
The Side Effects and Adverse Clinical Cases Reported after COVID-19 Immunization

 ,
,  ,
,  ,
, 
Abstract
:1. Need for Vaccination against COVID-19
2. Side Effects (SEs) and COVID-19 Vaccination Resistance
3. Selection and Collection of Data
4. COVID-19 Vaccinations’ Approval/Authorization
5. Studies Reporting SEs of COVID-19 Immunizations
5.1. Messenger RNA Based COVID-19 Immunization
5.1.1. Pfizer–BioNTech (BNT162b2) COVID-19 Vaccination
5.1.2. Moderna (mRNA-1273) COVID-19 Vaccination
5.2. Viral Vector-Based COVID-19 Immunization
5.2.1. AstraZeneca (ChAdOx1 nCoV-19) COVID-19 Vaccination
5.2.2. Covishield (AZD1222)
5.2.3. Janssen (Ad26.COV2.S) COVID-19 Vaccination
5.2.4. Sputnik V (Gam-COVID-Vac) COVID-19 Vaccination
5.3. Inactivated COVID-19 Immunization
5.3.1. Covaxin Vaccine (BBV152)
5.3.2. Sinovac
5.3.3. Sinopharm (BBIBP-CorV/Vero Cells) COVID-19 Vaccination
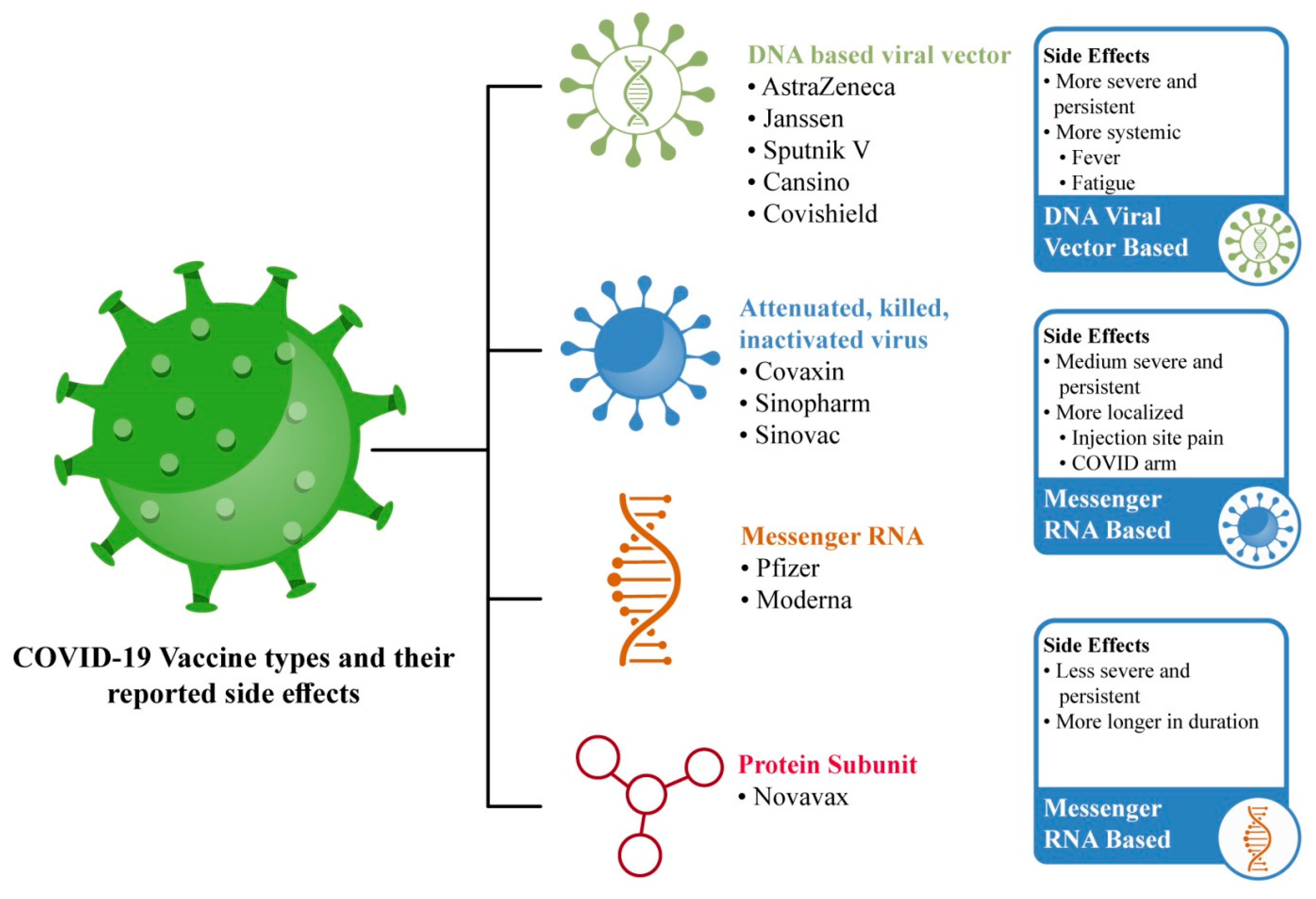
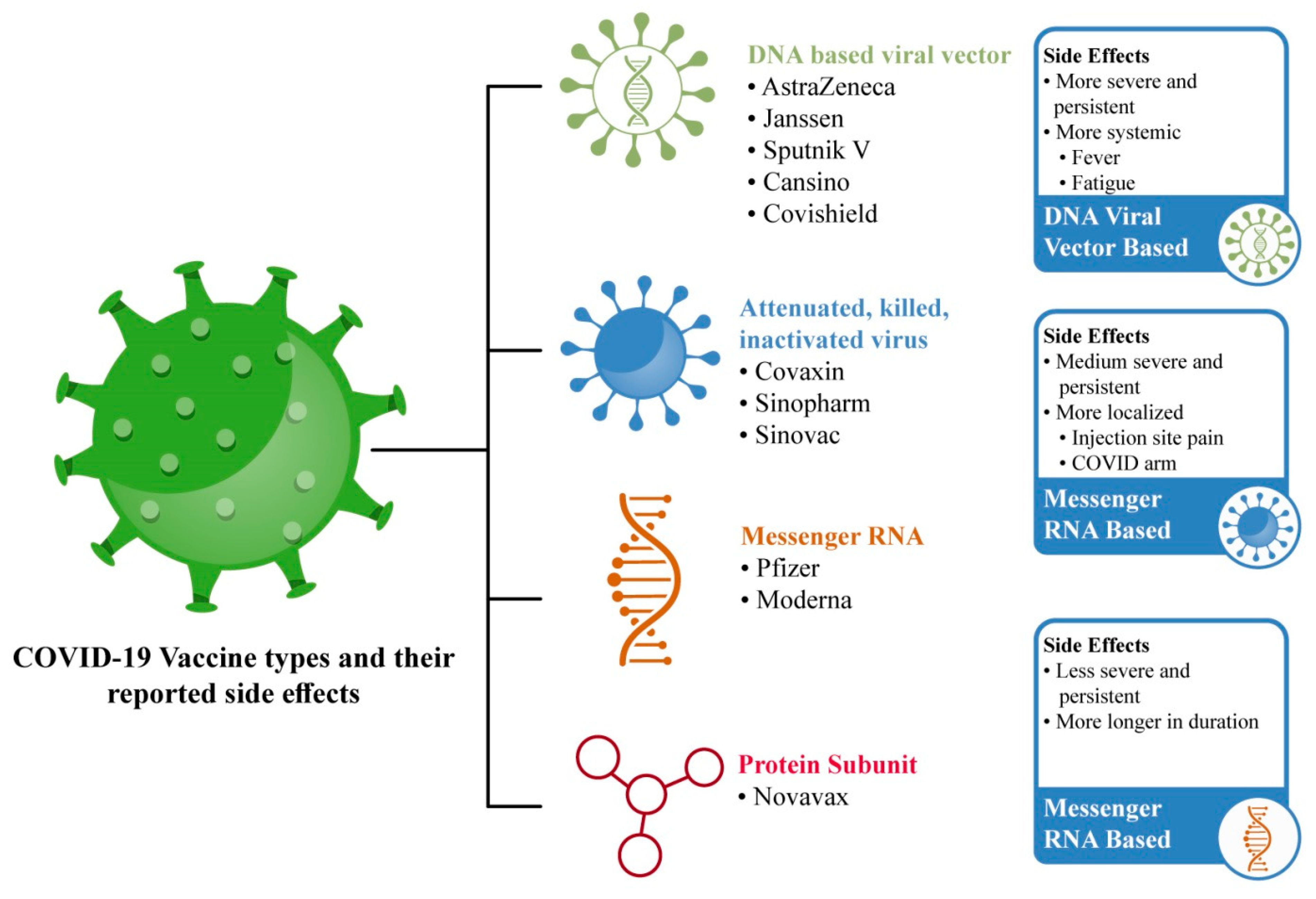
6. COVID-19 Vaccinations’ Reported Minor Side Effects
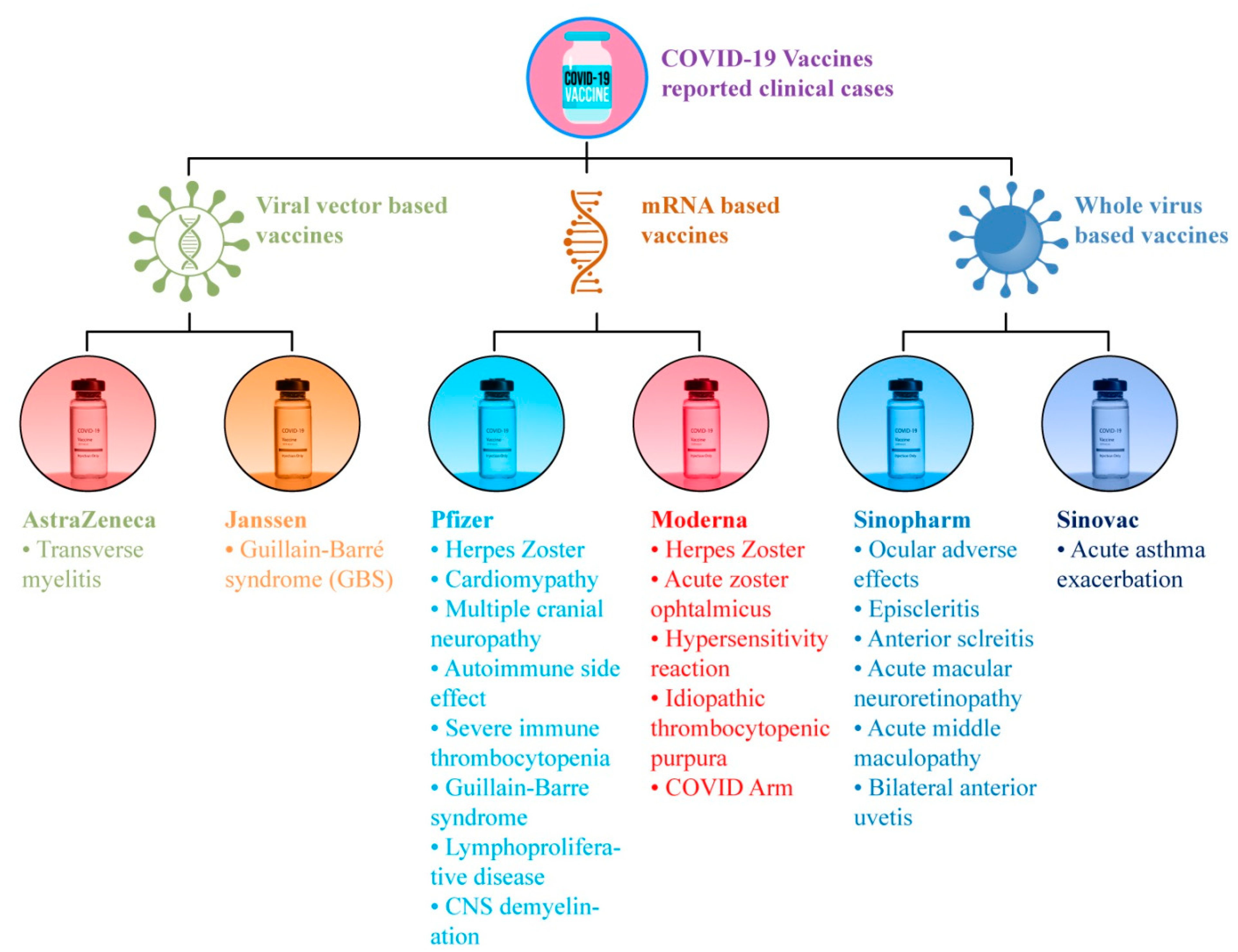
7. COVID-19 Vaccinations’ Reported Major Side Effects
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akarsu, B.; Canbay Özdemir, D.; Ayhan Baser, D.; Aksoy, H.; Fidancı, İ.; Cankurtaran, M. While studies on COVID-19 vaccine is ongoing, the public’s thoughts and attitudes to the future COVID-19 vaccine. Int. J. Clin. Pract. 2021, 75, e13891. [Google Scholar] [CrossRef] [PubMed]
- Di Micco, P.; Camporese, G.; Cardillo, G.; Lodigiani, C.; Carannante, N.; Annunziata, A.; Fiorentino, G.; Russo, V.; Imbalzano, E. Pathophysiology of vaccine-induced prothrombotic immune thrombocytopenia (Vipit) and vaccine-induced thrombocytopenic thrombosis (vitt) and their diagnostic approach in emergency. Med. Lith. 2021, 57, 997. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of covid-19 vaccine side effects among healthcare workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef] [PubMed]
- Rabail, R.; Saleem, J.; Tanveer, Z.; Patching, S.G.; Khalid, A.R.; Sultan, M.T.; Manzoor, M.F.; Karrar, E.; Inam-Ur-Raheem, M.; Shabbir, M.A.; et al. Nutritional and lifestyle changes required for minimizing the recovery period in home quarantined COVID-19 patients of Punjab, Pakistan. Food Sci. Nutr. 2021, 9, 5036–5059. [Google Scholar] [CrossRef] [PubMed]
- Rahaman, A.; Kumari, A.; Zeng, X.A.; Khalifa, I.; Farooq, M.A.; Singh, N.; Ali, S.; Alee, M.; Aadil, R.M. The increasing hunger concern and current need in the development of sustainable food security in the developing countries. Trends Food Sci. Technol. 2021, 113, 423–429. [Google Scholar] [CrossRef]
