

Quantitative Benefit–Risk Assessment of COVID-19 Vaccines Using the Multi-Criteria Decision Analysis


Abstract
1. Introduction
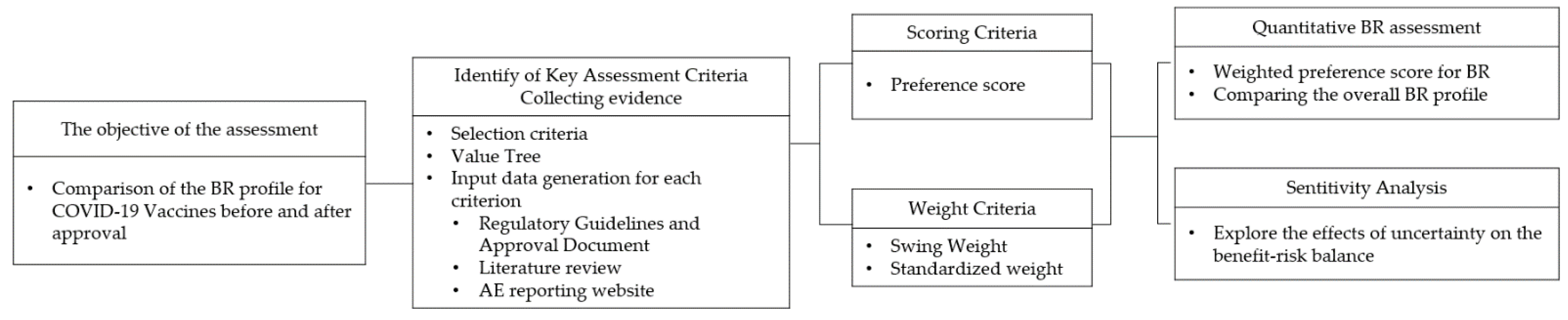
2. Materials and Methods
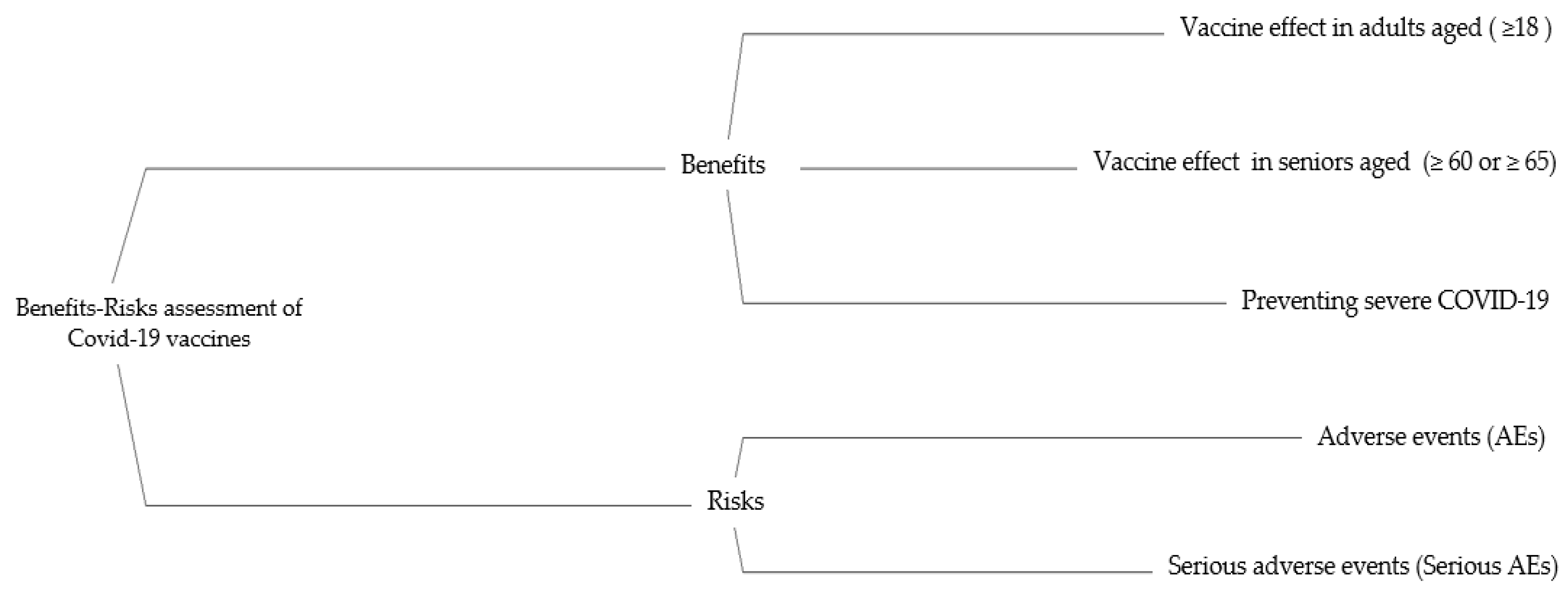
2.1. Criteria Selection
2.2. Preference Score
| For benefit | (1) | |
| For risk | (2) |
2.3. Weighting
| all Standardized weight (Wi) sum to 1 | (3) |
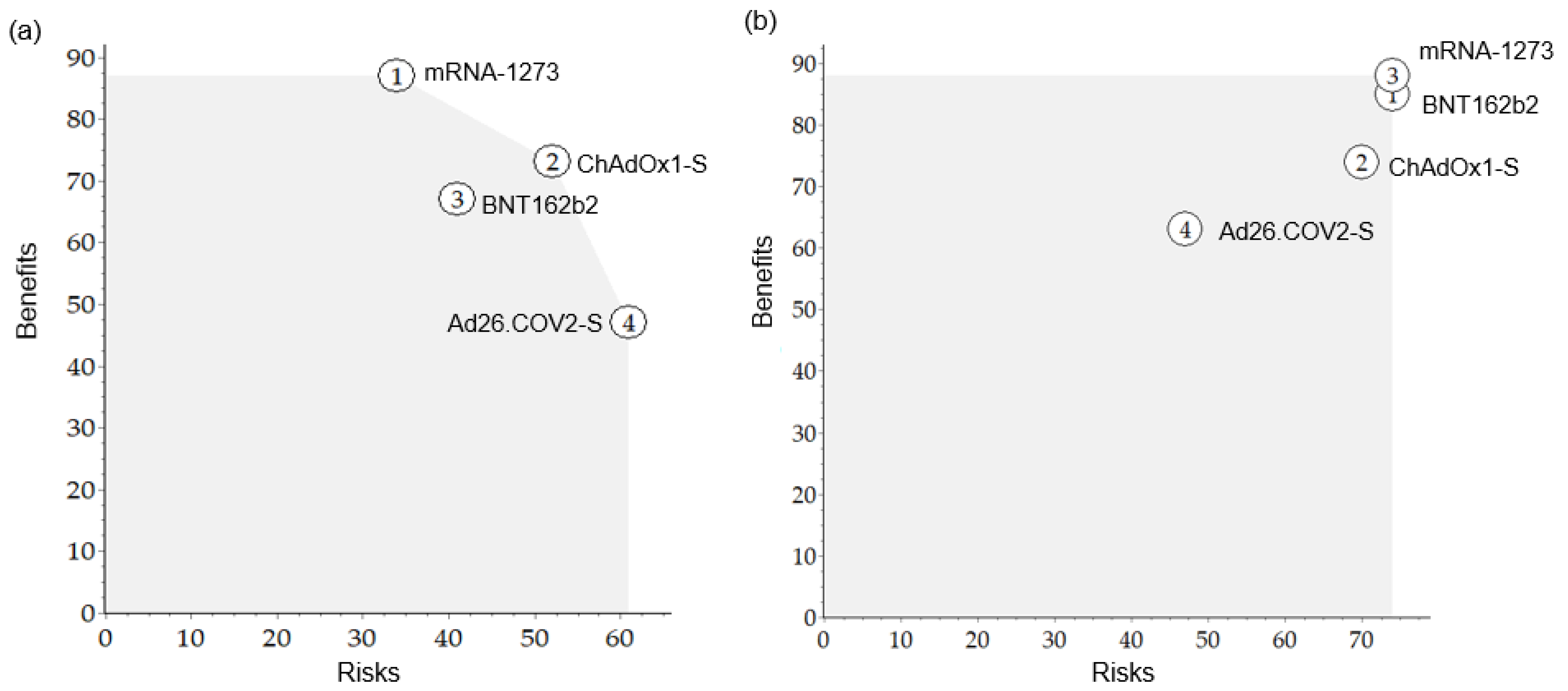
2.4. Base case and Sensitivity Analyses
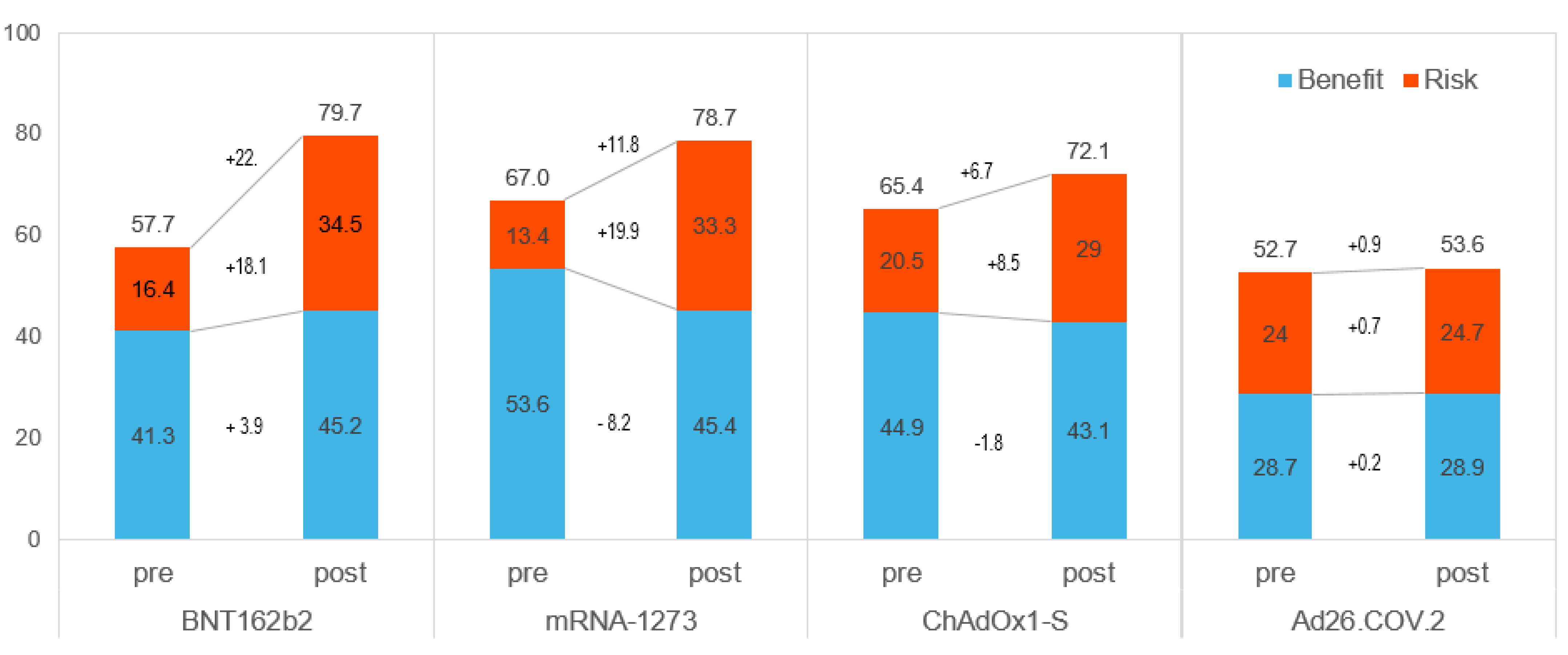
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Dashboard; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Lythgoe, M.P.; Middleton, P. Comparison of COVID-19 Vaccine Approvals at the US Food and Drug Administration, European Medicines Agency, and Health Canada. JAMA Netw. Open 2021, 4, e2114531. [Google Scholar] [CrossRef]
- Juhaeri, J. Benefit-risk evaluation: The past, present and future. Ther. Adv. Drug Saf. 2019, 10, 2042098619871180. [Google Scholar] [CrossRef]
- Abbing-Karahagopian, V.; Kurz, X.; de Vries, F.; van Staa, T.P.; Alvarez, Y.; Hesse, U.; Hasford, J.; Dijk, L.; de Abajo, F.J.; Weil, J.G.; et al. Bridging differences in outcomes of pharmacoepidemiological studies: Design and first results of the PROTECT project. Curr. Clin. Pharmacol. 2014, 9, 130–138. [Google Scholar] [CrossRef]
- Menzies, T.; Saint-Hilary, G.; Mozgunov, P. A comparison of various aggregation functions in multi-criteria decision analysis for drug benefit-risk assessment. Stat. Methods Med. Res. 2022, 31, 899–916. [Google Scholar] [CrossRef]
- Chisholm, O.; Sharry, P.; Phillips, L. Multi-Criteria Decision Analysis for Benefit-Risk Analysis by National Regulatory Authorities. Front. Med. 2021, 8, 820335. [Google Scholar] [CrossRef]
