
SARS-CoV-2 Seroprevalence in Unvaccinated Adults in Thailand in November 2021

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sampling Plan Strategies
2.3. Blood Collection and Processing
2.4. Laboratory Testing
2.4.1. SARS-CoV-2 Antibody Testing by In-House Immunoassay (ELISA)
2.4.2. Quantitative for SARS-CoV-2
2.5. Data Collection and Data Analysis
3. Results
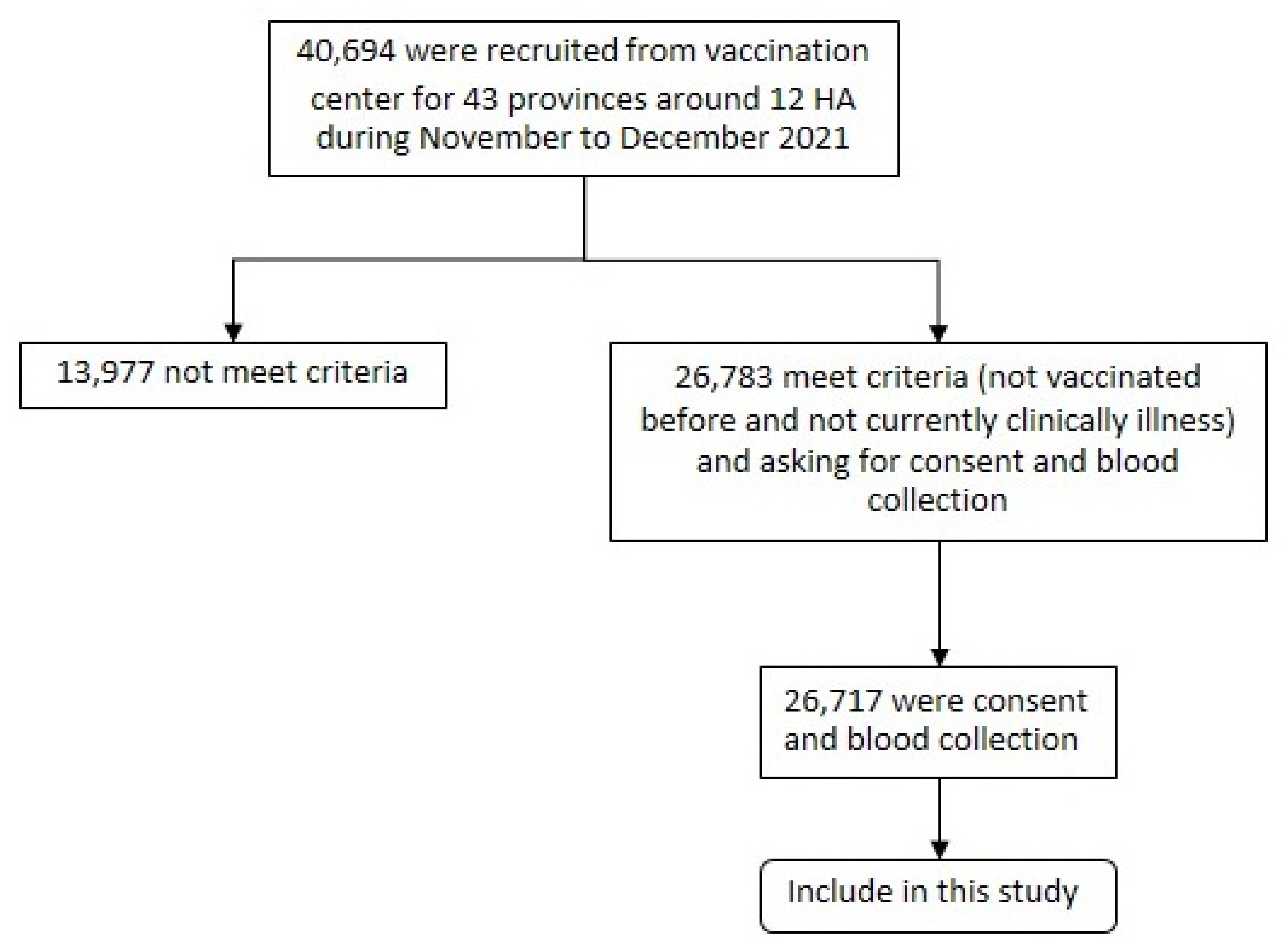
3.1. Participant Data
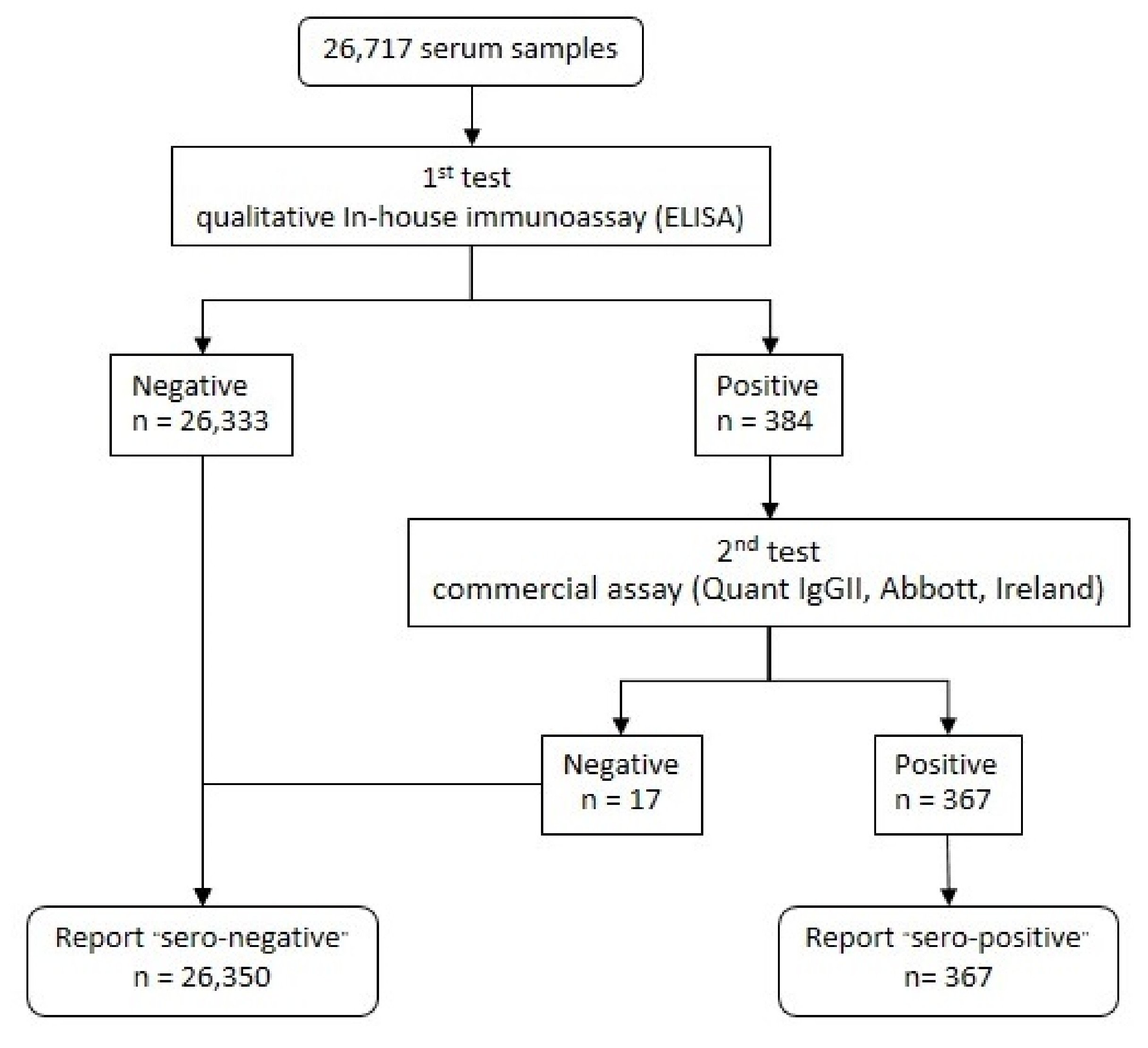
3.2. Serological Test Result
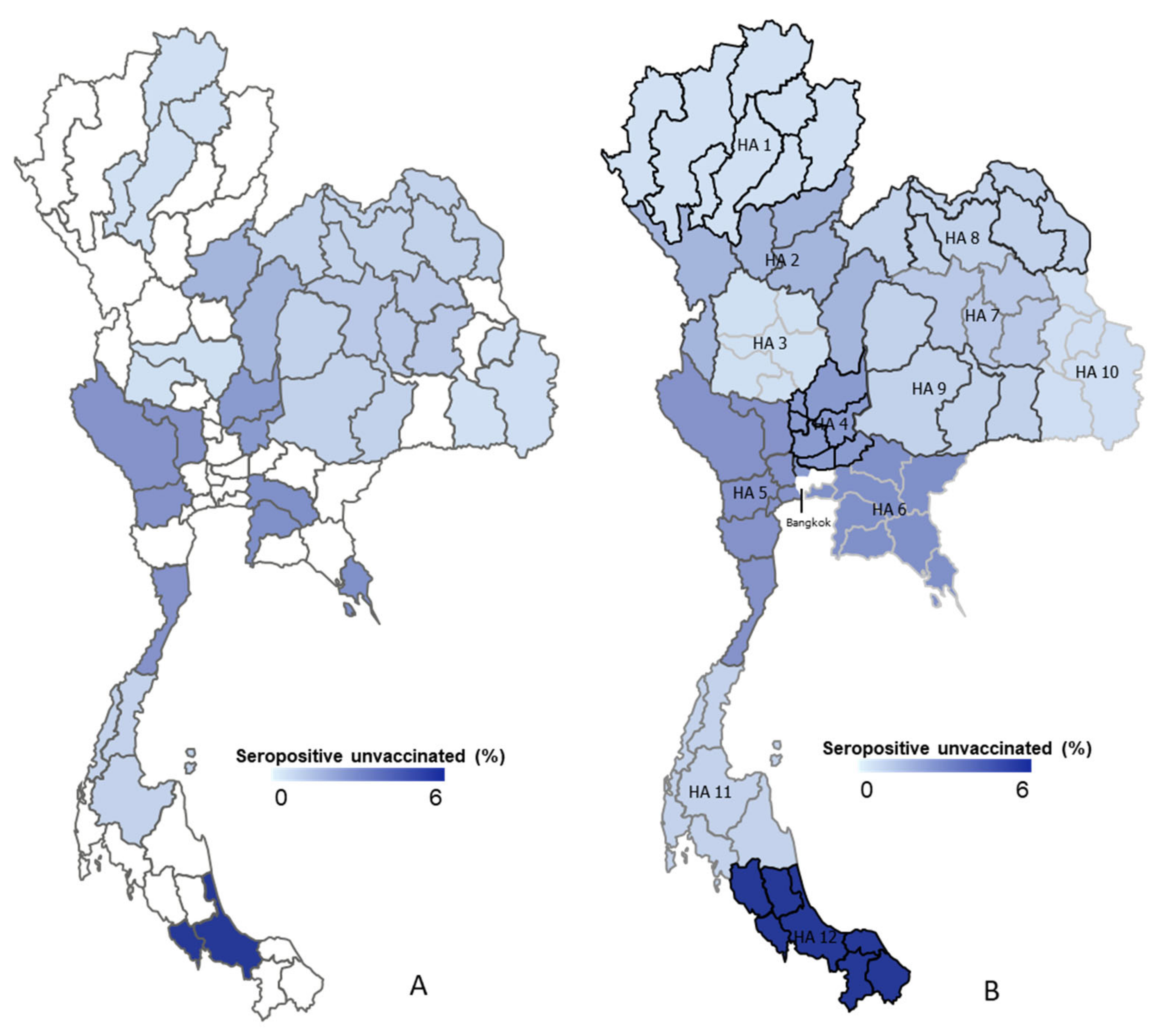
3.3. Seroprevalence by Geographic Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Public Health Areas | Random Provinces | Population |
|---|---|---|
| North | ||
| Public health area 1 | 5,876,353 | |
| Chiang Mai, Chiang Rai, Lampang, Phayao, Phrae, Nan, Lamphun, Mae Hong Son | Chiang Rai, Lampang, Lamphun, Phayao | |
| Public health area 2 | 3,538,314 | |
| Phetchabun, Phitsanulok, Tak, Uttaradit, Sukhothai | Phetchabun, Phitsanulok | |
| Central | ||
| Public health area 3 | 2,935,081 | |
