

Neutralizing Antibody and T-Cell Responses against SARS-CoV-2 Wild-Type and Variants of Concern in Chronic Obstructive Pulmonary Disease Subjects after ChAdOx-1/ChAdOx-1 Homologous Vaccination: A Preliminary Study
 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Study Design and Participants
2.3. Study Procedures
2.4. Assay for Neutralizing Antibodies
2.5. Assay for CD4 and CD8 T Responses
2.6. Statistical Analysis
3. Results
3.1. Study Cohort
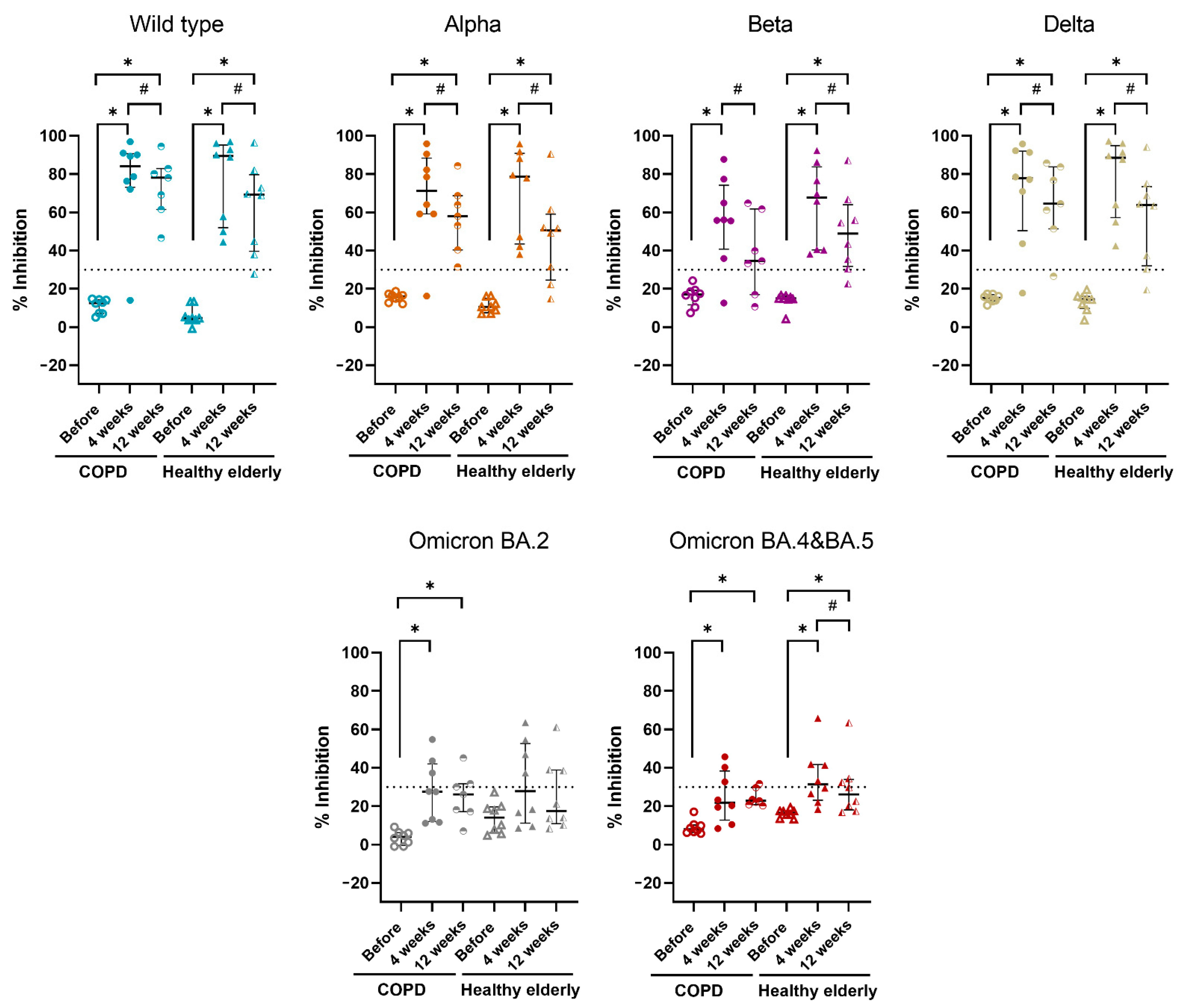
3.2. Neutralizing Antibody Responses
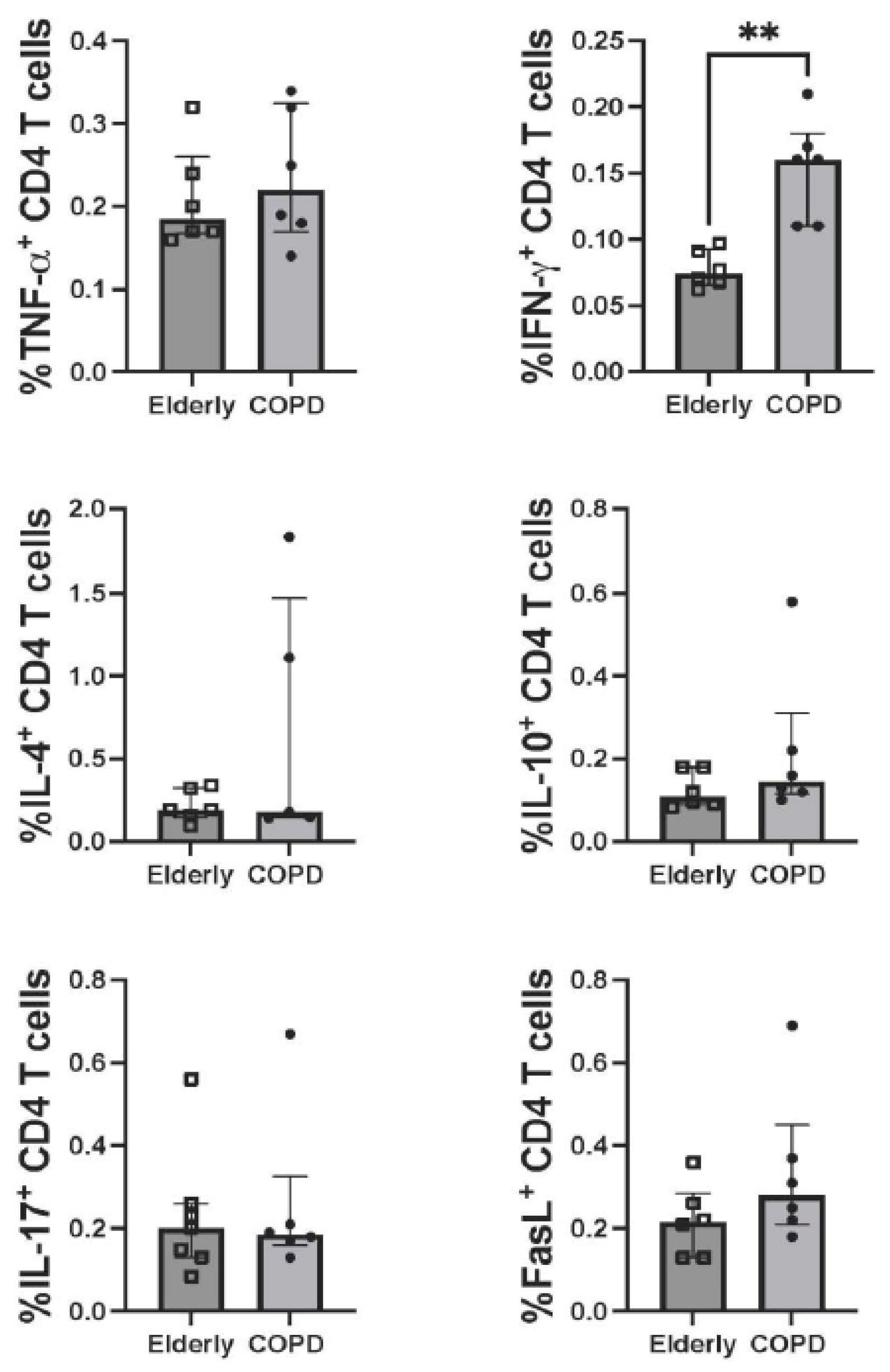
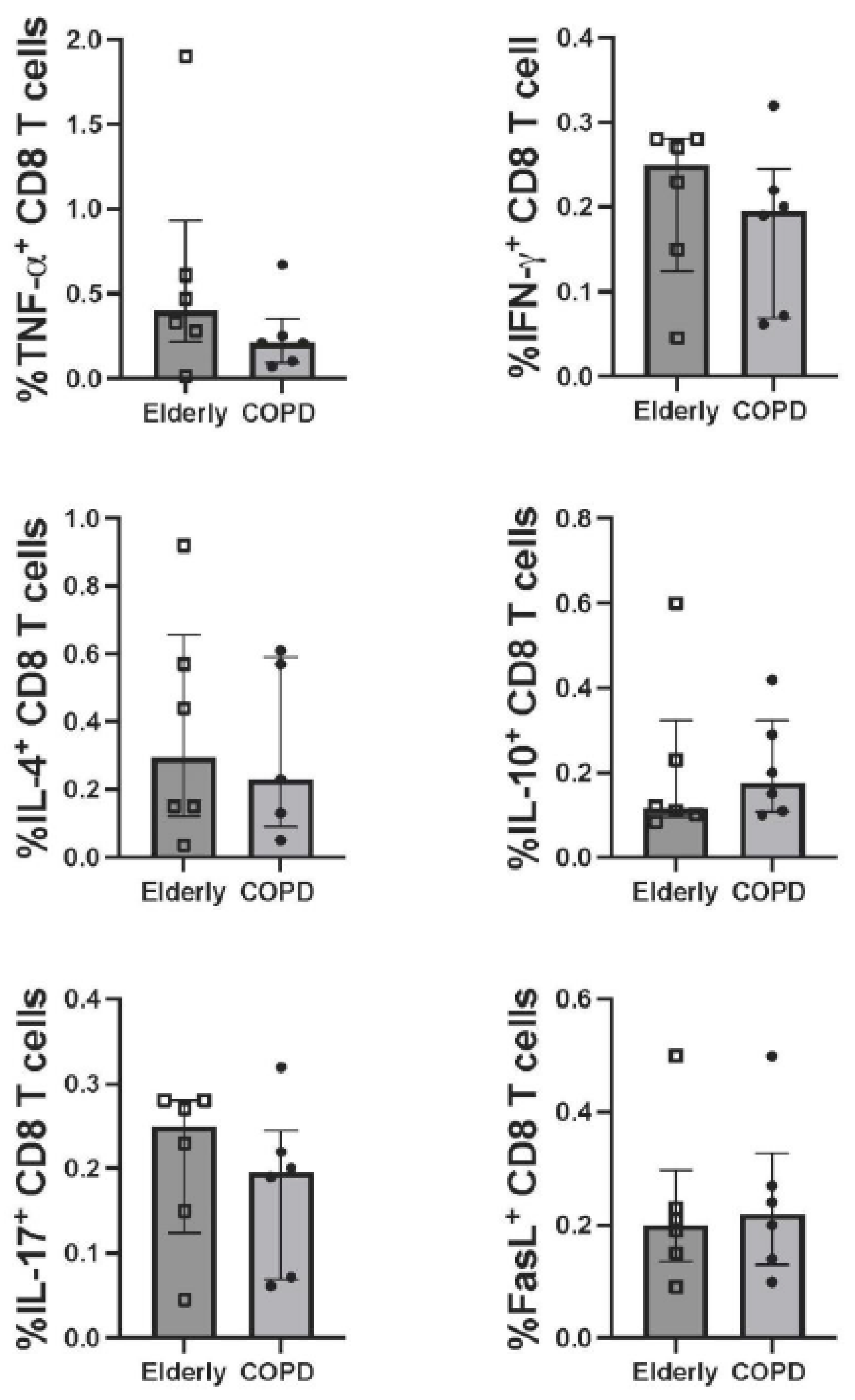
3.3. T-Cell Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Alghamdi, S.M.; Almehmadi, M.; Alqahtani, A.S.; Quaderi, S.; Mandal, S.; Hurst, J.R. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: A rapid systematic review and meta-analysis. PLoS ONE 2020, 15, e0233147. [Google Scholar] [CrossRef] [PubMed]
- Saheb Sharif-Askari, N.; Saheb Sharif-Askari, F.; Alabed, M.; Temsah, M.H.; Al Heialy, S.; Hamid, Q.; Halwani, R. Airways expression of SARS-CoV-2 receptor, ACE2, and TMPRSS2 is lower in children than adults and increases with smoking and COPD. Mol. Ther. Methods Clin. Dev. 2020, 18, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care. Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Nath, K.D.; Burel, J.G.; Shankar, V.; Pritchard, A.L.; Towers, M.; Looke, D.; Davies, J.M.; Upham, J.W. Clinical factors associated with the humoral immune response to influenza vaccination in chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Parpaleix, A.; Boyer, L.; Wiedemann, A.; Lacabaratz, C.; Margarit, L.; Enouf, V.; Le Corvoisier, P.; Lino, A.; Covali-Noroc, A.; Housset, B.; et al. Impaired humoral and cellular immune responses to influenza vaccination in chronic obstructive pulmonary disease patients. J. Allergy Clin. Immunol. 2017, 140, 1754–1757.e6. [Google Scholar] [CrossRef] [PubMed]