- Kurzinger, M.L.; Douarin, L.; Uzun, I.; El-Haddad, C.; Hurst, W.; Juhaeri, J.; Tcherny-Lessenot, S. Structured benefit-risk evaluation for medicinal products: Review of quantitative benefit-risk assessment findings in the literature. Ther. Adv. Drug Saf. 2020, 11, 2042098620976951. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.; Waddingham, E.; Mt-Isa, S.; Goginsky, A.; Chan, E.; Downey, G.; Hallgreen, C.E.; Hockley, K.S.; Juhaeri, J.; Lieftucht, A. IMI-PROTECT Benefit-Risk Grouprecommendations Report: Recommendations for the Methodology Andvisualisation Techniques to Be Used in Theassessment of Benefit and Risk of Medicines; PROTECT Consortium: London, UK, 2014. [Google Scholar]
- Moore, A.; Crossley, A.; Ng, B.; Phillips, L.; Sancak, O.; Rainsford, K.D. Use of multicriteria decision analysis for assessing the benefit and risk of over-the-counter analgesics. J. Pharm. Pharmacol. 2017, 69, 1364–1373. [Google Scholar] [CrossRef] [PubMed]
- Vermersch, P.; Martinelli, V.; Pfleger, C.; Rieckmann, P.; Alonso-Magdalena, L.; Galazka, A.; Dangond, F.; Phillips, L. Benefit-risk Assessment of Cladribine Using Multi-criteria Decision Analysis (MCDA) for Patients With Relapsing-remitting Multiple Sclerosis. Clin. Ther. 2019, 41, 249–260.e218. [Google Scholar] [CrossRef] [PubMed]
- Baltussen, R.; Marsh, K.; Thokala, P.; Diaby, V.; Castro, H.; Cleemput, I.; Garau, M.; Iskrov, G.; Olyaeemanesh, A.; Mirelman, A.; et al. Multicriteria Decision Analysis to Support Health Technology Assessment Agencies: Benefits, Limitations, and the Way Forward. Value Health 2019, 22, 1283–1288. [Google Scholar] [CrossRef]
- Marcelon, L.; Verstraeten, T.; Dominiak-Felden, G.; Simondon, F. Quantitative benefit-risk assessment by MCDA of the quadrivalent HPV vaccine for preventing anal cancer in males. Expert Rev. Vaccines 2016, 15, 139–148. [Google Scholar] [CrossRef] [PubMed]
