

Vaccine-Related Autoimmune Hepatitis: Emerging Association with SARS-CoV-2 Vaccination or Coincidence?

 , , ,
, , ,
Abstract
1. Introduction
2. Autoimmune Hepatitis and Its Association with Vaccination
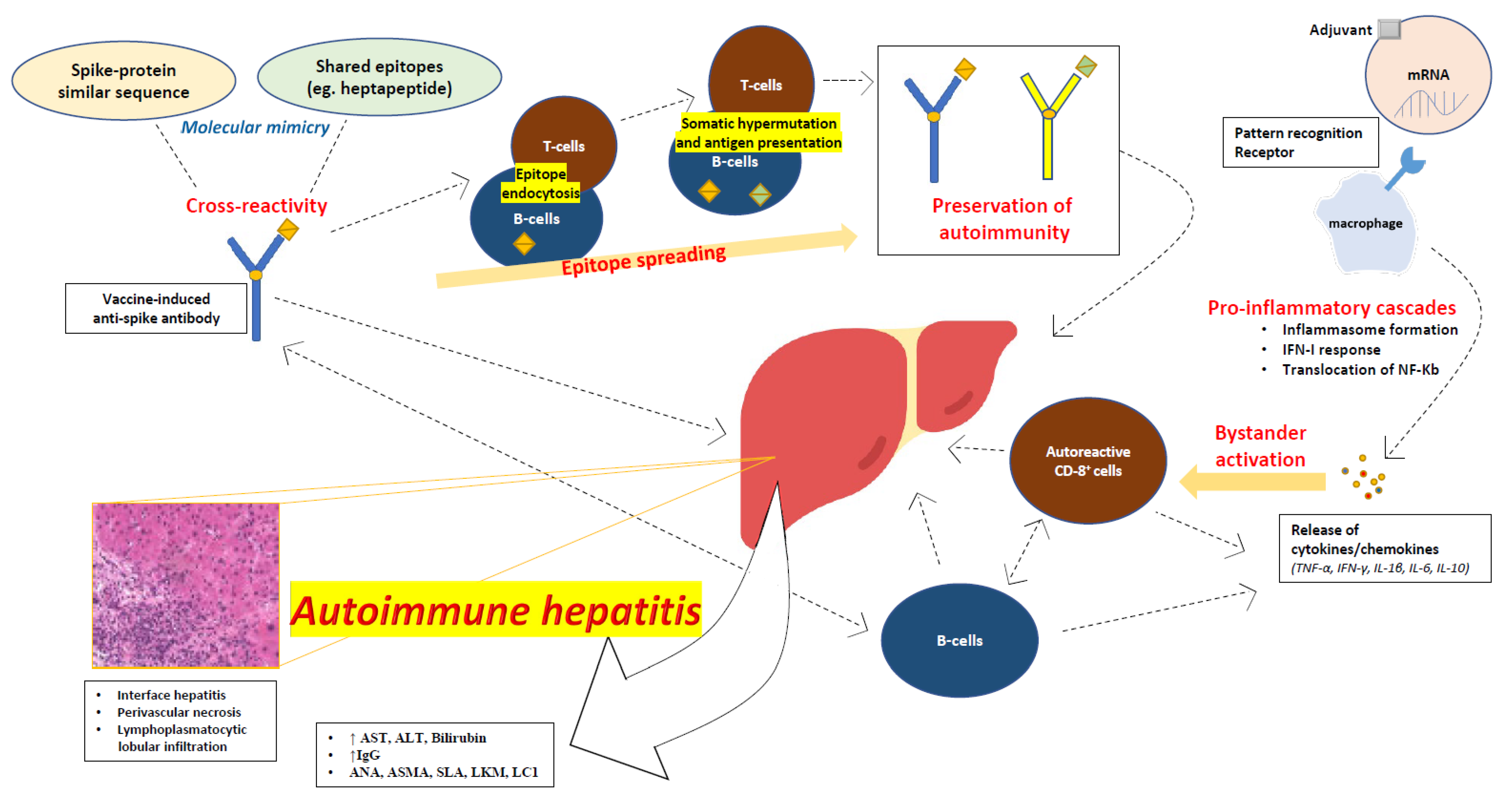
3. Proposed Mechanisms of Autoimmune Hepatitis following SARS-CoV-2 Vaccination
3.1. Molecular Mimicry
3.2. Autoimmune/Inflammatory Syndrome Caused by Adjuvants
3.3. Direct mRNA Effects
3.4. Bystander Hepatitis and Autoreactive Lymphocytes
3.5. Epitope Spreading Hypothesis
3.6. Overt Autoimmunity Triggered by Vaccination
4. Reported Cases of Autoimmune Hepatitis following SARS-CoV-2 Vaccination
4.1. Demographic Data and Concurrent Diseases
4.2. Vaccination History
4.3. Clinical Presentation
4.4. Laboratory Investigation
4.5. Liver Histology
4.6. Management and Outcomes
4.7. Evidence from Excluded Studies and Reports
5. Causal Association or Coincidence?
5.1. Simplified Diagnostic Criteria for Autoimmune Hepatitis Diagnosis
5.2. Naranjo Score for Adverse Drug Reactions for Vaccination Causality
5.3. Definite Cases of Autoimmune Hepatitis Associated with SARS-CoV-2 Vaccination
6. Variable Phenotypes of Autoimmune Hepatitis following SARS-CoV-2 Vaccination
6.1. Immune-Mediated Drug-Induced Liver Injury following SARS-CoV-2 Vaccination
6.2. Flare of Pre-Existing Autoimmune Hepatitis following SARS-CoV-2 Vaccination
6.3. New-Onset Autoimmune Hepatitis following SARS-CoV-2 Vaccination
6.4. Mixed Autoimmune Type of Hepatitis following SARS-CoV-2 Vaccination
7. Discussion
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FDA. Approves First COVID-19 Vaccine; FDA: Silver Spring, MD, USA, 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine (accessed on 28 September 2022).
- Yesudhas, D.; Srivastava, A.; Gromiha, M.M. COVID-19 outbreak: History, mechanism, transmission, structural studies and therapeutics. Infection 2021, 49, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.P.; Chen, Y.; Dave, J.; Chen, Z.S.; Chauhan, S.C.; Yallapu, M.M.; Uversky, V.N.; Bezbaruah, R.; Patel, S.; Apostolopoulos, V. COVID-19 and vaccination: Myths vs. science. Expert. Rev. Vaccines 2022, 21, 1603–1620. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 28 September 2022).
