
Decline of Humoral Responses 6 Months after Vaccination with BNT162b2 (Pfizer–BioNTech) in Patients on Hemodialysis

 , , ,
, , ,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. SARS-CoV-2 IgG Quantification Assays
2.2. SARS-CoV-2 Neutralization Assay
2.3. Statistical Analysis
2.4. Analysis of Risk Factors
2.5. Ethics
3. Results
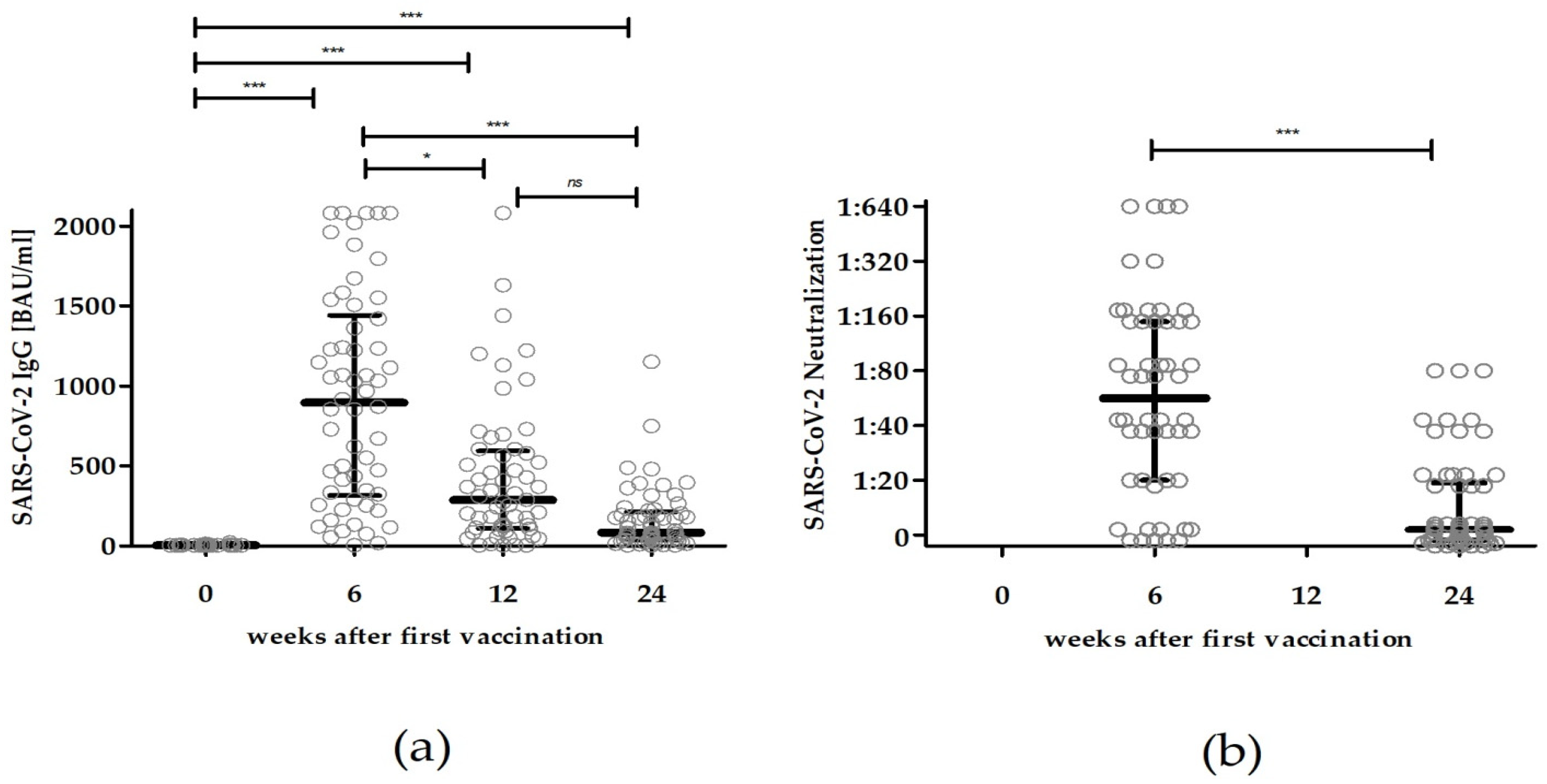
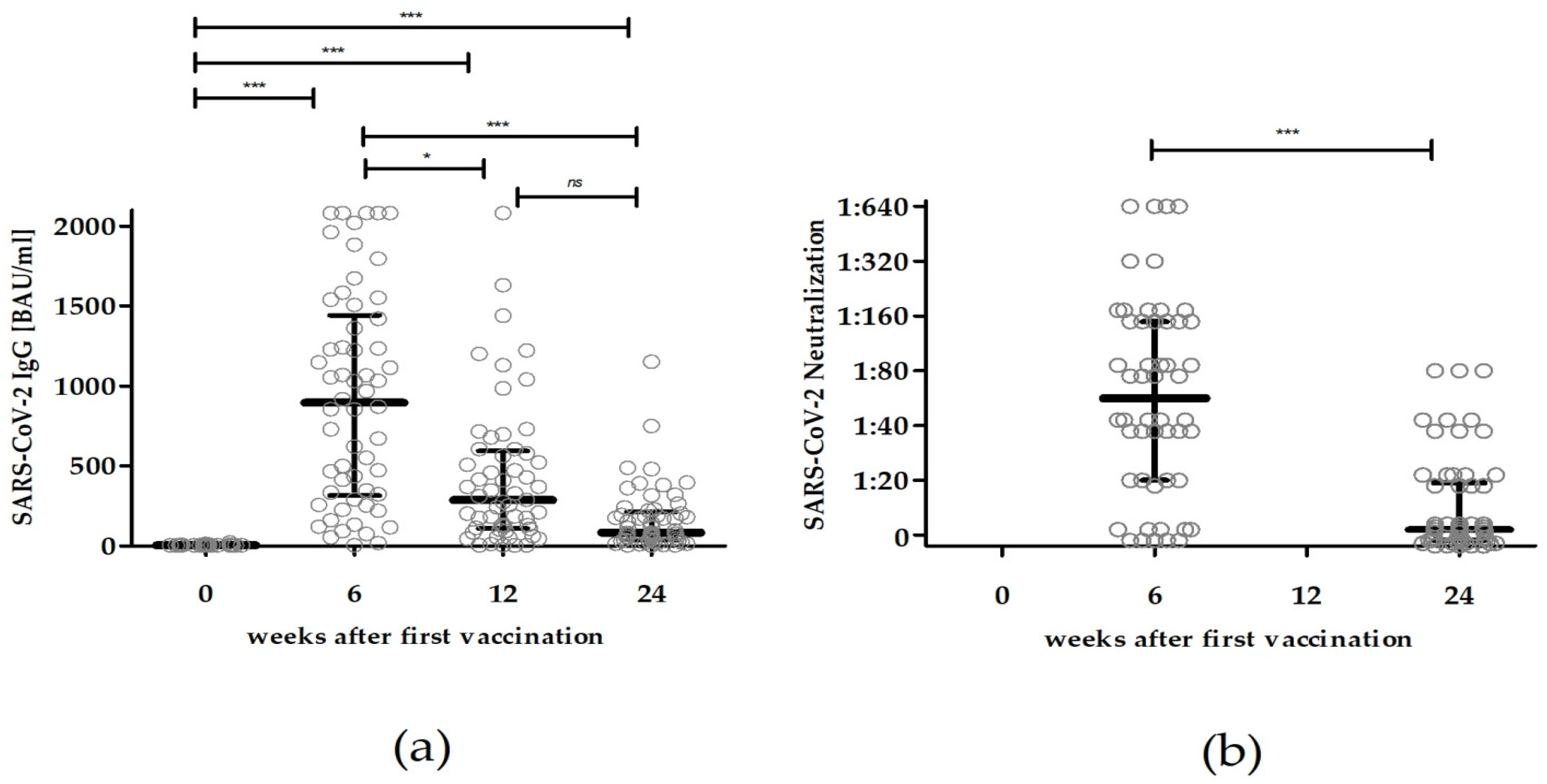
3.1. SARS-CoV-2 Binding Serum Antibody Titers after Vaccination with BNT162b2
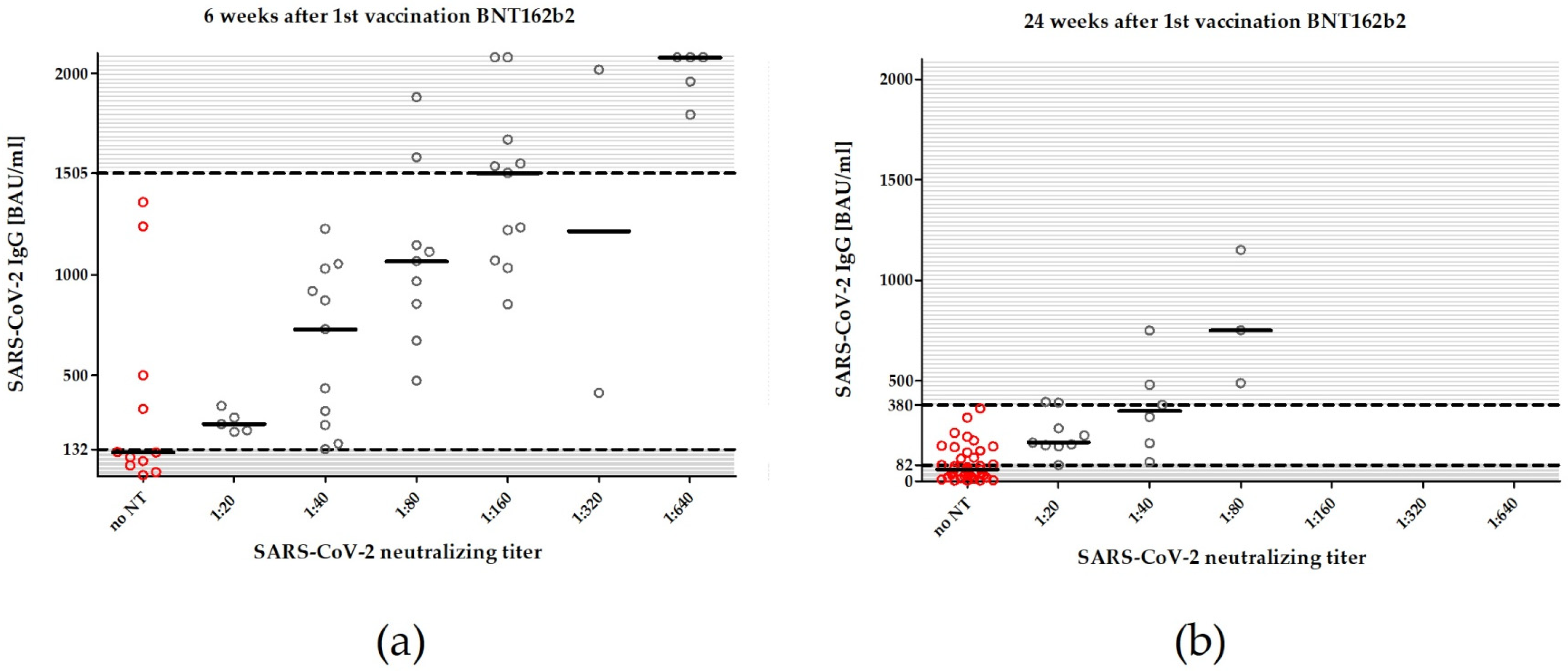
3.2. SARS-CoV-2 Neutralizing Antibody Titers after Vaccination with BNT162b2
3.3. Risk Factors for Antibody Titers <33.8 BAU/mL 24 Weeks after the First Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruchfeld, A. The COVID-19 pandemic: Consequences for nephrology. Nat. Rev. Nephrol. 2021, 17, 81–82. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Valeri, A.M.; Robbins-Juarez, S.Y.; Stevens, J.S.; Ahn, W.; Rao, M.K.; Radhakrishnan, J.; Gharavi, A.G.; Mohan, S.; Husain, S.A. Presentation and Outcomes of Patients with ESKD and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1409–1415. [Google Scholar] [CrossRef] [PubMed]
- Goffin, E.; Candellier, A.; Vart, P.; Noordzij, M.; Arnol, M.; Covic, A.; Lentini, P.; Malik, S.; Reichert, L.J.; Sever, M.S.; et al. COVID-19-related mortality in kidney transplant and haemodialysis patients: A comparative, prospective registry-based study. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 36, 2094–2105. [Google Scholar] [CrossRef]
- Labriola, L.; Scohy, A.; Van Regemorter, E.; Robert, A.; Clerbaux, G.; Gillerot, G.; Pochet, J.-M.; Biller, P.; De Schuiteneer, M.; Morelle, J.; et al. Immunogenicity of BNT162b2 SARS-CoV-2 Vaccine in a Multicenter Cohort of Nursing Home Residents Receiving Maintenance Hemodialysis. Am. J. Kidney Dis. 2021, 78, 766–768. [Google Scholar] [CrossRef]
- Pilgram, L.; Eberwein, L.; Wille, K.; Koehler, F.C.; Stecher, M.; Rieg, S.; Kielstein, J.T.; Jakob, C.E.M.; Rüthrich, M.; Burst, V.; et al. Clinical course and predictive risk factors for fatal outcome of SARS-CoV-2 infection in patients with chronic kidney disease. Infection 2021, 49, 725–737. [Google Scholar] [CrossRef]
- Wilde, B.; Korth, J.; Jahn, M.; Kribben, A. COVID-19 vaccination in patients receiving dialysis. Nat. Rev. Nephrol. 2021, 17, 788–789. [Google Scholar] [CrossRef]
- Combe, C.; Kirsch, A.H.; Alfano, G.; Luyckx, V.A.; Shroff, R.; Kanbay, M.; van der Sande, F.; Basile, C. At least 156 reasons to prioritize COVID-19 vaccination in patients receiving in-centre haemodialysis. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 36, 571–574. [Google Scholar] [CrossRef]
- Kosmadakis, G.; Albaret, J.; Correia, E.D.C.; Somda, F.; Aguilera, D. Vaccination practices in dialysis patients: A narrative review. Semin. Dial. 2018, 31, 507–518. [Google Scholar] [CrossRef]