- WHO. Considerations for Evaluation of COVID-19 Vaccines; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Mehrotra, D.V.; Janes, H.E.; Fleming, T.R.; Annunziato, P.W.; Neuzil, K.M.; Carpp, L.N.; Benkeser, D.; Brown, E.R.; Carone, M.; Cho, I.; et al. Clinical Endpoints for Evaluating Efficacy in COVID-19 Vaccine Trials. Ann. Intern. Med. 2021, 174, 221–228. [Google Scholar] [CrossRef] [PubMed]
- FDA. Development and Licensure of Vaccines to Prevent COVID-19; FDA: Silver Spring, MA, USA, 2020. [Google Scholar]
- Pfizer. Assessment Report Comirnaty Common Name: COVID-19 mRNA Vaccine (Nucleoside-Modified); EMEA Assessment Report; Pfizer: New York, NY, USA, 2021. [Google Scholar]
- Pfizer. Vaccines and Related Biological Products Advisory Committee Meeting_FDA Briefing Document Pfizer BioNTech COVID-19 Vaccine. In FDA Briefing Document Pfizer-BioNTech COVID-19 Vaccine; FDA: Silver Spring, MA, USA, 2020. [Google Scholar]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- Moderna. Vaccines and Related Biological Products Advisory Committee Meeting_FDA Briefing Document Moderna COVID-19 Vaccine. In FDA Briefing Document Moderna COVID-19 Vaccine; FDA: Silver Spring, MA, USA, 2020. [Google Scholar]
- AstraZeneca. Assessment Report COVID-19 Vaccine AstraZeneca Common Name: COVID-19 Vaccine (ChAdOx1-S [Recombinant]; EMEA Assessment Report; AstraZeneca: Cambridge, UK, 2021. [Google Scholar]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 nCoV-19) COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 2348–2360. