
Comparison of Immunogenicity and Safety of Inactivated, Adenovirus-Vectored, and Heterologous Adenovirus-Vectored/mRNA Vaccines in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Prospective Cohort Study

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedure
2.3. Immunogenicity Assessment
2.4. Safety Assessment
2.5. Statistical Analyses
3. Results
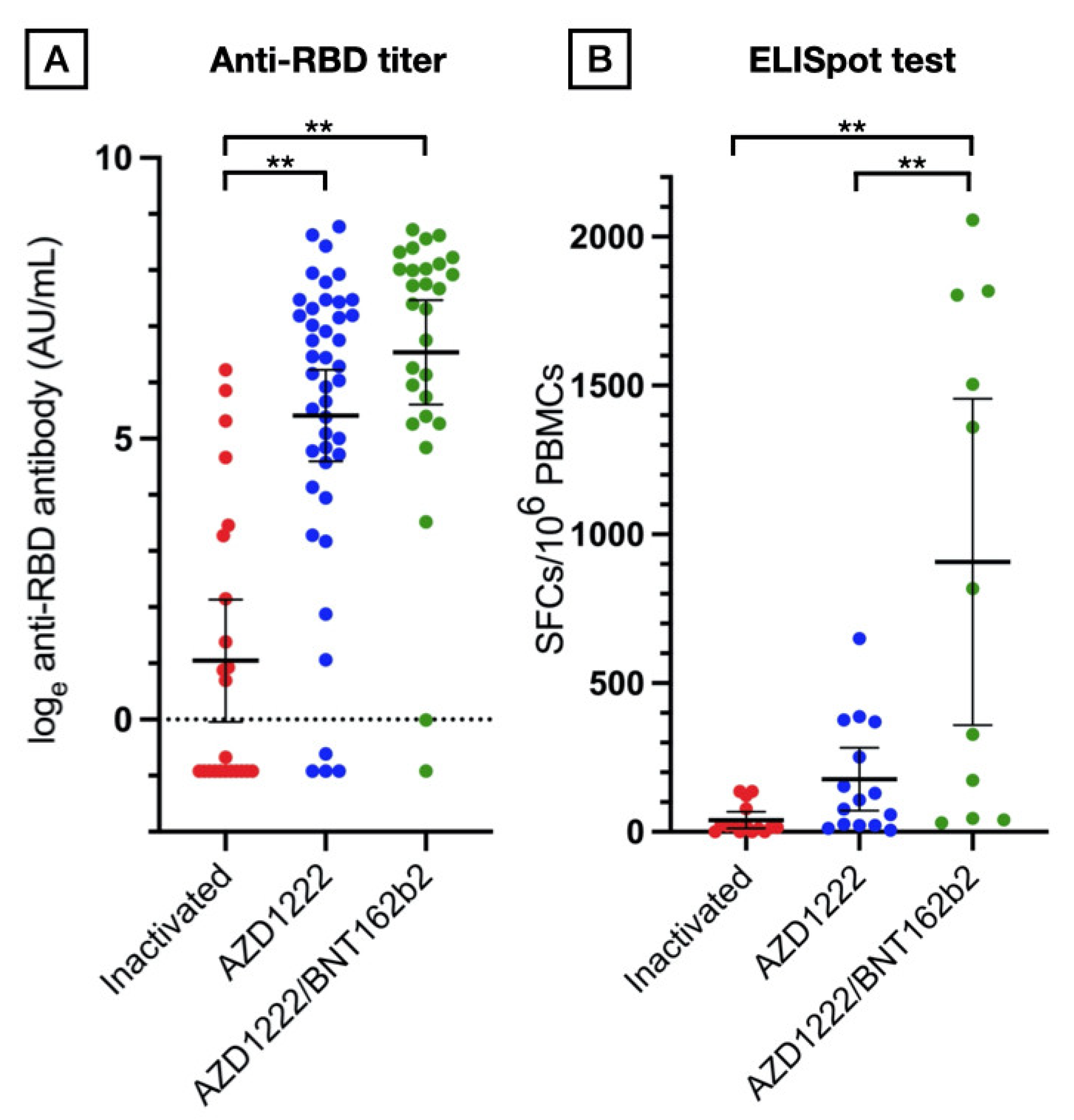
3.1. Humoral Immune Responses
3.2. Cellular Responses
3.3. Safety, Reactogenicity, and Disease Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Worldometer. COVID-19 Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 19 April 2022).