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef] [PubMed]
- CDC Selected Adverse Events Reported after COVID-19 Vaccination. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html (accessed on 28 September 2022).
- Coronavirus Vaccine-Summary of Yellow Card Reporting. Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 28 September 2022).
- Mieli-Vergani, G.; Vergani, D.; Czaja, A.J.; Manns, M.P.; Krawitt, E.L.; Vierling, J.M.; Lohse, A.W.; Montano-Loza, A.J. Autoimmune hepatitis. Nat. Rev. Dis. Primers 2018, 4, 18017. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, E.; Talwalkar, J.; Treeprasertsuk, S.; Kamath, P.S.; Takahashi, N.; Sanderson, S.; Neuhauser, M.; Lindor, K. Drug-induced autoimmune hepatitis: Clinical characteristics and prognosis. Hepatology 2010, 51, 2040–2048. [Google Scholar] [CrossRef]
- Della Corte, C.; Carlucci, A.; Francalanci, P.; Alisi, A.; Nobili, V. Autoimmune hepatitis type 2 following anti-papillomavirus vaccination in a 11-year-old girl. Vaccine 2011, 29, 4654–4656. [Google Scholar] [CrossRef]
- Perumalswami, P.; Peng, L.; Odin, J.A. Vaccination as a triggering event for autoimmune hepatitis. Semin. Liver Dis. 2009, 29, 331–334. [Google Scholar] [CrossRef]
- Muratori, P.; Serio, I.; Lalanne, C.; Lenzi, M. Development of autoimmune hepatitis after influenza vaccination; trigger or killer? Clin. Res. Hepatol. Gastroenterol. 2019, 43, e95–e96. [Google Scholar] [CrossRef]
- Sasaki, T.; Suzuki, Y.; Ishida, K.; Kakisaka, K.; Abe, H.; Sugai, T.; Takikawa, Y. Autoimmune hepatitis following influenza virus vaccination: Two case reports. Medicine 2018, 97, e11621. [Google Scholar] [CrossRef]
- Berry, P.A.; Smith-Laing, G. Hepatitis A vaccine associated with autoimmune hepatitis. World J. Gastroenterol. 2007, 13, 2238–2239. [Google Scholar] [CrossRef]
- van Gemeren, M.A.; van Wijngaarden, P.; Doukas, M.; de Man, R.A. Vaccine-related autoimmune hepatitis: The same disease as idiopathic autoimmune hepatitis? Two clinical reports and review. Scand. J. Gastroenterol. 2017, 52, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Csepregi, A.; Treiber, G.; Rocken, C.; Malfertheiner, P. Acute exacerbation of autoimmune hepatitis induced by Twinrix. World J. Gastroenterol. 2005, 11, 4114–4116. [Google Scholar] [CrossRef] [PubMed]
- Beer, A.; Dienes, H.P. Autoimmune hepatitis-is histology conclusive? Ann. Transl. Med. 2021, 9, 733. [Google Scholar] [CrossRef] [PubMed]
- Palle, S.K.; Naik, K.B.; McCracken, C.E.; Kolachala, V.L.; Romero, R.; Gupta, N.A. Racial disparities in presentation and outcomes of paediatric autoimmune hepatitis. Liver Int. 2019, 39, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.J.; Dinh, H.; Arenovich, T.; Marcus, V.A.; Wanless, I.R.; Heathcote, E.J. Autoimmune hepatitis: Effect of symptoms and cirrhosis on natural history and outcome. Hepatology 2005, 42, 53–62. [Google Scholar] [CrossRef]
- Puustinen, L.; Barner-Rasmussen, N.; Pukkala, E.; Farkkila, M. Incidence, prevalence, and causes of death of patients with autoimmune hepatitis: A nationwide register-based cohort study in Finland. Dig. Liver Dis. 2019, 51, 1294–1299. [Google Scholar] [CrossRef]
- Theocharidou, E.; Heneghan, M.A. Current and future perspectives in autoimmune hepatitis. Br. J. Hosp. Med. 2018, 79, 151–159. [Google Scholar] [CrossRef]
- Liberal, R.; Krawitt, E.L.; Vierling, J.M.; Manns, M.P.; Mieli-Vergani, G.; Vergani, D. Cutting edge issues in autoimmune hepatitis. J. Autoimmun. 2016, 75, 6–19. [Google Scholar] [CrossRef]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.; Czaja, A.J.; Desmet, V.J.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef]
- Hennes, E.M.; Zeniya, M.; Czaja, A.J.; Pares, A.; Dalekos, G.N.; Krawitt, E.L.; Bittencourt, P.L.; Porta, G.; Boberg, K.M.; Hofer, H.; et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008, 48, 169–176. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef] [PubMed]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef] [PubMed]
- Weiler-Normann, C.; Schramm, C. Drug induced liver injury and its relationship to autoimmune hepatitis. J. Hepatol. 2011, 55, 747–749. [Google Scholar] [CrossRef] [PubMed]
- Chow, K.W.; Pham, N.V.; Ibrahim, B.M.; Hong, K.; Saab, S. Autoimmune Hepatitis-Like Syndrome Following COVID-19 Vaccination: A Systematic Review of the Literature. Dig. Dis. Sci. 2022, 67, 4574–4580. [Google Scholar] [CrossRef]
- Roy, A.; Verma, N.; Singh, S.; Pradhan, P.; Taneja, S.; Singh, M. Immune-mediated liver injury following COVID-19 vaccination: A systematic review. Hepatol. Commun. 2022, 6, 2513–2522. [Google Scholar] [CrossRef]
- Alhumaid, S.; Al Mutair, A.; Rabaan, A.A.; FM, A.L.; Choudhary, O.P.; Yong, S.J.; Nainu, F.; Khan, A.; Muhammad, J.; Alhelal, F.; et al. New-onset and relapsed liver diseases following COVID-19 vaccination: A systematic review. BMC Gastroenterol. 2022, 22, 433. [Google Scholar] [CrossRef]
- WHO. VigiAccess, SARS-CoV-2 Vaccine Reported Potential Side Affects. Available online: https://vigiaccess.org (accessed on 28 September 2022).
