

COVID-19 and Pulmonary Embolism Outcomes among Hospitalized Patients in the United States: A Propensity-Matched Analysis of National Inpatient Sample
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
- Patient: age, race (white, black, Hispanic, Native American, Asian, other), sex, insurance status (Medicare, Medicaid, private insurance, self-payment, no charge), median income based on patient’s zip code, and disposition.
- Hospital: location, teaching status, bed size, and region.
- Illness severity: length of stay (L.O.S.), mortality, hospitalization cost, comorbidities, mechanical ventilation, circulatory support, and vasopressor use.
- Intubation and mechanical ventilation;
- Vasopressor use;
- Length of stay, the financial burden on healthcare, and resource utilization.
Statistical Analysis
3. Results
3.1. Demographics and Baseline Comorbidities
3.2. In-Hospital Mortality
3.3. In-Hospital Complications
3.4. In-Hospital Quality Measures and Disposition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trends in Number of COVID-19 Cases and Deaths in the US Reported to CDC, by State/Territory. Centers for Disease Control and Prevention. 2022. Available online: https://covid.cdc.gov/ (accessed on 15 October 2022).
- Hanff, T.C.; Mohareb, A.M.; Giri, J.; Cohen, J.B.; Chirinos, J.A. Thrombosis in COVID-19. Am. J. Hematol. 2020, 95, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Giovini, M.; Leone, M.; Pizzilli, G.; Kortgen, A.; Bauer, M.; Tonetti, T.; Duclos, G.; Zieleskiewicz, L.; Buschbeck, S.; et al. Pulmonary embolism in patients with coronavirus disease-2019 (COVID-19) pneumonia: A narrative review. Ann. Intensiv. Care 2020, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Paz, L.; Talasaz, A.H.; Sadeghipour, P.; Potpara, T.S.; Aronow, H.D.; Jara-Palomares, L.; Sholzberg, M.; Angiolillo, D.J.; Lip, G.Y.; Bikdeli, B. COVID-19-Associated Pulmonary Embolism: Review of the Pathophysiology, Epidemiology, Prevention, Diagnosis, and Treatment. Semin. Thromb. Hemost. 2022. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.-Y.; Cheng, W.-W.; Mou, Z.-W.; Xiao, D.; Li, Y.-Y.; Li, Y.-J.; Li, W.-T.; Chen, Z.-M. Risk factors for pulmonary embolism in patients with COVID-19: A systemic review and meta-analysis. Int. J. Infect. Dis. 2021, 111, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.P.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis. Radiology 2021, 298, E70–E80. [Google Scholar] [CrossRef]