| Nakhon Sawan, Uthai Thani, Kamphaeng Phet, Phichit, Chai Nat | Nakhon Sawan, Uthai Thani | |
| Public health area 4 | 5,401,564 | |
| Ang Thong, Lop Buri, Sing Buri, Saraburi, Nonthaburi, Nakhon Nayok, Phra Nakhon Si Ayutthaya, Pathum Thani | Ang Thong, Lop Buri, Sing Buri, Saraburi | |
| Public health area 5 | 5,331,768 | |
| Kanchanaburi, Nakhon Pathom, Prachuap Khiri Khan, Ratchaburi, Suphan Buri, Samut Songkhram, Samut Sakhon, Phetchaburi | Kanchanaburi, Nakhon Pathom, Prachuap Khiri Khan, Ratchaburi, Suphan Buri, Samut Songkhram | |
| Public health area 6 | 6,199,296 | |
| Chon Buri, Chachoengsao, Trat, Sa Kaeo, Prachin Buri, Samut Prakan, Chanthaburi, Rayong | Chon Buri, Chachoengsao, Trat | |
| North-East | ||
| Public health area 7 | 5,024,006 | |
| Khon Kaen, Kalasin, Maha Sarakham, Roi Et | Khon Kaen, Kalasin, Maha Sarakham, Roi Et | |
| Public health area 8 | 5,519,803 | |
| Bueng Kan, Nong Bua Lam Phu, Nong Khai, Loei, Nakhon Phanom, Sakon Nakhon, Udon Thani | Bueng Kan, Nong Bua Lam Phu, Nong Khai, Loei, Nakhon Phanom, Sakon Nakhon, Udon Thani | |