- Miskulin, D.C.; Weiner, D.E.; Tighiouart, H.; Lacson, E.K.J.; Meyer, K.B.; Dad, T.; Manley, H.J. High-Dose Seasonal Influenza Vaccine in Patients Undergoing Dialysis. Clin. J. Am. Soc. Nephrol. 2018, 13, 1703–1711. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Takkavatakarn, K.; Praditpornsilpa, K.; Nader, C.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Hepatitis B virus vaccine immune response and mortality in dialysis patients: A meta-analysis. J. Nephrol. 2020, 33, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Stein, G.E.; Bhupalam, S.; Havlichek, D.H. Immunogenicity of 13-Valent Conjugate Pneumococcal Vaccine in Patients 50 Years and Older with End-Stage Renal Disease and on Dialysis. Clin. Vaccine Immunol. 2016, 23, 884–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grupper, A.; Sharon, N.; Finn, T.; Cohen, R.; Israel, M.; Agbaria, A.; Rechavi, Y.; Schwartz, I.F.; Schwartz, D.; Lellouch, Y.; et al. Humoral Response to the Pfizer BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Jahn, M.; Korth, J.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Tyczynski, B.; Gäckler, A.; Witzke, O.; Dittmer, U.; Dolff, S.; et al. Humoral Response to SARS-CoV-2-Vaccination with BNT162b2 (Pfizer-BioNTech) in Patients on Hemodialysis. Vaccines 2021, 9, 360. [Google Scholar] [CrossRef] [PubMed]
- Speer, C.; Schaier, M.; Nusshag, C.; Töllner, M.; Buylaert, M.; Kälble, F.; Reichel, P.; Grenz, J.; Süsal, C.; Zeier, M.; et al. Longitudinal Humoral Responses after COVID-19 Vaccination in Peritoneal and Hemodialysis Patients over Twelve Weeks. Vaccines 2021, 9, 1130. [Google Scholar] [CrossRef] [PubMed]
- Zitt, E.; Davidovic, T.; Schimpf, J.; Abbassi-Nik, A.; Mutschlechner, B.; Ulmer, H.; Benda, M.A.; Sprenger-Mähr, H.; Winder, T.; Lhotta, K. The Safety and Immunogenicity of the mRNA-BNT162b2 SARS-CoV-2 Vaccine in Hemodialysis Patients. Front. Immunol. 2021, 12, 704773. [Google Scholar] [CrossRef]
- Paal, M.; Arend, F.M.; Lau, T.; Hasmann, S.; Soreth-Rieke, D.; Sorodoc-Otto, J.; Beuthien, W.; Krappe, J.; Toepfer, M.; von Gersdorff, G.; et al. Antibody response to mRNA SARS-CoV-2 vaccines in haemodialysis patients. Clin. Kidney J. 2021, 14, 2234–2238. [Google Scholar] [CrossRef]
- Chan, L.; Fuca, N.; Zeldis, E.; Campbell, K.N.; Shaikh, A. Antibody Response to mRNA-1273 SARS-CoV-2 Vaccine in Hemodialysis Patients with and without Prior COVID-19. Clin. J. Am. Soc. Nephrol. 2021, 16, 1258–1260. [Google Scholar] [CrossRef]
- Ducloux, D.; Colladant, M.; Chabannes, M.; Yannaraki, M.; Courivaud, C. Humoral response after 3 doses of the BNT162b2 mRNA COVID-19 vaccine in patients on hemodialysis. Kidney Int. 2021, 100, 702–704. [Google Scholar] [CrossRef]
- Dekervel, M.; Henry, N.; Torreggiani, M.; Pouteau, L.-M.; Imiela, J.-P.; Mellaza, C.; Garnier, A.-S.; Dujardin, A.; Asfar, M.; Ducancelle, A.; et al. Humoral response to a third injection of BNT162b2 vaccine in patients on maintenance haemodialysis. Clin. Kidney J. 2021, 14, 2349–2355. [Google Scholar] [CrossRef]
- Yanay, N.B.; Freiman, S.; Shapira, M.; Wishahi, S.; Hamze, M.; Elhaj, M.; Zaher, M.; Armaly, Z. Experience with SARS-CoV-2 BNT162b2 mRNA vaccine in dialysis patients. Kidney Int. 2021, 99, 1496–1498. [Google Scholar] [CrossRef] [PubMed]
- Tillmann, F.-P.; Figiel, L.; Ricken, J.; Still, H.; Korte, C.; Plassmann, G.; von Landenberg, P. Evolution of SARS-CoV-2-Neutralizing Antibodies after Two Standard Dose Vaccinations, Risk Factors for Non-Response and Effect of a Third Dose Booster Vaccination in Non-Responders on Hemodialysis: A Prospective Multi-Centre Cohort Study. J. Clin. Med. 2021, 10, 5113. [Google Scholar] [CrossRef] [PubMed]