- Poor, H.D. Pulmonary Thrombosis and Thromboembolism in COVID-19. Chest 2021, 160, 1471–1480. [Google Scholar] [CrossRef]
- Roncon, L.; Zuin, M.; Barco, S.; Valerio, L.; Zuliani, G.; Zonzin, P.; Konstantinides, S.V. Incidence of acute pulmonary embolism in Patients with COVID-19: Systematic review and meta-analysis. Eur. J. Intern. Med. 2020, 82, 29–37. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Lagou, S.; Kontopantelis, E.; Stergiou, G.S.; Syrigos, K. Venous thromboembolism in COVID-19: A systematic review and meta-analysis. Vasc. Med. 2021, 26, 415–425. [Google Scholar] [CrossRef]
- Bilaloglu, S.; Aphinyanaphongs, Y.; Jones, S.; Iturrate, E.; Hochman, J.; Berger, J.S. Thrombosis in Hospitalized Patients with COVID-19 in a New York City Health System. JAMA 2020, 324, 799–801. [Google Scholar] [CrossRef]
- Scudiero, F.; Silverio, A.; Di Maio, M.; Russo, V.; Citro, R.; Personeni, D.; Cafro, A.; D’Andrea, A.; Attena, E.; Pezzullo, S.; et al. Pulmonary embolism in Patients with COVID-19: Prevalence, predictors and clinical outcome. Thromb. Res. 2021, 198, 34–39. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar]
- Miró, Ò.; Jiménez, S.; Mebazaa, A.; Freund, Y.; Burillo-Putze, G.; Martín, A.; Martín-Sánchez, F.J.; García-Lamberechts, E.J.; Alquézar-Arbé, A.; Jacob, J.; et al. Pulmonary embolism in patients with COVID-19: Incidence, risk factors, clinical characteristics, and outcome. Eur. Heart J. 2021, 42, 3127–3142. [Google Scholar] [CrossRef]
- Xu, H.; Martin, A.; Singh, A.; Narasimhan, M.; Lau, J.; Weinberg, M.; Jauhar, R.; Rao, G. Pulmonary Embolism in Patients Hospitalized with COVID-19 (From a New York Health System). Am. J. Cardiol. 2020, 133, 148–153. [Google Scholar] [CrossRef]
- de Cossio, S.; Paredes-Ruiz, D.; Gómez-Cuervo, C.; González-Olmedo, J.; Lalueza, A.; Revilla, Y.; Lumbreras, C.; Díaz-Pedroche, C. Clinical Differences and Outcomes of COVID-19 Associated Pulmonary Thromboembolism in Comparison with Non-COVID-19 Pulmonary Thromboembolism. J. Clin. Med. 2022, 11, 6011. [Google Scholar] [CrossRef]
