
Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 or Post-Vaccination in Libyan Population: Comparison of Four Vaccines

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants and Study Design
2.2. Detection of SARS-CoV-2 Specific Serum Antibodies
2.3. Statistical Analysis
3. Results
3.1. Participant Selection and Characteristics of Study Group
3.2. Overall View of Vaccinations and Seropositivity
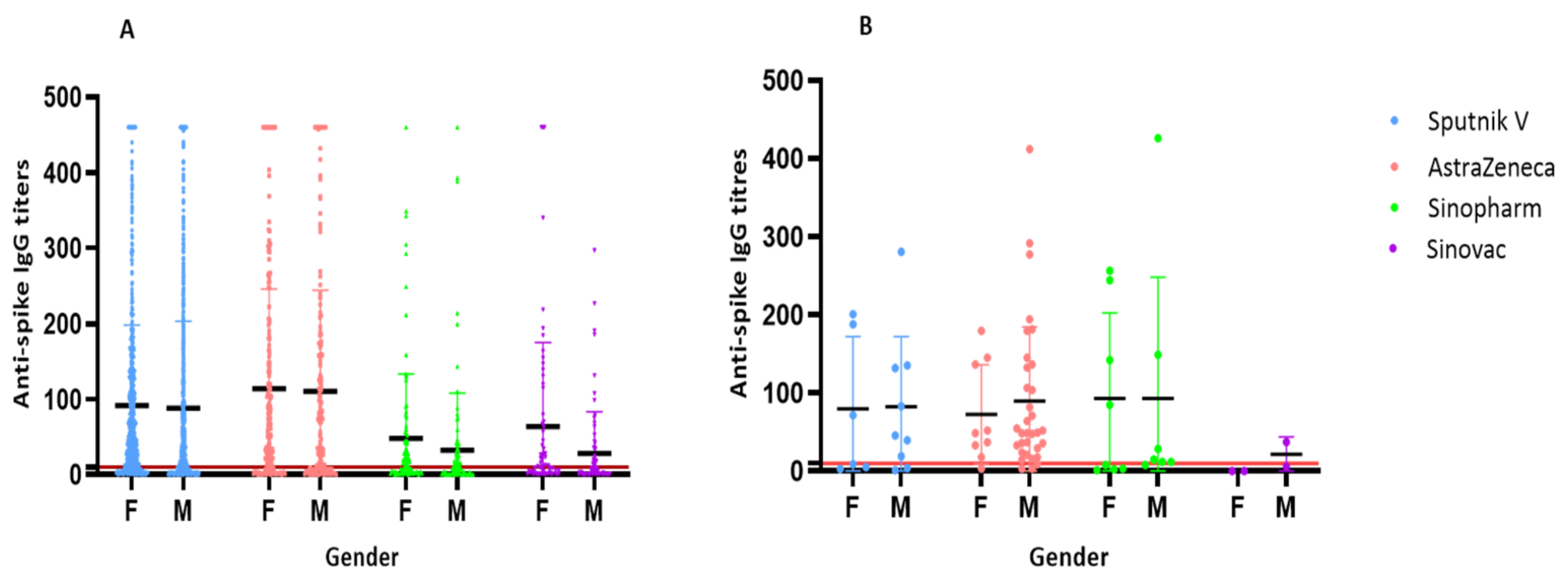
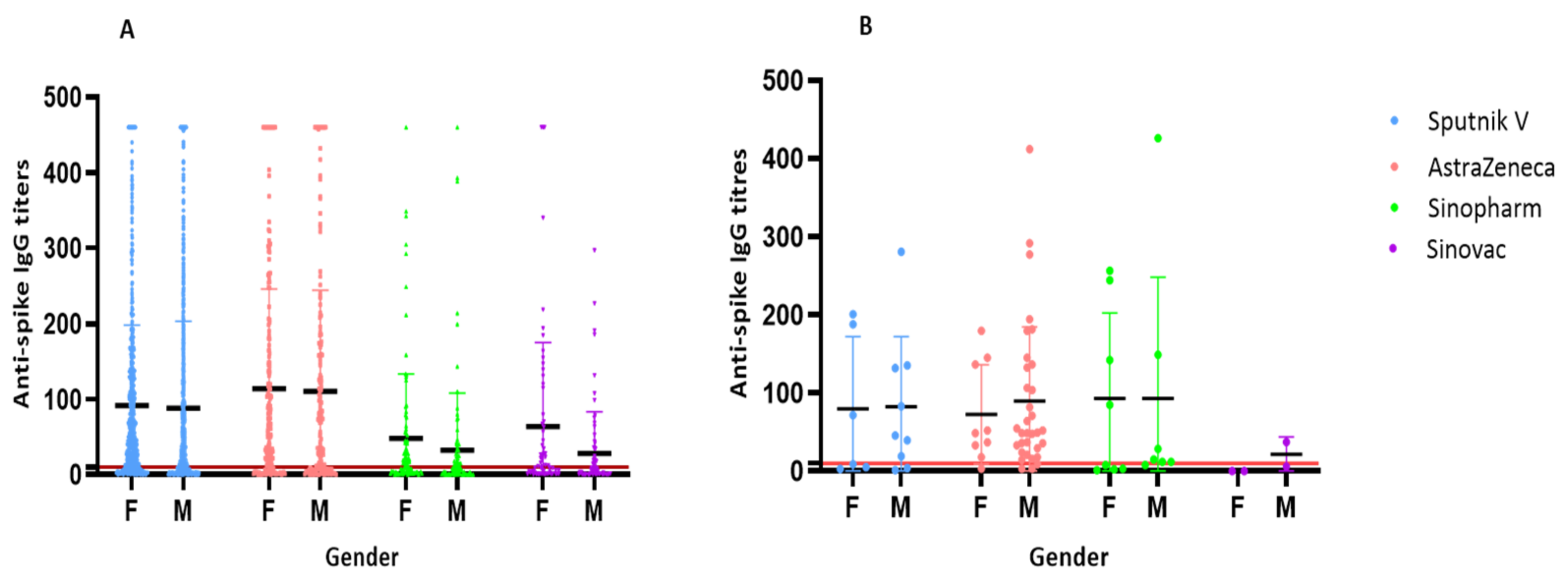
3.3. Analysis of Seropositivity by Age, Vaccination, and Prior Infection Status
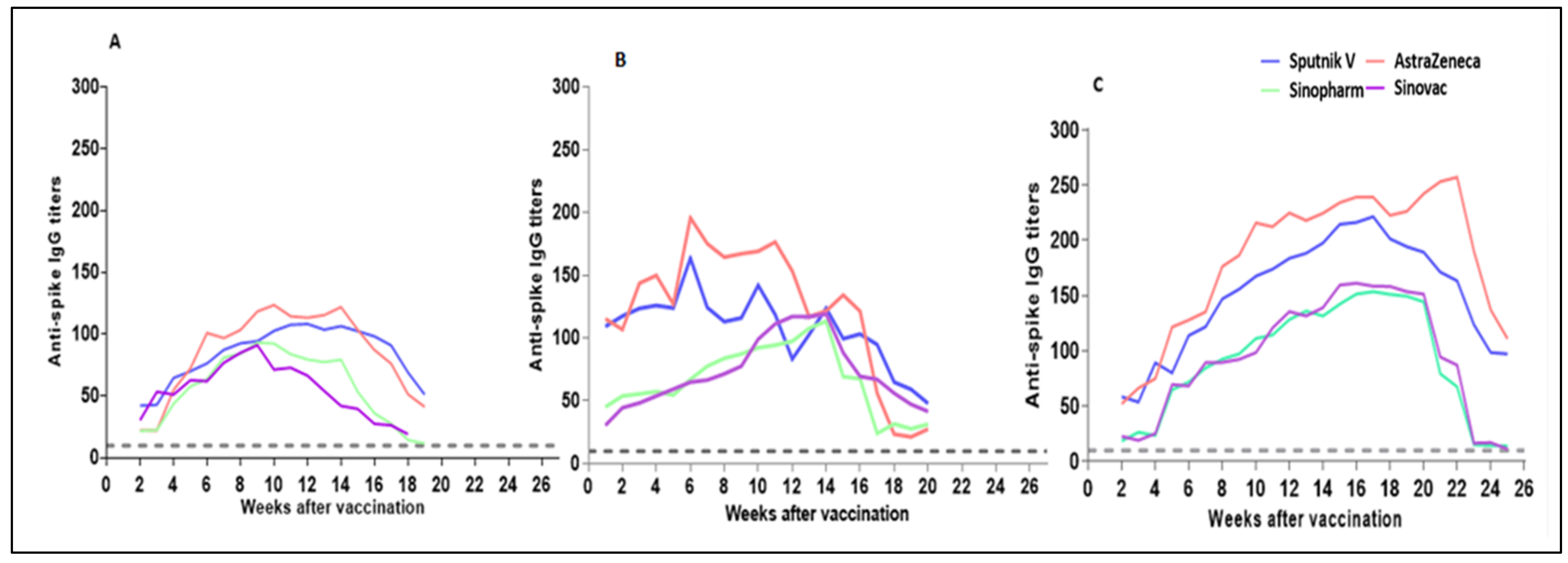
3.4. Waning Dynamics of IgG Anti-Spike RBD Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weekly Epidemiological Update on COVID-19 - 11 January 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---11-january-2022 (accessed on 10 January 2022).
