
The Effect of Smoking on Humoral Response to COVID-19 Vaccines: A Systematic Review of Epidemiological Studies





Abstract
:1. Introduction
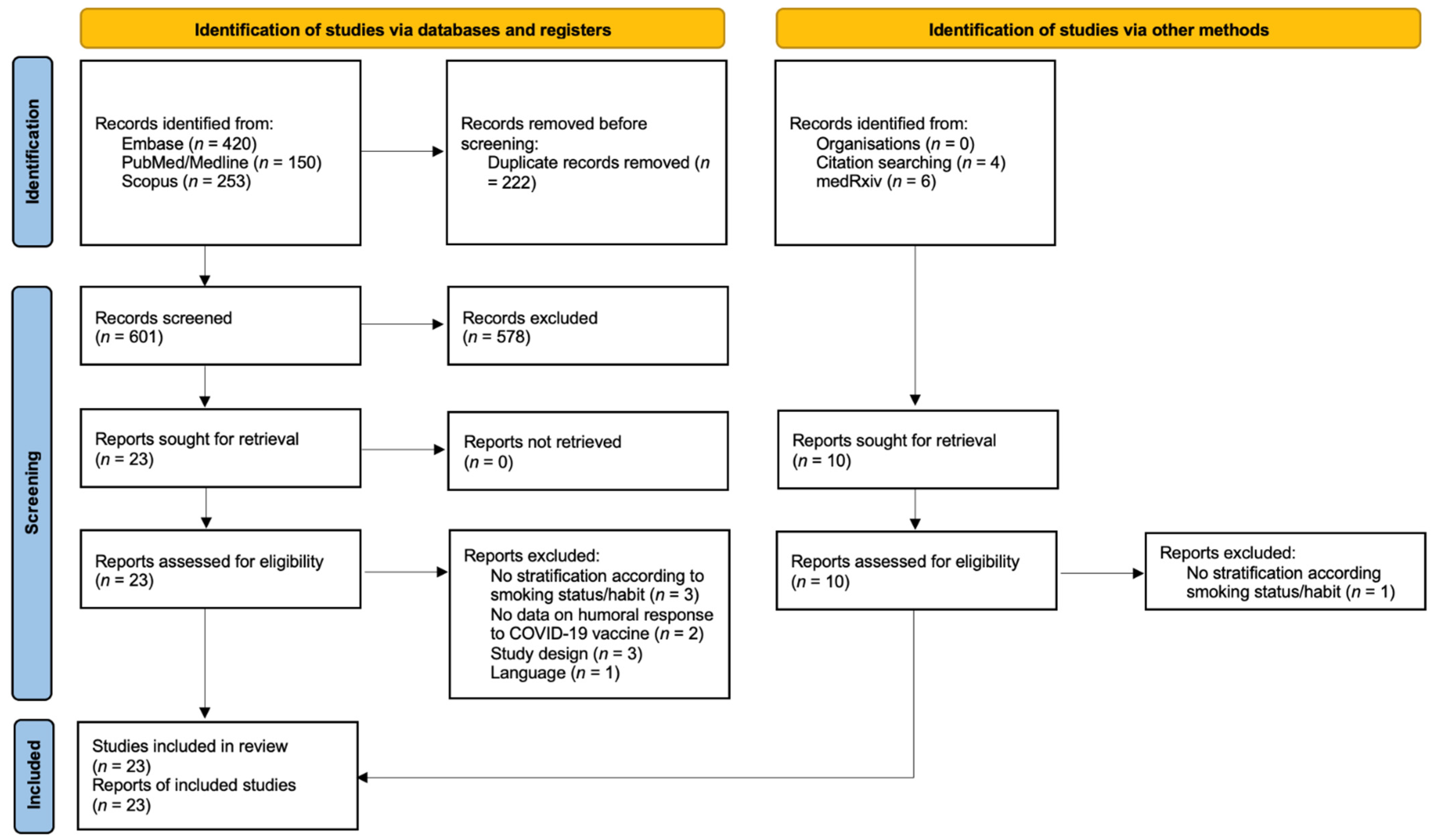
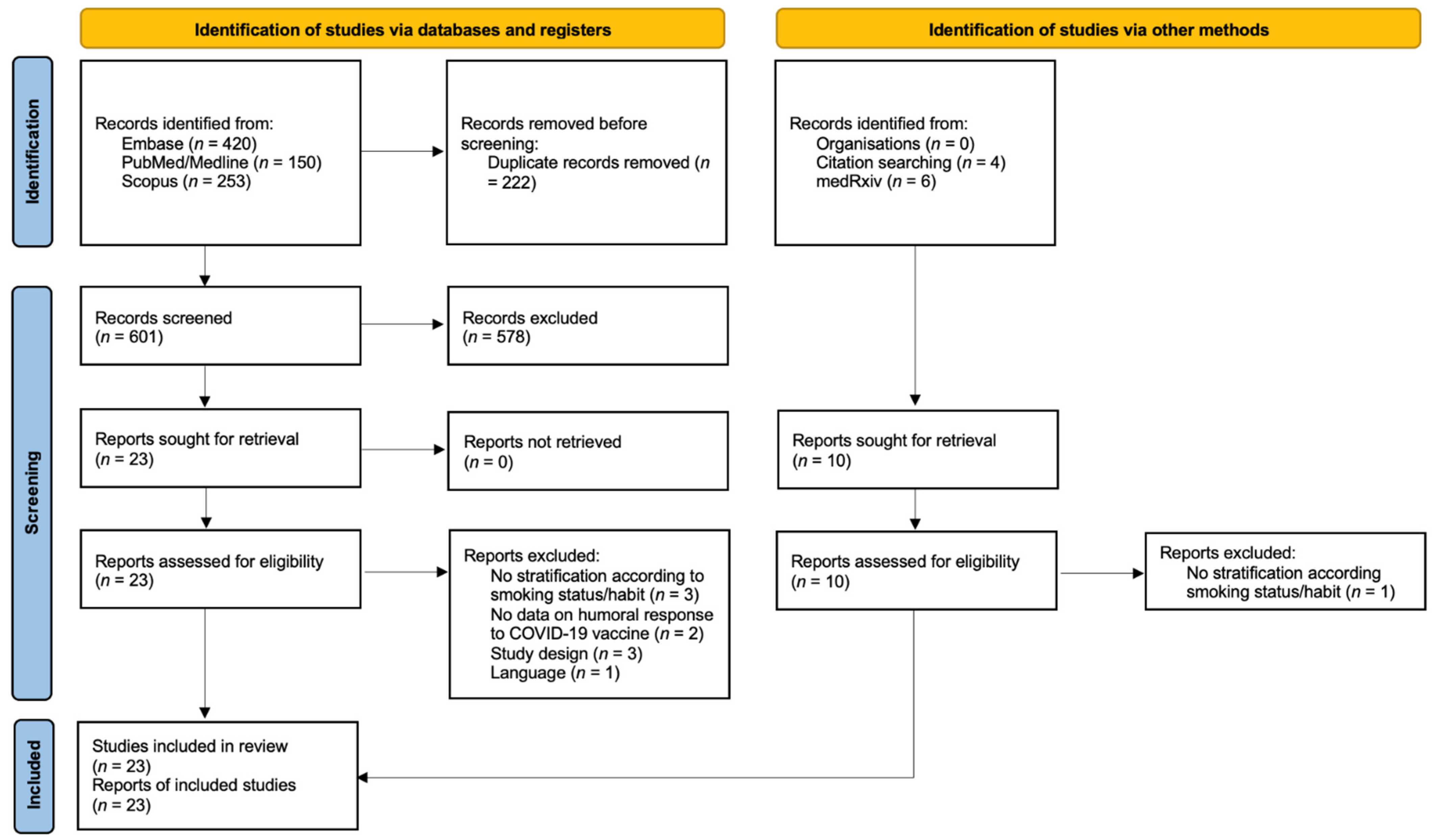
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Tobacco. Newsroom. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 2 February 2022).
- Institute for Health Metrics and Evaluation Findings from the Global Burden of Disease Study 2017. Institute for Health Metrics and Evaluation. 2018. Available online: http://www.healthdata.org/sites/default/files/files/policy_report/2019/GBD_2017_Booklet.pdf (accessed on 27 January 2022).
- Reitsma, M.B.; Kendrick, P.J.; Ababneh, E.; Abbafati, C.; Abbasi-Kangevari, M.; Abdoli, A.; Abedi, A.; Abhilash, E.S.; Abila, D.B.; Aboyans, V.; et al. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. The Health Consequences of Smoking: 50 Years of Progress: A Report of the Surgeon General; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; US Department of Health and Human Services: Atlanta, GA, USA, 2014.