- Yau, K.; Abe, K.T.; Naimark, D.; Oliver, M.J.; Perl, J.; Leis, J.A.; Bolotin, S.; Tran, V.; Mullin, S.I.; Shadowitz, E.; et al. Evaluation of the SARS-CoV-2 Antibody Response to the BNT162b2 Vaccine in Patients Undergoing Hemodialysis. JAMA Netw. Open 2021, 4, e2123622. [Google Scholar] [CrossRef] [PubMed]
- Espi, M.; Charmetant, X.; Barba, T.; Koppe, L.; Pelletier, C.; Kalbacher, E.; Chalencon, E.; Mathias, V.; Ovize, A.; Cart-Tanneur, E.; et al. The ROMANOV study found impaired humoral and cellular immune responses to SARS-CoV-2 mRNA vaccine in virus-unexposed patients receiving maintenance hemodialysis. Kidney Int. 2021, 100, 928–936. [Google Scholar] [CrossRef]
- Simon, B.; Rubey, H.; Treipl, A.; Gromann, M.; Hemedi, B.; Zehetmayer, S.; Kirsch, B. Haemodialysis patients show a highly diminished antibody response after COVID-19 mRNA vaccination compared with healthy controls. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 36, 1709–1716. [Google Scholar] [CrossRef]
- Strengert, M.; Becker, M.; Ramos, G.M.; Dulovic, A.; Gruber, J.; Juengling, J.; Lürken, K.; Beigel, A.; Wrenger, E.; Lonnemann, G.; et al. Cellular and humoral immunogenicity of a SARS-CoV-2 mRNA vaccine in patients on haemodialysis. EBioMedicine 2021, 70, 103524. [Google Scholar] [CrossRef]
- Hsu, C.M.; Weiner, D.E.; Aweh, G.N.; Manley, H.J.; Ladik, V.; Frament, J.; Miskulin, D.; Argyropoulos, C.; Abreo, K.; Chin, A.; et al. Seroresponse to SARS-CoV-2 Vaccines among Maintenance Dialysis Patients. Am. J. Kidney Dis. 2021, 79, 307–310. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Agur, T.; Ben-Dor, N.; Goldman, S.; Lichtenberg, S.; Herman-Edelstein, M.; Yahav, D.; Rozen-Zvi, B.; Zingerman, B. Antibody response to mRNA SARS-CoV-2 vaccine among dialysis patients—A prospectivecohort study. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 36, 1347–1349. [Google Scholar] [CrossRef]
- Broseta, J.J.; Rodríguez-Espinosa, D.; Rodríguez, N.; Mosquera, M.D.M.; Marcos, M.Á.; Egri, N.; Pascal, M.; Soruco, E.; Bedini, J.L.; Bayés, B.; et al. Humoral and Cellular Responses to mRNA-1273 and BNT162b2 SARS-CoV-2 Vaccines Administered to Hemodialysis Patients. Am. J. Kidney Dis. 2021, 78, 571–581. [Google Scholar] [CrossRef]
- Longlune, N.; Nogier, M.B.; Miedougé, M.; Gabilan, C.; Cartou, C.; Seigneuric, B.; Del Bello, A.; Marion, O.; Faguer, S.; Izopet, J.; et al. High immunogenicity of a messenger RNA-based vaccine against SARS-CoV-2 in chronic dialysis patients. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 36, 1704–1709. [Google Scholar] [CrossRef] [PubMed]
- Bensouna, I.; Caudwell, V.; Kubab, S.; Acquaviva, S.; Pardon, A.; Vittoz, N.; Bozman, D.-F.; Hanafi, L.; Faucon, A.-L.; Housset, P. SARS-CoV-2 Antibody Response After a Third Dose of the BNT162b2 Vaccine in Patients Receiving Maintenance Hemodialysis or Peritoneal Dialysis. Am. J. Kidney Dis. 2021, 79, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Danthu, C.; Hantz, S.; Dahlem, A.; Duval, M.; Ba, B.; Guibbert, M.; El Ouafi, Z.; Ponsard, S.; Berrahal, I.; Achard, J.-M.; et al. Humoral Response after SARS-CoV-2 mRNA Vaccination in a Cohort of Hemodialysis Patients and Kidney Transplant Recipients. J. Am. Soc. Nephrol. 2021, 32, 2153–2158. [Google Scholar] [CrossRef] [PubMed]