- Shahzamani, K.; Mahmoudian, F.; Ahangarzadeh, S.; Ranjbar, M.M.; Beikmohammadi, L.; Bahrami, S.; Mohammadi, E.; Esfandyari, S.; Alibakhshi, A.; Javanmard, S.H. Vaccine design and delivery approaches for COVID-19. Int. Immunopharmacol. 2021, 100, 108086. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Mekhemar, M.; Conrad, J.; Klugarová, J.; Koščík, M.; Klugar, M.; Attia, S. Safety of chadox1 ncov-19 vaccine: Independent evidence from two eu states. Vaccines 2021, 9, 673. [Google Scholar] [CrossRef]
- Murdaca, G.; Noberasco, G.; Olobardi, D.; Lunardi, C.; Maule, M.; Delfino, L.; Triggiani, M.; Cardamone, C.; Benfaremo, D.; Moroncini, G.; et al. Current take on systemic sclerosis patients’ vaccination recommendations. Vaccines 2021, 9, 1426. [Google Scholar] [CrossRef]
- Klugar, M.; Riad, A.; Mekhemar, M.; Conrad, J.; Buchbender, M.; Howaldt, H.P.; Attia, S. Side effects of mrna-based and viral vector-based covid-19 vaccines among german healthcare workers. Biology 2021, 10, 752. [Google Scholar] [CrossRef]
- Goss, A.L.; Samudralwar, R.D.; Das, R.R.; Nath, A. ANA Investigates: Neurological Complications of COVID-19 Vaccines. Ann. Neurol. 2021, 89, 856. [Google Scholar] [CrossRef]
- Saeed, B.Q.; Al-Shahrabi, R.; Alhaj, S.S.; Alkokhardi, Z.M.; Adrees, A.O. Side effects and perceptions following Sinopharm COVID-19 vaccination. Int. J. Infect. Dis. 2021, 111, 219–226. [Google Scholar] [CrossRef]
- Yoda, T.; Katsuyama, H. Willingness to receive covid-19 vaccination in japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Magadmi, R.M.; Kamel, F.O. Beliefs and barriers associated with COVID-19 vaccination among the general population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Shabbir, M.A.; Mehak, F.; Khan, Z.M.; Ahmed, W.; Haq, S.M.A.U.; Khan, M.R.; Bhat, Z.F.; Aadil, R.M. Delving the role of nutritional psychiatry to mitigate the COVID-19 pandemic induced stress, anxiety and depression. Trends Food Sci. Technol. 2022, 120, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Maitland, E.; Wang, S.; Nicholas, S.; Liu, R.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2021, 39, 247–254. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef]
- Kaplan, R.M.; Milstein, A. Influence of a COVID-19 vaccine’s effectiveness and safety profile on vaccination acceptance. Proc. Natl. Acad. Sci. USA 2021, 118, 2021726118. [Google Scholar] [CrossRef]
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS One 2021, 16, e0250555. [Google Scholar] [CrossRef]
- Gavi The COVID-19 Vaccine Race—Weekly Update. Available online: https://www.gavi.org/vaccineswork/covid-19-vaccine-race?gclid=Cj0KCQjw8eOLBhC1ARIsAOzx5cEoa2VnSPnys3WznKcdeff8JBByVvOjPuCNkXg8P4Gcy0nsLU8xJ5QaAuRwEALw_wcB (accessed on 20 October 2021).