| Public health area 9 | 6,717,536 | |
| Buri Ram, Chaiyaphum, Nakhon Ratchasima, Surin | Buri Ram, Chaiyaphum, Nakhon Ratchasima | |
| Public health area 10 | 4,586,883 | |
| Si Sa Ket, Ubon Ratchathani, Amnat Charoen, Mukdahan | Si Sa Ket, Ubon Ratchathani, Amnat Charoen | |
| South | ||
| Public health area 11 | 4,482,497 | |
| Chumphon, Ranong, Surat Thani, Nakhon Si Thammarat, Phuket, Krabi | Chumphon, Ranong, Surat Thani | |
| Public health area 12 | 4,985,404 | |
| Songkhla, Satun, Trang, Phatthalung, Pattani, Yala, Narathiwat | Songkhla, Satun | |
| Public health area 13 (Bangkok) | - | 5,588,222 |
| Grand Total | 66,186,727 |
References
- Dousari, A.S.; Moghadam, M.T.; Satarzadeh, N. COVID-19 (Coronavirus Disease 2019): A New Coronavirus Disease. Infect. Drug Resist. 2020, 13, 2819–2828. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Tiwari, S.; Deb, M.K.; Marty, J.L. Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2): A Global Pandemic and Treatment Strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 5 July 2022).
- Uansri, S.; Tuangratananon, T.; Phaiyarom, M.; Rajatanavin, N.; Suphanchaimat, R.; Jaruwanno, W. Predicted Impact of the Lockdown Measure in Response to Coronavirus Disease 2019 (COVID-19) in Greater Bangkok, Thailand, 2021. Int. J. Environ. Res. Public Health 2021, 18, 12816. [Google Scholar] [CrossRef] [PubMed]
- Tahamtan, A.; Ardebili, A. Real-Time RT-PCR in COVID-19 Detection: Issues Affecting the Results. Expert Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Coronavirus Disease 2019 (COVID-19): Situation Report, 26. Available online: https://apps.who.int/iris/handle/10665/331443 (accessed on 5 July 2022).
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal Dynamics in Viral Shedding and Transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Laboratory Testing for Coronavirus Disease (COVID-19) in Suspected Human Cases: Interim Guidance, 19 March 2020. Available online: https://apps.who.int/iris/handle/10665/331501 (accessed on 17 September 2022).