- Kyriakidis, N.C.; López-Cortés, A.; González, E.V.; Grimaldos, A.B.; Prado, E.O. SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. NPJ Vaccines 2021, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Bin Lee, A.R.Y.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of covid-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar]
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the clinical efficacy of COVID-19 vaccines: A systematic review and network meta-analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef] [PubMed]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; Demissie, E.G.; El-Qunniet, A.A.; Haile, A.; Huang, K.; Kinnett, B.; et al. Effect of Immunosuppression on the Immunogenicity of mRNA Vaccines to SARS-CoV-2: A Prospective Cohort Study. Ann. Intern. Med. 2021, 174, 1572–1585. [Google Scholar] [CrossRef]
- Hadjadj, J.; Planas, D.; Ouedrani, A.; Buffier, S.; Delage, L.; Nguyen, Y.; Bruel, T.; Stolzenberg, M.-C.; Staropoli, I.; Ermak, N.; et al. Immunogenicity of BNT162b2 vaccine against the Alpha and Delta variants in immunocompromised patients with systemic inflammatory diseases. Ann. Rheum. Dis. 2022, 81, 720–728. [Google Scholar] [CrossRef]
- Tang, K.-T.; Hsu, B.-C.; Chen, D.-Y. Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 834. [Google Scholar] [CrossRef]
- Yuki, E.F.N.; Borba, E.F.; Pasoto, S.G.; Seguro, L.P.; Lopes, M.; Saad, C.G.S.; Medeiros-Ribeiro, A.C.; Silva, C.A.; de Andrade, D.C.O.; de Vinci, K.; et al. Impact of Distinct Therapies on Antibody Response to SARS-CoV-2 Vaccine in Systemic Lupus Erythematosus. Arthritis Care Res. 2022, 74, 562–571. [Google Scholar] [CrossRef]
- Vasudev, B.; Hariharan, S.; Hussain, S.A.; Zhu, Y.R.; Bresnahan, B.A.; Cohen, E.P. BK virus nephritis: Risk factors, timing, and outcome in renal transplant recipients. Kidney Int. 2005, 68, 1834–1839. [Google Scholar] [CrossRef] [Green Version]
- Mabtech. Human IFN-γ ELISpot PRO kit Datasheet/Protocol [19 April 2022]. Available online: https://www.mabtech.com/sites/default/files/datasheets/3420-2APT-2.pdf (accessed on 19 April 2022).
- Palacios, R.; Patino, E.G.; de Oliveira Piorelli, R.; Conde, M.; Batista, A.P.; Zeng, G.; Xin, Q.; Kallas, E.G.; Flores, J.; Ockenhouse, C.F.; et al. Double-Blind, Randomized, Placebo-Controlled Phase III Clinical Trial to Evaluate the Efficacy and Safety of treating Healthcare Professionals with the Adsorbed COVID-19 (Inactivated) Vaccine Manufactured by Sinovac—PROFISCOV: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 853. [Google Scholar]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillieet, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Hanet, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Papagoras, C.; Fragoulis, G.E.; Zioga, N.; Simopoulou, T.; Deftereou, K.; Kalavri, E.; Zampeli, E.; Gerolymatou, N.; Kataxaki, E.; Melissaropoulos, K.; et al. Better outcomes of COVID-19 in vaccinated compared to unvaccinated patients with systemic rheumatic diseases. Ann. Rheum. Dis. 2021; ahead of print. [Google Scholar]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Sughayer, M.A.; Souan, L.; Abu Alhowr, M.M.; Al Rimawi, D.; Siag, M.; Albadr, S.; Owdeh, M.; Al Atrash, T. Comparison of the effectiveness and duration of anti-RBD SARS-CoV-2 IgG antibody response between different types of vaccines: Implications for vaccine strategies. Vaccine 2022, 40, 2841–2847. [Google Scholar] [CrossRef]