- Burel, J.G.; Nath, K.; Pritchard, A.L.; White, O.J.; Davies, J.M.; Towers, M.; Looke, D.; Upham, J.W. Evaluation of immune responses to influenza vaccination in chronic obstructive pulmonary disease. J. Vaccines Vaccin. 2012, S4, 001. [Google Scholar]
- Harboe, Z.B.; Hamm, S.R.; Pérez-Alós, L.; Sivapalan, P.; Priemé, H.; Wilcke, T.; Kjeldgaard, P.; Shaker, S.; Svorre Jordan, A.; Møller, D.L.; et al. Antibody responses and risk factors associated with impaired immunological outcomes following two doses of BNT162b2 COVID-19 vaccination in patients with chronic pulmonary diseases. BMJ. Open Respir. Res. 2022, 9, e001268. [Google Scholar] [CrossRef]
- Pelletier, É.; Desmeules, P.; Lacasse, Y.; Tanguay, S.; Milot, J.; Morissette, M.C.; Maltais, F. Antibody response to severe acute respiratory syndrome coronavirus-2 vaccination in COPD: A cohort study. Chronic Obstr. Pulm. Dis. 2022, 9, 591–595. [Google Scholar] [CrossRef]
- Southworth, T.; Jackson, N.; Singh, D. Airway immune responses to COVID-19 vaccination in COPD patients and healthy subjects. Eur. Respir. J. 2022, 60, 2200497. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of spirometry 2019 update. An official american thoracic society and european respiratory society technical statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Knudson, R.J.; Lebowitz, M.D.; Holberg, C.J.; Burrows, B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am. Rev. Respir. Dis. 1983, 127, 725–734. [Google Scholar] [PubMed]
- Mohseni Afshar, Z.; Babazadeh, A.; Janbakhsh, A.; Mansouri, F.; Sio, T.T.; Sullman, M.J.M.; Carson-Chahhoud, K.; Hosseinzadeh, R.; Barary, M.; Ebrahimpour, S. Coronavirus disease 2019 (COVID-19) vaccination recommendations in special populations and patients with existing comorbidities. Rev. Med. Virol. 2022, 32, e2309. [Google Scholar] [CrossRef] [PubMed]