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cardenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Janssen. Vaccines and Related Biological Products Advisory Committee Meeting_FDA Briefing Document Janssen Ad26.COV2.S Vaccine for the Prevention of COVID-19. In FDA Briefing Document Moderna COVID-19 Vaccine; FDA: Silver Spring, MA, USA, 2021. [Google Scholar]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination with BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections among Health Care Workers. JAMA 2021, 325, 2457–2465. [Google Scholar] [CrossRef] [PubMed]
- Arregoces-Castillo, L.; Fernandez-Nino, J.; Rojas-Botero, M.; Palacios-Clavijo, A.; Galvis-Pedraza, M.; Rincon-Medrano, L.; Pinto-Alvarez, M.; Ruiz-Gomez, F.; Trejo-Valdivia, B. Effectiveness of COVID-19 vaccines in older adults in Colombia: A retrospective, population-based study of the ESPERANZA cohort. Lancet Healthy Longev. 2022, 3, e242–e252. [Google Scholar] [CrossRef]
- Britton, A.; Jacobs Slifka, K.M.; Edens, C.; Nanduri, S.A.; Bart, S.M.; Shang, N.; Harizaj, A.; Armstrong, J.; Xu, K.; Ehrlich, H.Y.; et al. Effectiveness of the Pfizer-BioNTech COVID-19 Vaccine Among Residents of Two Skilled Nursing Facilities Experiencing COVID-19 Outbreaks-Connecticut, December 2020-February 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 396–401. [Google Scholar] [CrossRef]
- Fabiani, M.; Ramigni, M.; Gobbetto, V.; Mateo-Urdiales, A.; Pezzotti, P.; Piovesan, C. Effectiveness of the Comirnaty (BNT162b2, BioNTech/Pfizer) vaccine in preventing SARS-CoV-2 infection among healthcare workers, Treviso province, Veneto region, Italy, 27 December 2020 to 24 March 2021. Eurosurveillance 2021, 26, 2100420. [Google Scholar] [CrossRef]