- Carr, E.J.; Wu, M.; Harvey, R.; Wall, E.C.; Kelly, G.; Hussain, S.; Howell, M.; Kassiotis, G.; Swanton, C.; Gandhi, S.; et al. Neutralising antibodies after COVID-19 vaccination in UK haemodialysis patients. Lancet 2021, 398, 1038–1041. [Google Scholar] [CrossRef]
- Galmiche, S.; Luong Nguyen, L.B.; Tartour, E.; de Lamballerie, X.; Wittkop, L.; Loubet, P.; Launay, O. Immunological and clinical efficacy of COVID-19 vaccines in immunocompromised populations: A systematic review. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2022, 28, 163–177. [Google Scholar] [CrossRef]
- Korth, J.; Jahn, M.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Eisenberger, U.; Gäckler, A.; Dittmer, U.; Witzke, O.; Wilde, B.; et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses 2021, 13, 756. [Google Scholar] [CrossRef]
- Rashidi-Alavijeh, J.; Frey, A.; Passenberg, M.; Korth, J.; Zmudzinski, J.; Anastasiou, O.E.; Saner, F.H.; Jahn, M.; Lange, C.M.; Willuweit, K. Humoral Response to SARS-CoV-2 Vaccination in Liver Transplant Recipients-A Single-Center Experience. Vaccines 2021, 9, 738. [Google Scholar] [CrossRef]
- Gandjour, A.; Armsen, W.; Wehmeyer, W.; Multmeier, J.; Tschulena, U. Costs of patients with chronic kidney disease in Germany. PLoS ONE 2020, 15, e0231375. [Google Scholar] [CrossRef]
- Collier, D.A.; Ferreira, I.A.T.M.; Kotagiri, P.; Datir, R.P.; Lim, E.Y.; Touizer, E.; Meng, B.; Abdullahi, A.; Elmer, A.; Kingston, N.; et al. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef]
- Collier, D.A.; De Marco, A.; Ferreira, I.A.T.M.; Meng, B.; Datir, R.P.; Walls, A.C.; Kemp, S.A.; Bassi, J.; Pinto, D.; Silacci-Fregni, C.; et al. Sensitivity of SARS-CoV-2 B.1.1.7 to mRNA vaccine-elicited antibodies. Nature 2021, 593, 136–141. [Google Scholar] [CrossRef]
- Madhi, S.A.; Baillie, V.; Cutland, C.L.; Voysey, M.; Koen, A.L.; Fairlie, L.; Padayachee, S.D.; Dheda, K.; Barnabas, S.L.; Bhorat, Q.E.; et al. Efficacy of the ChAdOx1 nCoV-19 COVID-19 Vaccine against the B.1.351 Variant. N. Engl. J. Med. 2021, 384, 1885–1898. [Google Scholar] [CrossRef] [PubMed]
- Volz, E.; Mishra, S.; Chand, M.; Barrett, J.C.; Johnson, R.; Geidelberg, L.; Hinsley, W.R.; Laydon, D.J.; Dabrera, G.; O’Toole, Á.; et al. Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England. Nature 2021, 593, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Schwarzkopf, S.; Krawczyk, A.; Knop, D.; Klump, H.; Heinold, A.; Heinemann, F.M.; Thümmler, L.; Temme, C.; Breyer, M.; Witzke, O.; et al. Cellular Immunity in COVID-19 Convalescents with PCR-Confirmed Infection but with Undetectable SARS-CoV-2-Specific IgG. Emerg. Infect. Dis. 2021, 27, 122. [Google Scholar] [CrossRef]
- Lindemann, M.; Lenz, V.; Knop, D.; Klump, H.; Alt, M.; Aufderhorst, U.W.; Schipper, L.; Schwarzkopf, S.; Meller, L.; Steckel, N.; et al. Convalescent plasma treatment of critically ill intensive care COVID-19 patients. Transfusion 2021, 61, 1394–1403. [Google Scholar] [CrossRef]