- Bogdanov, G.; Bogdanov, I.; Kazandjieva, J.; Tsankov, N. Cutaneous adverse effects of the available COVID-19 vaccines: Effects of COVID-19 vaccines. Clin. Dermatol. 2021, 39, 523–531. [Google Scholar] [CrossRef]
- Yang, S.; Li, Y.; Dai, L.; Wang, J.; He, P.; Li, C.; Fang, X.; Wang, C.; Zhao, X.; Huang, E.; et al. Safety and immunogenicity of a recombinant tandem-repeat dimeric RBD-based protein subunit vaccine (ZF2001) against COVID-19 in adults: Two randomised. Lancet Infect. Dis. 2021, 21, 1107–1119. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, L.; Cao, H.; Liu, C. Research Article SARS-CoV-2 S1 is superior to the RBD as a COVID-19 subunit vaccine antigen. Med. Virol. 2020, 93, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Shemer, A.; Pras, E.; Einan-Lifshitz, A.; Dubinsky-Pertzov, B.; Hecht, I. Association of COVID-19 Vaccination and Facial Nerve Palsy A Case-Control Study. JAMA Otolaryngol. –Head Neck Surg. 2021, 147, 739–743. [Google Scholar] [CrossRef] [PubMed]
- FDA Emergency Use Authorization. Available online: https://www.fda.gov.ph/list-of-fda-issued-emergency-use-authorization (accessed on 17 October 2021).
- World Health Organization. 7 Vaccines Approved for Use by WHO. Available online: https://covid19.trackvaccines.org/agency/who (accessed on 23 October 2021).
- Karpiński, T.M.; Ożarowski, M.; Seremak-Mrozikiewicz, A.; Wolski, H.; Wlodkowic, D. The 2020 race towards SARS-CoV-2 specific vaccines. Theranostics 2021, 11, 1690–1702. [Google Scholar] [CrossRef] [PubMed]
- Siddique, S.; Ahmed, S. COVID-19 Vaccines in Pakistan: Efficacy, Adverse Effects and Availability. J. Islamabad Med. Dent. Coll. 2021 2021, 10, 125–130. [Google Scholar] [CrossRef]
- Craig, A.M.; Hughes, B.L.; Swamy, G.K. Coronavirus disease 2019 vaccines in pregnancy. Am. J. Obstet. Gynecol. MFM 2021, 3, 100295. [Google Scholar] [CrossRef]
- Pious, N.; Ingole, S.D. Race for COVID-19 Vaccine. Trends Biomater. Artif. Organs 2020, 34, 62–65. [Google Scholar]
- Kashte, S.; Gulbake, A.; El-Amin, S.F.; Gupta, A. COVID-19 vaccines: Rapid development, implications, challenges and future prospects. Hum. Cell 2021, 34, 711–733. [Google Scholar] [CrossRef]
- Self, W.H.; Tenforde, M.W.; Rhoads, J.P.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Parks, L.; et al. Comparative Effectiveness of Moderna, Pfizer-BioNTech, and Janssen (Johnson & Johnson) Vaccines in Preventing COVID-19 Hospitalizations Among Adults Without Immunocompromising Conditions—United States, March–August 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1337–1343. [Google Scholar]
- Mathioudakis, A.G.; Ghrew, M.; Ustianowski, A.; Ahmad, S.; Borrow, R.; Papavasileiou, L.P.; Petrakis, D.; Bakerly, N.D. Self-reported real-world safety and reactogenicity of covid-19 vaccines: A vaccine recipient survey. Life 2021, 11, 249. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Abu-halaweh, S.; Alqassieh, R.; Suleiman, A.; Al-sabbagh, M.Q. Qualitative Assessment of Early Adverse Effects of Pfizer – BioNTech and Sinopharm COVID-19 Vaccines by Telephone Interviews. Vaccines 2021, 9, 950. [Google Scholar] [CrossRef] [PubMed]
- Mcmahon, D.E.; Amerson, E.; Rosenbach, M.; Lipoff, J.B.; Moustafa, D.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: A registry-based study of 414 cases. J. Am. Dermatol. 2021, 85, 46–55. [Google Scholar] [CrossRef] [PubMed]
- El-Shitany, N.A.; Harakeh, S.; Badr-Eldin, S.M.; Bagher, A.M.; Eid, B.; Almukadi, H.; Alghamdi, B.S.; Alahmadi, A.A.; Hassan, N.A.; Sindi, N.; et al. Minor to moderate side effects of pfizer-biontech COVID-19 vaccine among saudi residents: A retrospective cross-sectional study. Int. J. Gen. Med. 2021, 14, 1389–1401. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, T.; Umeda, H.; Kojima, M.; Kanno, Y.; Tanaka, Y.; Kinoshita, N. Cumulative Adverse Event Reporting of Anaphylaxis After mRNA COVID-19 Vaccine (Pfizer-BioNTech) Injections in Japan: The First-Month Report. Drug Saf. 2021, 44, 1209–1214. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Sessa, M.; Kragholm, K.; Hviid, A.; Andersen, M.; Sessa, M.; Kragholm, K.; Hviid, A.; Andersen, M.; Sessa, M. Expert Opinion on Drug Safety Thromboembolic Events in Younger Women Exposed to Pfizer-BioNTech or Moderna COVID-19 Vaccines COVID-19 Vaccines; Taylor & Francis: Abingdon, UK, 2021. [Google Scholar]
- Shimabukuro, T.; Nair, N. Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine. Am. J. Transplant. 2021, 325, 780–781. [Google Scholar] [CrossRef]
- Andrzejczak-Grządko, S.; Czudy, Z.; Donderska, M. Side effects after COVID-19 vaccinations among residents of Poland. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4418–4421. [Google Scholar] [CrossRef]
- Al Khames Aga, Q.A.; Alkhaffaf, W.H.; Hatem, T.H.; Nassir, K.F.; Batineh, Y.; Dahham, A.T.; Shaban, D.; Al Khames Aga, L.A.; Agha, M.Y.R.; Traqchi, M. Safety of COVID-19 vaccines. J. Med. Virol. 2021, 93, 6588–6594. [Google Scholar] [CrossRef]
- Zare, H.; Rezapour, H.; Mahmoodzadeh, S.; Fereidouni, M. Prevalence of COVID-19 vaccines (Sputnik V, AZD-1222, and Covaxin) side effects among healthcare workers in the Birjand, Iran. Int. Immunopharmacol. 2021, 101, 108351. [Google Scholar] [CrossRef]
- Sahraian, M.A.; Ghadiri, F.; Azimi, A.; Moghadasi, A.N. Adverse events reported by Iranian patients with multiple sclerosis after the first dose of Sinopharm BBIBP-CorV. Vaccine 2021, 39, 6347–6350. [Google Scholar] [CrossRef] [PubMed]
- Anne, M.H.; Julianne, G.; Tara, J.; Amelia, J.; Paige, M.; Elaine, M.; John, S.; Tom, T.S.; David, K.S. Anxiety-Related Adverse Event Clusters After Janssen COVID-19 Vaccination. MMWR Morb Mortal Wkly Rep. 2021, 70, 685–688. [Google Scholar]
- Babamahmoodi, F.; Saeedi, M.; Navaei, R.A.; Akbar, H.; Seyed, A.M.; Gasem, O.; Shirafkan, K.; Zahra, A.; Mazaher, A.; Fatemeh, A.; et al. Side effects and Immunogenicity following administration of the Sputnik V COVID-19 vaccine in health care workers in Iran. Sci. Rep. 2021, 11, 21464. [Google Scholar] [CrossRef] [PubMed]
- Marco, M.; Giorgia, S.; Di, Z.V.; Salussolia, A.; Lenzi, J.; Montalti, M.; Sold, G.; Forcellini, M.; Barvas, E.; Guttmann, S.; et al. ROCCA observational study: Early results on safety of Sputnik V vaccine (Gam-COVID-Vac) in the Republic of San Marino using active surveillance. EClinicalMedicine 2021, 38, 4–10. [Google Scholar] [CrossRef]
- Pagotto, V.; Ferloni, A.; Soriano, M.M.; Diaz, M.; Golde, N.B.; González, M.I.; Asprea, V.; Staneloni, M.I.; Zingoni, P.; Vidal, G.; et al. Original article active monitoring of early safety of sputnik v vaccine in buenos aires, Argentina. Rev. Med. 2021, 81, 408–414. [Google Scholar]