- Yoo, J.-H. What We Do Know and Do Not Yet Know about COVID-19 Vaccines as of the Beginning of the Year 2021. J. Korean Med. Sci. 2021, 36, e54. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.-X.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and Immunological Assessment of Asymptomatic SARS-CoV-2 Infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Altawalah, H. Antibody Responses to Natural SARS-CoV-2 Infection or after COVID-19 Vaccination. Vaccines 2021, 9, 910. [Google Scholar] [CrossRef] [PubMed]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Sci. Immunol. 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody responses to SARS-CoV-2 in patients with novel coronavirus disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What Defines an Efficacious COVID-19 Vaccine? A Review of the Challenges Assessing the Clinical Efficacy of Vaccines against SARS-CoV-2. Lancet. Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef]
- Dinnes, J.; Deeks, J.J.; Adriano, A.; Berhane, S.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; Beese, S.; et al. Rapid, Point-of-Care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2020, 2020, CD013705. [Google Scholar] [CrossRef]
- Gudbjartsson, D.F.; Norddahl, G.L.; Melsted, P.; Gunnarsdottir, K.; Holm, H.; Eythorsson, E.; Arnthorsson, A.O.; Helgason, D.; Bjarnadottir, K.; Ingvarsson, R.F.; et al. Humoral immune response to SARS-CoV-2 in iceland. N. Engl. J. Med. 2020, 383, 1724–1734. [Google Scholar] [CrossRef]
- Jeyanathan, M.; Afkhami, S.; Smaill, F.; Miller, M.S.; Lichty, B.D.; Xing, Z. Immunological considerations for COVID-19 vaccine strategies. Nat. Rev. Immunol. 2020, 20, 615–632. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- He, Z.; Ren, L.; Yang, J.; Guo, L.; Feng, L.; Ma, C.; Wang, X.; Leng, Z.; Tong, X.; Zhou, W.; et al. Seroprevalence and humoral immune durability of Anti-SARS-CoV-2 antibodies in Wuhan, China: A longitudinal, population-level, cross-sectional study. Lancet 2021, 397, 1075–1084. [Google Scholar] [CrossRef]
- National Center for Disease Control. Available online: https://ncdc.org.ly/Ar/ (accessed on 31 March 2022).