- Edwards, D. Immunological effects of tobacco smoking in “healthy” smokers. COPD 2009, 6, 48–58. [Google Scholar] [CrossRef]
- Qiu, F.; Fan, P.; Nie, G.D.; Liu, H.; Liang, C.-L.; Yu, W.; Dai, Z. Effects of Cigarette Smoking on Transplant Survival: Extending or Shortening It? Front. Immunol. 2017, 8, 127. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Yang, S.M.; Kim, S.H.; Han, K.H.; Park, S.J.; Shin, J.I. Smoking and Rheumatoid Arthritis. Int. J. Mol. Sci. 2014, 15, 22279–22295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saulyte, J.; Regueira, C.; Montes-Martínez, A.; Khudyakov, P.; Takkouche, B. Active or passive exposure to tobacco smoking and allergic rhinitis, allergic dermatitis, and food allergy in adults and children: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001611. [Google Scholar] [CrossRef] [Green Version]
- Winter, A.P.; Follett, E.A.; McIntyre, J.; Stewart, J.; Symington, I.S. Influence of smoking on immunological responses to hepatitis B vaccine. Vaccine 1994, 12, 771–772. [Google Scholar] [CrossRef]
- Petráš, M.; Oleár, V.; Molitorisová, M.; Dáňová, J.; Čelko, A.M.; Nováková, E.; Štefkovičová, M.; Krištúfková, Z.; Malinová, J.; Lesná, I.K. Factors Influencing Persistence of Diphtheria Immunity and Immune Response to a Booster Dose in Healthy Slovak Adults. Vaccines 2019, 7, 139. [Google Scholar] [CrossRef] [Green Version]
- Petráš, M.; Oleár, V. Predictors of the immune response to booster immunisation against tetanus in Czech healthy adults. Epidemiol. Infect. 2018, 146, 2079–2085. [Google Scholar] [CrossRef] [Green Version]
- Namujju, P.B.; Pajunen, E.; Simen-Kapeu, A.; Hedman, L.; Merikukka, M.; Surcel, H.M.; Kirnbauer, R.; Apter, D.; Paavonen, J.; Hedman, K.; et al. Impact of smoking on the quantity and quality of antibodies induced by human papillomavirus type 16 and 18 AS04-adjuvanted virus-like-particle vaccine—A pilot study. BMC Res. Notes 2014, 7, 445. [Google Scholar] [CrossRef] [Green Version]
- Nath, K.D.; Burel, J.G.; Shankar, V.; Pritchard, A.L.; Towers, M.; Looke, D.; Davies, J.M.; Upham, J.W. Clinical factors associated with the humoral immune response to influenza vaccination in chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Signorelli, C.; Odone, A.; Gianfredi, V.; Bossi, E.; Bucci, D.; Oradini-Alacreu, A.; Frascella, B.; Capraro, M.; Chiappa, F.; Blandi, L.; et al. COVID-19 mortality rate in nine high-income metropolitan regions. Acta Biomed. 2020, 91, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Balasco, N.; d’Alessandro, V.; Ferrara, P.; Smaldone, G.; Vitagliano, L. Analysis of the time evolution of COVID-19 lethality during the first epidemic wave in Italy. Acta Biomed. 2021, 92, e2021171. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, D.; Madotto, F.; Conti, S.; Antonazzo, I.C.; Vitale, A.; Della Ragione, G.; Romano, M.L.; Borrelli, M.; Schiavone, B.; Polosa, R.; et al. Response to BNT162b2 mRNA COVID-19 vaccine among healthcare workers in Italy: A 3-month follow-up. Intern. Emerg. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.; Antonazzo, I.C.; Polosa, R. Response to BNT162b2 mRNA COVID-19 vaccine among healthcare workers in Italy: A 3-month follow-up—Reply. Intern. Emerg. Med. 2022, 17, 313–314. [Google Scholar] [CrossRef]
- Ponticelli, D.; Antonazzo, I.C.; Caci, G.; Vitale, A.; Della Ragione, G.; Romano, M.L.; Borrelli, M.; Schiavone, B.; Polosa, R.; Ferrara, P. Dynamics of antibody response to BNT162b2 mRNA COVID-19 vaccine after 6 months. J. Travel Med. 2021, 28, taab173. [Google Scholar] [CrossRef]
- Tsatsakis, A.; Vakonaki, E.; Tzatzarakis, M.; Flamourakis, M.; Nikolouzakis, T.K.; Poulas, K.; Papazoglou, G.; Hatzidaki, E.; Papanikolaou, N.C.; Drakoulis, N.; et al. Immune response (IgG) following full inoculation with BNT162b2 COVID-19 mRNA among healthcare professionals. Int. J. Mol. Med. 2021, 48, 200. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.; Ponticelli, D.; Agüero, F.; Caci, G.; Vitale, A.; Borrelli, M.; Schiavone, B.; Antonazzo, I.; Mantovani, L.; Tomaselli, V.; et al. Does smoking have an impact on the immunological response to COVID-19 vaccines? Evidence from VASCO study and need for further studies. Public Health 2022, 203, 97–99. [Google Scholar] [CrossRef]
- Tricco, A.C.; Langlois, E.V.; Straus, S.E. Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Gianfredi, V.; Mauer, N.S.; Gentile, L.; Riccò, M.; Odone, A.; Signorelli, C. COVID-19 and Recreational Skiing: Results of a Rapid Systematic Review and Possible Preventive Measures. Int. J. Environ. Res. Public Health 2021, 18, 4349. [Google Scholar] [CrossRef]