- Jarynowski, A.; Semenov, A.; Kamiński, M.; Belik, V. Mild Adverse Events of Sputnik V Vaccine Extracted from Russian Language Telegram Posts via BERT Deep Learning Model. medRxiv 2021, 23, e30529. [Google Scholar] [CrossRef]
- Malik, H.A.; Faraz, A.; Bhatty, A.; Mumtaz, T. Prevalence of Adverse Reactions to Different COVID-19 Vaccinations among Karachi Residents. J. Pharm. Res. Int. 2021, 33, 379–386. [Google Scholar] [CrossRef]
- Amer, M.; Altaf, S.; Azhar, A. The safety of verocell covid-19 (sinopharm) vaccination among health care workers in khyber teaching hospital, peshawar. J. Med. Sci Ence 2021, 19, 99–103. [Google Scholar]
- Jaiswal, K.M.; Dudhgaonkar, S.; Raghute, L.; Uike, P.; Kohli, S.; Anand, I. An assessment of AEFI COVID-19 vaccination in health care workers at a tertiary health care centre in central India. Microbiol. Res. Int. 2021, 9, 46–50. [Google Scholar] [CrossRef]
- Bati, S.; Burucu, R.; Cantekin, I.; Donmez, H. Determining the Side Effects Of Covid-19 (Sinovac) Vaccination On Nurses; An Independent Descriptive Study. Konuralp Tıp Derg. 2021, 19, 479–487. [Google Scholar] [CrossRef]
- Papasavvas, I.; de Courten, C.; Herbort, C.P. Varicella-zoster virus reactivation causing herpes zoster ophthalmicus (HZO) after SARS-CoV-2 vaccination—Report of three cases. J. Ophthalmic Inflamm. Infect. 2021, 11, 28. [Google Scholar] [CrossRef]
- Pichi, F.; Aljneibi, S.; Neri, P.; Hay, S.; Dackiw, C.; Ghazi, N.G. Association of Ocular Adverse Events with Inactivated COVID-19 Vaccination in Patients in Abu Dhabi. JAMA Ophthalmol. 2021, 139, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Toida, R.; Uezono, S.; Komatsu, H.; Toida, T.; Imamura, A.; Fujimoto, S. Takotsubo Cardiomyopathy after Vaccination for Coronavirus Disease 2019 in a Patient on Maintenance Hemodialysis; Springer: Singapore, 2021. [Google Scholar]
- Manea, M.M.; Dragoș, D.; Enache, I.; George, A.; Tuta, S. Multiple cranial nerve palsies following COVID-19–Case report. Acta Neurol Scand. 2021, 145, 257–259. [Google Scholar] [CrossRef] [PubMed]
- ElSheikh, R.H.; Haseeb, A.; Eleiwa, T.K.; Elhusseiny, A.M. Acute Uveitis following COVID-19 Vaccination. Ocul. Immunol. Inflamm. 2021, 145, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Dube, G.K.; Benvenuto, L.J.; Batal, I. Antineutrophil Cytoplasmic Autoantibody–Associated Glomerulonephritis Following the Pfizer-BioNTech COVID-19 Vaccine. Kidney Int. Rep. 2021, 6, 3087–3089. [Google Scholar] [CrossRef]
- Shah, S.R.A.; Dolkar, S.; Mathew, J.; Vishnu, P. Case Report Covid-19 Vaccination Associated Severe Immune Thrombocytopenia. Exp. Hematol. Oncol. 2021, 10, 42. [Google Scholar]
- Waheed, S.; Bayas, A.; Hindi, F.; Rizvi, Z.; Espinosa, P.S. Neurological Complications of COVID-19: Guillain-Barre Syndrome Following Pfizer COVID-19 Vaccine. Cureus 2021, e134526. [Google Scholar] [CrossRef]
- Hiller, N.; Goldberg, S.N.; Cohen-Cymberknoh, M.; Vainstein, V.; Simanovsky, N. Lymphadenopathy Associated with the COVID-19 Vaccine. Cureus 2021, 13, e13524. [Google Scholar] [CrossRef]
- Mustafa, S.S.; Ramsey, A.; Staicu, M.L.; Information, D. Administration of a Second Dose of the Moderna COVID-19 Vaccine After an Immediate Hypersensitivity Reaction with the First Dose: Two Case Reports. Ann. Intern. Med. 2020, 174, 1177–1178. [Google Scholar] [CrossRef]
- Kristen, L.; Nichols, C.S.; Stephen, J.M.; Mark, C.M.; Fnu, N. REPORT A Case of Severe Cutaneous Adverse Reaction Following Administration of the Janssen; Elsevier, Inc.: Amsterdam, The Netherlands, 2021; Volume 13, pp. 134–137. [Google Scholar]
- Prasad, A.; Hurlburt, G.; Podury, S.; Tandon, M.; Kingree, S.; Sriwastava, S. A Novel Case of Bifacial Diplegia Variant of Guillain-Barr é Syndrome Following Janssen COVID-19 Vaccination. Neurol. Int. 2021, 13, 404–409. [Google Scholar] [CrossRef]
- Jeffrey, A.J.; Douglas, R.M. Idiopathic Thrombocytopenic Purpura and the Moderna Covid-19 Vaccine. Ann. Emerg. Med. 2021, 77, 654–656. [Google Scholar]
- Wei, N.; Fishman, M.; Wattenberg, D.; Gordon, M.; Lebwohl, M. COVID Arm: A reaction to the Moderna Vaccine; Elsevier, Inc.: Amsterdam, The Netherlands, 2021; Volume 10. [Google Scholar]
- Lee, C.; Cotter, D.; Basa, J.; Greenberg, H.L. 20 Post-COVID-19 vaccine-related shingles cases seen at the Las Vegas Dermatology clinic and sent to us via social media. J. Cosmet. Dermatol. 2021, 20, 1960. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Jiménez, P.; Chicharro, P.; Cabrera, L.M.; Seguí, M.; Morales-Caballero, Á.; Llamas-Velasco, M.; Sánchez-Pérez, J. Varicella-zoster virus reactivation after SARS- CoV-2 BNT162b2 mRNA vaccination: Report of 5 cases. JAAD Case Rep. 2021, 12, 58–59. [Google Scholar] [CrossRef]
- Sekar, A.; Campbell, R.; Tabbara, J.; Rastogi, P. ANCA Glomerulonephritis after the Moderna COVID-19 Vaccination; De Novo Vasculitis after mRNA-1273 (Moderna); International Society of Nephrology: Brussels, Belgium, 2021; Volume 100. [Google Scholar]
- Liu, B.D.; Ugolini, C.; Jha, P. Two Cases of Post-Moderna COVID-19 Vaccine Encephalopathy Associated with Nonconvulsive Status Epilepticus Case Presentation. Cureus 2021, 13, e16172. [Google Scholar]
- Ogai, A.; Yoshida, R.; Yuasa, C.; Chin, K.; Fujimaki, K.; Nakajima, H. Acute immune thrombocytopenia following SARS - CoV - 2 vaccination in chronic ITP patients and a healthy individual. Int. J. Hematol. 2021, 115, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Khayat, M.; Shamik, K.; Joshua, B.; Daniel, K.; Shahamat, H. COVID-19 mRNA vaccination leading to CNS inflammation: A case series. J. Neurol. 2021, 269, 1093–1106. [Google Scholar] [CrossRef] [PubMed]
- Uzer, F.; Cilli, A. Acute asthma exacerbation after SARS-CoV-2 vaccine (Sinovac®): A case report. Med. Gas Res. 2022, 12, 67–68. [Google Scholar] [CrossRef]
- De Matos, A.A.; Cardoso, G.P.; Neto, M.L. Sputnik v: Is the Russian Vaccine Safe? J. Clin. Epidemiol. 2021, 2, 1–2. [Google Scholar]
- Raina Maclntyre, C.; Veness, B.; Berger, D.; Hamad, N.; Bari, N. Thrombosis with Thrombocytopenia Syndrome (TTS) following AstraZeneca ChAdOx1 nCoV-19 (AZD1222) COVID-19 vaccination—A risk-benefit analysis for people < 60 years in Australia. Vaccine 2021, 39, 4784–4787. [Google Scholar]
- Soiza, R.L.; Scicluna, C.; Thomson, E.C. Efficacy and safety of COVID-19 vaccines in older people. Age Ageing 2021, 279–283. [Google Scholar] [CrossRef]
- Baraniuk, C. Covid-19: What do we know about Sputnik V and other Russian vaccines? BMJ 2021, 372, I743. [Google Scholar] [CrossRef] [PubMed]
- Saeed, U.; Uppal, S.R.; Piracha, Z.Z.; Uppal, R. SARS-CoV-2 Spike Antibody Levels Trend among Sinopharm Vaccinated People. Iran. J. Public Health 2021, 50, 1486. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Local/Given Name | Codename | Type | Origin: Company/Country | Approval/Authorization | Efficacy Trials Phase II/III/IV | References |