- Grannis, S.J.; Rowley, E.A.; Ong, T.C.; Stenehjem, E.; Klein, N.P.; DeSilva, M.B.; Naleway, A.L.; Natarajan, K.; Thompson, M.G.; Network, V. Interim Estimates of COVID-19 Vaccine Effectiveness Against COVID-19-Associated Emergency Department or Urgent Care Clinic Encounters and Hospitalizations among Adults During SARS-CoV-2 B.1.617.2 (Delta) Variant Predominance-Nine States, June–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1291–1293. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Martinez-Baz, I.; Miqueleiz, A.; Casado, I.; Navascues, A.; Trobajo-Sanmartin, C.; Burgui, C.; Guevara, M.; Ezpeleta, C.; Castilla, J.; Working Group for the Study of, C.-i.N. Effectiveness of COVID-19 vaccines in preventing SARS-CoV-2 infection and hospitalisation, Navarre, Spain, January to April 2021. Eurosurveillance 2021, 26, 2100438. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Paris, C.; Perrin, S.; Hamonic, S.; Bourget, B.; Roué, C.; Brassard, O.; Tadié, E.; Gicquel, V.; Bénézit, F.; Thibault, V. Effectiveness of mRNA-BNT162b2, mRNA-1273, and ChAdOx1 nCoV-19 vaccines against COVID-19 in healthcare workers: An observational study using surveillance data. Clin. Microbiol. Infect. 2021, 27, 1699.e1695–1699.e1698. [Google Scholar] [CrossRef]
- Pawlowski, C.; Lenehan, P.; Puranik, A.; Agarwal, V.; Venkatakrishnan, A.J.; Niesen, M.J.M.; O’Horo, J.C.; Virk, A.; Swift, M.D.; Badley, A.D.; et al. FDA-authorized mRNA COVID-19 vaccines are effective per real-world evidence synthesized across a multi-state health system. Med (NY) 2021, 2, 979–992.e978. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. COVID-19 Vaccine Effectiveness in New York State. N. Engl. J. Med. 2022, 386, 116–127. [Google Scholar] [CrossRef]
- Thompson, M.G.; Stenehjem, E.; Grannis, S.; Ball, S.W.; Naleway, A.L.; Ong, T.C.; DeSilva, M.B.; Natarajan, K.; Bozio, C.H.; Lewis, N.; et al. Effectiveness of COVID-19 Vaccines in Ambulatory and Inpatient Care Settings. N. Engl. J. Med. 2021, 385, 1355–1371. [Google Scholar] [CrossRef]