- Daugirdas, J.T. Second generation logarithmic estimates of single-pool variable volume Kt/V: An analysis of error. J. Am. Soc. Nephrol. 1993, 4, 1205–1213. [Google Scholar] [CrossRef]
- Burdick, R.A.; Bragg-Gresham, J.L.; Woods, J.D.; Hedderwick, S.A.; Kurokawa, K.; Combe, C.; Saito, A.; LaBrecque, J.; Port, F.K.; Young, E.W. Patterns of hepatitis B prevalence and seroconversion in hemodialysis units from three continents: The DOPPS. Kidney Int. 2003, 63, 2222–2229. [Google Scholar] [CrossRef] [Green Version]
- Clarke, C.L.; Prendecki, M.; Dhutia, A.; Gan, J.; Edwards, C.; Prout, V.; Lightstone, L.; Parker, E.; Marchesin, F.; Griffith, M.; et al. Longevity of SARS-CoV-2 immune responses in hemodialysis patients and protection against reinfection. Kidney Int. 2021, 99, 1470–1477. [Google Scholar] [CrossRef]
- Sakhi, H.; Dahmane, D.; Attias, P.; Kofman, T.; Bouvier, M.; Lapidus, N.; Fourati, S.; El Karoui, K. Kinetics of Anti-SARS-CoV-2 IgG Antibodies in Hemodialysis Patients Six Months after Infection. J. Am. Soc. Nephrol. 2021, 32, 1033–1036. [Google Scholar] [CrossRef]
- Ciabattini, A.; Pastore, G.; Fiorino, F.; Polvere, J.; Lucchesi, S.; Pettini, E.; Auddino, S.; Rancan, I.; Durante, M.; Miscia, M.; et al. Evidence of SARS-CoV-2-Specific Memory B Cells Six Months After Vaccination with the BNT162b2 mRNA Vaccine. Front. Immunol. 2021, 12, 740708. [Google Scholar] [CrossRef]
- Pegu, A.; O’Connell, S.E.; Schmidt, S.D.; O’Dell, S.; Talana, C.A.; Lai, L.; Albert, J.; Anderson, E.; Bennett, H.; Corbett, K.S.; et al. Durability of mRNA-1273 vaccine-induced antibodies against SARS-CoV-2 variants. Science 2021, 373, 1372–1377. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Frenck, R.W.J.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Karalis, V.; Ntanasis-Stathopoulos, I.; Gavriatopoulou, M.; Gumeni, S.; Malandrakis, P.; Papanagnou, E.-D.; Kastritis, E.; Trougakos, I.P.; Dimopoulos, M.A. Robust Neutralizing Antibody Responses 6 Months Post Vaccination with BNT162b2: A Prospective Study in 308 Healthy Individuals. Life 2021, 11, 1077. [Google Scholar] [CrossRef] [PubMed]
- Glöckner, S.; Hornung, F.; Baier, M.; Weis, S.; Pletz, M.W.; Deinhardt-Emmer, S.; Löffler, B.; Group, T.C.S. Robust Neutralizing Antibody Levels Detected after Either SARS-CoV-2 Vaccination or One Year after Infection. Viruses 2021, 13, 2003. [Google Scholar] [CrossRef]
- Tober-Lau, P.; Schwarz, T.; Vanshylla, K.; Hillus, D.; Gruell, H.; Suttorp, N.; Landgraf, I.; Kappert, K.; Seybold, J.; Drosten, C.; et al. Long-term immunogenicity of BNT162b2 vaccination in older people and younger health-care workers. Lancet. Respir. Med. 2021, 9, e104–e105. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Davidovic, T.; Schimpf, J.; Abbassi-Nik, A.; Stockinger, R.; Sprenger-Mähr, H.; Lhotta, K.; Zitt, E. Waning humoral response 6 months after SARS-CoV-2 vaccination with the mRNA-BNT162b2 vaccine in hemodialysis patients: Time for a boost. Kidney Int. 2021, 100, 1334–1335. [Google Scholar] [CrossRef]