- León, T.M.; Dorabawila, V.; Nelson, L.; Lutterloh, E.; Bauer, U.E.; Backenson, B. COVID-19 cases and hospitalizations by COVID-19 vaccination status and previous COVID-19 diagnosis—California and New York, May–November 2021. MMWR Recomm. Rep. 2022, 71, 125–131. [Google Scholar] [CrossRef]
- Ma, H.; Zeng, W.; He, H.; Zhao, D.; Jiang, D.; Zhou, P.; Cheng, L.; Li, Y.; Ma, X.; Jin, T. Serum IgA, IgM, and IgG Responses in COVID-19. Cell Mol. Immunol. 2020, 17, 773–775. [Google Scholar] [CrossRef]
- Mantus, G.; Nyhoff, L.E.; Edara, V.-V.; Zarnitsyna, V.I.; Ciric, C.R.; Flowers, M.W.; Norwood, C.; Ellis, M.; Hussaini, L.; Manning, K.E.; et al. Pre-Existing SARS-CoV-2 immunity influences potency, breadth, and durability of the humoral response to SARS-CoV-2 vaccination. Cell Rep. Med. 2022, 3, 100603. [Google Scholar] [CrossRef]
- Callegaro, A.; Borleri, D.; Farina, C.; Napolitano, G.; Valenti, D.; Rizzi, M.; Maggiolo, F. Antibody response to SARS-CoV-2 vaccination is extremely vivacious in subjects with previous SARS-CoV-2 infection. J. Med. Virol. 2021, 93, 4612–4615. [Google Scholar] [CrossRef]
- Wei, J.; Stoesser, N.; Matthews, P.C.; Ayoubkhani, D.; Studley, R.; Bell, I.; Bell, J.I.; Newton, J.N.; Farrar, J.; Diamond, I.; et al. Antibody Responses to SARS-CoV-2 Vaccines in 45,965 Adults from the General Population of the United Kingdom. Nat. Microbiol. 2021, 6, 1140–1149. [Google Scholar] [CrossRef]
- Tukhvatulin, A.I.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; Botikov, A.G.; et al. An Open, Non-Randomised, Phase 1/2 Trial on the Safety, Tolerability, and Immunogenicity of Single-Dose Vaccine “Sputnik Light” for Prevention of Coronavirus Infection in Healthy Adults. Lancet Reg. Health-Eur. 2021, 11, 100241. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 NCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Jeewandara, C.; Aberathna, I.S.; Pushpakumara, P.D.; Kamaladasa, A.; Guruge, D.; Wijesinghe, A.; Gunasekera, B.; Tanussiya, S.; Kuruppu, H.; Ranasinghe, T.; et al. Persistence of Antibody and T Cell Responses to the Sinopharm/BBIBP-CorV Vaccine in Sri Lankan Individuals. medRxiv Prepr. Serv. Health Sci. 2021. [Google Scholar] [CrossRef]
- Vályi-Nagy, I.; Matula, Z.; Gönczi, M.; Tasnády, S.; Bekő, G.; Réti, M.; Ajzner, É.; Uher, F. Comparison of antibody and t Cell responses elicited by BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) vaccines against SARS-CoV-2 in healthy adult humans. GeroScience 2021, 43, 2321–2331. [Google Scholar] [CrossRef]
- Alqassieh, R.; Suleiman, A.; Abu-Halaweh, S.; Santarisi, A.; Shatnawi, O.; Shdaifat, L.; Tarifi, A.; Al-Tamimi, M.; Al-Shudifat, A.E.; Alsmadi, H.; et al. Pfizer-BioNTech and sinopharm: A comparative study on post-vaccination antibody titers. Vaccines 2021, 9, 1223. [Google Scholar] [CrossRef] [PubMed]
- Mallapaty, S. China’s COVID vaccines have been crucial—Now immunity is waning. Nature 2021, 598, 398–399. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health-Eur. 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; Alahmad, B.; Al-Shammari, A.A.; Alterki, A.; Hammad, M.; Cherian, P.; Alkhairi, I.; Sindhu, S.; Thanaraj, T.A.; Mohammad, A.; et al. Previous COVID-19 Infection and Antibody Levels After Vaccination. Front. Public Health 2021, 9, 778243. [Google Scholar] [CrossRef]