- Zacay, G.; Shasha, D.; Bareket, R.; Kadim, I.; Hershkowitz Sikron, F.; Tsamir, J.; Mossinson, D.; Heymann, A.D. BNT162b2 Vaccine Effectiveness in Preventing Asymptomatic Infection with SARS-CoV-2 Virus: A Nationwide Historical Cohort Study. Open Forum Infect Dis. 2021, 8, ofab262. [Google Scholar] [CrossRef]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Takhar, H.S.; Tubert, J.E.; et al. Real-world effectiveness of the mRNA-1273 vaccine against COVID-19: Interim results from a prospective observational cohort study. Lancet Reg. Health Am. 2022, 6, 100134. [Google Scholar] [CrossRef]
- Bekker, L.G.; Garrett, N.; Goga, A.; Fairall, L.; Reddy, T.; Yende-Zuma, N.; Kassanjee, R.; Collie, S.; Sanne, I.; Boulle, A.; et al. Effectiveness of the Ad26.COV2.S vaccine in health-care workers in South Africa (the Sisonke study): Results from a single-arm, open-label, phase 3B, implementation study. Lancet 2022, 399, 1141–1153. [Google Scholar] [CrossRef]
- Corchado-Garcia, J.; Puyraimond-Zemmour, D.; Hughes, T.; Cristea-Platon, T.; Lenehan, P.; Pawlowski, C.; Bade, S.; O’Horo, J.C.; Gores, G.J.; Williams, A.W.; et al. Real-world effectiveness of Ad26.COV2.S adenoviral vector vaccine for COVID-19. medRxiv 2021. 2021.2004.2027.21256193. [Google Scholar] [CrossRef]
- Polinski, J.M.; Weckstein, A.R.; Batech, M.; Kabelac, C.; Kamath, T.; Harvey, R.; Jain, S.; Rassen, J.A.; Khan, N.; Schneeweiss, S. Effectiveness of the Single-Dose Ad26.COV2.S COVID Vaccine. medRxiv 2021. 2021.2009.2010.21263385. [Google Scholar] [CrossRef]
- Our World in Data COVID-19 Data Explorer. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer (accessed on 11 September 2022).