- Vergani, D.; Choudhuri, K.; Bogdanos, D.P.; Mieli-Vergani, G. Pathogenesis of autoimmune hepatitis. Clin. Liver Dis. 2002, 6, 727–737. [Google Scholar] [CrossRef]
- Goldberg, A.C.; Bittencourt, P.L.; Mougin, B.; Cancado, E.L.; Porta, G.; Carrilho, F.; Kalil, J. Analysis of HLA haplotypes in autoimmune hepatitis type 1: Identifying the major susceptibility locus. Hum. Immunol. 2001, 62, 165–169. [Google Scholar] [CrossRef]
- Miyakawa, H.; Kitazawa, E.; Kikuchi, K.; Fujikawa, H.; Kawaguchi, N.; Abe, K.; Matsushita, M.; Matsushima, H.; Igarashi, T.; Hankins, R.W.; et al. Immunoreactivity to various human cytochrome P450 proteins of sera from patients with autoimmune hepatitis, chronic hepatitis B, and chronic hepatitis C. Autoimmunity 2000, 33, 23–32. [Google Scholar] [CrossRef]
- Michel, G.; Ritter, A.; Gerken, G.; Meyer zum Buschenfelde, K.H.; Decker, R.; Manns, M.P. Anti-GOR and hepatitis C virus in autoimmune liver diseases. Lancet 1992, 339, 267–269. [Google Scholar] [CrossRef]
- Lunel, F.; Abuaf, N.; Frangeul, L.; Grippon, P.; Perrin, M.; Le Coz, Y.; Valla, D.; Borotto, E.; Yamamoto, A.M.; Huraux, J.M.; et al. Liver/kidney microsome antibody type 1 and hepatitis C virus infection. Hepatology 1992, 16, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Crispe, I.N. Liver antigen-presenting cells. J. Hepatol. 2011, 54, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimkhani, M.R.; Mohar, I.; Crispe, I.N. Cross-presentation of antigen by diverse subsets of murine liver cells. Hepatology 2011, 54, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Kanduc, D.; Shoenfeld, Y. On the molecular determinants of the SARS-CoV-2 attack. Clin. Immunol. 2020, 215, 108426. [Google Scholar] [CrossRef] [PubMed]
- Ehrenfeld, M.; Tincani, A.; Andreoli, L.; Cattalini, M.; Greenbaum, A.; Kanduc, D.; Alijotas-Reig, J.; Zinserling, V.; Semenova, N.; Amital, H.; et al. Covid-19 and autoimmunity. Autoimmun. Rev. 2020, 19, 102597. [Google Scholar] [CrossRef]
- Vojdani, A.; Kharrazian, D. Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases. Clin. Immunol. 2020, 217, 108480. [Google Scholar] [CrossRef]
- Shoenfeld, Y.; Agmon-Levin, N. ‘ASIA’-autoimmune/inflammatory syndrome induced by adjuvants. J. Autoimmun. 2011, 36, 4–8. [Google Scholar] [CrossRef]
- Agmon-Levin, N.; Paz, Z.; Israeli, E.; Shoenfeld, Y. Vaccines and autoimmunity. Nat. Rev. Rheumatol. 2009, 5, 648–652. [Google Scholar] [CrossRef]
- Talotta, R. Do COVID-19 RNA-based vaccines put at risk of immune-mediated diseases? In reply to “potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases”. Clin. Immunol. 2021, 224, 108665. [Google Scholar] [CrossRef]
- AstraZeneca, C.-V. Summary of Product Characteristis (SPC); EMA: Amsterdam, The Netherlands, 2021.
- Kabacam, G.; Wahlin, S.; Efe, C. Autoimmune hepatitis triggered by COVID-19: A report of two cases. Liver Int. 2021, 41, 2527–2528. [Google Scholar] [CrossRef]
- Rodriguez, Y.; Novelli, L.; Rojas, M.; De Santis, M.; Acosta-Ampudia, Y.; Monsalve, D.M.; Ramirez-Santana, C.; Costanzo, A.; Ridgway, W.M.; Ansari, A.A.; et al. Autoinflammatory and autoimmune conditions at the crossroad of COVID-19. J. Autoimmun. 2020, 114, 102506. [Google Scholar] [CrossRef] [PubMed]
- Boettler, T.; Csernalabics, B.; Salie, H.; Luxenburger, H.; Wischer, L.; Salimi Alizei, E.; Zoldan, K.; Krimmel, L.; Bronsert, P.; Schwabenland, M.; et al. SARS-CoV-2 vaccination can elicit a CD8 T-cell dominant hepatitis. J. Hepatol. 2022, 77, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Powell, A.M.; Black, M.M. Epitope spreading: Protection from pathogens, but propagation of autoimmunity? Clin. Exp. Dermatol. 2001, 26, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Cornaby, C.G.L.; Mayhew, V.; Sloan, C.S.; Welling, A.; Poole, B.D. B cell epitope spreading: Mechanisms and contribution to autoimmune diseas. Immunol. Lett. 2015, 163, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Akinosoglou, K.; Tzivaki, I.; Marangos, M. Covid-19 vaccine and autoimmunity: Awakening the sleeping dragon. Clin. Immunol. 2021, 226, 108721. [Google Scholar] [CrossRef]
- Izagirre, A.; Arzallus, T.; Garmendia, M.; Torrente, S.; Castiella, A.; Zapata, E.M. Autoimmune hepatitis following COVID-19 vaccination. J. Autoimmun. 2022, 132, 102874. [Google Scholar] [CrossRef]
- Torrente, S.; Castiella, A.; Garmendia, M.; Zapata, E. Probable autoimmune hepatitis reactivated after COVID-19 vaccination. Gastroenterol. Hepatol. 2022, 45 (Suppl. 1), 115–116. [Google Scholar] [CrossRef]
- Barary, M.; Sharifi-Razavi, A.; Rakhshani, N.; Sio, T.T.; Ebrahimpour, S.; Baziboroun, M. Fulminant hepatitis following COVID-19 vaccination: A case report. Clin. Case Rep. 2022, 10, e6066. [Google Scholar] [CrossRef]
- Mekritthikrai, K.; Jaru-Ampornpan, P.; Komolmit, P.; Thanapirom, K. Autoimmune Hepatitis Triggered by COVID-19 Vaccine: The First Case From Inactivated Vaccine. ACG Case Rep. J. 2022, 9, e00811. [Google Scholar] [CrossRef]
- Brubaker, J.E.D.; Casaccio, C.L.; Brazeau, M.J. Recurrence of AutoimmuneHepatitisAfter COVID-19Vaccination. Cureus 2022, 14, e25339. [Google Scholar] [CrossRef]