- Takalay, S.; Ngo-Giang-Huong, N.; Kongnim, W.; Mongkolwat, P.; Phoseng, P.; Wangsaeng, N.; Hongjaisee, S.; Butr-Indr, B.; Tragoolpua, K.; Jourdain, G.; et al. Prevalences of SARS-CoV-2 RNA and Anti-SARS-CoV-2 among at-Risk Populations in Chiang Mai and Lamphun Provinces, Thailand, during November 2020–January 2021. PLoS ONE 2022, 17, e0263127. [Google Scholar] [CrossRef] [PubMed]
- Kittikraisak, W.; Piyaraj, P.; Vachiraphan, A.; Wongrapee, T.; Punjasamanvong, S.; Hunsawong, T.; Sinthuwattanawibool, C.; Leepiyasakulchai, C.; Yoocharoen, P.; Azziz-Baumgartner, E.; et al. Sero-Surveillance for SARS-CoV-2 Infection among Healthcare Providers in Four Hospitals in Thailand One Year after the First Community Outbreak. PLoS ONE 2021, 16, e0254563. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M.; Opsomer, J.D.; Stone, M.; Benoit, T.; Ferg, R.A.; Stramer, S.L.; Busch, M.P. Updated US Infection- and Vaccine-Induced SARS-CoV-2 Seroprevalence Estimates Based on Blood Donations, July 2020–December 2021. JAMA 2022, 328, 298–301. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Immunity Task Force. Latest Canadian Blood Services Data Reflect Uptick in Infections Prior to Omicron Surge—COVID-19 Immunity Task Force. Available online: https://www.covid19immunitytaskforce.ca/latest-canadian-blood-services-data-reflect-uptick-in-infections-prior-to-omicron-surge/ (accessed on 18 September 2022).
- Scotland, P.H. Enhanced Surveillance of COVID-19 in Scotland—Population-Based Seroprevalence Surveillance 19 January 2022. Public Health 2022, 190, 132–134. [Google Scholar] [CrossRef]
- Cable, R.; Coleman, C.; Glatt, T.; Grebe, E.; Mhlanga, L.; Nyoni, C.; Pieterson, N.; Swanevelder, R.; Swarts, A.; Sykes, W.; et al. Estimates of Prevalence of Anti-SARS-CoV-2 Antibodies among Blood Donors in Eight Provinces of South Africa in November 2021; Research Square: Durham, NC, USA, 2022. [Google Scholar] [CrossRef]
- Nopsopon, T.; Pongpirul, K.; Chotirosniramit, K.; Hiransuthikul, N. COVID-19 Seroprevalence among Hospital Staff and Preprocedural Patients in Thai Community Hospitals: A Cross-Sectional Study. BMJ Open 2021, 11, e046676. [Google Scholar] [CrossRef] [PubMed]
- Kunno, J.; Supawattanabodee, B.; Sumanasrethakul, C.; Wiriyasivaj, B.; Kuratong, S.; Kaewchandee, C. Comparison of Different Waves during the COVID-19 Pandemic: Retrospective Descriptive Study in Thailand. Adv. Prev. Med. 2021, 2021, 5807056. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Ho, F.K.; Gill, J.M.; Ghouri, N.; Gray, S.R.; Celis-Morales, C.A.; Katikireddi, S.V.; Berry, C.; Pell, J.P.; McMurray, J.J.; et al. BMI and Future Risk for COVID-19 Infection and Death across Sex, Age and Ethnicity: Preliminary Findings from UK Biobank. Diabetes Metab. Syndr. 2020, 14, 1149–1151. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, J.; Plante, K.S.; Plante, J.A.; Xie, X.; Zhang, X.; Ku, Z.; An, Z.; Scharton, D.; Schindewolf, C.; et al. The N501Y Spike Substitution Enhances SARS-CoV-2 Infection and Transmission. Nature 2021, 602, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Ioannidis, J.P.A. SARS-CoV-2 Reinfections: Overview of Efficacy and Duration of Natural and Hybrid Immunity. Environ. Res. 2022, 209, 112911. [Google Scholar] [CrossRef] [PubMed]