- Balshema, H.; Helfanda, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Gümüş, H.H.; Ödemiş, I.; Alışka, H.E.; Karslı, A.; Kara, S.; Özkale, M.; Gül, E. Side effects and antibody response of an inactive severe acute respiratory syndrome coronavirus 2 vaccine among health care workers. Rev. Assoc. Med. Bras. 2021, 67, 1825–1831. [Google Scholar] [CrossRef] [PubMed]
- Ikezaki, H.; Nakashima, R.; Miyoshi, K.; Hara, Y.; Hayashi, J.; Hara, H.; Nomura, H.; Shimono, N. Dynamics of anti-Spike IgG antibody level after full BNT162b2 COVID-19 vaccination in health care workers. medRxiv 2021. [Google Scholar] [CrossRef]
- Zhang, J.; Teng, F.; Zhang, X.; Wang, H.; Liang, T.; Guo, S.B. Down-regulation of SARS-CoV-2 neutralizing antibodies in vaccinated smokers. medRxiv 2021. [Google Scholar] [CrossRef]
- Pitzalis, M.; Idda, M.L.; Lodde, V.; Loizedda, A.; Lobina, M.; Zoledziewska, M.; Virdis, F.; Delogu, G.; Pirinu, F.; Marini, M.G.; et al. Effect of Different Disease-Modifying Therapies on Humoral Response to BNT162b2 Vaccine in Sardinian Multiple Sclerosis Patients. Front. Immunol. 2021, 12, 781843. [Google Scholar] [CrossRef]
- Herzberg, J.; Vollmer, T.; Fischer, B.; Becher, H.; Becker, A.-K.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. SARS-CoV-2-antibody response in health care workers after vaccination or natural infection in a longitudinal observational study. Vaccine 2021, 40, 206–212. [Google Scholar] [CrossRef]
- Malavazos, A.E.; Basilico, S.; Iacobellis, G.; Milani, V.; Cardani, R.; Boniardi, F.; Dubini, C.; Prandoni, I.; Capitanio, G.; Renna, L.V.; et al. Antibody responses to BNT162b2 mRNA vaccine: Infection-naïve individuals with abdominal obesity warrant attention. Obesity 2021. [Google Scholar] [CrossRef]
- Yamamoto, S.; Tanaka, A.; Ohmagari, N.; Yamaguchi, K.; Ishitsuka, K.; Morisaki, N.; Kojima, M.; Nishikimi, A.; Tokuda, H.; Inoue, M.; et al. Use of heat-not-burn tobacco products, moderate alcohol drinking, and anti-SARS-CoV-2 IgG antibody titers after BNT162b2 vaccination among Japanese healthcare workers. medRxiv 2021. [Google Scholar] [CrossRef]
- Kato, H.; Miyakawa, K.; Ohtake, N.; Go, H.; Yamaoka, Y.; Yajima, S.; Shimada, T.; Goto, A.; Nakajima, H.; Ryo, A. Antibody titers against the Alpha, Beta, Gamma, and Delta variants of SARS-CoV-2 induced by BNT162b2 vaccination measured using automated chemiluminescent enzyme immunoassay. J. Infect. Chemother. 2021, 28, 273–278. [Google Scholar] [CrossRef]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; Sugiyama, K. Attenuation of antibody titres during 3-6 months after the second dose of the BNT162b2 vaccine depends on sex, with age and smoking as risk factors for lower antibody titres at 6 months. Vaccines 2021, 9, 1500. [Google Scholar] [CrossRef]
- Kato, H.; Miyakawa, K.; Ohtake, N.; Yamaoka, Y.; Yajima, S.; Yamazaki, E.; Shimada, T.; Goto, A.; Nakajima, H.; Ryo, A. Vaccine-induced humoral and cellular immunity against SARS-CoV-2 at 6 months post BNT162b2 vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Uysal, E.B.; Gümüş, S.; Bektöre, B.; Bozkurt, H.; Gözalan, A. Evaluation of antibody response after COVID-19 vaccination of healthcare workers. J. Med. Virol. 2021, 94, 1060–1066. [Google Scholar] [CrossRef] [PubMed]
- Alqassieh, R.; Suleiman, A.; Abu-Halaweh, S.; Santarisi, A.; Shatnawi, O.; Shdaifat, L.; Tarifi, A.; Al-Tamimi, M.; Al-Shudifat, A.-E.; Alsmadi, H.; et al. Pfizer-BioNTech and Sinopharm: A Comparative Study on Post-Vaccination Antibody Titers. Vaccines 2021, 9, 1223. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Kurihara, M.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; et al. Age and Smoking Predict Antibody Titres at 3 Months after the Second Dose of the BNT162b2 COVID-19 Vaccine. Vaccines 2021, 9, 1042. [Google Scholar] [CrossRef] [PubMed]
- Linardou, H.; Spanakis, N.; Koliou, G.-A.; Christopoulou, A.; Karageorgopoulou, S.; Alevra, N.; Vagionas, A.; Tsoukalas, N.; Sgourou, S.; Fountzilas, E.; et al. Responses to SARS-CoV-2 Vaccination in Patients with Cancer (ReCOVer Study): A Prospective Cohort Study of the Hellenic Cooperative Oncology Group. Cancers 2021, 13, 4621. [Google Scholar] [CrossRef]
- Moncunill, G.; Aguilar, R.; Ribes, M.; Ortega, N.; Rubio, R.; Salmeron, G.; Molina, M.J.; Vidal, M.; Barrios, D.; Mitchell, R.A.; et al. Determinants of early antibody responses to COVID-19 mRNA vaccines in exposed and naive healthcare workers. medRxiv 2021. [Google Scholar] [CrossRef]
- Parthymou, A.; Habeos, E.E.; Habeos, G.I.; Deligakis, A.; Livieratos, E.; Marangos, M.; Chartoumpekis, D.V. SARS-CoV-2 antibody titer 3 months post-vaccination is affected by age, gender, smoking and vitamin D. medRxiv 2021. [Google Scholar] [CrossRef]