- Shahrani, S.; Sooi, C.Y.; Hilmi, I.N.; Mahadeva, S. Autoimmune hepatitis (AIH) following coronavirus (COVID-19) vaccine-No longer exclusive to mRNA vaccine? Liver Int. 2022, 42, 2344–2345. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, N.; Matsuoka, R.; Ishikawa, N.; Endo, M.; Terasaki, M.; Seo, E.; Tsuchiya, K. Autoimmune hepatitis with history of HCV treatment triggered by COVID-19 vaccination: Case report and literature review. Clin. J. Gastroenterol. 2022, 15, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Lasagna, A.; Lenti, M.V.; Cassaniti, I.; Sacchi, P. Development of hepatitis triggered by SARS-CoV-2 vaccination in patient with cancer during immunotherapy: A case report. Immunotherapy 2022, 14, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Pinazo-Bandera, J.M.; Hernandez-Albujar, A.; Garcia-Salguero, A.I.; Arranz-Salas, I.; Andrade, R.J.; Robles-Diaz, M. Acute hepatitis with autoimmune features after COVID-19 vaccine: Coincidence or vaccine-induced phenomenon? Gastroenterol. Rep. 2022, 10, goac014. [Google Scholar] [CrossRef]
- Kang, S.H.; Kim, M.Y.; Cho, M.Y.; Baik, S.K. Autoimmune Hepatitis Following Vaccination for SARS-CoV-2 in Korea: Coincidence or Autoimmunity? J. Korean Med. Sci. 2022, 37, e116. [Google Scholar] [CrossRef]
- Ghorbani, H.; Rouhi, T.; Vosough, Z.; Shokri-Shirvani, J. Drug-induced hepatitis after Sinopharm COVID-19 vaccination: A case study of a 62-year-old patient. Int. J. Surg. Case Rep. 2022, 93, 106926. [Google Scholar] [CrossRef]
- Fimiano, F.; D’Amato, D.; Gambella, A.; Marzano, A.; Saracco, G.M.; Morgando, A. Autoimmune hepatitis or drug-induced autoimmune hepatitis following Covid-19 vaccination? Liver Int. 2022, 42, 1204–1205. [Google Scholar] [CrossRef]
- Camacho-Dominguez, L.; Rodriguez, Y.; Polo, F.; Restrepo Gutierrez, J.C.; Zapata, E.; Rojas, M.; Anaya, J.M. COVID-19 vaccine and autoimmunity. A new case of autoimmune hepatitis and review of the literature. J. Transl. Autoimmun. 2022, 5, 100140. [Google Scholar] [CrossRef]
- Erard, D.; Villeret, F.; Lavrut, P.M.; Dumortier, J. Autoimmune hepatitis developing after COVID 19 vaccine: Presumed guilty? Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101841. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kakisaka, K.; Takikawa, Y. Letter to the editor: Autoimmune hepatitis after COVID-19 vaccination: Need for population-based epidemiological study. Hepatology 2022, 75, 759–760. [Google Scholar] [CrossRef]
- Cao, Z.; Gui, H.; Sheng, Z.; Xin, H.; Xie, Q. Letter to the editor: Exacerbation of autoimmune hepatitis after COVID-19 vaccination. Hepatology 2022, 75, 757–759. [Google Scholar] [CrossRef] [PubMed]
- Avci, E.; Abasiyanik, F. Autoimmune hepatitis after SARS-CoV-2 vaccine: New-onset or flare-up? J. Autoimmun. 2021, 125, 102745. [Google Scholar] [CrossRef] [PubMed]
- Garrido, I.; Lopes, S.; Simoes, M.S.; Liberal, R.; Lopes, J.; Carneiro, F.; Macedo, G. Autoimmune hepatitis after COVID-19 vaccine-more than a coincidence. J. Autoimmun. 2021, 125, 102741. [Google Scholar] [CrossRef] [PubMed]
- Palla, P.; Vergadis, C.; Sakellariou, S.; Androutsakos, T. Letter to the editor: Autoimmune hepatitis after COVID-19 vaccination: A rare adverse effect? Hepatology 2022, 75, 489–490. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Fronhoffs, F.; Dold, L.; Strassburg, C.P.; Weismuller, T.J. New-onset autoimmune hepatitis following mRNA COVID-19 vaccination in a 36-year-old woman with primary sclerosing cholangitis-should we be more vigilant? J. Hepatol. 2022, 76, 218–220. [Google Scholar] [CrossRef]
- Ghielmetti, M.; Schaufelberger, H.D.; Mieli-Vergani, G.; Cerny, A.; Dayer, E.; Vergani, D.; Terziroli Beretta-Piccoli, B. Acute autoimmune-like hepatitis with atypical anti-mitochondrial antibody after mRNA COVID-19 vaccination: A novel clinical entity? J. Autoimmun. 2021, 123, 102706. [Google Scholar] [CrossRef]
- McShane, C.; Kiat, C.; Rigby, J.; Crosbie, O. The mRNA COVID-19 vaccine-A rare trigger of autoimmune hepatitis? J. Hepatol. 2021, 75, 1252–1254. [Google Scholar] [CrossRef]
- Clayton-Chubb, D.; Schneider, D.; Freeman, E.; Kemp, W.; Roberts, S.K. Autoimmune hepatitis developing after the ChAdOx1 nCoV-19 (Oxford-AstraZeneca) vaccine. J. Hepatol. 2021, 75, 1249–1250. [Google Scholar] [CrossRef]
- Tan, C.K.; Wong, Y.J.; Wang, L.M.; Ang, T.L.; Kumar, R. Autoimmune hepatitis following COVID-19 vaccination: True causality or mere association? J. Hepatol. 2021, 75, 1250–1252. [Google Scholar] [CrossRef]
- Rocco, A.; Sgamato, C.; Compare, D.; Nardone, G. Autoimmune hepatitis following SARS-CoV-2 vaccine: May not be a casuality. J. Hepatol. 2021, 75, 728–729. [Google Scholar] [CrossRef]
- Bril, F.; Al Diffalha, S.; Dean, M.; Fettig, D.M. Autoimmune hepatitis developing after coronavirus disease 2019 (COVID-19) vaccine: Causality or casualty? J. Hepatol. 2021, 75, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Goulas, A.; Kafiri, G.; Kranidioti, H.; Manolakopoulos, S. A typical autoimmune hepatitis (AIH) case following Covid-19 mRNA vaccination. More than a coincidence? Liver Int. 2022, 42, 254–255. [Google Scholar] [CrossRef] [PubMed]
- Lodato, F.; Larocca, A.; D’Errico, A.; Cennamo, V. An unusual case of acute cholestatic hepatitis after m-RNABNT162b2 (Comirnaty) SARS-CoV-2 vaccine: Coincidence, autoimmunity or drug-related liver injury. J. Hepatol. 2021, 75, 1254–1256. [Google Scholar] [CrossRef] [PubMed]