- Wanlapakorn, N.; Suntronwong, N.; Phowatthanasathian, H.; Yorsaeng, R.; Vichaiwattana, P.; Thongmee, T.; Auphimai, C.; Srimuan, D.; Thatsanatorn, T.; Assawakosri, S.; et al. Safety and immunogenicity of heterologous and homologous inactivated and adenoviral-vectored COVID-19 vaccine regimens in healthy adults: A prospective cohort study. Hum. Vaccin Immunother. 2022, 18, 2029111. [Google Scholar] [CrossRef]
- Kang, C.-M.; Lee, N.-Y.; Lin, C.-H.; Hsu, Y.-S.; Chang, Y.-C.; Chung, M.-Y.; Lee, Y.-F.; Tseng, W.-P.; Wu, J.-L.; Chen, S.-Y.; et al. Immunogenicity and safety of homologous and heterologous ChAdOx1-S and mRNA-1273 vaccinations in healthy adults in Taiwan. J. Clin. Virol. 2022, 150–151, 105156. [Google Scholar] [CrossRef]
- Sheng, W.-H.; Chang, S.-Y.; Lin, P.-H.; Hsieh, M.-J.; Chang, H.-H.; Cheng, C.-Y.; Yanget, H.-C.; Pan, C.-F.; Ieong, S.-M.; Chao, T.-L.; et al. Immune response and safety of heterologous ChAdOx1-nCoV-19/mRNA-1273 vaccination compared with homologous ChAdOx1-nCoV-19 or homologous mRNA-1273 vaccination. J. Formos. Med. Assoc. 2022, 121, 766–777. [Google Scholar] [CrossRef]
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef]
- Geers, D.; Shamier, M.C.; Bogers, S.; den Hartog, G.; Gommers, L.; Nieuwkoop, N.N.; Schmitz, K.S.; Rijsbergen, L.C.; Van Osch, J.A.T.; Dijkhuizen, E.; et al. SARS-CoV-2 variants of concern partially escape humoral but not T-cell responses in COVID-19 convalescent donors and vaccinees. Sci. Immunol. 2021, 6, eabj1750. [Google Scholar] [CrossRef]
- Redd, A.D.; Nardin, A.; Kared, H.; Bloch, E.M.; Pekosz, A.; Laeyendecker, O.; Abel, B.; Fehlings, M.; Quinn, T.C.; Tobianet, A.A.R. CD8+ T-Cell Responses in COVID-19 Convalescent Individuals Target Conserved Epitopes from Multiple Prominent SARS-CoV-2 Circulating Variants. Open Forum Infect. Dis. 2021, 8, ofab143. [Google Scholar] [CrossRef]
- Esquivel-Valerio, J.A.; Skinner-Taylor, C.M.; Moreno-Arquieta, I.A.; Cardenas-de la Garza, J.A.; Garcia-Arellano, G.; Gonzalez-Garcia, P.L.; del Rocio Almaraz-Juarez, F.; Galarza-Delgado, D.A. Adverse events of six COVID-19 vaccines in patients with autoimmune rheumatic diseases: A cross-sectional study. Rheumatol. Int. 2021, 41, 2105–2108. [Google Scholar] [CrossRef] [PubMed]
- Cherian, S.; Paul, A.; Ahmed, S.; Alias, B.; Manoj, M.; Santhosh, A.K.; Varghese, D.R.; Krishnan, N.; Shenoy, P. Safety of the ChAdOx1 nCoV-19 and the BBV152 vaccines in 724 patients with rheumatic diseases: A post-vaccination cross-sectional survey. Rheumatol. Int. 2021, 41, 1441–1445. [Google Scholar] [CrossRef] [PubMed]
- Connolly, C.M.; Ruddy, J.A.; Boyarsky, B.J.; Barbur, I.; Werbel, W.A.; Geetha, D.; Garonzik-Wang, J.M.; Segev, D.L.; Christopher-Stine, L.; Paik, J.J. Disease Flare and Reactogenicity in Patients with Rheumatic and Musculoskeletal Diseases Following Two-Dose SARS-CoV-2 Messenger RNA Vaccination. Arthritis Rheumatol. 2022, 74, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccaset, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Immunosuppression Units | Agents | Unit Dose |
|---|---|---|
| 1 | Prednisone | 5 mg/day |
| 1 | Azathioprine | 100 mg/day |
| 1 | Cyclosporine | 100 mg/day |
| 1 | Tacrolimus | 2 mg/day |
| 1 | Mycophenolate mofetil | 500 mg/day |
| 1 | Methotrexate | 15 mg/week |
| 1 | Leflunomide | 10 mg/day |
| Characteristic | AZD1222 (n = 43) | AZD1222/BNT162b2 (n = 28) | Inactivated (n = 23) | p-Value |
|---|---|---|---|---|
| Age (year) | 49.5 (12.5) | 44.8 (10.1) | 38.9 (13.2) | 0.004 |
| Female gender (%) | 40 (93%) | 26 (93%) | 21 (91%) | 1 |
| Duration of disease (year) | 10.2 (9.7) | 11.9 (7.8) | 8.3 (8.8) | 0.4 |
| Underlying autoimmune disease (%) | ||||
| - RA | 15 (35%) | 9 (32%) | 6 (26%) | |