- Liwsrisakun, C.; Pata, S.; Laopajon, W.; Takheaw, N.; Chaiwong, W.; Inchai, J.; Pothirat, C.; Bumroongkit, C.; Deesomchok, A.; Theerakittikul, T.; et al. Neutralizing antibody and T cell responses against SARS-CoV-2 variants of concern following ChAdOx-1 or BNT162b2 boosting in the elderly previously immunized with CoronaVac vaccine. Immun. Ageing 2022, 19, 24. [Google Scholar] [CrossRef]
- Chau, N.V.V.; Nguyet, L.A.; Truong, N.T.; Toan, L.M.; Dung, N.T.; Hung, L.M.; Nhan, M.T.; Man, D.N.H.; Ngoc, N.M.; Thao, H.P.; et al. Immunogenicity of oxford-astrazeneca COVID-19 vaccine in vietnamese health-care workers. Am. J. Trop. Med. Hyg. 2022, 106, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Brockman, M.A.; Mwimanzi, F.; Lapointe, H.R.; Sang, Y.; Agafitei, O.; Cheung, P.K.; Ennis, S.; Ng, K.; Basra, S.; Lim, L.Y.; et al. Reduced magnitude and durability of humoral immune responses to COVID-19 mRNA vaccines among older adults. J. Infect. Dis. 2022, 225, 1129–1140. [Google Scholar] [CrossRef]
- Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 2022, 23, 186–193. [Google Scholar] [CrossRef]
- Young, A. T cells in SARS-CoV-2 infection and vaccination. Ther. Adv. Vaccines Immunother. 2022, 10, 25151355221115011. [Google Scholar] [CrossRef]
- Li, Q.; Wang, Y.; Sun, Q.; Knopf, J.; Herrmann, M.; Lin, L.; Jiang, J.; Shao, C.; Li, P.; He, X.; et al. Immune response in COVID-19: What is next? Cell Death. Differ. 2022, 29, 1107–1122. [Google Scholar] [CrossRef]
- Zhu, X.; Zhu, J. CD4 T helper cell subsets and related human immunological disorders. Int. J. Mol. Sci. 2020, 21, 8011. [Google Scholar] [CrossRef]
- Topham, D.J.; Tripp, R.A.; Doherty, P.C. CD8+ T cells clear influenza virus by perforin or Fas-dependent processes. J. Immunol. 1997, 159, 5197–5200. [Google Scholar]
- Ratner, A.; Clark, W.R. Role of TNF-alpha in CD8+ cytotoxic T lymphocyte-mediated lysis. J. Immunol. 1993, 150, 4303–4314. [Google Scholar] [PubMed]