- Londono, M.C.; Gratacos-Gines, J.; Saez-Penataro, J. Another case of autoimmune hepatitis after SARS-CoV-2 vaccination-still casualty? J. Hepatol. 2021, 75, 1248–1249. [Google Scholar] [CrossRef] [PubMed]
- Rela, M.; Jothimani, D.; Vij, M.; Rajakumar, A.; Rammohan, A. Auto-immune hepatitis following COVID vaccination. J. Autoimmun. 2021, 123, 102688. [Google Scholar] [CrossRef]
- Zin Tun, G.S.; Gleeson, D.; Al-Joudeh, A.; Dube, A. Immune-mediated hepatitis with the Moderna vaccine, no longer a coincidence but confirmed. J. Hepatol. 2022, 76, 747–749. [Google Scholar] [CrossRef]
- Vuille-Lessard, E.; Montani, M.; Bosch, J.; Semmo, N. Autoimmune hepatitis triggered by SARS-CoV-2 vaccination. J. Autoimmun. 2021, 123, 102710. [Google Scholar] [CrossRef]
- Mathew, M.; John, S.B.; Sebastian, J.; Ravi, M.D. COVID-19 vaccine triggered autoimmune hepatitis: Case report. Eur. J. Hosp. Pharm. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Ferronato, M.L.M.; Muratori, L. Liver injury with autoimmune features after vaccination against SARS-CoV-2: The verdict is still open. Eur. J. Intern. Med. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Lopez Romero-Salazar, F.; Veras Lista, M.; Gomez-Dominguez, E.; Ibarrola-Andres, C.; Munoz Gomez, R.; Fernandez Vazquez, I. SARS-CoV-2 vaccine, a new autoimmune hepatitis trigger? Rev. Esp. Enferm Dig. 2022, 114, 567–568. [Google Scholar] [CrossRef]
- Mahalingham, A.; Duckworth, A.; Griffiths, W.J.H. First report of post-transplant autoimmune hepatitis recurrence following SARS-CoV-2 mRNA vaccination. Transpl. Immunol. 2022, 72, 101600. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Kwon, J.H.; Yoon, N.; Lee, S.H.; Sung, P.S. Immune-mediated liver injury represented as overlap syndrome after SARS-CoV-2 vaccination. J. Hepatol. 2022, 77, 1209–1211. [Google Scholar] [CrossRef] [PubMed]
- Efe, C.; Kulkarni, A.V.; Terziroli Beretta-Piccoli, B.; Magro, B.; Stattermayer, A.; Cengiz, M.; Clayton-Chubb, D.; Lammert, C.; Bernsmeier, C.; Gul, O.; et al. Liver injury after SARS-CoV-2 vaccination: Features of immune-mediated hepatitis, role of corticosteroid therapy and outcome. Hepatology 2022, 76, 1576–1586. [Google Scholar] [CrossRef] [PubMed]
- Shroff, H.; Satapathy, S.K.; Crawford, J.M.; Todd, N.J.; VanWagner, L.B. Liver injury following SARS-CoV-2 vaccination: A multicenter case series. J. Hepatol. 2022, 76, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Rigamonti, C.; Coco, B.; Brunetto, M.; Labanca, S.; Giannini, E.; Magro, B.; Fagiuoli, S.; Baroni, G.S.; Sgamato, C.; Miele, L.; et al. Clinical features of patients with new onset of autoimmune hepatitis following SARS-CoV-2 vaccination. Dig. Liver Dis. 2022, 54, S48. [Google Scholar] [CrossRef]
- Nyein, C.M.; Liew, Z.H.S.; Leow, W.Q.; Yeong, P.S.J.; Ho, G.H. Severe de novo liver injury after Moderna vaccination-not always autoimmune hepatitis. J. Hepatol. 2022, 77, 556–558. [Google Scholar] [CrossRef]
- Czaja, A.J. Performance parameters of the diagnostic scoring systems for autoimmune hepatitis. Hepatology 2008, 48, 1540–1548. [Google Scholar] [CrossRef]
- Doherty, M. Algorithms for assessing the probability of an Adverse Drug Reaction. Respir. Med. CME 2009, 2, 63–67. [Google Scholar] [CrossRef]
- Danan, G.; Teschke, R. Roussel Uclaf Causality Assessment Method for Drug-Induced Liver Injury: Present and Future. Front. Pharmacol. 2019, 10, 853. [Google Scholar] [CrossRef]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef]
- Garcia-Cortes, M.; Lucena, M.I.; Pachkoria, K.; Borraz, Y.; Hidalgo, R.; Andrade, R.J.; Spanish Group for the Study of Drug-induced Liver Disease. Evaluation of naranjo adverse drug reactions probability scale in causality assessment of drug-induced liver injury. Aliment. Pharmacol. Ther. 2008, 27, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Castiella, A.; Zapata, E.; Lucena, M.I.; Andrade, R.J. Drug-induced autoimmune liver disease: A diagnostic dilemma of an increasingly reported disease. World J. Hepatol. 2014, 6, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.X.; Kaplowitz, N. Immune-mediated drug-induced liver disease. Clin. Liver Dis. 2002, 6, 755–774. [Google Scholar] [CrossRef] [PubMed]
- David, S.; Hamilton, J.P. Drug-induced Liver Injury. US Gastroenterol. Hepatol. Rev. 2010, 6, 73–80. [Google Scholar]
- Heurgue-Berlot, A.; Bernard-Chabert, B.; Diebold, M.D.; Thiefin, G. Drug-induced autoimmune-like hepatitis: A case of chronic course after drug withdrawal. Dig. Dis. Sci. 2011, 56, 2504–2505. [Google Scholar] [CrossRef]
- Castiella, A.; Lucena, M.I.; Zapata, E.M.; Otazua, P.; Andrade, R.J. Drug-induced autoimmune-like hepatitis: A diagnostic challenge. Dig. Dis. Sci. 2011, 56, 2501–2502. [Google Scholar] [CrossRef]
- Hoo, C.-Z.; Tan, K.-C.; Abdullah, S.; Sim, B.L.-H.; Omar, H.; Tan, S.-S. Severe Hepatocellular Liver Injury After COVID-19 Vaccination Without Autoimmune Hepatitis Features: A Case Serires. ACG Case Rep. J. 2022, 9, e00760. [Google Scholar] [CrossRef]
- AASLD. Expert Panel Consensus Statement: Vaccines to Prevent COVID-19 in Patients with Liver Disease. Available online: https://www.aasld.org/sites/default/files/2022-07/AASLD%20COVID-19%20Vaccine%20Document%20Update%203.28.2022%20FINAL.pdf (accessed on 20 October 2022).