- Sa, S.; Lee, C.W.; Shim, S.R.; Yoo, H.; Choi, J.; Kim, J.H.; Lee, K.; Hong, M.; Han, H.W. The Safety of mRNA-1273, BNT162b2 and JNJ-78436735 COVID-19 Vaccines: Safety Monitoring for Adverse Events Using Real-World Data. Vaccines 2022, 10, 320. [Google Scholar] [CrossRef] [PubMed]
- Ezell, B.; Lynch, C.J.; Hester, P.T. Methods for Weighting Decisions to Assist Modelers and Decision Analysts: A Review of Ratio Assignment and Approximate Techniques. Appl. Sci. 2021, 11, 10397. [Google Scholar] [CrossRef]
- Prugger, C.; Spelsberg, A.; Keil, U.; Erviti, J.; Doshi, P. Evaluating COVID-19 vaccine efficacy and safety in the post-authorisation phase. BMJ 2021, 375, e067570. [Google Scholar] [CrossRef] [PubMed]
- Angelis, A.; Phillips, L.D. Advancing structured decision-making in drug regulation at the FDA and EMA. Br. J. Clin. Pharmacol. 2021, 87, 395–405. [Google Scholar] [CrossRef]
- Lackey, L.; Thompson, G.; Eggers, S. FDA’s Benefit-Risk Framework for Human Drugs and Biologics: Role in Benefit-Risk Assessment and Analysis of Use for Drug Approvals. Ther. Innov. Regul. Sci. 2021, 55, 170–179. [Google Scholar] [CrossRef]
- Oh, S.; Purja, S.; Shin, H.; Kim, M.S.; Park, S.; Kronbichler, A.; Smith, L.; Eisenhut, M.; Shin, J.I.; Kim, E. Efficacy, Immunogenicity, and Safety of COVID-19 Vaccines in Randomized Control Trials in the Pre-Delta Era: A Systematic Review and Network Meta-Analysis. Vaccines 2022, 10, 1572. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, K.; Shavaleh, R.; Forouhi, M.; Disfani, H.F.; Kamandi, M.; Oskooi, R.K.; Foogerdi, M.; Soltani, M.; Rahchamani, M.; Mohaddespour, M.; et al. The effectiveness of COVID-19 vaccines in reducing the incidence, hospitalization, and mortality from COVID-19: A systematic review and meta-analysis. Front. Public Health 2022, 10, 873596. [Google Scholar] [CrossRef]
- Alzarea, A.I.; Khan, Y.H.; Alatawi, A.D.; Alanazi, A.S.; Alzarea, S.I.; Butt, M.H.; Almalki, Z.S.; Alahmari, A.K.; Mallhi, T.H. Surveillance of Post-Vaccination Side Effects of COVID-19 Vaccines among Saudi Population: A Real-World Estimation of Safety Profile. Vaccines 2022, 10, 924. [Google Scholar] [CrossRef]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Khillan, R.; Mishra, Y.; Khurana, S. The safety profile of COVID-19 vaccinations in the United States. Am. J. Infect. Control. 2022, 50, 15–19. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Description | |
|---|---|---|
| Benefits | Vaccine effect in adults aged ≥18 | Vaccine efficacy to prevent the occurrence of COVID-19 in adult (age ≥ 18) after full dose of vaccines |
| Vaccine effect in seniors aged ≥60 or ≥65 | Vaccine efficacy to prevent the occurrence of COVID-19 in people aged 60 and over (or age ≥ 65) after full dose of vaccines | |
| Preventing severe COVID-19 | Vaccine efficacy to prevent severe COVID-19 Severe COVID-19: severe systemic illness with medical care including death | |