- Kotov, D.I.; Kotov, J.A.; Goldberg, M.F.; Jenkins, M.K. Many Th cell subsets have Fas ligand-dependent cytotoxic potential. J. Immunol. 2018, 200, 2004–2012. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, T.M.A.; Schembri, S.; Brightling, C.; Bakerly, N.D.; Lewis, K.; MacNee, W.; Rombo, L.; Hedner, J.; Allen, M.; Walker, P.P.; et al. Non-typeable Haemophilus influenzae protein vaccine in adults with COPD: A phase 2 clinical trial. Vaccine 2019, 37, 6102–6111. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.X.; Tomchaney, M.; Landecho, M.F.; Zamacona, B.R.; Marin Oto, M.; Zulueta, J.; Malo, J.; Knoper, S.; Contoli, M.; Papi, A.; et al. Lung spatial profiling reveals a T cell signature in COPD patients with fatal SARS-CoV-2 infection. Cells 2022, 11, 1864. [Google Scholar] [CrossRef]
- Lafon, E.; Diem, G.; Witting, C.; Zaderer, V.; Bellmann-Weiler, R.M.; Reindl, M.; Bauer, A.; Griesmacher, A.; Fux, V.; Hoermann, G.; et al. Potent SARS-CoV-2-specific T cell immunity and low anaphylatoxin levels correlate with mild disease progression in COVID-19 patients. Front. Immunol. 2021, 12, 684014. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.T.; Linster, M.; Tan, C.W.; Le Bert, N.; Chia, W.N.; Kunasegaran, K.; Zhuang, Y.; Tham, C.Y.L.; Chia, A.; Smith, G.J.D.; et al. Early induction of functional SARS-CoV-2-specific T cells associates with rapid viral clearance and mild disease in COVID-19 patients. Cell. Rep. 2021, 34, 108728. [Google Scholar] [CrossRef]
- Gao, L.; Zhou, J.; Yang, S.; Wang, L.; Chen, X.; Yang, Y.; Li, R.; Pan, Z.; Zhao, J.; Li, Z.; et al. The dichotomous and incomplete adaptive immunity in COVID-19 patients with different disease severity. Signal Transduct. Target. Ther. 2021, 6, 113. [Google Scholar] [CrossRef]