- Michos, A.; Tatsi, E.; Filippatos, F.; Dellis, C.; Koukou, D.; Efthymiou, V.; Kastrinelli, E.; Mantzou, A.; Syriopoulou, V. Association of total and neutralizing SARS-CoV-2 spike -receptor binding domain antibodies with epidemiological and clinical characteristics after immunization with the 1st and 2nd doses of the BNT162b2 vaccine. Vaccine 2021, 39, 5963–5967. [Google Scholar] [CrossRef]
- Lombardi, A.; Consonni, D.; Oggioni, M.; Bono, P.; Renteria, S.U.; Piatti, A.; Pesatori, A.C.; Castaldi, S.; Muscatello, A.; Riboldi, L.; et al. SARS-CoV-2 anti-spike antibody titres after vaccination with BNT162b2 in naïve and previously infected individuals. J. Infect. Public Health 2021, 14, 1120–1122. [Google Scholar] [CrossRef]
- Modenese, A.; Paduano, S.; Bargellini, A.; Bellucci, R.; Marchetti, S.; Bruno, F.; Grazioli, P.; Vivoli, R.; Gobba, F. Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart. Vaccines 2021, 9, 652. [Google Scholar] [CrossRef]
- Watanabe, M.; Balena, A.; Tuccinardi, D.; Tozzi, R.; Risi, R.; Masi, D.; Caputi, A.; Rossetti, R.; Spoltore, M.E.; Filippi, V.; et al. Central obesity, smoking habit, and hypertension are associated with lower antibody titres in response to COVID-19 mRNA vaccine. Diabetes/Metab. Res. Rev. 2021, 38, e3465. [Google Scholar] [CrossRef]
- Kennedy, N.A.; Simeng Lin, S.; Goodhand, J.R.; Chanchlani, N.; Hamilton, B.; Bewshea, C.; Nice, R.; Chee, D.; Cummings, J.F.; Fraser, A.; et al. Infliximab is associated with attenuated immunogenicity to BNT162b2 and ChAdOx1 nCoV-19 SARS-CoV-2 vaccines in patients with IBD. Gut 2021, 70, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.M.; Çolak, Y.; Ellervik, C.; Hasselbalch, H.C.; Bojesen, S.E.; Nordestgaard, B.G. Smoking and Increased White and Red Blood Cells. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 965–977. [Google Scholar] [CrossRef] [PubMed]
- Qiu, F.; Liang, C.; Liu, H.; Zeng, Y.Q.; Hou, S.; Huang, S.; Lai, X.; Dai, Z. Impacts of cigarette smoking on immune responsiveness: Up and down or upside down? Oncotarget 2017, 8, 268–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sopori, M.L. Effects of cigarette smoke on the immune system. Nat. Rev. Immunol. 2002, 2, 372–377. [Google Scholar] [CrossRef]
- Hernandez, C.P.; Morrow, K.; Velasco, C.; Wyczechowska, D.D.; Naura, A.S.; Rodriguez, P.C. Effects of ciga-rette smoke extract on primary activated T cells. Cell Immunol. 2013, 282, 38–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piaggeschi, G.; Rolla, S.; Rossi, N.; Brusa, D.; Naccarati, A.; Couvreur, S.; Spector, T.D.; Roederer, M.; Mangino, M.; Cordero, F.; et al. Immune Trait Shifts in Associa-tion with Tobacco Smoking: A Study in Healthy Women. Front. Immunol. 2021, 12, 637974. [Google Scholar] [CrossRef] [PubMed]
- Bekki, K.; Inaba, Y.; Uchiyama, S.; Kunugita, N. Comparison of Chemicals in Mainstream Smoke in Heat-not-burn Tobacco and Combustion Cigarettes. J. UOEH 2017, 39, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Simonavicius, E.; McNeill, A.; Shahab, L.; Brose, L.S. Heat-not-burn tobacco products: A systematic literature review. Tob. Control. 2019, 28, 582–594. [Google Scholar] [CrossRef]
- Younas, M.; Carrat, F.; Desaint, C.; Launay, O.; Corbeau, P. Immune activation, smoking, and vaccine response. Aids 2017, 31, 171–173. [Google Scholar] [CrossRef]
- Jackson, S.E.; Paul, E.; Brown, J.; Steptoe, A.; Fancourt, D. Negative Vaccine Attitudes and Intentions to Vaccinate Against COVID-19 in Relation to Smoking Status: A Population Survey of UK Adults. Nicotine Tob. Res. 2021, 23, 1623–1628. [Google Scholar] [CrossRef]
- Polosa, R.; Tomaselli, V.; Ferrara, P.; Romeo, A.C.; Rust, S.; Saitta, D.; Caraci, F.; Romano, C.; Thangaraju, M.; Zuccarello, P.; et al. Seroepidemiological Survey on the Impact of Smoking on SARS-CoV-2 Infection and COVID-19 Outcomes: Protocol for the Troina Study. JMIR Res. Protoc. 2021, 10, e32285. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Pennisi, F.; Lume, A.; Ricciardi, G.E.; Minerva, M.; Riccò, M.; Odone, A.; Signorelli, C. Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature. Vaccines 2021, 9, 574. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author (and Year) | Country | Population Type and Numerosity | Male (%) | Mean or Median Age | Smokers (%) | COVID-19 Vaccine | Median Time Since Vaccination (in Days) | Serologic Test | Main Findings |
|---|---|---|---|---|---|---|---|---|---|