- Gornyk, D.; Harries, M.; Glöckner, S.; Strengert, M.; Kerrinnes, T.; Heise, J.K.; Maaß, H.; Ortmann, J.; Kessel, B.; Kemmling, Y.; et al. SARS-CoV-2 Seroprevalence in Germany: A Population-Based Sequential Study in Seven Regions. Dtsch. Ärzteblatt Int. 2021, 118, 824. [Google Scholar] [CrossRef]



| Characteristics | Count | Percentage |
|---|---|---|
| Gender | ||
| Female | 13,873 | 51.9 |
| Male | 12,844 | 48.1 |
| Age groups (years) | ||
| 18–27 | 8158 | 30.5 |
| 28–37 | 5186 | 19.4 |
| 38–47 | 5146 | 19.3 |
| 48–57 | 6127 | 22.9 |
| ≥58 | 2100 | 7.9 |
| Body mass index (BMI) groups (kg/m2) | ||
| <18.5 (underweight) | 2564 | 9.6 |
| 18.5–24.9 | 14,221 | 53.2 |
| 25–30 (overweight) | 6240 | 23.4 |
| >30 (obese) | 2593 | 9.7 |
| Not defined | 1099 | 11.1 |
| Blood pressure (SBP/DBP) | ||
| Normal (91–120/61–80) | 7144 | 26.8 |
| Pre high (121–140/81–90) | 5873 | 21.9 |
| High (141–190/91–100) | 2674 | 10.0 |
| Not defined | 11,026 | 41.3 |
| Occupation groups | ||
| Government employed (e.g., military, police) | 1282 | 4.8 |
| Non-government employed (e.g., clerk, accountant) | 846 | 3.2 |
| Freelance (non-salaried worker, owner, farmer, trader, rider) | 17,309 | 64.8 |
| Other (e.g., student, monk, retired, unemployed) | 2898 | 10.8 |
| Not defined | 4382 | 16.4 |
| Number of household member | ||
| Alone | 3644 | 13.6 |
| 1–2 | 4089 | 15.3 |
| 3–5 | 14,868 | 55.6 |
| >5 | 4116 | 15.4 |
| Underlying diseases | ||
| No | 21,210 | 79.4 |
| Yes | 5507 | 20.6 |
| Close contact with COVID-19 cases | ||
| No | 26,275 | 98.3 |
| Yes | 442 | 1.7 |
| Public Health Areas | n | SARS-CoV-2 IgG Seropositive (Cases) | % Seropositive (95% CI) |
|---|---|---|---|
| North | |||
| Public health area 1 | 1416 | 6 | 0.4 (0.16–0.92) |
| Public health area 2 | 1431 | 24 | 1.6 (1.08–2.49) |
| Central | |||
| Public health area 3 | 1366 | 6 | 0.4 (0.16–0.95) |
| Public health area 4 | 1382 | 34 | 2.5 (1.71–3.42) |
| Public health area 5 | 1084 | 29 | 2.7 (1.80–3.82) |
| Public health area 6 | 2517 | 70 | 2.8 (2.17–3.50) |
| North-East | |||
| Public health area 7 | 3726 | 40 | 1.1 (0.77–1.46) |
| Public health area 8 | 3137 | 27 | 0.9 (0.57–1.25) |
| Public health area 9 | 4084 | 35 | 0.9 (0.60–1.19) |
| Public health area 10 | 3702 | 17 | 0.5 (0.27–0.73) |
| South | |||
| Public health area 11 | 1744 | 14 | 0.8 (0.44–1.34) |
| Public health area 12 | 1128 | 65 | 5.8 (4.48–7.29) |
| Bangkok (Public health area 13) | - | - | - |
| Overall | 26,717 | 367 | 1.4 (1.24–1.52) |
| Characteristics | Count | SARS-CoV-2 IgG Seropositive (Cases) | % Seropositive (95% CI) |
|---|---|---|---|
| Gender | |||
| Female | 13,873 | 219 | 1.6 (1.38–1.80) |
| Male | 12,844 | 148 | 1.2 (0.98–1.35) |
| Age groups (years) | |||
| 18–27 | 8150 | 101 | 1.2 (0.10–1.50) |
| 28–37 | 5186 | 82 | 1.6 (1.26–1.96) |
| 38–47 | 5146 | 79 | 1.5 (1.22–1.91) |