- COVID-19 Vaccines. U.S. Department of Health & Human Services. Available online: https://www.hhs.gov/coronavirus/covid-19-vaccines/index.html (accessed on 15 October 2022).
- Law, N.; Chan, J.; Kelly, C.; Auffermann, W.F.; Dunn, D.P. Incidence of pulmonary embolism in COVID-19 infection in the ED: Ancestral, Delta, Omicron variants and vaccines. Emerg. Radiol. 2022, 29, 625–629. [Google Scholar] [CrossRef]
- Remap-Cap Investigators; ACTIV-4a Investigators; Attacc Investigators. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef]
- Health NIo. COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 17 October 2022).
- Sánchez-Recalde, Á.; Solano-López, J.; Miguelena-Hycka, J.; Martín-Pinacho, J.J.; Sanmartín, M.; Zamorano, J.L. COVID-19 and cardiogenic shock. Different cardiovascular presentations with high mortality. Rev. Esp. Cardiol. 2020, 73, 669–672. [Google Scholar] [CrossRef]
- Boukhris, M.; Hillani, A.; Moroni, F.; Annabi, M.S.; Addad, F.; Ribeiro, M.H.; Mansour, S.; Zhao, X.; Ybarra, L.F.; Abbate, A.; et al. Cardiovascular Implications of the COVID-19 Pandemic: A Global Perspective. Can. J. Cardiol. 2020, 36, 1068–1080. [Google Scholar] [CrossRef]
- Bompard, F.; Monnier, H.; Saab, I.; Tordjman, M.; Abdoul, H.; Fournier, L.; Sanchez, O.; Lorut, C.; Chassagnon, G.; Revel, M.-P. Pulmonary embolism in patients with COVID-19 pneumonia. Eur. Respir. J. 2020, 56, 2001365. [Google Scholar] [CrossRef]
- Fauvel, C.; Weizman, O.; Trimaille, A.; Mika, D.; Pommier, T.; Pace, N.; Douair, A.; Barbin, E.; Fraix, A.; Bouchot, O.; et al. Pulmonary embolism in Patients with COVID-19: A French multicentre cohort study. Eur. Heart J. 2020, 41, 3058–3068. [Google Scholar] [CrossRef]
- Mariani, S.; De Piero, M.E.; Ravaux, J.M.; Saelmans, A.; Kawczynski, M.J.; van Bussel, B.C.; Di Mauro, M.; Willers, A.; Swol, J.; Kowalewski, M.; et al. Temporary mechanical circulatory support for Patients with COVID-19: A systematic review of literature. Artif. Organs 2022, 46, 1249–1267. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Fujioka, H.; Yamada, N.; Nakano, T.; Sakuma, M.; Okada, O.; Kuriyama, M.D.T.; Nakanishi, M.D.N.; Miyahara, M.D.Y.; Kunieda, M.D.T.; et al. Clinical characteristics of acute pulmonary thromboembolism in Japan: Results of a multicenter registry in the japanese society of pulmonary embolism research. Clin. Cardiol. 