- Zmievskaya, E.; Valiullina, A.; Ganeeva, I.; Petukhov, A.; Rizvanov, A.; Bulatov, E. Application of CAR-T Cell Therapy beyond Oncology: Autoimmune Diseases and Viral Infections. Biomedicines 2021, 9, 59. [Google Scholar] [CrossRef]


{kind=link}
| Case | Publication | Gender, Age | Type of Vaccine | Number of Doses | History of Liver Disease or AD | Symptoms, Signs, Laboratory Results/Outcome | Latency (Days) | Serology | Increase in IgG | Biopsy Consistent with AIH |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | [52,53] * | 4× F/ 1× M, 62+ | 3× mRNA, 2× Viral vector | n/a | One patient had a probable diagnosis of AIH | All 5 cases demonstrated LFT abnormalities. Resolution in all 5 patients. Four of them needed immunomodulators (corticosteroids–azathioprine) and one did not need any drug remedy. | 19+ | All 5 cases were ANA positive | All 5 cases demonstrated elevation of IgG | Four patients had liver biopsies consistent with AIH, one patient did not have liver biopsy |
| 2 | ||||||||||
| 3 | ||||||||||
| 4 | ||||||||||
| 5 | ||||||||||
| 6 | [54] | M, 35 | Viral vector | 1 | No | Fatigue, fever, headache, vomiting, abdominal pain, jaundice, ↑ ATs, ↑ Bil, liver failure, DIC. Death due to fulminant hepatitis, despite high-dose corticosteroids. | 5 | Negative | n/a | Not consistent with AIH |
| 7 | [55] | F, 52 | Inactivated | 2 | No | Fatigue, jaundice, ↑ ATs, ↑ Bil. Rapid improvement with corticosteroids–azathioprine. | 7 | ANA, ASMA | Yes | Yes |
| 8 | [56] | F, 35 | mRNA | 2 | AIH | ↑ ATs. Flare of AIH. Remission without medical intervention. | 14 | ASMA | n/a | Biopsy confirmed AIH 5 years ago |
| 9 | [57] | F, 59 | Viral vector | 2 | No | Jaundice, ↑ ATs, ↑ Bil. Responded well to high-dose corticosteroids. | 12 | Negative | Yes | Yes |
| 10 | F, 63 | Viral vector | 1 | PSC | Jaundice, ↑ ATs, ↑ Bil. Initially improved with corticosteroids, but soon relapsed and died due to sepsis. | 14 | ANA | Yes | Yes | |
| 11 | F, 72 | 2× Inactivated, booster with mRNA | 3 | No | Jaundice, ↑ ATs, ↑ Bil. Responded well to high-dose corticosteroids. | 10 | AMA | Yes | Yes | |
| 12 | [58] | F, 82 | mRNA | 1 | Treated HCV | Anorexia, fatigue, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 4 | ANA | Yes | Yes |
| 13 | [59] | F, 52 | mRNA | 1 | ICIs for lung cancer | Diarrhea (ICI-related colitis), ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 10 | Negative | No | Biopsy not compatible with AIH |
| 14 | [60] | F, 77 | mRNA | 2 | No | Disorientation, vomiting, nausea, jaundice, ↑ ATs, ↑ Bil. HLA-DR4. Resolution with corticosteroids–azathioprine. | 2 | ANA, AMA | No | Yes |
| 15 | M, 23 | mRNA | 2 | No | Mononucleosis-like syndrome, jaundice, ↑ ATs, ↑ Bil. HLA-DR3. Resolution with corticosteroids. | 10 | Negative | No | Yes | |
| 16 | [48] | M, 52 | mRNA | Episodes after both 1st and 2nd dose. | No | Nausea, fatigue, anorexia, pruritus, jaundice, ↑ ATs, ↑ Bil. Peripheral anti-spike CD8 T-cells. Resolution without medical treatment. Relapse after 2nd dose. Resolution with corticosteroids. | First episode 10 days, 2nd episode 41 days after first dose | ANA, ASMA, AMA | Yes | Yes, panlobular CD8 T-cell infiltration |
| 17 | [61] | F, 27 | mRNA | 2 | No | Nausea, vomiting, headache, fever, jaundice, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 6 | ANA | Yes | Yes, along with eosinophilic infiltrates |
| 18 | [62] | M, 62 | Inactivated | 2 | No | Weakness, jaundice, pruritus, weight loss, ↑ ATs, ↑ Bil. Resolution without corticosteroids. | 3 | Negative | n/a | Yes, along with eosinophilic infiltrates |
| 19 | [63] | F, 63 | mRNA | 2 | No | Abdominal pain, nausea, jaundice, dark urine, acholic stools, ↑ ATs, ↑ Bil. Resolution with corticosteroids–azathioprine. | 53 | Negative | Yes | Yes |
| 20 | [64] | M, 79 | Viral vector | Symptoms started after the 1st dose; however, he received a 2nd dose before hospital evaluation. | No | Abdominal pain, jaundice, pruritus, dark urine, acholic stools, ↑ ATs, ↑ Bil. Resolution with corticosteroids–azathioprine. | 15 | ANA, ASMA | Yes | Yes, along with eosinophilic infiltrates |
| 21 | [65] | F, 80 | mRNA | 2 | No | Similar clinical manifestations for all three patients; fatigue, pruritus, jaundice, ↑ ATs, ↑ Bil. Two of them responded well to corticosteroids, one developed liver failure despite treatment and died. | 10 | All patients were ANA positive; one of them was ASMA positive | All 3 patients demonstrated IgG elevation | All 3 patients had liver biopsy consistent with AIH |
| 22 | F, 73 | mRNA | 1 | 21 | ||||||
| 23 | F, 68 | Viral vector | 1 | 20 | ||||||