- Vicenti, I.; Gatti, F.; Scaggiante, R.; Boccuto, A.; Zago, D.; Basso, M.; Dragoni, F.; Zazzi, M.; Parisi, S.G. Single-dose BNT162b2 MRNA COVID-19 vaccine significantly boosts neutralizing antibody response in health care workers recovering from asymptomatic or mild natural SARS-CoV-2 infection. Int. J. Infect. Dis. 2021, 108, 176–178. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Vaccine | n | Seropositive | Seronegative | ||||
|---|---|---|---|---|---|---|---|
| Females | Males | Total | n | % | n | % | |
| Sputnik V | 1874 | 2282 | 4156 | 2988 | 71.9 | 1168 | 28.1 |
| AstraZeneca | 479 | 586 | 1065 | 786 | 73.8 | 279 | 26.2 |
| Sinopharm | 237 | 257 | 494 | 259 | 52.4 | 235 | 47.6 |
| Sinovac | 306 | 307 | 613 | 320 | 52.2 | 293 | 47.8 |
| All vaccines | 2896 | 3432 | 6328 | 4353 | 68.8 | 1975 | 31.2 |
| 1 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ≤35 Years | 36–45 Years | 46–55 Years | 56–65 Years | >65 Years | ||||||
| p = 0.0001 | p < 0.0001 | p = 0.0003 | p < 0.0001 | p = 0.0002 | ||||||
| N | % | N | % | N | % | N | % | N | % | |
| Vaccinated with one dose Apparent Prior infection | 358 | 100 | 582 | 100 | 419 | 100 | 308 | 100 | 383 | 100 |
| No prior infection | 585 | 87.9 | 637 | 100 | 678 | 100 | 443 | 100 | 354 | 100 |
| Vaccinated with two doses EmaApparent Prior infection | 150 | 100 | 149 | 94.2 | 164 | 100 | 56 | 97.0 | 227 | 93.8 |
| No prior infection | 210 | 72.8 | 129 | 79.3 | 184 | 82.8 | 126 | 86.9 | 188 | 90.9 |
| 2 | ||||||||||
| ≤35 years | 36–45 years | 46–55 years | 56–65 years | >65 years | ||||||
| p= 0.0001 | p< 0.0001 | p= 0.0003 | p< 0.0001 | p= 0.0002 | ||||||
| n | % | n | % | n | % | n | % | n | % | |
| Unvaccinated EmaPrior infection | 386 | 77.0 | 320 | 96.0 | 307 | 93.0 | 147 | 95.0 | 40 | 88.8 |
| No prior infection | 597 | 62.8 | 484 | 74.3 | 536 | 82.0 | 206 | 92.0 | 102 | 78.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebrahim, F.; Tabal, S.; Lamami, Y.; Alhudiri, I.M.; El Meshri, S.E.; Al Dwigen, S.; Arfa, R.; Alboeshi, A.; Alemam, H.A.; Abuhtna, F.; et al. Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 or Post-Vaccination in Libyan Population: Comparison of Four Vaccines. Vaccines 2022, 10, 2002. https://doi.org/10.3390/vaccines10122002
Ebrahim F, Tabal S, Lamami Y, Alhudiri IM, El Meshri SE, Al Dwigen S, Arfa R, Alboeshi A, Alemam HA, Abuhtna F, et al. Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 or Post-Vaccination in Libyan Population: Comparison of Four Vaccines. Vaccines. 2022; 10(12):2002. https://doi.org/10.3390/vaccines10122002
Chicago/Turabian StyleEbrahim, Fawzi, Salah Tabal, Yosra Lamami, Inas M. Alhudiri, Salah Edin El Meshri, Samira Al Dwigen, Ramadan Arfa, Asma Alboeshi, Hafsa A. Alemam, Fauzia Abuhtna, and et al. 2022. "Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 or Post-Vaccination in Libyan Population: Comparison of Four Vaccines" Vaccines 10, no. 12: 2002. https://doi.org/10.3390/vaccines10122002
APA StyleEbrahim, F., Tabal, S., Lamami, Y., Alhudiri, I. M., El Meshri, S. E., Al Dwigen, S., Arfa, R., Alboeshi, A., Alemam, H. A., Abuhtna, F., Altrhouni, R., Milad, M. B., Elgriw, N. A., Ruaua, M. A., Abusrewil, Z., Harroush, W., Jallul, M., Ali, F. S., Eltaib, F., & Elzagheid, A. (2022). Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 or Post-Vaccination in Libyan Population: Comparison of Four Vaccines. Vaccines, 10(12), 2002. https://doi.org/10.3390/vaccines10122002