2001, 24, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Poyiadji, N.; Cormier, P.; Patel, P.Y.; Hadied, M.O.; Bhargava, P.; Khanna, K.; Nadig, J.; Keimig, T.; Spizarny, D.; Reeser, N.; et al. Acute Pulmonary Embolism and COVID-19. Radiology 2020, 297, E335–E338. [Google Scholar] [CrossRef] [PubMed]
- Creel-Bulos, C.; Hockstein, M.; Amin, N.; Melhem, S.; Truong, A.; Sharifpour, M. Acute Cor Pulmonale in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2020, 382, e70. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- John, K.; Mishra, A.K.; Nayar, J.; Mehawej, J.; Lal, A. Coronavirus disease 2019 and mechanical circulatory support devices: A comprehensive review. Monaldi Arch. Chest Dis. 2022. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | COVID-19 without Pulmonary Embolism n (%) | COVID-19 with Pulmonary Embolism n (%) | p Value |
|---|---|---|---|
| n = 1,659,040 | 1,612,600 (97.2%) | 46,440 (2.8%) | |
| SEX (Female) | 789,368 (48.95%) | 19,064 (41.05%) | <0.001 |
| Mean age years (SD) | <0.001 | ||
| Male | 63.4 (16.3) | 62.92 (14.9) | |
| Female | 63.0 (18.9) | 65.68 (15.9) | |
| AGE GROUPS (%) | <0.001 | ||
| ≥18–29 | 80,953 (5.02%) | 1059 (2.28%) | |
| 30–49 | 271,562 (16.84%) | 7156 (15.41%) | |
| 50–69 | 597,791 (37.07%) | 19,890 (42.83%) | |
| ≥70 | 662,295 (41.07%) | 18,335 (39.48%) | |
| RACE (%) | <0.001 | ||
| Caucasians | 819,846 (50.84%) | 24,757 (53.31%) | |
| African American | 305,265 (18.93%) | 10,788 (23.23%) | |
| Hispanics | 348,644 (21.62%) | 7625 (16.42%) | |
| Asian or Pacific Islander | 52,732 (3.27%) | 1073 (2.31%) | |
| Native American | 16,610 (1.03%) | 418 (0.9%) | |
| Others | 69,342 (4.3%) | 1765 (3.8%) | |
| MEDIAN HOUSEHOLD INCOME (%) | <0.001 | ||
| <49,999$ | 550,542 (34.14%) | 15,423 (33.21%) | |
| 50,000–64,999$ | 438,143 (27.17%) | 13,073 (28.15%) | |
| 65,000–85,999$ | 357,352 (22.16%) | 10,286 (22.15%) | |
| >86,000$ | 266,563 (16.53%) | 7658 (16.49%) | |
| INSURANCE STATUS (%) | 0.003 | ||
| Medicare | 859,354 (53.29%) | 23,847 (51.35%) | |
| Medicaid | 245,599 (15.23%) | 5930 (12.77%) | |
| Private | 443,787 (27.52%) | 14,875 (32.03%) | |
| Self-pay | 63,859 (3.96%) | 1788 (3.85%) | |