| 24 | [66] | F, 80 | mRNA | 2 | No | Jaundice, ↑ ATs, ↑ Bil. Improvement with corticosteroids. | 10 | All patients were ANA positive; one was AMA positive | All 3 patients demonstrated IgG elevation | All 3 patients had liver biopsy consistent with AIH |
| 25 | F, 75 | mRNA | 2 | No | ↑ ATs, ↑ Bil. Improvement with corticosteroids. | 4 | ||||
| 26 | F, 78 | mRNA | 1 | PBC | Fever, malaise, ↑ ATs, ↑ Bil. Improvement with corticosteroids. | 7 | ||||
| 27 | [67] | F, 57 | Inactivated | She developed symptoms after the 1st dose, but she did not seek medical advice and received a 2nd dose. | No | Jaundice, dark urine, acholic stools, pruritus, ↑ ATs, ↑ Bil. Resolution with corticosteroids–azathioprine. | 14 | ANA, SSA | Yes | Yes |
| 28 | [68] | F, 61 | mRNA | n/a | Hashimoto thyroiditis | Malaise, fatigue, anorexia, nausea, jaundice, ↑ ATs, ↑ Bil. Resolution with corticosteroids–azathioprine. | 14 | ANA, ASMA | Yes | Yes |
| 29 | [69] | F, 65 | mRNA | 1 | No | Abdominal pain after vaccine injection, jaundice, dark urine, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 14 | ANA | Yes | Yes |
| 30 | [70] | F, 40 | mRNA | 2 | Sarcoidosis | ↑ ATs. Resolution with corticosteroids. | 30 | ANA | Yes | Yes |
| 31 | [71] | F, 36 | mRNA | 1 | PSC, ulcerative colitis | ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 12 | ANA | n/a | Yes, along with eosinophilic infiltrates |
| 32 | [72] | M, 63 | mRNA | 1 | No | Fatigue, jaundice, anorexia, ↑ ATs, ↑ Bil. HLA-DRB1, DQA1, DQB1. Resolution with corticosteroids. | 7 | ANA, anti-gastric parietal | Yes | Yes |
| 33 | [73] | F, 71 | mRNA | 1 | No | Jaundice, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 4 | ASMA | Yes | Yes, along with eosinophilic infiltrates |
| 34 | [74] | M, 36 | Viral vector | 1 | No | Pruritus, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 26 | ANA | No | Yes |
| 35 | [75] | F, 56 | mRNA | 1 | Fatigue, jaundice, anorexia, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 40 | ANA, ASMA | Yes | Yes, along with eosinophilic infiltrates | |
| 36 | [76] | F, 80 | mRNA | 2 | Hashimoto thyroiditis | Jaundice, dark urine, ↑ ATs, ↑ Bil. Improvement with corticosteroids. | 7 | ANA | Yes | Yes |
| 37 | [77] | F, 35 | mRNA | 1 | No | Jaundice, pruritus, dark urine, ↑ ATs, ↑ Bil. Improvement with corticosteroids. | 6 | ANA, anti-ds DNA | No | Yes, along with eosinophilic infiltrates |
| 38 | [78] | F, 52 | mRNA | 1 | No | Nausea, jaundice, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 14 | ANA, ASMA | Yes | Yes, along with eosinophilic infiltrates |
| 39 | [79] | F, 43 | mRNA | First symptoms presented after 1st dose; however, she received a 2nd vaccine dose. | No | Jaundice, pruritus, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 15 | Negative | No | Yes |
| 40 | [80] | F, 41 | mRNA | First symptoms presented after 1st dose and lasted for 3 weeks; however, she received a 2nd vaccine dose, which flared the symptoms. | No | Abdominal pain, nausea, vomiting, jaundice, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 1 | ANA, ASMA, SLA, anti-liver cytosol | Yes | Yes |
| 41 | [81] | F, 38 | Viral vector | 1 | No | Jaundice, fatigue, pedal edema, dark urine, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 7 | ANA | Yes | Yes |
| 42 | M, 62 | Viral vector | 1 | History of jaundice episodes (unknown etiology) with spontaneous resolution | Fever, anorexia, jaundice, ↑ ATs, ↑ Bil. Patient was managed with corticosteroids and plasmapheresis with poor response and died 3 weeks later. | 13 | Negative | n/a | Compatible, but not typical | |
| 43 | [82] | M, 47 | mRNA | First symptoms presented after 1st dose; however, he received a 2nd vaccine dose, which flared symptoms. | No | Jaundice, malaise, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 3 | ANA | Yes | Yes, along with eosinophilic infiltrates |
| 44 | [83] | M, 76 | mRNA | 1 | Hashimoto thyroiditis | Dark urine, weight loss, fatigue, ↑ ATs, ↑ Bil. Resolution with corticosteroids–azathioprine. | 3 | ANA, ASMA, anti-actin, anti-neutrophilic cytoplasmic | Yes | Yes |
| 45 | [84] | F, ≈30 | Viral vector | 1 | No | Jaundice, dark urine, acholic stools, fatigue, ↑ ATs, ↑ Bil. Resolution with corticosteroids. | 10 | ANA | Yes | Yes, along with findings compatible with drug toxicity |
| 46 | [85] | F, 30 | mRNA | 2 | Hashimoto thyroiditis, family history of ADs | Fatigue, anorexia, arthralgia, dark urine, ↑ ATs, ↑ Bil. Spontaneous resolution. | ≈30 | ANA | Yes | Yes |
| 47 | M, 26 | mRNA | 2 | Vitiligo | ↑ ATs, ↑ Bil. HLA-A1, B8, DR3. Persistence of LFT abnormalities, as declined treatment with corticosteroids. | ≈30 | ANA | Yes | Yes | |