- Stumpf, J.; Tonnus, W.; Paliege, A.; Rettig, R.; Steglich, A.; Gembardt, F.; Kessel, F.; Kröger, H.; Arndt, P.; Sradnick, J.; et al. Cellular and Humoral Immune Responses After 3 Doses of BNT162b2 mRNA SARS-CoV-2 Vaccine in Kidney Transplant. Transplantation 2021, 105, e267–e269. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Callaway, E. Omicron likely to weaken COVID vaccine protection. Nature 2021, 600, 367–368. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of immune dysfunction in end-stage renal disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1526–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaziri, N.D.; Pahl, M.V.; Crum, A.; Norris, K. Effect of uremia on structure and function of immune system. J. Ren. Nutr. 2012, 22, 149–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betjes, M.G.H. Immune cell dysfunction and inflammation in end-stage renal disease. Nat. Rev. Nephrol. 2013, 9, 255–265. [Google Scholar] [CrossRef]
- Cohen, G. Immune Dysfunction in Uremia 2020. Toxins 2020, 12, 439. [Google Scholar] [CrossRef]
- Jofré, R.; Rodriguez-Benitez, P.; López-Gómez, J.M.; Pérez-Garcia, R. Inflammatory syndrome in patients on hemodialysis. J. Am. Soc. Nephrol. 2006, 17, S274–S280. [Google Scholar] [CrossRef]
- Fernández, E.; Betriu, M.A.; Gómez, R.; Montoliu, J. Response to the hepatitis B virus vaccine in haemodialysis patients: Influence of malnutrition and its importance as a risk factor for morbidity and mortality. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 1996, 11, 1559–1563. [Google Scholar]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Krueger, K.M.; Ison, M.G.; Ghossein, C. Practical Guide to Vaccination in All Stages of CKD, Including Patients Treated by Dialysis or Kidney Transplantation. Am. J. Kidney Dis. 2020, 75, 417–425. [Google Scholar] [CrossRef]
- Espi, M.; Charmetant, X.; Barba, T.; Mathieu, C.; Pelletier, C.; Koppe, L.; Chalencon, E.; Kalbacher, E.; Mathias, V.; Ovize, A.; et al. A prospective observational study for justification, safety, and efficacy of a third dose of mRNA vaccine in patients receiving maintenance hemodialysis. Kidney Int. 2021, 101, 390–402. [Google Scholar] [CrossRef] [PubMed]
- Batty, C.J.; Heise, M.T.; Bachelder, E.M.; Ainslie, K.M. Vaccine formulations in clinical development for the prevention of severe acute respiratory syndrome coronavirus 2 infection. Adv. Drug Deliv. Rev. 2021, 169, 168–189. [Google Scholar] [CrossRef] [PubMed]
- Nance, K.D.; Meier, J.L. Modifications in an Emergency: The Role of N1-Methylpseudouridine in COVID-19 Vaccines. ACS Cent. Sci. 2021, 7, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Dolff, S.; Zhou, B.; Korth, J.; Luo, D.; Dai, Y.; Jahn, M.; Dorsch, O.; Anastasiou, O.E.; Witzke, O.; Kribben, A.; et al. Evidence of cell-mediated immune response in kidney transplants with a negative mRNA vaccine antibody response. Kidney Int. 2021, 100, 479–480. [Google Scholar] [CrossRef] [PubMed]
- McMahan, K.; Yu, J.; Mercado, N.B.; Loos, C.; Tostanoski, L.H.; Chandrashekar, A.; Liu, J.; Peter, L.; Atyeo, C.; Zhu, A.; et al. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature 2021, 590, 630–634. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | All | Non-Responder | Insufficient Responder | Responder | Subgroup Comparison | Correlation with Anti -SARS-CoV-2 IgG 24 Weeks after 1st Vac |
|---|---|---|---|---|---|---|
| MD [Q1;Q3], (Range: Min–Max) or n (% of Subgroup) | ||||||
| Patients | 59 | 12 | 28 | 19 | NA | NA |