| HOSPITAL DIVISION (%) | <0.001 | ||
| New England | 60,956 (3.78%) | 1904 (4.1%) | |
| Middle Atlantic | 235,762 (14.62%) | 6627 (14.27%) | |
| East North Central | 248,824 (15.43%) | 8972 (19.32%) | |
| West North Central | 108,044.2 (6.7%) | 3864 (8.32%) | |
| South Atlantic | 323,488 (20.06%) | 9362 (20.61%) | |
| East South Central | 108,205 (6.71%) | 3144 (6.77%) | |
| West South Central | 232,376 (14.41%) | 5224 (11.25%) | |
| Mountain | 111,269 (6.9%) | 3334 (7.18%) | |
| Pacific | 183,675 (11.39%) | 3799 (8.18%) | |
| HOSPITAL BEDSIZE (%) | <0.001 | ||
| Small | 393,474 (24.4%) | 10,124 (21.8%) | |
| Medium | 46,733 (28.98%) | 13,570 (29.22%) | |
| Large | 751,633 (46.61%) | 22,746 (48.98%) | |
| HOSPTAL TEACHING STATUS (%) | <0.001 | ||
| Rural | 158,196 (9.81%) | 4458 (9.6%) | |
| Urban non-teaching | 301,556 (18.7%) | 7950 (17.12%) | |
| Urban teaching | 1,152,848 (71.49%) | 34,031 (73.28%) | |
| COMORBIDITIES (%) | |||
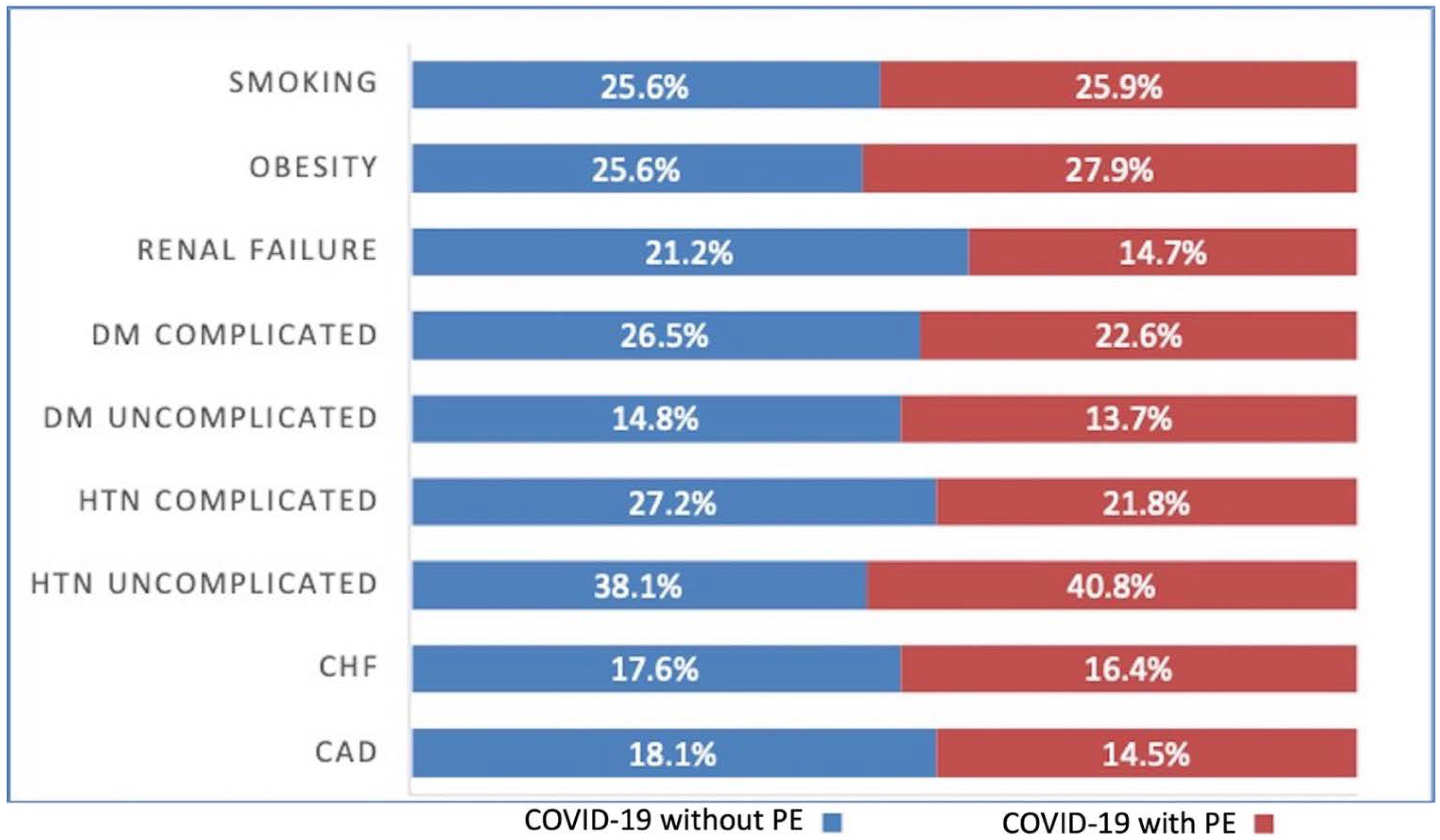
| CAD | 291,236 (18.06%) | 6715 (14.46%) | <0.001 |
| CHF | 283,818 (17.6%) | 7611 (16.39%) | 0.002 |
| HTN uncomplicated | 613,594(38.05%) | 18,952 (40.81%) | <0.001 |
| HTN complicated | 438,788 (27.21%) | 10,110 (21.77%) | <0.001 |
| DM uncomplicated | 238,181 (14.77%) | 6362 (13.7%) | 0.004 |
| DM complicated | 426,694 (26.46%) | 10,509 (22.63%) | <0.001 |
| Renal failure | 342,194 (21.22%) | 6827 (14.7%) | <0.001 |
| Chronic pulmonary disease | 354,933 (22.01%) | 10,040 (21.62%) | 0.38 |
| Obesity | 412,342 (25.57%) | 12,961 (27.91%) | <0.001 |
| Smoking | 412,664 (25.59%) | 12,014 (25.87%) | 0.56 |
| Characteristics | COVID-19 without Pulmonary Embolism | COVID-19 with Pulmonary Embolism | p Value |
|---|---|---|---|
| PE (83,950) | n = 41,975 | n = 41,975 | |
| SEX (Female) | 17,684 (42.13%) | 17,684 (42.18%) | 0.95 |
| Mean age years (SD) | 64.50 (13.99) | 64.45 (14.03) | 0.87 |
| AGE GROUPS (%) | 0.97 | ||
| ≥18–29 | 940 (2.24%) | 978 (2.33%) | |
| 30–49 | 6170 (14.70%) | 6149 (14.65%) | |
| 50–69 | 17,835 (42.49%) | 17,856 (42.54%) | |
| ≥70 | 17,029 (40.57%) | 16,991 (40.48%) | |
| RACE (%) | 0.99 | ||
| Caucasians | 22,641 (53.94%) | 2267 (54.02%) | |
| African American | 9684 (23.07%) | 9696 (23.10%) | |
| Hispanics | 6804 (16.21%) | 6833 (16.28%) | |