|---|---|---|---|---|---|---|
| Pfizer | BNT162b2 Vaccine | Uridine nucleoside modified mRNA (encodes the receptor-binding domain or full-length version of SARS-CoV-2 spike protein) | BioNTech (Germany) in collaboration with Fosun Pharmaceuticals (Shanghai, China) and Pfizer (Canada) | FDA-approved; FDA Emergency Use Authorization (EUA); WHO-approved in 103 countries; among first vaccines to get EUA in December 2020 | 95% efficacy. Safe during pregnancy. 38 trials in 20 countries. Phase IV registered on 27 September 2021 | [6,20,25,26,27,28,29,30] |
| Moderna | mRNA-1273 Vaccine | mRNA-based vaccine designed to express the coronavirus spike protein | Massachusetts (the United States) along with the National Institute of Allergy and Infectious Diseases and Biomedical Advanced Research and Development Authority | FDA-approved; FDA (EUA); WHO-approved in 76 countries; among first vaccines to get EUA in December 2020 | 94% efficacy; safe during pregnancy. 31 trials in 7 countries; phase II in August 2021; phase IV launched in June 2021 | [6,20,25,26,27,28,29,30] |
| Janssen | Ad26.COV2.S | Adenoviral-based vaccine | Johnson and Johnson/the United States, the Netherlands. | FDA-approved; FDA (EUA); WHO-approved in 75 countries | 13 trials in 3 countries. Phase IV launched in June 2021 | [6,20,25,26,28] |
| AstraZeneca/Vaxzevria | AZD1222 Vaccine/ChAdOx1 | Chimpanzee Adenovirus-Vectored vaccine | Oxford University under British pharmaceutical company | FDA (EUA); WHO emergency use listing (EUL) WHO-approved in 124 countries | 70% efficacy. 46 trials in 3 countries. Phase II/III was completed in June 2021; Phase IV was registered on 27 September 2021 [26] | [4,16,21,22,23,24,26] |
| Sputnik V | Gam-COVID-Vac | Adenoviral-based vaccine | Gamaleya National Research Centre of Epidemiology and Microbiology (Moscow, Russia) | FDA (EUA) | 91.6% efficacy; | [25,27,28,30] |
| Convidecia/CanSino | Ad5-nCoV Vaccine | The recombinant vaccine which involves replication-defective adenovirus type 5 as vector | Tianjin, China in collaboration with the Beijing Institute of Biotechnology in the Academy of Military Medical Sciences | - | 90% efficacy. Phase IV registered in May 2021 | [20,27,30] |
| Covaxin Vaccine | BBV152 | Inactivated vaccine candidate; deactivated rabies vaccine as a vehicle for coronavirus proteins | Bharat Biotech (India) in collaboration with Thomas Jefferson University of Philadelphia, Indian Council of Medical Research (ICMR) and National Institute of Virology (Pune, India) | FDA (EUA) | - | [25,27] |
| Sinopharm | New Crown COVID-19 Vaccine | Inactivated vaccine candidate | Wuhan Institute of Biological Products, (China) | FDA (EUA); WHO (EUL); WHO-approved in 68 countries | 79.34% efficacy. 15 trials in 9 countries | [20,25,26,27,28,30] |
| Sinovac/CoronaVac | CoronaVac Vaccine | Adsorbed (inactivated) vaccine | Sinovac Life Sciences Co. Ltd. (China) in collaboration with Instituto Butantan | WHO emergency use listing (EUL); WHO-approved in 41 countries | 65% efficacy; 22 trials in 2 countries. Phase IV registered on 27 September 2021 | [20,26,27,30] |
| Covishield | AZD1222 | (Oxford/ AstraZeneca formulation) | Serum Institute of India | WHO-approved in 46 countries? | 2 trials in 1 country | [26] |
| Novavax | NVX-CoV2373 | Antigenic components (spike (S) protein) generated in vitro (Viral subunit) | - | - | - | [30,31] |
| Vaccine Name | Methodology | Participant/Area | Date/Duration | Minor Side Effects | Major Side Effects | Duration | Concluding Remarks | References |
|---|---|---|---|---|---|---|---|---|
| Pfizer– BioNTech COVID-19 (17%) and Moderna (83%) | A collaborative study between the American Academy of Dermatology and the International League of Dermatological Societies | 414 cutaneous reaction cases | December 2020–February 2021 | Local injection site reactions, urticarial eruptions, morbilliform eruptions. | Pernio/chilblains, cosmetic filler reactions, zoster, herpes simplex flares, pityriasis rosea. | - | The presence of a cutaneous reaction to the first vaccine dose, when it appears 4 h after injection, is not a contraindication to receiving the second dose of the Pfizer or Moderna vaccine. | [36] |
| Pfizer–BioNTech COVID-19 | Google Form-questionnaire (online survey) | 455 individuals Saudi Arabia inhabitants | 10–21 January 2021 | Injection site pain, headaches, flu-like symptoms, fever, tiredness, fast heartbeat, whole-body aches, difficulty breathing, joint pain, chills, drowsiness. | Bell’s palsy, lymph node swelling and tenderness. | - | - | [37] |
| Pfizer–BioNTech COVID-19 | Pharmaceutical and Medical Devices Agency (PMDA) reported adverse events following immunization (AEFI) | 578,835 doses | February–March 2021 | - | 181 suspected event reports of anaphylaxis and anaphylactoid symptoms (reporting rate: 8.1/100,000 doses) | - | In 171 of these 181 cases, women developed these symptoms. | [38] |
| Pfizer–BioNTech COVID-19 (64.5%) and Moderna (35.5%) | Cross-sectional trial with an independent online questionnaire | 1245 HCWs | 24 January–10 March 2021 | Soreness, fatigue, myalgia, headache, chills, fever, joint pain, nausea, muscle spasm, sweating, dizziness, flushing, feelings of relief, brain fogging, anorexia, localized swelling, decreased sleep quality, itching, tingling, diarrhea, nasal stuffiness, palpitations. | - | - | - | [39] |
| Pfizer–BioNTech COVID-19 and Moderna | Vaccine Adverse Event Reporting System (VAERS); Food and Drug Administration Adverse Event Reporting System (FAERS) | Women aged ≤50 years with hormonal contraceptive use | 19 March 2021 | - | 68 thromboembolic events (1 case per 222,951 vaccinated) thromboembolic events under investigation: thrombosis, cerebrovascular accident, myocardial infarction, pulmonary embolism. | 1–6 days after vaccination | - | [40] |
| Pfizer–BioNTech COVID-19 | Cross-sectional survey-based study | HCW in the Czech Republic | January–February 2021 | Injection site pain, fatigue, headache, muscle pain, chills. | - | 1 or 3 days | SEs more prevalent among the ≤43-year-old age group. | [7] |
| Moderna COVID-19 vaccine | CDC report (VAERS) | 108 case reports of severe allergic reaction, including anaphylaxis | 21 December 2020–10 January 2021 | Pruritus, rash, itchy sensations in the mouth and throat, sensations of throat closure, and respiratory symptoms. | 10 cases of anaphylaxis (2.5 anaphylaxis cases/million Moderna COVID-19 vaccine doses. | 7–30 min after vaccination | - | [41] |