| Ferrara (2022) [20] | Italy | Healthcare workers, 162 | 42.0 | 42.5 | 34.8 | BNT162b2 | 60 | CLIA with reactivity cutoff equal to or greater than 1.0 AU/mL. Sensitivity of 100% (95%CI: 99.9–100) and specificity of 99.6% (95%CI: 98.7–100). | In the study of the dynamics of antibody response to COVID-19 vaccine after 6 months, at the 60-day serology, a difference in vaccine-induced IgG titre was seen, with median antibody titres of, respectively, 211.80 (IQR 149.80–465.50) and 487.50 (IQR 308.45–791.65) AU/mL (p-value = 0.002). In the multivariate regression model, the β coefficient was equal to −335.62 (95%CI: −557.41–−113.83; p = 0.004) for active smoking. No other differences were seen in other sample timings (30 days, and 3–6 months). |
| Gümüş (2021) [25] | Turkey | Healthcare workers, 94 | 54.3 | 41 | 36.2 | CoronaVac | 21 | CLIA with reactivity cutoff equal to or greater than 1.1. Sensitivity: NR; specificity: NR. | Seropositivity was predominantly detected nonsmokers, but the difference was not statistically significant (64.1%, p-value = 0.999) |
| Ikezaki (2021) [26] | Japan | Healthcare workers, 373 | 20.1 | 42 | 5.9 | BNT162b2 | 185 | CMIA with positivity cutoff equal to or greater than 50 AU/mL. Sensitivity of 98.3% (95%CI: 90.6–100) and specificity 99.5% (95%CI: 97.1–100). | The current smoker group tended to have lower antispike IgG levels than the past and never-smoker groups, but the difference was not statistically significant. |
| Zhang (2021) [27] | China | NR, 164 | 23.2 | 34 | 6.7 | CoronaVac | 14, 42, and 90 | SARS-CoV-2 S-RBD protein microarray. COI: NR. Sensitivity: NR; specificity: NR. | Compared to nonsmokers, the levels of neutralizing antibodies in smokers remained low throughout the period of testing. Notably, the median IgG titres in the smoking group was 1.40-, 1.32-, or 3.00-fold lower than that of nonsmoking group on day 14, 42, or 90, respectively. |
| Pitzalis (2021) [28] | Italy | Multiple Sclerosis patients, 658 | 26.9 | 48,8 | 28.6 | BNT162b2 | 30 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | There was a reduced anti-S antibodies production in smokers (median = 719 U/mL) compared to nonsmokers (median = 1054 U/mL) (p-value < 0.001). |
| Herzberg (2021) [29] | Germany | Healthcare workers, 562 | 22.8 | 43.5 | 26.0 | BNT162b2 (two doses) or ChAdOx1 (one dose) | 21–90 | ELISA with positivity ratio equal to or greater than 1.1. Sensitivity of 100% (95%CI: 91.6–100) and specificity of 97.7% (95%CI: 91.9–99.6). | A negative effect of current smoking on antibody response was observed at linear regression for anti-SARS-CoV-2 antibody ratio: estimate −0.41 (95%CI, −0.70–−0.12; p-value = 0.006). |
| Malavazos (2021) [30] | Italy | Patients with obesity, 1060 | 38.0 | 41.4 | 15.8 | BNT162b2 | T0 and day 21 after the first; and within 30–40 and 90–100 days after the second dose | CLIA with positivity threshold equal to or greater than 33.8 BAU/mL. Sensitivity of 98.7% (95%CI: 94.5–99.6) and specificity of 99.5% (95%CI: 99.0–99.7). | Smoking was associated with drops in IgG-TrimericS levels at three months after the second dose (absolute variation in IgG levels starting from one month after the second dose) at univariate (p-value = 0.03) and multivariate linear regression analyses (p-value = 0.04). |
| Yamamoto (2021) [31] | Japan | Healthcare workers, 3457 | 38.0 | 41 | 6.1 | BNT162b2 | 64 | CLEIA with positivity threshold equal to or greater than 10 SU/mL. Sensitivity of 98.3% and specificity of 99.6%. | Of 212 current smokers, 53% used HNB tobacco products. Current smokers using any tobacco product had lower antibody titres (GMT, 101; ratio of mean, 0.85 [95%CI: 0.77–0.93]) compared with never smokers. Exclusive cigarette smokers had significantly lower GMT than never smokers (GMT, 119 versus 99; ratio of means, 0.81 [95%CI: 0.71–0.92]). Exclusive HNB tobacco product users and dual users also showed similarly lowered GMT (103 and 108, respectively), although the differences from never smokers were not statistically significant (ratio of means, 0.87 [95%CI: 0.74–1.02] and 0.91 [95%CI: 0.76–1.08], respectively). Combining the two categories of HNB tobacco users (n = 113), the reduction reached statistical significance (GMT, 105; ratio of mean, 0.88 [95%CI: 0.78–0.99]). Among daily cigarette smokers, those consuming 11 or more cigarettes per day showed a greater reduction in IgG titres than those consuming less than 11 cigarettes per day; GMTs (ratio of means) were 92 (0.77 [95%CI: 0.62–0.95]) and 104 (0.87 [95% CI: 0.76–1.00]), respectively. |