| Asian or Pacific Islander | 995 (2.37%) | 949 (2.26%) | |
| Native American | 332 (0.79%) | 294 (0.70%) | |
| Others | 1519 (3.62%) | 1524 (3.63%) | |
| MEDIAN HOUSEHOLD INCOME (%) | 1 | ||
| <49,999$ | 13,810 (32.90%) | 13,801 (32.88%) | |
| 50,000–64,999$ | 11,690 (27.85%) | 11,711 (27.90%) | |
| 65,000–85,999$ | 9390 (22.37%) | 9394 (22.38%) | |
| >86,000$ | 7085 (16.88%) | 7069 (16.84%) | |
| INSURANCE STATUS (%) | 0.99 | ||
| Medicare | 21,638 (51.55%) | 21,621 (51.51%) | |
| Medicaid | 5293 (12.61%) | 5327 (12.69%) | |
| Private | 13,436 (32.01%) | 13,461 (32.07%) | |
| Self-pay | 1603 (3.82%) | 1570 (3.74%) | |
| HOSPITAL DIVISION (%) | <0.001 | ||
| New England | 1742 (4.15%) | 24,329 (57.96%) | |
| Middle Atlantic | 6271 (14.94%) | 15,606 (37.18%) | |
| East North Central | 8370 (19.94%) | 1184 (2.82%) | |
| West North Central | 3077 (7.33%) | 218 (0.52%) | |
| South Atlantic | 8525 (20.31%) | 365 (0.87%) | |
| East South Central | 2909 (6.93%) | 504 (1.20%) | |
| West South Central | 4596 (10.95%) | 101 (0.24%) | |
| Mountain | 3026 (7.21%) | 109 (0.26%) | |
| Pacific | 3463 (8.25%) | 55 (0.13%) | |
| HOSPITAL BEDSIZE (%) | <0.001 | ||
| Small | 9134 (21.76%) | 12,836 (30.58%) | |
| Medium | 12,265 (29.22%) | 13,969 (33.28%) | |
| Large | 20,576 (49.02%) | 15,170 (36.14%) | |
| HOSPTAL TEACHING STATUS (%) | <0.001 | ||
| Rural | 3874 (9.23%) | 1943 (4.63%) | |
| Urban non-teaching | 7312 (17.42%) | 4814 (11.47%) | |
| Urban teaching | 30,789 (73.35%) | 35,217 (83.90%) |
| Variable | COVID-19 with Pulmonary Embolism | COVID-19 without Pulmonary Embolism | p Value |
|---|---|---|---|
| Disposition | <0.001 | ||
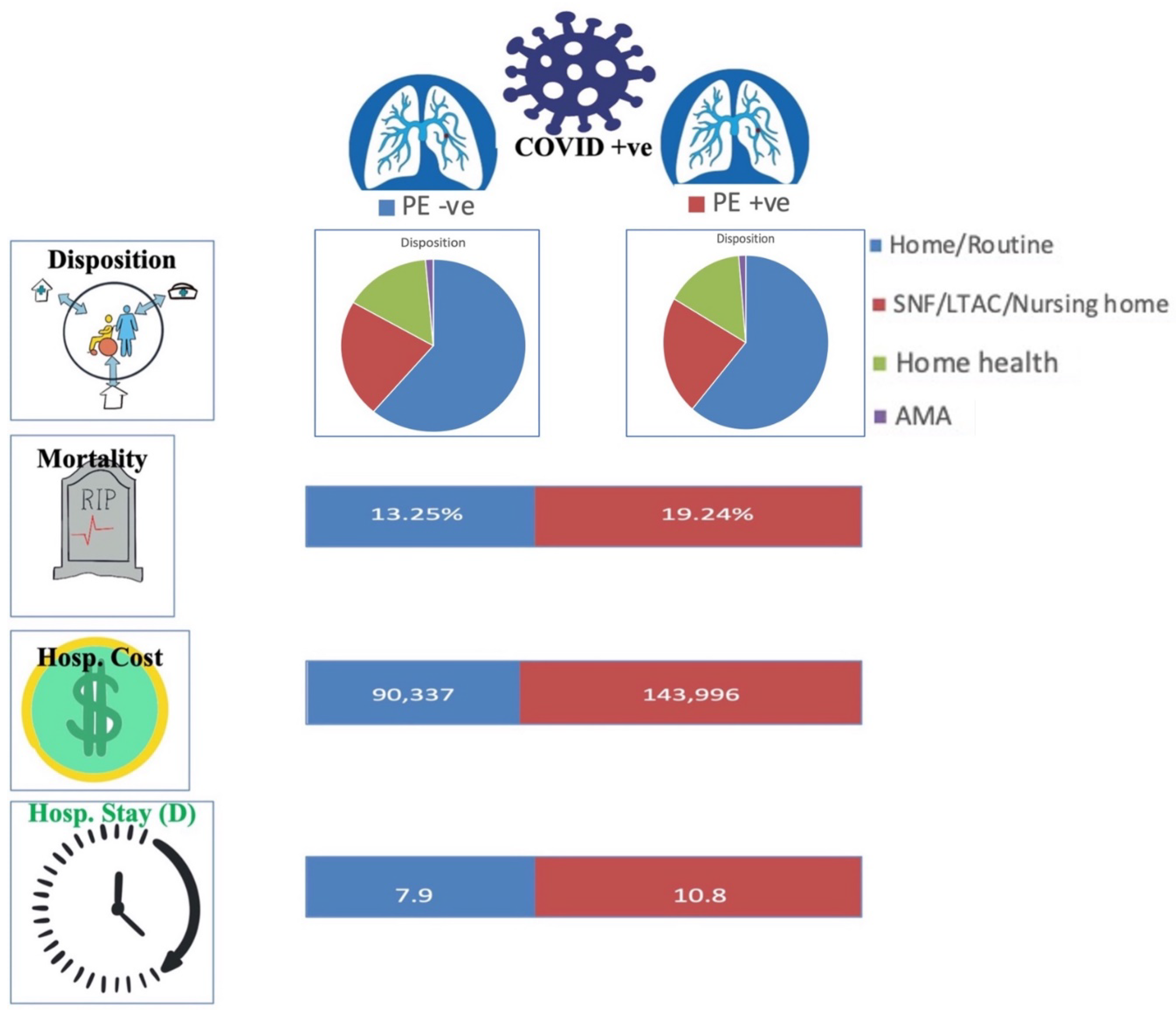
| Home/Routine | 26,076 (56.15%) | 986,750 (61.19%) | |
| SNF/LTAC/Nursing home | 11,020 (23.73%) | 357,191 (22.15%) | |
| Home health | 9019 (19.42%) | 246,566.54 (15.29%) | |
| AMA | 325 (0.7%) | 22,093 (1.37%) | |
| Vasopressor use | 2508 (5.4%) | 41,444 (2.57%) | |
| Adjusted odds ratio 1 1.62 (95% CI 1.45–1.81) | <0.001 | ||
| Mechanical ventilation | 11,926 (25.68%) | 251,888 (15.62%) | |
| Adjusted odds ratio 1 1.44 (95% CI 1.36–1.52) | <0.001 | ||
| Sudden Cardiac Arrest | 2322 (5%) | 43,056 (2.67%) | <0.001 |
| Adjusted odds ratio 1 1.53 (95% CI 1.38–1.70) | |||