- Zhang, L.; Li, R.; Song, G.; Scholes, G.D.; She, Z.S. Impairment of T cells’ antiviral and anti-inflammation immunities may be critical to death from COVID-19. R. Soc. Open. Sci. 2021, 8, 211606. [Google Scholar] [CrossRef]
- Zenarruzabeitia, O.; Astarloa-Pando, G.; Terrén, I.; Orrantia, A.; Pérez-Garay, R.; Seijas-Betolaza, I.; Nieto-Arana, J.; Imaz-Ayo, N.; Pérez-Fernández, S.; Arana-Arri, E.; et al. T cell activation, highly armed cytotoxic cells and a shift in monocytes CD300 receptors expression is characteristic of patients with severe COVID-19. Front. Immunol. 2021, 12, 655934. [Google Scholar] [CrossRef]
- Lacedonia, D.; Scioscia, G.; Santomasi, C.; Fuso, P.; Carpagnano, G.E.; Portacci, A.; Mastroianni, F.; Larizza, G.; Sabato, E.; Profilo, E.; et al. Impact of smoking, COPD and comorbidities on the mortality of COVID-19 patients. Sci. Rep. 2021, 11, 19251. [Google Scholar] [CrossRef]
- Kim, Y.; An, T.J.; Park, Y.B.; Kim, K.; Cho, D.Y.; Rhee, C.K.; Yoo, K.H. Chronic obstructive pulmonary disease is not associated with a poor prognosis in COVID-19. Tuberc. Respir. Dis. 2022, 85, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.S.; Kim, J.S.; You, Y.S.; Yeom, S.W.; Lee, Y.C. COPD is a risk factor for COVID-19, but does not confer increased severity of the disease. Respir. Med. 2021, 189, 106640. [Google Scholar] [CrossRef] [PubMed]
- Turan, O.; Arpınar Yigitbas, B.; Turan, P.A.; Mirici, A. Clinical characteristics and outcomes of hospitalized COVID-19 patients with COPD. Expert. Rev. Respir. Med. 2021, 15, 1069–1076. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | COPD (N = 8) | Healthy Elderly (N = 8) | p-Value |
|---|---|---|---|
| Age (years) | 77.1 ± 6.5 | 73.5 ± 4.8 | 0.224 |
| Male (sex) | 7 (87.5) | 7 (87.5) | 1.000 |
| Height (cm) | 159.9 ± 7.2 | 165.1 ± 9.8 | 0.240 |
| Body weight (kg) | 54.9 ± 10.1 | 62.0 ± 8.9 | 0.157 |
| Body mass index (kg/m2) | 21.6 ± 5.0 | 22.8 ± 2.9 | 0.593 |
| Underlying diseases | 0.721 | ||