| 48 | F, 21 | mRNA | ↑ ATs before vaccination. Workup was consistent with AIH diagnosis. Flare of symptoms after both 1st and 2nd vaccine dose. | AIH | ↑ ATs. HLA-A1, B8, DR3. First episode remitted spontaneously. After 2nd dose, resolution with corticosteroids. | n/a | ANA, ASMA | No | Yes | |
| 49 | [86] | M, 76 | mRNA | n/a | Liver cirrhosis secondary to PBC | ↑ ATs, ↑ Bil. Resolution with corticosteroids–azathioprine. | ≈30 | ANA | Yes | Yes |
| 50 | [87] | F, 32 | mRNA | 3 | Liver transplantation due to AIH | ↑ ATs, ↑ Bil. Remission resolution with corticosteroids–azathioprine. | 21 | Liver cytosol antibody 1 | No | Yes |
| 51 | [88] | F, 57 | mRNA | 1 | No | Fatigue, ↑ ATs, ↑ Bil, ↑γGT, ↑ALP. Resolution without administration of immunomodulation (patient treated with ursodeoxycholic acid). | 14 | ANA, AMA | No | Yes, along with findings of granulomatous, non-suppurative cholangitis with destruction and proliferation of bile duct (AIH/PBC variant) |
| Cases | Publication | Simplified Criteria for AIH | Naranjo Score for Vaccine Causality | ||
|---|---|---|---|---|---|
| Score | Probability | Score | Probability | ||
| 1 | [52] * | 7 + | Definite | 5 | Probable |
| 2 | [53] | 8 + | Definite | May be 2 to 5 for each patient | Possible/probable |
| 3 | 8 + | Definite | |||
| 4 | 8 + | Definite | |||
| 5 | n/a | n/a | |||
| 6 | [54] | 2 | Non-probable | 2 | Possible |
| 7 | [55] | 8 | Definite | 7 | Probable |
| 8 | [56] | 4 | Non-probable | 6 | Probable |
| 9 | [57] | 4 | Non-probable | 7 | Probable |
| 10 | 6 | Probable | 7 | Probable | |
| 11 | 5 | Non-probable | 7 | Probable | |
| 12 | [58] | 6 | Probable | 7 | Probable |
| 13 | [59] | 0 | Non-probable | 3 | Possible |
| 14 | [60] | 6 | Probable | 7 | Probable |
| 15 | 4 | Non-probable | 7 | Probable | |
| 16 | [48] | 7 | Definite | 9 | Definite |
| 17 | [61] | 7 | Definite | 7 | Probable |
| 18 | [62] | 3 | Non-probable | 6 | Probable |
| 19 | [63] | 5 | Non-probable | 7 | Probable |
| 20 | [64] | 7 | Definite | 7 | Probable |
| 21 | [65] | ≥6 for each patient | At least probable AIH for each patient | 7 | Probable |
| 22 | 7 | Probable | |||
| 23 | 6 | Probable | |||
| 24 | [66] | 6 | Probable | 7 | Probable |
| 25 | 7 | Definite | 7 | Probable | |
| 26 | 7 | Definite | 7 | Probable | |
| 27 | [67] | 7 + | Definite | 7 | Probable |
| 28 | [68] | 7 + | Definite | 7 | Probable |
| 29 | [69] | 8 + | Definite | 7 | Probable |
| 30 | [70] | 8 | Definite | 7 | Probable |
| 31 | [71] | 6 | Probable | 7 | Probable |
| 32 | [72] | 7 | Definite | 7 | Probable |
| 33 | [73] | 7 | Definite | 7 | Probable |
| 34 | [74] | 6 | Probable | 7 | Probable |
| 35 | [75] | ≥7 | Definite | 7 | Probable |
| 36 | [76] | 8 | Definite | 7 | Probable |
| 37 | [77] | 6 | Probable | 7 | Probable |
| 38 | [78] | 7 | Definite | 7 | Probable |
| 39 | [79] | 4 | Non-probable | 7 | Probable |
| 40 | [81] | 8 + | Definite | 9 | Definite |
| 41 | [81] | 7 | Definite | 7 | Probable |
| 42 | 3 | Non-probable | 3 | Possible | |
| 43 | [82] | ≥6 | At least probable | 9 | Definite |
| 44 | [83] | 8 + | Definite | 7 | Probable |
| 45 | [84] | 6 + | Probable | 4 | Possible |
| 46 | [85] | 7 | Definite | 6 | Probable |
| 47 | 7 | Definite | 6 | Probable | |
| 48 | 6 | Probable | 8 | Probable | |
| 49 | [86] | 7 | Definite | 7 | Probable |
| 50 | [87] | 6 | Probable | 7 | Probable |
| 51 | [88] | 6 | Probable | 6 | Probable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trontzas, I.P.; Kyriakoulis, K.G.; Vathiotis, I.A.; Syrigos, A.; Kounadis, G.; Siasiakou, S.; Poulakou, G. Vaccine-Related Autoimmune Hepatitis: Emerging Association with SARS-CoV-2 Vaccination or Coincidence? Vaccines 2022, 10, 2073. https://doi.org/10.3390/vaccines10122073
Trontzas IP, Kyriakoulis KG, Vathiotis IA, Syrigos A, Kounadis G, Siasiakou S, Poulakou G. Vaccine-Related Autoimmune Hepatitis: Emerging Association with SARS-CoV-2 Vaccination or Coincidence? Vaccines. 2022; 10(12):2073. https://doi.org/10.3390/vaccines10122073
Chicago/Turabian StyleTrontzas, Ioannis P., Konstantinos G. Kyriakoulis, Ioannis A. Vathiotis, Alexandros Syrigos, Georgios Kounadis, Sofia Siasiakou, and Garyphalia Poulakou. 2022. "Vaccine-Related Autoimmune Hepatitis: Emerging Association with SARS-CoV-2 Vaccination or Coincidence?" Vaccines 10, no. 12: 2073. https://doi.org/10.3390/vaccines10122073
APA StyleTrontzas, I. P., Kyriakoulis, K. G., Vathiotis, I. A., Syrigos, A., Kounadis, G., Siasiakou, S., & Poulakou, G. (2022). Vaccine-Related Autoimmune Hepatitis: Emerging Association with SARS-CoV-2 Vaccination or Coincidence? Vaccines, 10(12), 2073. https://doi.org/10.3390/vaccines10122073