| Cardiogenic Shock (%) | 827 (1.78%) | 9514 (0.59%) | |
| Adjusted odds ratio 1 2.15 (95% CI 1.80–2.57) | <0.001 | ||
| Mechanical Circulatory Support (%) (LVAD or pVAD or ECMO) | 385 (0.83%) | 4193 (0.26%) | |
| Adjusted odds ratio 1 2.03 (95% CI 1.53–2.69) | <0.001 | ||
| In-hospital mortality (n = 222,490) (%) | 8935 (19.24%) | 213,555 (13.25%) | |
| Adjusted odds ratio 1 1.36 (95% CI 1.28–1.45) | <0.001 | ||
| Mean total hospitalization charge ($) | 143,996$ | 90,337$ | |
| Adjusted total charge 1 38,907$ higher | <0.001 | ||
| Mean length of stay (days) | 10.8 (10.5–11.1) | 7.9 (7.8–8.0) | |
| Adjusted length of stay 1 1.9 day higher | <0.001 | ||
| Variable | COVID-19 with Pulmonary Embolism | COVID-19 without Pulmonary Embolism | p Value |
|---|---|---|---|
| Total died (222,490) | 8935 | 213,555 | |
| SEX (%) | <0.001 | ||
| Male | 5663 (63.38%) | 124,417 (58.%) | |
| Female | 3272 (36.62%) | 89,138 (41.7%) | |
| AGE GROUPS (%) | |||
| ≥18–29 | 70 (0.78%) | 1260 (0.59%) | 0.30 |
| 30–49 | 730 (8.17%) | 10,251 (4.8%) | <0.001 |
| 50–69 | 3527 (39.47%) | 64,387 (30.1%) | <0.001 |
| ≥70 | 4608 (51.57%) | 137,658 (64.%) | <0.001 |
| RACE (%) | |||
| Caucasians | 4273 (47.82%) | 110,280 (51.%) | 0.004 |
| African American | 1661 (18.59%) | 35,877 (16.8%) | 0.05 |
| Hispanics | 1876 (21%) | 41,707 (19.5%) | 0.19 |
| Asian or Pacific Islander | 240 (2.69%) | 7218 (3.38%) | 0.13 |
| Native American | 130 (1.46%) | 2584 (1.21%) | 0.41 |
| Others | 385 (4.31%) | 9418 (4.41%) | 0.85 |
| HOSPTAL TEACHING STATUS (%) | |||
| Rural | 566 (6.33%) | 16,849 (7.89%) | 0.03 |
| Urban non-teaching | 1316 (14.73%) | 38,162 (17.8%) | 0.002 |
| Urban teaching | 7054 (78.95%) | 158,565 (74%) | <0.001 |
| Variable | COVID-19 with Pulmonary Embolism | COVID-19 without Pulmonary Embolism | p Value |
|---|---|---|---|
| Disposition | <0.001 | ||
| Home/Routine | 23,141 (55.13%) | 22,138 (52.74%) | |
| SNF/LTAC/Nursing home | 10,238 (24.39%) | 10,892 (25.95%) | |
| Home health | 8303 (19.78%) | 8370 (19.94%) | |
| AMA | 298 (0.71%) | 575 (1.37%) | |
| Vasopressor use (%) | 2246 (5.35%) | 1587 (3.78%) | |
| Adjusted odds ratio 1 1.79 (95% CI 1.41–2.28) | <0.001 | ||
| Mechanical ventilation (%) | 10,569 (25.18%) | 6834 (16.28%) | |