| AstraZeneca and Pfizer–BioNTech | Online survey | Total 705: Pfizer 196. AstraZeneca 509 | - | Injection site pain, shoulder pain, muscle aches, headaches, fever, chills, weakness, nausea, vomiting, diarrhea in both vaccines. General stomach problems, osteoarticular pain, back pain, neck pain, drowsiness, feeling cold, fast heart rate and palpitations in AstraZeneca. Hand numbness, enlarged lymph nodes in Pfizer. | - | - | AstraZeneca causes more SEs. Pfizer had the same or more adverse reactions after the second dose; AstraZeneca’s second dose caused even stronger SEs. | [42] |
| Pfizer-BioNTech, Moderna and AstraZeneca | Online questionnaire | 599 HCWs in the Federal Republic of Germany | February–April 2021 | Injection site pain, headache, fatigue, muscle pain, malaise, chills, joint pain. More than one-sixth participants reported at least one oral side effect, including mucosal lesions, oral paresthesia, taste disturbance. | - | 1–3 days | mRNA-based vaccines: more local SEs. Viral vector-based vaccine: higher systemic SEs. Females and the younger age groups are more associated with an increased risk of SEs. | [9] |
| Pfizer- BioNTech and AstraZeneca | COVID symptom study app | 282103 individuals (aged 16–99 years) | 8 December 2020–10 March 2021 | Headache, fatigue, chills, shivering, diarrhea, fever, arthralgia, myalgia, nausea, pain, swelling, tenderness, itch, swollen armpit glands, redness, warmth, bruising, allergic reactions, rash, skin burning, red welts on face and lip. | - | 1–2 days | Adverse effects are more frequently reported in younger individuals, women, and among those who previously had COVID-19. | [34] |
| Pfizer-BioNTech, AstraZeneca, and Sinopharm | An interactive web-based system interview with an electronic version of the questionnaire | 1736 (18–86 years age). Pfizer 700. AstraZeneca 696; Sinopharm 340 | 1 January–10 April 2021 | Fatigue, body pain, headache, muscle pain, fever, gastrointestinal effects (nausea, vomiting, anorexia, and diarrhea) in all three vaccines; tenderness or swollen lymph nodes in Pfizer; sweating, dizziness, dry cough, anxiety, shortness of breath, tachycardia, abdominal pain, sore throat, joint pain, nasal discharge in AstraZeneca | Six cases: (four- Pfizer and two AstraZeneca) admitted into the hospital due to severe hypotension, generalized body aches, shortness of breath, and fever of more than 39 °C. Four cases (2 swelling and severe allergic reaction of eyelids and 2 acute hypertension—over 210/105 mm Hg) in Pfizer vaccine. | 1–2.5 days | Signs and symptoms are more persistent for AstraZeneca followed by Pfizer and less adverse with Sinopharm. | [43] |
| AstraZeneca, Sputnik-V and Covaxin | 503 HCWs in Birjand (Iran) | 21 February–7 March 2021 | Injection site pain, fatigue, muscle pain, fever in all three vaccines. | - | - | SEs more persistent in female; Sputnik V and Covaxin reported lower SE occurrence in the elderly. | [44] | |
| Sinopharm (51.1%) and Pfizer–BioNTech (48.9%) | Semi-structured interviews on a phone call | 1004 Jordanian adults with no history of previous allergies | 10 March–2 April 2021 | Local and systemic effects: pain at the injection site, fatigue, headaches, myalgia, arthralgia, fever, rigors. | No serious cases of hospitalization. | - | Pfizer was associated with greater rates, while Sinopharm was associated with a longer duration of SEs. | [35] |
| Sinopharm | Google form | 583 Iranian multiple sclerosis (MS) patients | 1 May–22 May 2021 | Malaise, fatigue, fever, shivering, body pain, headache. | Five recipients (0.9%) reported MS relapse. | - | - | [45] |
| AstraZeneca | Cross-sectional survey-based study | 92 HCWs/Germany and the Czech Republic | March 2021 | injection site discomfort, fatigue, muscle pain, chills, feeling unwell, nausea, headache | No serious cases of hospitalization/no blood disorder. | - | Chronic diseases were not associated with an increased risk of SE. | [7] |
| Janssen | VAERS | 64 anxiety-related events | 7–9 April 2021 | tachycardia (rapid heart rate), hyperventilation (rapid breathing), dyspnea (difficulty breathing), chest pain, paresthesia (numbness or tingling), light-headedness, hypotension (low blood pressure), headache, pallor, or syncope | 17 reports of syncope (fainting): 8.2 episodes per 100,000 doses. | Immediately after vaccination. | - | [46] |
| Sputnik V | Observational study | 3236 reports out of 13,435 HCW | February–April 2021 | pain in the injection site, fatigue, body pain, headache, fever, joint pain, chilling, drowsiness. | - | - | SEs more frequent in females and younger individuals. | [47] |
| Sputnik V | E-questionnaire | 2558 people from San Marino; aged 18-89 years | 4 March–8 April 2021 | Local site pain, nodules, swelling, warmth, asthenia, headache, joint pain, muscle pain, chills, malaise, fever. | - | - | Sputnik V shows a strong tolerance profile in the population aged ≥60 years. | [48] |
| Sputnik V | An observational cohort study by the Ministry of Health of Buenos Aires City (CABA) | 707 HCWs in Hospital Italiano de Buenos Aires | 5–20 January 2021 | Injection site pain, redness, swelling. Fever, diarrhea, muscle pain. | - | - | - | [49] |
| Sputnik V | LabelStudio data labeling tool to label the dataset | 4579 entities | December 2020–April 2021 | Injection site pain, fever, fatigue, headache, insomnia, nausea, vomiting, redness, pruritus, swelling, lymph nodes enlargement, diarrhea, chills. | - | - | - | [50] |
| Sinopharm | Cross-sectional survey | The United Arab Emirates | January–April 2021 | Injection site pain, fatigue, headache, lethargy, fatigue, tenderness. | No serious cases of hospitalization. | - | SEs are more common in ≤49 years of age and females. | [11] |
| Sinopharm | Web-based cross-sectional survey. | ≥18 years of age 2000 resident of Karachi | 11 April–23 April 2021 | Fever, muscle pain, chills, arm pain, breathlessness, diarrhea, cough, flu, fatigue, chest pain, headache, abdominal pain, swelling in the legs and arms, multiple bruises, productive bleeding. | - | - | - | [51] |
| Sinopharm COVID-19 | Closed-ended questionnaire | 155/400 Healthcare workers (HCWs) >18 years old; Khyber Teaching Hospital, Peshawar, Pakistan | March 2021 | Pain at the injection site, weariness, headache, light-headedness, myalgia. | No serious cases of hospitalization. | - | More SE in the 24–42-year age group; Sinopharm vaccine has no or minor negative effects. | [52] |
| Covishield | Web-based self-report submission or vaccine event reporting system | 5637 HCWs in India | 16 January–6 February 2021 | Mild fever, myalgia, cold, cough, headache, local pain, swelling, fatigue, diarrhea, rigors, joint pain, nausea | - | - | - | [53] |
| Sinovac | Questionnaire | 355 nurses in Turkey | - | fatigue, headache, arthritis, sore throat, nausea, fever, vertigo, nasal flow, appetite changes, diarrhea, itchiness, abdominal pain, cough, changes in the mucosa, changes in taste sensation. | - | - | - | [54] |
