Elecsys anti-SARS-CoV-2 S assay in COVID-19 vaccination: An exploratory analysis of the mRNA-1273 phase 1 Trial. Front. Immunol. 2022, 19. Preprint. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M.; Plebani, M. Anti-SARS-CoV-2 antibodies testing in recipients of COVID-19 vaccination: Why, when, and how? Diagnostics 2021, 11, 941. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.I.; Hagan-Burke, S. Useful effect size interpretations for single case research. Behav. Ther. 2007, 38, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; Ferrante di Ruffano, L.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 6, Cd013652. [Google Scholar] [CrossRef]
- Lau, C.S.; Phua, S.K.; Liang, Y.L.; Oh, M.L.H.; Aw, T.C. SARS-CoV-2 spike and neutralizing antibody kinetics 90 days after three doses of BNT162b2 mRNA COVID-19 vaccine in Singapore. Vaccines 2022, 10, 331. [Google Scholar] [CrossRef]
- Romero-Ibarguengoitia, M.E.; Rivera-Salinas, D.; Hernández-Ruíz, Y.G.; Armendariz-Vázquez, A.G.; González-Cantú, A.; Barco-Flores, I.A.; González-Facio, R.; Montelongo-Cruz, L.P.; Del Rio-Parra, G.F.; Garza-Herrera, M.R.; et al. Effect of the third dose of BNT162b2 vaccine on quantitative SARS-CoV-2 spike 1-2 IgG antibody titers in healthcare personnel. PLoS ONE 2022, 17, e0263942. [Google Scholar] [CrossRef]
- Glück, V.; Tydykov, L.; Mader, A.L.; Warda, A.S.; Bertok, M.; Weidlich, T.; Gottwald, C.; Köstler, J.; Salzberger, B.; Wagner, R.; et al. Humoral immunity in dually vaccinated SARS-CoV-2-naïve individuals and in booster-vaccinated COVID-19-convalescent subjects. Infection 2022. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Hoffmann, M.; Krüger, N.; Schulz, S.; Cossmann, A.; Rocha, C.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.S.; Winkler, M.S.; et al. The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Cell 2022, 185, 447–456. [Google Scholar] [CrossRef]
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.-W. Omicron variant (B.1.1.529): Infectivity, vaccine breakthrough, and antibody resistance. J. Chem. Inf. Model. 2022, 62, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Assis, R.; Jain, A.; Nakajima, R.; Jasinskas, A.; Khan, S.; Palma, A.; Parker, D.M.; Chau, A.; Specimen Collection Group; Obiero, J.M.; et al. Distinct SARS-CoV-2 antibody reactivity patterns elicited by natural infection and mRNA vaccination. NPJ Vaccines 2021, 4, 132. [Google Scholar] [CrossRef] [PubMed]
- Maine, G.N.; Krishnan, S.M.; Walewski, K.; Trueman, J.; Sykes, E.; Sun, Q. Clinical and analytical evaluation of the Abbott AdviseDx quantitative SARS-CoV-2 IgG assay and comparison with two other serological tests. J. Immunol. Methods 2022, 503, 113243. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SARS-CoV-2 Infection (−) (n = 91) | SARS-CoV-2 Infection (+) (n = 58) | p-Value | |
|---|---|---|---|
| Age | 32.0 (23.0–59.0) | 39.5 (22.0–60.0) | 0.8658 |
| Sex (male: female) | 85:6 | 51:7 | 0.2498 |
| Sampling days after the third vaccination (T1) * | 25.0 (7–32) | 23.5 (14–32) | 0.8318 |
| Sampling days after the third vaccination (T2) * | 129 (103–134) | 129 (113–151) | 0.8725 |
| Post-infection days after the third vaccination | N/A | 106 (77–136) | N/A |
| T2 sampling days after infection | N/A | 22.5 (7–62) | N/A |
| Groups * (Days after Infection) | n | Minimum (COI) | Maximum (COI) | Median (IQR) (COI) | p < 0.05 from Groups |
|---|---|---|---|---|---|
| 6–10 (D1) | 5 | 0.07 | 1.59 | 0.11 (0.08–1.13) | D3, D4, D5, D6, D7 |
| 11–15 (D2) | 3 | 0.19 | 1.22 | 0.64 (0.30–1.08) | D3, D5, D6, D7 |
| 16–20 (D3) | 14 | 0.06 | 34.5 | 5.27 (1.05–22.4) | D1, D2, D6 |
| 21–25 (D4) | 9 | 0.83 | 27.2 | 3.88 (1.88–15.8) | D1 |
| 26–30 (D5) | 8 | 0.91 | 45.2 | 7.25 (2.03–31.6) | D1, D2 |
| 31–35 (D6) | 9 | 0.94 | 103.0 | 10.5 (7.20–55.9) | D1, D2, D3 |
| 36–62 (D7) | 10 | 3.30. | 37.4 | 16.5 (4.92–30.5) | D1, D2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, N.; Jeong, S.; Lee, S.K.; Cho, E.-J.; Hyun, J.; Park, M.-J.; Song, W.; Kim, H.S. Quantitative Analysis of Anti-N and Anti-S Antibody Titers of SARS-CoV-2 Infection after the Third Dose of COVID-19 Vaccination. Vaccines 2022, 10, 1143. https://doi.org/10.3390/vaccines10071143
Lee N, Jeong S, Lee SK, Cho E-J, Hyun J, Park M-J, Song W, Kim HS. Quantitative Analysis of Anti-N and Anti-S Antibody Titers of SARS-CoV-2 Infection after the Third Dose of COVID-19 Vaccination. Vaccines. 2022; 10(7):1143. https://doi.org/10.3390/vaccines10071143
Chicago/Turabian StyleLee, Nuri, Seri Jeong, Su Kyung Lee, Eun-Jung Cho, Jungwon Hyun, Min-Jeong Park, Wonkeun Song, and Hyun Soo Kim. 2022. "Quantitative Analysis of Anti-N and Anti-S Antibody Titers of SARS-CoV-2 Infection after the Third Dose of COVID-19 Vaccination" Vaccines 10, no. 7: 1143. https://doi.org/10.3390/vaccines10071143
APA StyleLee, N., Jeong, S., Lee, S. K., Cho, E.-J., Hyun, J., Park, M.-J., Song, W., & Kim, H. S. (2022). Quantitative Analysis of Anti-N and Anti-S Antibody Titers of SARS-CoV-2 Infection after the Third Dose of COVID-19 Vaccination. Vaccines, 10(7), 1143. https://doi.org/10.3390/vaccines10071143