| SARS-CoV-2 IgG against the nucleocapsid protein, S/CO ratio | ||||||
| 24 weeks after 1st vac | 0.05 [0.03; 0.10], | 0.07 [0.04; 0.11], | 0.05 [0.04; 0.15], | 0.04 [0.04; 0.06], | p = 0.463 * | −0.175; p = 0.194 † |
| (0.02–0.47) | (0.02–0.17) | (0.02–0.47) | (0.03–0.23) | |||
| SARS-CoV-2 IgG against the spike protein, BAU/mL | ||||||
| before 1st vac | 5 [5; 5], | 5 [5; 5], | 5 [5; 5], | 5 [5; 5], | p = 0.844 * | 0.089; p = 0.506 † |
| (5–22) | (5–6) | (5–12.5) | (5–22) | |||
| 6 weeks after 1st vac | 918 [322; 1505], | 172 [58; 586], | 823 [364; 1127], | 1794 [1222; 2080], | p < 0.001 * | 0.669; p < 0.001 † |
| (5–2080) | (5–871) | (132–1672) | (117–2080) | |||
| 12 weeks after 1st vac | 298 [111; 605], | 44 [5; 85], | 265 [175; 414], | 723 [497; 1275], | p < 0.001 * | 0.918; p < 0.001 † |
| (5–2080) | (5–132) | (54–1040) | (130–2080) | |||
| 24 weeks after 1st vac | 89 [38; 224], | 13 [5; 23], | 78 [57; 172], | 292 [183; 482], | p < 0.001 * | NA |
| (5–1150) | (5–30) | (34–362) | (82–1150) | |||
| Variable | All | Non-Responder | Insufficient Responder | Responder | Subgroup Comparison | Correlation with Anti -SARS-CoV-2 IgG 24 Weeks after 1st Vac |
|---|---|---|---|---|---|---|
| MD [Q1;Q3], (Range: Min–Max) or n (% of Subgroup) | ||||||
| Patients | 59 | 12 | 28 | 19 | NA | NA |
| Gender, n (%) | ♀ 22 (37.3%) | ♀ 6 (50.0%) | ♀ 7 (25.0%) | ♀ 9 (47.4%) | p = 0.156 ° | 0.112, p = 0.401 ‡ |
| ♂ 37 (62.7%) | ♂ 6 (50.0%) | ♂ 21 (75.0%) | ♂ 10 (52.6%) | |||
| Age, years | 68 [59; 77], | 76 [66; 78], | 68 [57; 76], | 62 [54; 70], | p = 0.034 * | −0.411; p < 0.001 † |
| (50–90) | (63–85) | (53–83) | (50–90) | |||
| Body Mass Index, kg/m² | 27.1 [22.4; 30.3], | 27.6 [23.5; 30.3], | 26.8 [21.5; 29.9], | 27.0 [23.5; 31.6], | p = 0.819 * | 0.037; p = 0.786 † |
| (17.9–46.3) | (19.0–36.7) | (18.4–42.8) | (17.9–46.3) | |||
| Dialysis vintage, years | 4 [2; 12], | 4 [1; 10], | 4 [2; 9], | 4 [1; 26], | p = 0.892 * | 0.118; p = 0.376 † |
| (0–46) | (0–46) | (0–31) | (0–38) | |||
| HepB- vac responders | 16 (27.1 %) | 2 (16.7 %) | 6 (21.4 %) | 8 (42.1 %) | p = 0.239 ° | 0.268; p = 0.042 † |
| Diabetes mellitus | 29 (49.2 %) | 7 (58.3 %) | 13 (46.4 %) | 9 (47.4 %) | p = 0.838 ° | −0.256; p = 0.053 † |
| C-reactive Protein, mg/dL | 3.4 [1.8; 9.4], | 4.9 [2.4; 22.6], | 4.5 [2.0; 10.7], | 2.3 [0.9; 4.5], | p = 0.036 * | −0.319; p = 0.015 † |
| (<0.4–60.7) | (2.2–22.6) | (0.6–60.7) | (<0.4–11.2) | |||
| Leukocytes, e3/µL | 6.7 [5.6; 8.0], | 6.8 [5.7; 9.4], | 6.8 [5.4; 8.1], | 6.6 [5.8; 7.8], | p = 0.729 * | −0.081; p = 0.544 † |
| (1.6–11.7) | (5.3–11.7) | (1.6–11.0) | (4.3–10.7) | |||
| Vitamin D, ng/mL | 23.4 [16.2; 32.0], | 15.2 [11.0; 22.6], | 24.3 [16.5; 30.5], | 27.0 [20.8; 35.0], | p = 0.015 * | 0.361; p = 0.006 † |
| (9.4–45.7) | (9.4–37.9) | (9.6–45.7) | (15.4–45.3) | |||
| Serum albumin, g/dL | 3.9 [3.8; 4.2], | 3.7 [3.1; 3.9], | 3.9 [3.8; 4.2] | 4.2 [3.9; 4.3], | p = 0.007 * | 0.466; p < 0.001 † |
| (2.6–4.5) | (2.6–4.3) | (3.5–4.4) | (3.6–4.5) | |||
| Kt/V | 1.47 [1.22; 1.70], | 1.45 [1.13; 1.67], | 1.45 [1.19; 1.66], | 1.58 [1.24; 1.92], | p = 0.564 * | 0.168; p = 0.207 † |
| (0.91–2.19) | (0.99–1.81) | (0.91–2.05) | (0.94–2.19) | |||