| - SLE | 28 (65%) | 17 (68%) | 17 (74%) | 0.8 |
| Disease activity | ||||
| - SLEDAI | 3.14 (2.95) | 2.11 (2.35) | 3.12 (2.74) | 0.4 |
| - DAS28 | 3.59 (1.68) | 3.84 (1.52) | 2.47 (0.72) | 0.2 |
| - CDAI | 12.1 (13.6) | 17.2 (13.1) | 3.3 (5.4) | 0.1 |
| Immunosuppressant load (unit) | 2.42 (1.61) | 2.66 (1.68) | 3.62 (2.33) | 0.04 |
| Immunosuppressive therapy (%) | ||||
| Mycophenolate mofetil | 21 (45.7%) | 14 (48.3%) | 16 (43.2%) | |
| Azathioprine | 4 (8.7%) | 3 (10.3%) | 4 (10.8%) | |
| Tacrolimus | 0 (0%) | 0 (0%) | 3 (8.1%) | |
| Cyclosporine | 4 (8.7%) | 1 (3.4%) | 2 (5.4%) | |
| Methotrexate | 14 (30.4%) | 8 (27.6%) | 12 (32.4%) | |
| Leflunomide | 3 (6.5%) | 3 (10.3%) | 4 (10.8%) | |
| Prednisolone | 36 (78.3%) | 23 (79.3%) | 32 (86.5%) | |
| Antimalarial | 30 (65.2%) | 19 (65.5%) | 25 (67.6%) | |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Variable | Regression Coefficient | 95% CI | p-Value | Regression Coefficient | 95% CI | p-Value |
| Age | 0.02 | 0.04 to 0.14 | 0.0006 | 0.02 | −0.03 to 0.07 | 0.4 |
| Female | 0.33 | −0.96 to 1.62 | 0.6 | 0.38 | −0.56 to 1.32 | 0.4 |
| Diagnosis | ||||||
| RA | Ref | Ref | Ref | Ref | ||
| SLE | −0.82 | −1.53 to −0.11 | 0.02 | −0.59 | −1.22 to 0.03 | 0.06 |
| Vaccine group | ||||||
| AZD1222 | Ref | Ref | Ref | Ref | ||
| Inactivated | −3.28 | −4.10 to −2.47 | <0.0001 | −2.82 | −3.63 to −2.01 | <0.0001 |
| AZD1222/BNT162b2 | 2.2 | 1.43 to 2.98 | <0.0001 | 2.09 | 1.36 to 2.81 | <0.0001 |
| Immunosuppressant load | −0.64 | −0.98 to −0.30 | 0.0003 | −0.38 | −0.66 to −1.0 | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assawasaksakul, T.; Lertussavavivat, T.; Sathitratanacheewin, S.; Oudomying, N.; Vichaiwattana, P.; Wanlapakorn, N.; Poovorawan, Y.; Avihingsanon, Y.; Assawasaksakul, N.; Buranapraditkun, S.; et al. Comparison of Immunogenicity and Safety of Inactivated, Adenovirus-Vectored, and Heterologous Adenovirus-Vectored/mRNA Vaccines in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Prospective Cohort Study. Vaccines 2022, 10, 853. https://doi.org/10.3390/vaccines10060853
Assawasaksakul T, Lertussavavivat T, Sathitratanacheewin S, Oudomying N, Vichaiwattana P, Wanlapakorn N, Poovorawan Y, Avihingsanon Y, Assawasaksakul N, Buranapraditkun S, et al. Comparison of Immunogenicity and Safety of Inactivated, Adenovirus-Vectored, and Heterologous Adenovirus-Vectored/mRNA Vaccines in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Prospective Cohort Study. Vaccines. 2022; 10(6):853. https://doi.org/10.3390/vaccines10060853
Chicago/Turabian StyleAssawasaksakul, Theerada, Tanat Lertussavavivat, Seelwan Sathitratanacheewin, Nont Oudomying, Preeyaporn Vichaiwattana, Nasamon Wanlapakorn, Yong Poovorawan, Yingyos Avihingsanon, Nawaporn Assawasaksakul, Supranee Buranapraditkun, and et al. 2022. "Comparison of Immunogenicity and Safety of Inactivated, Adenovirus-Vectored, and Heterologous Adenovirus-Vectored/mRNA Vaccines in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Prospective Cohort Study" Vaccines 10, no. 6: 853. https://doi.org/10.3390/vaccines10060853
APA StyleAssawasaksakul, T., Lertussavavivat, T., Sathitratanacheewin, S., Oudomying, N., Vichaiwattana, P., Wanlapakorn, N., Poovorawan, Y., Avihingsanon, Y., Assawasaksakul, N., Buranapraditkun, S., & Kittanamongkolchai, W. (2022). Comparison of Immunogenicity and Safety of Inactivated, Adenovirus-Vectored, and Heterologous Adenovirus-Vectored/mRNA Vaccines in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Prospective Cohort Study. Vaccines, 10(6), 853. https://doi.org/10.3390/vaccines10060853