| Different/Others | Online poll | 2002 | February 2021 | Fever, dyspnea, flu-like illness, weariness, local reactions. | Few serious adverse effects such as anaphylaxis, in viral vector-based immunizations. | - | mRNA vaccines linked with higher but milder incidence of any side effect. | [33] |
| Different/Others | VAERS | 9442 reports of adverse events in the United States | March 2021 | Dizziness, headaches, discomfort, muscular spasms, myalgia, paresthesia. | Stroke (17), GBS (32), facial palsy (190), transverse myelitis (9 cases), acute disseminated encephalomyelitis (6 cases). | - | The rare occurrence of tinnitus, dysphonia, convulsions, and herpes zoster recurrence was reported. | [10] |
| Vaccine | Cases | Patient | Date/Duration | Complication/Side Effects | References |
|---|---|---|---|---|---|
| mRNA-based COVID-19 immunization | Case I (Pfizer BioNTech) | 73-year-old female | 16 days after the first dose | Acute zoster ophthalmicus (HZO) in right V1 dermatome | [55] |
| Case II (Pfizer BioNTech) | 69-year-old female | 10 days after the first dose | HZO in left V1 dermatome | ||
| Case II (Moderna) | 72-year-old female | 13 days after the first dose | An eruption in the left V1 dermatome | ||
| Inactivated COVID-19 immunization | 7 cases (Sinopharm COVID-19) | 30–55 year seven patients (3 males) | Within 15 days of first dose | Ocular adverse effects: episcleritis, anterior scleritis, acute macular neuroretinopathy, acute middle maculopathy, subretinal fluid | [56] |
| mRNA-based COVID-19 immunization | One case (Pfizer BioNTech) | 80-year-old female on hemodialysis for two and half years | 4 days after the first dose | Takotsubo cardiomyopathy with LV outflow tract obstruction | [57] |
| mRNA-based COVID-19 immunization | One case (Pfizer BioNTech) | 29-year- old male | 6 days after the first dose | Multiple cranial neuropathy | [58] |
| Inactivated COVID-19 immunization | One case (Sinopharm COVID-19) | 18-year-old female | 5 days after second dose | Anterior uveitis associated with juvenile idiopathic arthritis (JIA) | [59] |
| viral vector-based COVID-19 immunization | Two cases (AstraZeneca vaccine) | - | - | Transverse myelitis is a neurological disorder; unlikely to be related to the vaccine as the patient already had multiple sclerosis | [10] |
| mRNA-based COVID-19 immunization | One case (Pfizer- BioNTech) | 29-year-old female | 16 days after the second dose | Autoimmune side effect: antineutrophil cytoplasmic autoantibody (ANCA)-associated vasculitis of acute kidney injury | [60] |
| mRNA-based COVID-19 immunization | Case I (Pfizer- BioNTech COVID-19 vaccine) | 53-year-old male with no previous history | 8 days after the second dose | Severe immune thrombocytopenia (ITP); platelet count of 2 × 109/L | [61] |
| Case II (Pfizer- BioNTech COVID-19 vaccine) | 67-year-old male previous chronic ITP patient but no history of recent flares of ITP | 2 days after the first dose | Severe ITP; platelet count of 2 × 109/L | ||
| Viral vector-based COVID-19 immunization | Case III (Janssen COVID-19 vaccine) | 59-year-old female with a history of chronic ITP | 2 days after the first dose | Severe ITP; platelet count of 64 × 109/L | |
| mRNA-based COVID-19 immunization | One case (Pfizer- BioNTech COVID-19 vaccine) | 82-year-old female | 2 weeks after the first dose | Guillain-Barré syndrome (GBS) with generalized body aches, paresthesia, and difficulty walking | [62] |
| mRNA-based COVID-19 immunization | Case I (Pfizer- BioNTech COVID-19 vaccine) | 47-year-old female | 15 days after first dose | Lympho-proliferative disease: left infra-clavicular non-painful lump along with fatigue, myalgia, and mild pyrexia to 38 °C | [63] |
| Case II (Pfizer- BioNTech COVID-19 vaccine) | 46-year-old female | 5 days after first dose | Left supraclavicular and axillary painful multiple enlarged lymph nodes, along with headaches, chills. | ||
| Case III (Pfizer- BioNTech COVID-19 vaccine) | 42-year-old female | 18 days after the first dose | Left axillary lymph nodes up to 2 cm in diameter | ||
| mRNA-based COVID-19 immunization | Case I (Moderna COVID-19 vaccine) | 64 -year-old female with a history of shellfish allergy | Within 10 min of the first dose | Hypersensitivity reaction with generalized pruritus, urticaria, and self-reported tachycardia | [64] |
| Case II (Moderna COVID-19 vaccine) | 39-year-old female with history of allergic rhinitis | Within 15 min of the first dose | Hypersensitivity reaction with chest and neck urticarial and mild facial angioedema | ||
| Inactivated COVID-19 immunization | One case (Sinopharm COVID-19) | 18-year-old female with a history of antinuclear antibody positive oligoarticular juvenile idiopathic arthritis (JIA) | 5 days after the second dose | Bilateral anterior uveitis with reduced visual acuity in both eyes | [59] |
| Viral vector-based COVID-19 immunization | One case (Janssen COVID-19 vaccine) | 74-year-old male | 3 days after the dose | Severe cutaneous adverse reaction with panhypopituitarism secondary to craniopharyngioma resection, vision loss of the left eye, neurogenic bladder, and obstructive sleep apnea | [65] |
| Viral vector-based COVID-19 immunization | One case (Janssen COVID-19 vaccine) | 41-year-old morbidly obese gentleman | Within four weeks of dose | Guillain-Barré syndrome (GBS) | [66] |
| mRNA-based COVID-19 immunization | One case (Moderna COVID-19 vaccine) | 72-year-old female | 1 day after receiving the first dose | Idiopathic thrombocytopenic purpura with a rash, spontaneous oral bleeding, headache and easy bruising or abnormal bleeding. | [67] |
| mRNA-based COVID-19 immunization | Case I (Moderna COVID-19 vaccine) | 74-year-old female | 8 days after the first dose | COVID arm: pruritic, erythematous plaque with mild scaling on her left upper arm, rash spread to 15 cm in diameter over 10 days | [68] |
| Case II (Moderna COVID-19 vaccine) | 62-year-old female | 8 days after the first dose | COVID arm: Pruritic erythematous rash on her left deltoid, began as a maculopapular eruption over the injection site | ||
| Case III (Moderna COVID-19 vaccine) | 54-year-old female | 7 days after the first dose | COVID arm: Erythematous, non-scaly patch on her left upper arm | ||
| Case IV (Moderna COVID-19 vaccine) | 72-year-old female | 10 days after the first dose | COVID arm: Erythematous patch on left deltoid surrounding the injection site, pruritic, warm to the touch, and measured 14 cm in diameter | ||
| mRNA-based COVID-19 immunization | Case I (Moderna COVID-19 vaccine) | 77-year-old male with a history of Psoriasis and Crohn’s Disease | 2 days after the first dose | Shingles (herpes zoster) with severely painful, unilateral dermatomal herpetiform eruptions | [69] |