| 48–57 | 6127 | 71 | 1.2 (0.91–1.46) |
| ≥58 | 2100 | 33 | 1.6 (1.08–2.19) |
| Body Mass Index (BMI) groups (kg/m2) | |||
| <18.5 (underweight) | 2564 | 32 | 1.2 (0.86–1.76) |
| 18.5–24.9 | 14,221 | 172 | 1.2 (1.04–1.40) |
| 25–30 (overweight) | 6240 | 90 | 1.4 (1.16–1.77) |
| >30 (obese) | 2593 | 52 | 2.0 (1.50–2.62) |
| Not defined | 1099 | 21 | 1.9 (1.19–2.9.1) |
| Blood Pressure (SBP/DBP) | |||
| Normal (70–120/40–80) | 7144 | 77 | 1.1 (0.85–1.34) |
| Pre high (121–140/81–90) | 5873 | 75 | 1.3 (1.01–1.60) |
| High (141–190/91–100) | 2674 | 22 | 0.8 (0.51–1.24) |
| Not defined | 11,026 | 193 | 1.8 (1.51–2.01) |
| Occupations groups | |||
| Government employed (e.g., military, police) | 1282 | 20 | 1.6 (0.96–2.40) |
| Non-government employed (e.g., clerk, accountant) | 846 | 12 | 1.4 (0.74–2.46) |
| Freelance (non-salaried worker, owner, farmer, trader, rider) | 17,309 | 235 | 1.4 (1.19–1.54) |
| Other (e.g., student, monk, retired, unemployed) | 2898 | 20 | 0.7 (0.42–1.06) |
| Not defined | 4382 | 80 | 1.8 (1.45–2.27) |
| Number of household member | |||
| Alone | 3644 | 72 | 1.9 (1.55–2.48) |
| 1–2 | 4089 | 51 | 1.2 (0.93–1.64) |
| 3–5 | 14,868 | 178 | 1.2 (1.03–1.39) |
| >5 | 4116 | 66 | 1.6 (1.24–2.04) |
| Underlying Diseases | |||
| No | 21,210 | 291 | 1.4 (1.22–1.54) |
| Yes | 5507 | 76 | 1.4 (1.09–1.72) |
| Close Contact with COVID-19 cases | |||
| No | 26,275 | 330 | 1.3 (1.12–1.40) |
| Yes | 442 | 37 | 8.3 (5.96–11.35) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahasirimongkol, S.; Uppapong, B.; Puangtubtim, W.; Dhepakson, P.; Panyajai, P.; Thawong, N.; Pinyosukhee, N.; Rojanawiwat, A.; Wichukchinda, N.; Soonthorncharttrawat, S.; et al. SARS-CoV-2 Seroprevalence in Unvaccinated Adults in Thailand in November 2021. Vaccines 2022, 10, 2169. https://doi.org/10.3390/vaccines10122169
Mahasirimongkol S, Uppapong B, Puangtubtim W, Dhepakson P, Panyajai P, Thawong N, Pinyosukhee N, Rojanawiwat A, Wichukchinda N, Soonthorncharttrawat S, et al. SARS-CoV-2 Seroprevalence in Unvaccinated Adults in Thailand in November 2021. Vaccines. 2022; 10(12):2169. https://doi.org/10.3390/vaccines10122169
Chicago/Turabian StyleMahasirimongkol, Surakameth, Ballang Uppapong, Wiroj Puangtubtim, Panadda Dhepakson, Parnuphan Panyajai, Naphatcha Thawong, Nadthanan Pinyosukhee, Archawin Rojanawiwat, Nuanjun Wichukchinda, Sakulrat Soonthorncharttrawat, and et al. 2022. "SARS-CoV-2 Seroprevalence in Unvaccinated Adults in Thailand in November 2021" Vaccines 10, no. 12: 2169. https://doi.org/10.3390/vaccines10122169
APA StyleMahasirimongkol, S., Uppapong, B., Puangtubtim, W., Dhepakson, P., Panyajai, P., Thawong, N., Pinyosukhee, N., Rojanawiwat, A., Wichukchinda, N., Soonthorncharttrawat, S., Larpardisorn, K., Amonyingcharoen, S., Juntaped, K., Chaiyakum, T., Tongkamsen, C., Srilaket, J., Chipatoom, J., Wichajarn, R., Chatchawankanpanich, N., ... Sirilak, S. (2022). SARS-CoV-2 Seroprevalence in Unvaccinated Adults in Thailand in November 2021. Vaccines, 10(12), 2169. https://doi.org/10.3390/vaccines10122169