| Adjusted odds ratio 1 1.55 (95% CI 1.36–1.76) | <0.001 | ||
| Sudden Cardiac Arrest (%) | 2099 (5%) | 1007 (2.4%) | |
| Adjusted odds ratio 1 1.44 (95% CI 1.11–1.88) | 0.006 | ||
| Cardiogenic Shock (%) | 756 (1.8%) | 252 (0.6%) | |
| Adjusted odds ratio 1 3.1 (95% CI 2.02–4.75) | <0.001 | ||
| Mechanical Circulatory Support (%) (LVAD or pVAD or ECMO) | 344 (0.82%) | 126 (0.3%) | |
| Adjusted odds ratio 1 3.1 (95% CI 1.67–5.76) | <0.001 | ||
| In-hospital mortality (%) (n = 13,865) | 8014 (19.09%) | 5851 (13.94%) | |
| Adjusted odds ratio 1 1.29 (95% CI 1.13–1.47) | <0.001 | ||
| Mean total hospitalization charge ($) | 143,705$ | 78,407$ | |
| Adjusted total charge 1 52,024$ higher | <0.001 | ||
| Mean length of stay (days) | 10.8 | 8.4 | |
| Adjusted length of stay 1 2.3 day higher | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasrullah, A.; Gangu, K.; Shumway, N.B.; Cannon, H.R.; Garg, I.; Shuja, H.; Bobba, A.; Chourasia, P.; Sheikh, A.B.; Shekhar, R. COVID-19 and Pulmonary Embolism Outcomes among Hospitalized Patients in the United States: A Propensity-Matched Analysis of National Inpatient Sample. Vaccines 2022, 10, 2104. https://doi.org/10.3390/vaccines10122104
Nasrullah A, Gangu K, Shumway NB, Cannon HR, Garg I, Shuja H, Bobba A, Chourasia P, Sheikh AB, Shekhar R. COVID-19 and Pulmonary Embolism Outcomes among Hospitalized Patients in the United States: A Propensity-Matched Analysis of National Inpatient Sample. Vaccines. 2022; 10(12):2104. https://doi.org/10.3390/vaccines10122104
Chicago/Turabian StyleNasrullah, Adeel, Karthik Gangu, Nichole B. Shumway, Harmon R. Cannon, Ishan Garg, Hina Shuja, Aniesh Bobba, Prabal Chourasia, Abu Baker Sheikh, and Rahul Shekhar. 2022. "COVID-19 and Pulmonary Embolism Outcomes among Hospitalized Patients in the United States: A Propensity-Matched Analysis of National Inpatient Sample" Vaccines 10, no. 12: 2104. https://doi.org/10.3390/vaccines10122104
APA StyleNasrullah, A., Gangu, K., Shumway, N. B., Cannon, H. R., Garg, I., Shuja, H., Bobba, A., Chourasia, P., Sheikh, A. B., & Shekhar, R. (2022). COVID-19 and Pulmonary Embolism Outcomes among Hospitalized Patients in the United States: A Propensity-Matched Analysis of National Inpatient Sample. Vaccines, 10(12), 2104. https://doi.org/10.3390/vaccines10122104