| Cardiovascular | 2 (25.0) | 2 (25.0) | |
| Metabolic | 0 (0.0) | 1 (12.5) | |
| Cardiovascular + Metabolic | 2 (25.0) | 1 (12.5) | |
| None | 4 (50.0) | 4 (50.0) | |
| Smoking status | 0.026 | ||
| Non-smoker | 0 (0.0) | 5 (62.5) | |
| Ex-smoker | 8 (100.0) | 3 (37.5) | |
| Smoking pack-year (Median, IQR) | 45.0 (25.3, 50.0) | 0.0 (0.0, 30.0) | 0.012 |
| Spirometry results | N.A. | ||
| FVC | 2.49 ± 0.58 | ||
| % predicted of FVC | 96.9 ± 23.7 | ||
| FEV1 | 1.38 ± 0.45 | ||
| % predicted of FEV1 | 69.7 ± 27.7 | ||
| Ratio of FEV1/FVC | 54.4 ± 9.9 | ||
| Inhaled medication for COPD | N.A. | ||
| LAMA | 1 (12.5) | ||
| LABA + LAMA | 1 (12.5) | ||
| ICS + LABA | 1 (12.5) | ||
| ICS + LAMA | 1 (12.5) | ||
| ICS + LABA + LAMA | 4 (50.0) |
| COPD | Healthy Elderly | |||||
|---|---|---|---|---|---|---|
| Before (n = 8) | 4 Weeks (n = 8) | 12 Weeks (n = 7) | Before (n = 8) | 4 Weeks (n = 8) | 12 Weeks (n = 8) | |
| Wild-type | 12.6 (7.1, 14.3) | 84.0 * (73.2, 90.7) | 78.1 *,# (61.5, 82.9) | 4.7 (3.7, 11.2) | 89.4 * (51.9, 95.2) | 69.2 *,# (39.5, 79.7) |
| Alpha (B.1.1.7) | 15.9 (13.2, 17.1) | 71.2 * (59.1, 88.4) | 57.9 *,# (40.3, 68.7) | 10.5 (7.4, 15.1) | 78.6 * (43.4, 90.8) | 50.5 *,# (24.5, 59.0) |
| Beta (B.1.351) | 17.0 (11.5, 19.1) | 55.9 * (40.7, 74.2) | 34.6 # (16.9, 61.7) | 14.9 (14.6, 16.1) | 67.7 * (40.3, 83.7) | 48.9 *,# (31.7, 63.9) |
| Delta (B.1.617.2) | 15.2 (13.7, 16.9) | 77.8 * (50.4, 91.9) | 64.5 *,# (51.3, 83.8) | 14.5 (9.7, 15.9) | 88.6 * (57.2, 94.8) | 63.8 *,# (31.9, 73.4) |
| Omicron BA.2 | 3.9 (−0.4, 6.2) | 27.6 * (11.9, 41.9) | 26.2 * (17.1, 31.7) | 14.0 (6.2, 19.6) | 27.8 (11.1, 52.6) | 17.5 (10.9, 38.8) |