| Risks | Adverse events | Adverse events including solicited (local and systemic) and unsolicited AEs after vaccination |
| Serious adverse events | Serious adverse events including any medical complication that, at any dose, poses a risk of death is life-threatening, necessitates hospitalization or an extension of hospitalization, causes persistent or severe disability, or impairment of function | |
| Criteria | Pre-Authorization | Post-Authorization | ||||||
|---|---|---|---|---|---|---|---|---|
| BNT162b2 | mRNA-1273 | ChAdOx1-S | Ad26.COV.2 | BNT162b2 | mRNA-1273 | ChAdOx1-S | Ad26.COV.2 | |
| Benefits | ||||||||
| VE, age ≥ 18 | 90.0 | 88.2 | 48.0 | 33.8 | 80.0 | 74.0 | 44.0 | 42.0 |
| VE, age ≥ 60 (or 65) | 89.4 | 72.8 | 67.0 | 52.6 | 64.0 | 66.0 | 66.0 | 42.0 |
| Severe COVID-19 | 32.8 | 100.0 | 100.0 | 53.4 | 78.0 | 82.0 | 96.0 | 56.0 |
| Risks | ||||||||
| AEs | 41.6 | 33.5 | 51.9 | 60.5 | 86.5 | 78.4 | 71.8 | 49.1 |
| Serious AEs | 42.0 | 35.0 | 53.0 | 62.0 | 89.3 | 89.7 | 75.8 | 72.9 |
| Criteria | Weight | Pre-Authorization | Post-Authorization | ||||||
|---|---|---|---|---|---|---|---|---|---|
| mRNA-1273 | ChAdOx1-S | BNT162b2 | Ad26.COV.2 | mRNA-1273 | ChAdOx1-S | BNT162b2 | Ad26.COV.2 | ||
| BR score (rank) | 67.0 (1) | 65.4 (2) | 57.7 (3) | 52.7 (4) | 78.7 (2) | 72.1 (3) | 79.7 (1) | 53.6 (4) | |
| Benefits (rank) | 53.6 (1) | 44.9 (2) | 41.3 (3) | 28.7 (4) | 45.4 (1)\ | 43.1 (3) | 45.2 (2) | 28.9 (4) | |
| VE, age ≥ 18 | 0.188 | 16.6 | 9.0 | 16.9 | 6.4 | 13.9 | 8.3 | 15.0 | 7.9 |
| VE, age ≥ 60 (or 65) | 0.188 | 13.7 | 12.6 | 16.8 | 9.9 | 12.4 | 12.4 | 12.0 | 7.9 |
| Severe COVID-19 | 0.233 | 23.3 | 23.3 | 7.6 | 12.4 | 19.1 | 22.4 | 18.2 | 13.1 |
| Risks (rank) | 13.4 (4) | 20.5 (2) | 16.4 (3) | 24.0 (1) | 33.3 (2) | 29.0 (3) | 34.5 (1) | 24.7 (4) | |
| AEs | 0.158 | 5.3 | 8.2 | 6.6 | 9.5 | 12.4 | 11.3 | 13.7 | 7.7 |
| Serious AEs | 0.233 | 8.1 | 12.3 | 9.8 | 14.5 | 20.9 | 17.7 | 20.8 | 17.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, K.-H.; Kwon, S.-H.; Na, H.-J.; Baek, Y.; Kim, I.; Lee, E.-K. Quantitative Benefit–Risk Assessment of COVID-19 Vaccines Using the Multi-Criteria Decision Analysis. Vaccines 2022, 10, 2029. https://doi.org/10.3390/vaccines10122029
Son K-H, Kwon S-H, Na H-J, Baek Y, Kim I, Lee E-K. Quantitative Benefit–Risk Assessment of COVID-19 Vaccines Using the Multi-Criteria Decision Analysis. Vaccines. 2022; 10(12):2029. https://doi.org/10.3390/vaccines10122029
Chicago/Turabian StyleSon, Kyung-Hwa, Sun-Hong Kwon, Hye-Jung Na, Youngsuk Baek, Inok Kim, and Eui-Kyung Lee. 2022. "Quantitative Benefit–Risk Assessment of COVID-19 Vaccines Using the Multi-Criteria Decision Analysis" Vaccines 10, no. 12: 2029. https://doi.org/10.3390/vaccines10122029
APA StyleSon, K.-H., Kwon, S.-H., Na, H.-J., Baek, Y., Kim, I., & Lee, E.-K. (2022). Quantitative Benefit–Risk Assessment of COVID-19 Vaccines Using the Multi-Criteria Decision Analysis. Vaccines, 10(12), 2029. https://doi.org/10.3390/vaccines10122029