| Kato [a] (2021) [32] | Japan | Healthcare workers, 168 | 25.0 | 43 | 4.2 | BNT162b2 | 14, 28 and 42 after the first dose | CLEIA with cut-off index equal to or greater than 1. Sensitivity of 100% (95%CI: 97.6–100) and specificity 100% (95%CI: 99.6–100). | There was no significant association between the titre of IgG against spike proteins induced by the vaccine and smoking habit (p-value = 0.44). |
| Nomura [a] (2021) [33] | Japan | Healthcare workers, 365 | 31.5 | 44 | 40.8 | BNT162b2 | 183 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | Smokers group: 149 ever smokers of which 90 current smokers. The age-adjusted median (IQR) antibody titres were −97 (−277 to 184) and 56 (−182 to 342) in ever-smokers and never smokers, respectively (p-value < 0.001); and −205 (−320 to 7) and −72 (−264 to 256) in current-smokers and never smokers, respectively (p-value = 0.03). For age-adjusted median antibody titres, no significant sex differences were observed in the ever-smoker and never-smoker groups. However, both the male and female groups showed significant differences by smoking status in age-adjusted median antibody titres. No significant differences in the median rate of change in antibody titres by smoking status were observed in the male and female groups. Both the ever-smoker and never-smoker groups showed significant sex differences in the median rate of change in antibody titres. |
| Kato [b] (2021) [34] | Japan | Healthcare workers, 98 | 42.4 | 43 | 5.6 | BNT162b2 | 180 | CLEIA with cutoff index equal to or greater than 1. Sensitivity of 100% (95%CI: 97.6–100) and specificity 100% (95%CI: 99.6–100). | The titre of IgG against spike proteins induced by the vaccine did not correlate with smoking status. |
| Uysal (2021) [35] | Turkey | Healthcare workers, 314 | 42.4 | 40 | 32.5 | CoronaVac | 30 | ECLIA with reactivity COI equal to or greater than 1.0 and the highest antibody value was measured as 250 U/mL by the device. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | When the smoking habit and antibody response were compared, 40% of those with an antibody titre of 1–125 U/mL had a history of smoking, while this rate was decreased down to 24.7 in the group with 126–250 U/mL, and to 27.5% in participants with seropositivity of more than 250 U/mL: thus, 72.5% of those with an antibody titre of more than 250 U/mL were nonsmokers (p-value = 0.03). |
| Alqassieh (2021) [36] | Jordan | General population, 288 | 65.6 | NR | 31.6 | BNT162b2 or BBIBP-CorV | 42 | ELFA with positivity cutoff index equal to or greater than 1. Sensitivity: NR; specificity: NR. | No significant differences were found between the two groups in terms of smoking habit (p-value = 0.351), with either BNT162b2 and BBIBP-CorV COVID-19 vaccine |
| Nomura [b] (2021) [37] | Japan | Healthcare workers, 378 | 32.5 | 44 | 40.7 | BNT162b2 | 90 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | Smokers: 49 current smokers. In both the male and female groups, age-adjusted median antibody titres were significantly lower in ever smokers than in never smokers; age-adjusted median antibody titres (IQR) in men were −246 U/mL (−398 to 65) and 49 U/mL (−186 to 621) in ever smokers and never smokers, respectively, while those in women were −140 U/mL (−304 to 217) and 95 U/mL (−151 to 503) in ever smokers and never smokers, respectively. Compared with never smokers, median IgG were −271 (−475 to 33; p-value < 0.0001) for current smokers, and −162 (−332 to 285; p-value = 0.0019) for exsmokers. Antibody titres were significantly lower in current smokers than in exsmokers (p-value = 0.019). The number of cigarettes per day did not influence the antibody titres. In both the ever smoker and never smoker groups, no significant sex differences in age-adjusted median antibody titres were observed. Given that the smoking rates in the male and female groups were 61.0% and 31.0%, respectively, these results suggest that the sex difference in antibody titres strongly reflects sex differences in smoking, rather than biological sex differences. |
| Linardou (2021) [38] | Greece | Cancer patients, 189 | 46.0 | NR | 30.6 | BNT162b2, mRNA-1273, or ChAdOx1 | 30 | CLIA with positivity threshold equal to or greater than 33.8 BAU/mL. Sensitivity of 98.7% (95%CI: 94.5–99.6) and specificity of 99.5% (95%CI: 99.0–99.7). | A significant association was identified between IgG titres and smoking status (Kruskal–Wallis p-value = 0.017). Post hoc analysis revealed that never smokers had significantly higher antibody titres compared with current smokers (median value: 632 vs. 409.5, Wilcoxon rank-sum p-value = 0.006). |