| Omicron BA.4&BA.5 | 7.9 (6.3, 10.3) | 21.8 * (12.7, 38.3) | 22.8 * (20.7, 29.7) | 16.5 (13.9, 17.5) | 31.3 * (23.0, 41.7) | 26.2 *,# (17.9, 33.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaiwong, W.; Takheaw, N.; Laopajon, W.; Pata, S.; Duangjit, P.; Inchai, J.; Pothirat, C.; Bumroongkit, C.; Deesomchok, A.; Theerakittikul, T.; et al. Neutralizing Antibody and T-Cell Responses against SARS-CoV-2 Wild-Type and Variants of Concern in Chronic Obstructive Pulmonary Disease Subjects after ChAdOx-1/ChAdOx-1 Homologous Vaccination: A Preliminary Study. Vaccines 2022, 10, 2176. https://doi.org/10.3390/vaccines10122176
Chaiwong W, Takheaw N, Laopajon W, Pata S, Duangjit P, Inchai J, Pothirat C, Bumroongkit C, Deesomchok A, Theerakittikul T, et al. Neutralizing Antibody and T-Cell Responses against SARS-CoV-2 Wild-Type and Variants of Concern in Chronic Obstructive Pulmonary Disease Subjects after ChAdOx-1/ChAdOx-1 Homologous Vaccination: A Preliminary Study. Vaccines. 2022; 10(12):2176. https://doi.org/10.3390/vaccines10122176
Chicago/Turabian StyleChaiwong, Warawut, Nuchjira Takheaw, Witida Laopajon, Supansa Pata, Pilaiporn Duangjit, Juthamas Inchai, Chaicharn Pothirat, Chaiwat Bumroongkit, Athavudh Deesomchok, Theerakorn Theerakittikul, and et al. 2022. "Neutralizing Antibody and T-Cell Responses against SARS-CoV-2 Wild-Type and Variants of Concern in Chronic Obstructive Pulmonary Disease Subjects after ChAdOx-1/ChAdOx-1 Homologous Vaccination: A Preliminary Study" Vaccines 10, no. 12: 2176. https://doi.org/10.3390/vaccines10122176
APA StyleChaiwong, W., Takheaw, N., Laopajon, W., Pata, S., Duangjit, P., Inchai, J., Pothirat, C., Bumroongkit, C., Deesomchok, A., Theerakittikul, T., Limsukon, A., Tajarernmuang, P., Niyatiwatchanchai, N., Trongtrakul, K., Chuensirikulchai, K., Cheyasawan, P., Liwsrisakun, C., & Kasinrerk, W. (2022). Neutralizing Antibody and T-Cell Responses against SARS-CoV-2 Wild-Type and Variants of Concern in Chronic Obstructive Pulmonary Disease Subjects after ChAdOx-1/ChAdOx-1 Homologous Vaccination: A Preliminary Study. Vaccines, 10(12), 2176. https://doi.org/10.3390/vaccines10122176