| Case II (Pfizer- BioNTech COVID-19 vaccine) | 65-year-old male | After second dose | Shingles (herpes zoster) with painful, erythematous, clustered skin eruptions and pruritus | ||
| mRNA-based COVID-19 immunization | Case I (Pfizer- BioNTech COVID-19 vaccine) | 58-year-old male | 1 day after first dose | Varicella-zoster virus reactivation: herpetiform umbilicated vesicle with fever and cervical lymphadenopathy | [70] |
| Case II (Pfizer- BioNTech COVID-19 vaccine) | 47-year-old female | 5 days after the first dose | Varicella-zoster virus reactivation: herpetiform umbilicated vesicle with fever and dysesthesia | ||
| Case III (Pfizer- BioNTech COVID-19 vaccine) | 39-year-old male | 3 days after the first dose | Varicella-zoster virus reactivation: painful Herpetiform umbilicated vesicles | ||
| Case IV (Pfizer- BioNTech COVID-19 vaccine) | 56-year-old female | 2 days after the second dose | Varicella-zoster virus reactivation: herpetiform umbilicated vesicle with fever and dysesthesia | ||
| Case V (Pfizer- BioNTech COVID-19 vaccine) | 41-year-old female | 16 days after the second dose | Varicella-zoster virus reactivation: herpetiform umbilicated vesicle with fever and dysesthesia | ||
| mRNA-based COVID-19 immunization | Case I (Moderna COVID-19 vaccine) | 52-year-old male | 2 weeks after the dose | Anti-neutrophil cytoplasmic antibody (ANCA) glomerulonephritis | [71] |
| Case II (Moderna COVID-19 vaccine) | 39-year-old male | Immediately after second dose | Acute kidney injury (AKI) with nephritic syndrome, de novo vasculitis | ||
| Case III (Moderna COVID-19 vaccine) | 81-year-old male | Mild after the first dose, worsened after the second dose | AKI, proteinuria, de novo vasculitis | ||
| mRNA-based COVID-19 immunization | Case I (Moderna COVID-19 vaccine) | 86-year-old female | 7 days after the dose | Encephalopathy associated with non-convulsive status epilepticusat, poor neurological function, acute confusion, Visual hallucinations, Left frontal headache | [72] |
| Case II (Moderna COVID-19 vaccine) | 73-year-old male | 7 days after the first dose | Encephalopathy associated with non-convulsive status epilepticusat, staring episodes, restlessness, cognitive deficits. | ||
| mRNA-based COVID-19 immunization | Case I (Pfizer- BioNTech COVID-19 vaccine) | 64-year-old woman with chronic idiopathic thrombocytopenic purpura (ITP) | 2 days after the first dose | Acute immune thrombocytopenia with oral bleeding and generalized petechiae. | [73] |
| Case II (Pfizer- BioNTech COVID-19 vaccine) | 61-year-old woman with scleroderma | After the second dose | Acute immune thrombocytopenia with petechiae on both legs after. | ||
| Case III (Moderna COVID-19 vaccine) | 73-year-old woman | 11 days after the first dose | Acute immune thrombocytopenia with generalized petechiae. | ||
| mRNA-based COVID-19 immunization | Case I (Moderna COVID-19 vaccine) | 35-year-old Caucasian woman, stable history of clinically isolated demyelinating syndrome (CIS), | Twenty-one days after the second dose | CNS demyelination: New neurologic symptoms with ataxia/dysmetria in the right upper extremity, and mild gait ataxia, with an Expanded Disability Status Scale (EDSS) score of 2.5. | [74] |
| Case II (Moderna COVID-19 vaccine) | 26-year-old white Hispanic woman no significant past medical history | Fourteen days after the second dose | CNS demyelination: New visual symptoms involving the right eye, mild blurring, progressed to worsening blurriness and pain with eye movement OD. | ||
| Case III (Pfizer- BioNTech COVID-19 vaccine) | 24-year-old Vietnamese woman | One day after the second dose | CNS demyelination: Presented with new onset left eye vision changes; visual symptoms in the right eye with blurred vision and pain on eye movement with monocular decreased visual acuity. | ||
| Case IV (Pfizer- BioNTech COVID-19 vaccine) | 64-year-old Caucasian man with no history of neurologic diseases, | Eighteen days after the first dose | CNS demyelination: Pain and paresthesia in his upper abdomen progressed to right lower extremity numbness, weakness, pain and numbness in the bilateral lower extremities, saddle anesthesia, sphincter dysfunction, and balance/gait difficulty. | ||
| Case V (Pfizer- BioNTech COVID-19 vaccine) | 33-year-old Caucasian man with no significant past medical history | One day after the second dose | CNS demyelination: Unilateral painless blurring of vision with visual acuity of 20/50 OS and multiple T2 hyperintense white matter lesions on brain MRI. | ||
| Case VI (Moderna COVID-19 vaccine) | 44-year-old Caucasian woman with a medical history of MS at age 20 when | Six days after the second dose | CNS demyelination: Transient low-grade fever with new neurological symptoms including numbness that ascended from her feet to the middle of her waist without any bowel or bladder incontinence. EDSS score of 1.5 with mild right deltoid and iliopsoas weakness. | ||
| Case VII (Pfizer- BioNTech COVID-19 vaccine) | 48-year-old Caucasian woman with a history of the Clinically isolated demyelinating syndrome (CIS) | 15 days after the first dose | CNS demyelination: developed with a painful sensation behind her right eye, worsening with eye movement; Brain MRI showed three new T2 hyperintense white matter lesions compared to prior imaging 2 years earlier. | ||
| Inactivated COVID-19 immunization | One case (CoronaVac, Sinovac) | A 76-year-old female | 1 day after vaccination | Acute asthma exacerbation with multiple infiltrations in both lungs and ground-glass shadows in both lung fields. | [75] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabail, R.; Ahmed, W.; Ilyas, M.; Rajoka, M.S.R.; Hassoun, A.; Khalid, A.R.; Khan, M.R.; Aadil, R.M. The Side Effects and Adverse Clinical Cases Reported after COVID-19 Immunization. Vaccines 2022, 10, 488. https://doi.org/10.3390/vaccines10040488
Rabail R, Ahmed W, Ilyas M, Rajoka MSR, Hassoun A, Khalid AR, Khan MR, Aadil RM. The Side Effects and Adverse Clinical Cases Reported after COVID-19 Immunization. Vaccines. 2022; 10(4):488. https://doi.org/10.3390/vaccines10040488
Chicago/Turabian StyleRabail, Roshina, Waqar Ahmed, Madiha Ilyas, Muhammad Shahid Riaz Rajoka, Abdo Hassoun, Abdur Rauf Khalid, Moazzam Rafiq Khan, and Rana Muhammad Aadil. 2022. "The Side Effects and Adverse Clinical Cases Reported after COVID-19 Immunization" Vaccines 10, no. 4: 488. https://doi.org/10.3390/vaccines10040488
APA StyleRabail, R., Ahmed, W., Ilyas, M., Rajoka, M. S. R., Hassoun, A., Khalid, A. R., Khan, M. R., & Aadil, R. M. (2022). The Side Effects and Adverse Clinical Cases Reported after COVID-19 Immunization. Vaccines, 10(4), 488. https://doi.org/10.3390/vaccines10040488