| Parathormone, pmol/L | 19.3 [11.5; 30.3], | 22.5 [14.2; 32.2], | 18.8 [14.0; 30.2], | 14.8 [8.2; 27.3], | p = 0.706 * | −0.121; p = 0.367 † |
| (1.1–59.7) | (3.4–42.6) | (4.7–46.2) | (1.1–59.7) | |||
| Hemoglobin, g/dL | 11.5 [10.8; 12.6], | 10.9 [10.4; 11.9], | 11.3 [11.0; 12.2], | 12.1 [11.2; 12.7], | p = 0.104 * | 0.219; p = 0.098 † |
| (9.2–13.9) | (10.0–13.9) | (9.2–13.7) | (10.5–13.3) | |||
| Variable | Absence of SARS-CoV-2 IgG 24 Weeks after 1st Vac | Absence of Neutralizing Antibodies 24 Weeks after 1st Vac |
|---|---|---|
| Adjusted Odds Ratio (95% CI); Significance | Adjusted Odds Ratio (95% CI); Significance | |
| SARS-CoV-2 IgG, 6 weeks after 1st vac per 1 BAU/mL | 1.002 (0.996–1.008); p = 0.540 | 0.998 (0.997–1.000); p = 0.120 |
| SARS-CoV-2 IgG, 12 weeks after 1st vac per 1 BAU/mL | 0.955 (0.913–0.998); p = 0.039 | 0.996 (0.993–1.000); p = 0.037 |
| Variable | No SARS-CoV-2 IgG 24 Weeks after 1st Vac | No Neutralizing Antibodies 24 Weeks after 1st Vac |
|---|---|---|
| Adjusted Odds Ratio (95% CI); Significance | Adjusted Odds Ratio (95% CI); Significance | |
| Age per 1 year | 1.056 (0.962–1.160); p = 0.249 | 1.026 (0.960–1.096); p = 0.450 |
| CRP per 1 mg/dL | 1.017 (0.952–1.087); p = 0.617 | 1.127 (0.948–1.341); p = 0.176 |
| Serum albumin per 0,1 g/dL | 0.965 (0.937–0.994); p = 0.017 | 0.988 (0.963–1.014); p = 0.356 |
| Vitamin D per 1 ng/mL | 0.912 (0.816–1.019); p = 0.105 | 0.963 (0.893–1.039); p = 0.334 |
| Positive hepatitis B vac response | 0.514 (0.061–4.338); p = 0.541 | 0.263 (0.057–1.201); p = 0.085 |
| Hemoglobin per 1 g/L | 1.217 (0.513–2.888); p = 0.656 | 0.732 (0.364–1.471); p = 0.381 |
| Diabetes mellitus | 1.517 (0.280–8.207); p = 0.629 | 0.467 (0.107–2.034); p = 0.311 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jahn, M.; Korth, J.; Dorsch, O.; Anastasiou, O.E.; Krawczyk, A.; Brochhagen, L.; van de Sand, L.; Sorge-Hädicke, B.; Tyczynski, B.; Witzke, O.; et al. Decline of Humoral Responses 6 Months after Vaccination with BNT162b2 (Pfizer–BioNTech) in Patients on Hemodialysis. Vaccines 2022, 10, 327. https://doi.org/10.3390/vaccines10020327
Jahn M, Korth J, Dorsch O, Anastasiou OE, Krawczyk A, Brochhagen L, van de Sand L, Sorge-Hädicke B, Tyczynski B, Witzke O, et al. Decline of Humoral Responses 6 Months after Vaccination with BNT162b2 (Pfizer–BioNTech) in Patients on Hemodialysis. Vaccines. 2022; 10(2):327. https://doi.org/10.3390/vaccines10020327
Chicago/Turabian StyleJahn, Michael, Johannes Korth, Oliver Dorsch, Olympia Evdoxia Anastasiou, Adalbert Krawczyk, Leonie Brochhagen, Lukas van de Sand, Burkhard Sorge-Hädicke, Bartosz Tyczynski, Oliver Witzke, and et al. 2022. "Decline of Humoral Responses 6 Months after Vaccination with BNT162b2 (Pfizer–BioNTech) in Patients on Hemodialysis" Vaccines 10, no. 2: 327. https://doi.org/10.3390/vaccines10020327
APA StyleJahn, M., Korth, J., Dorsch, O., Anastasiou, O. E., Krawczyk, A., Brochhagen, L., van de Sand, L., Sorge-Hädicke, B., Tyczynski, B., Witzke, O., Dittmer, U., Dolff, S., Wilde, B., & Kribben, A. (2022). Decline of Humoral Responses 6 Months after Vaccination with BNT162b2 (Pfizer–BioNTech) in Patients on Hemodialysis. Vaccines, 10(2), 327. https://doi.org/10.3390/vaccines10020327