| Tsatsakis (2021) [19] | Greece | Healthcare workers, 517 | 33.7 | 47.7 | 34.4 | BNT162b2 | 60 | ELISA with positivity ratio equal to or greater than 1. Sensitivity of 97.3% (95%CI: 90.8–99.3) and specificity of 100% (95%CI: 96.0–100). | Nonsmokers had higher titres than smokers: 4.48 (±2.79 SD) and 3.80 (±2.64 SD), respectively; p-value = 0.003). No significance at multivariate linear regression analysis of antibody titre sampling postvaccination was found. |
| Moncunill (2021) [39] | Spain | Healthcare workers, 360 | 26.1 | 43.2 | 22.2 | BNT162b2 or mRNA-1273 | Up to 20 post vaccination | Quantitative suspension array technology with sensitivity of 95.8% and specificity of 100%. COI: NR. | Smoking was associated with significantly lower IgG S levels (62.5%; 95%CI 5.6–85.1; p-value = 0.038) after one (>7 days) and two doses of mRNA vaccines (12–19 days postvaccine). Being a smoker was also associated with 42.8% (95%CI 59.5–19.2; p-value = 0.002) lower plasma-neutralizing capacity. |
| Parthymou (2021) [40] | Greece | General population, 712 | 37.6 | 50.8 | 34.4 | BNT162b2 | ~ 90 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | Multivariate linear regression analysis revealed a negative association between smoking and antibody titre: β of −0.1097 (95%CI −0.173–−0.04567; p-value = 0.0008). The mean antibody titre of smokers 988 (±781.4 SD) versus 731.2 (±603.9 SD) in nonsmokers. |
| Michos (2021) [41] | Greece | Healthcare workers, 264 | 20.1 | 45.4 | 25.8 | BNT162b2 | 30 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | Smokers had a statistically significant lower antibody response for TAbs-RBD and NAbs-RBD after both the first (assessed after 20 days from the vaccination) and second vaccine doses (p-value = 0.033, p-value = 0.015, p-value =0.041, p-value = 0.002, respectively). At linear regression analysis, after the first vaccine dose, a statistically significant negative association of TAbs-RBD was detected for smoking status (p-value = 0.012). After the second vaccine dose, a statistically significant negative association of TAbs-RBD was detected for age smoking status (p-value = 0.011). |
| Lombardi (2021) [42] | Italy | Healthcare workers, 3475 | 28.8 | NR | 23.1 | BNT162b2 | 28 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | Smokers showed lower median titres than never smokers. |
| Modenese (2021) [43] | Italy | Healthcare workers, 74 | 19.9 | 48.4 | 23.0 | BNT162b2 | 28 | CLIA with reactivity cutoff equal to or greater than 1.0 AU/mL. Sensitivity of 100% (95%CI: 99.9–100) and specificity of 99.6% (95%CI: 98.7–100). | Smoking habit did not significantly affect the IgG titre (p-value = 0.55) |
| Watanabe (2021) [44] | Italy | Healthcare workers, 86 | 39.5 | 29 | 31.7 | BNT162b2 | 30 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). | Smokers had lower levels compared to nonsmokers [1099 (±1350 SD) vs. 1921 U/mL (±1375 SD), p-value = 0.007], at multivariate linear regression β coefficient was −698.28 (−1228.87 to −167.69) for current smokers (p-value = 0.011) |
| Kennedy (2021) [45] | United Kingdom | Inflammatory bowel disease patients, 1293 | 50.7 | 43.8 | 8.3 | BNT162b2 or ChAdOx1 | 21–70 | ECLIA with reactivity COI equal to or greater than 1.0. Sensitivity of 99.5% (95%CI: 97.0–100) and specificity of 99.8% (95%CI: 99.7–99.9). Positivity threshold fixed at 0.25-fold COI for patients with prior infection; of 0.12-fold for those with no evidence of prior infection. | Current smoking was independently associated with lower anti-SARS-CoV-2 antibody concentrations in subjects who received either vaccine. Fold change for both vaccines 0.53 (95%CI, 0.36−0.74; p-value < 0.001); for BNT162b2 alone 0.52 (95%CI, 0.31−0.86; p-value = 0.011); for ChAdOx1 alone 0.55 (95%CI, 0.36−0.84; p-value = 0.006). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrara, P.; Gianfredi, V.; Tomaselli, V.; Polosa, R. The Effect of Smoking on Humoral Response to COVID-19 Vaccines: A Systematic Review of Epidemiological Studies. Vaccines 2022, 10, 303. https://doi.org/10.3390/vaccines10020303
Ferrara P, Gianfredi V, Tomaselli V, Polosa R. The Effect of Smoking on Humoral Response to COVID-19 Vaccines: A Systematic Review of Epidemiological Studies. Vaccines. 2022; 10(2):303. https://doi.org/10.3390/vaccines10020303
Chicago/Turabian StyleFerrara, Pietro, Vincenza Gianfredi, Venera Tomaselli, and Riccardo Polosa. 2022. "The Effect of Smoking on Humoral Response to COVID-19 Vaccines: A Systematic Review of Epidemiological Studies" Vaccines 10, no. 2: 303. https://doi.org/10.3390/vaccines10020303
APA StyleFerrara, P., Gianfredi, V., Tomaselli, V., & Polosa, R. (2022). The Effect of Smoking on Humoral Response to COVID-19 Vaccines: A Systematic Review of Epidemiological Studies. Vaccines, 10(2), 303. https://doi.org/10.3390/vaccines10020303