
A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19
Abstract
1. Introduction
2. Materials and Methods
2.1. Routine Histology
2.2. Immunohistochemistry
2.3. Preparation of Positive Control Samples for the Immunohistochemical Detection of the Vaccine-Induced Spike Protein
2.4. Case Presentation and Description
2.4.1. Clinical History
2.4.2. Autopsy
3. Results
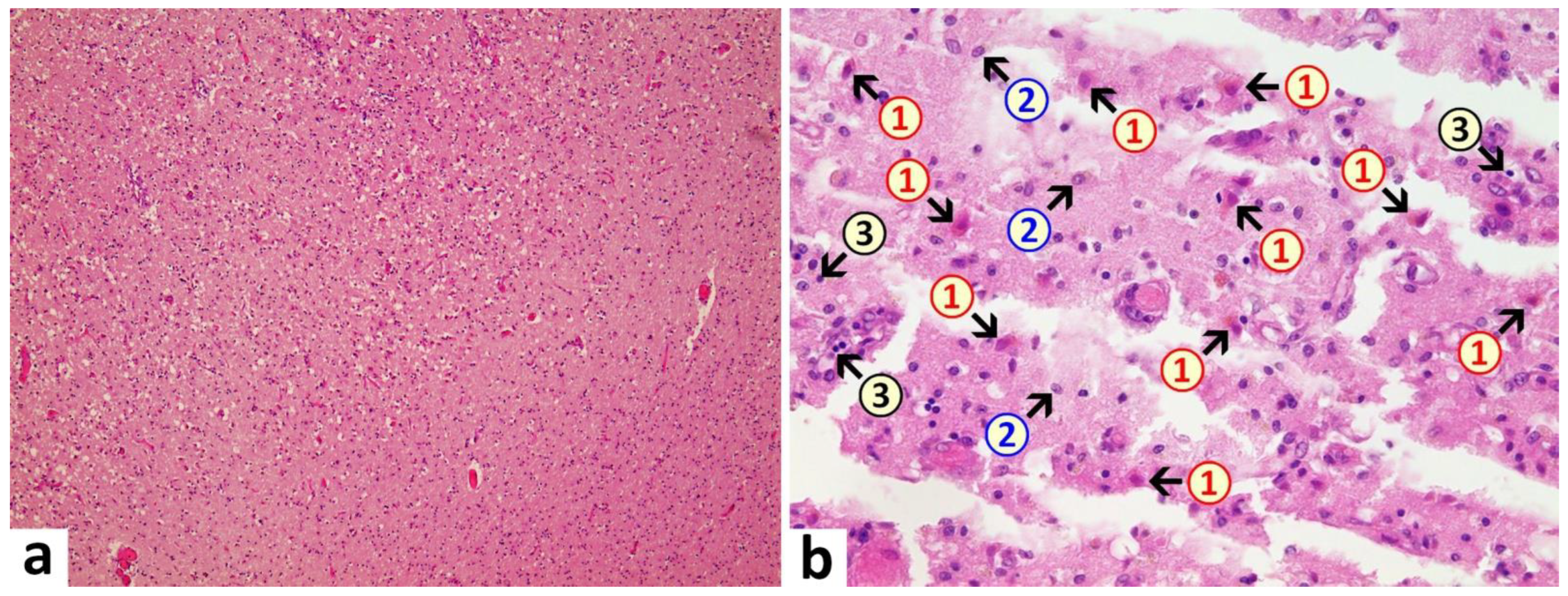
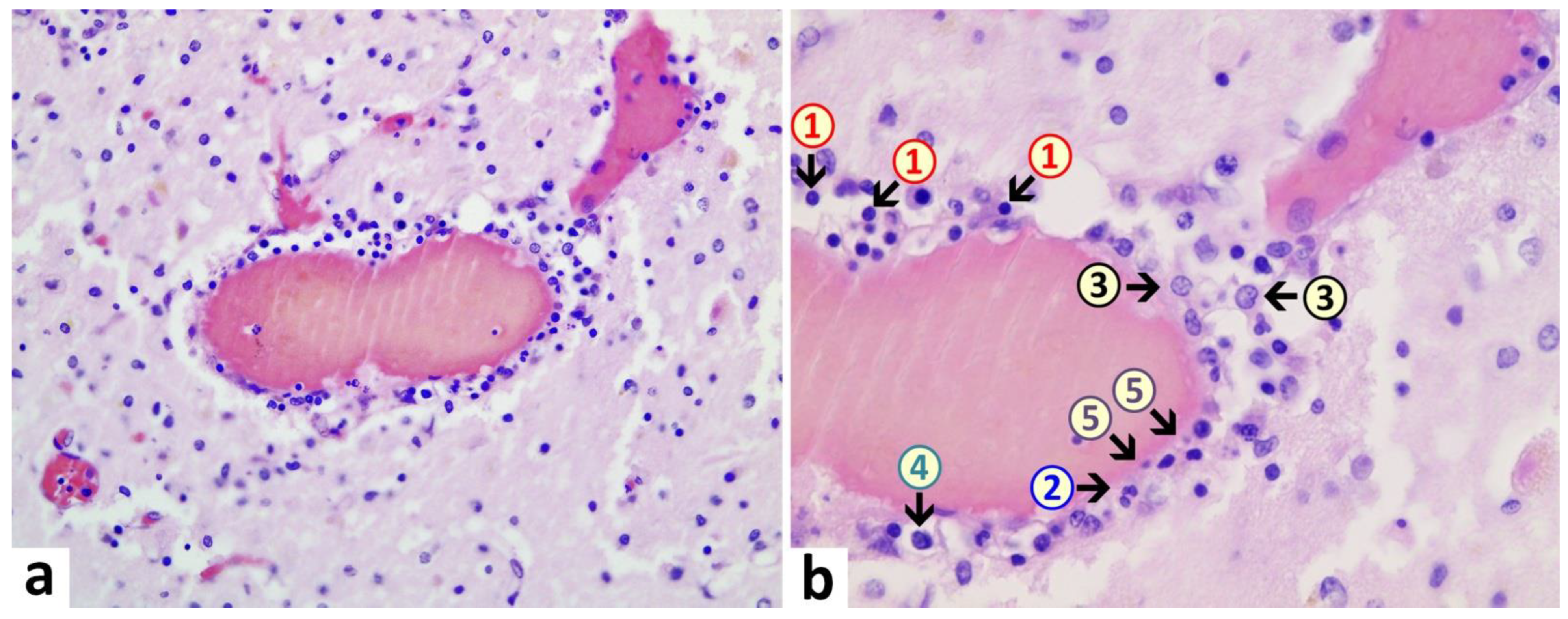
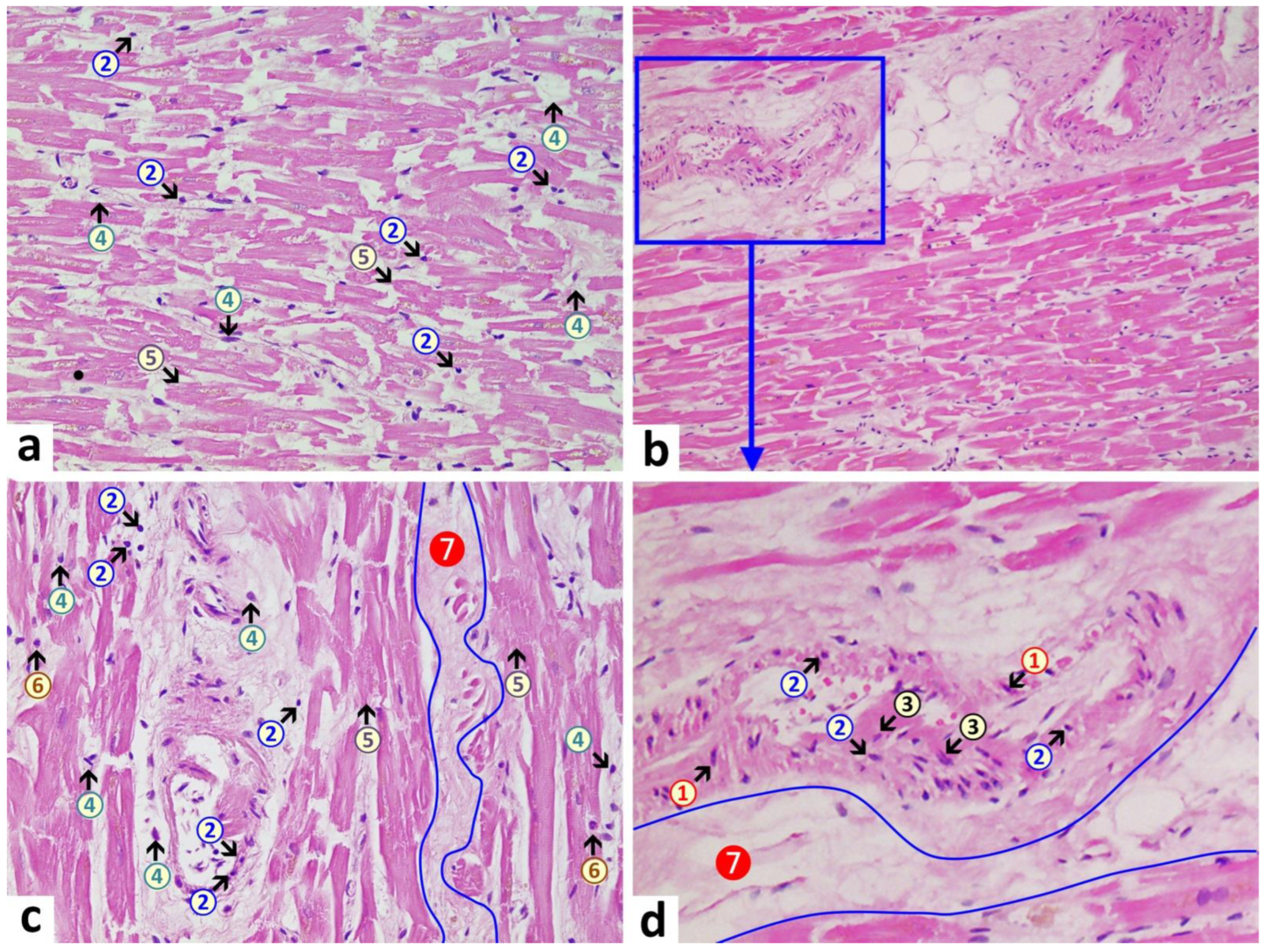
3.1. Autopsy Findings
3.2. Other Findings
- -
- Oral cavity: tongue bite was detected with bleeding under the tongue muscle (tongue bite is common with epileptic seizures).
- -
- Adrenal glands: bilateral mild cortical hyperplasia.
- -
- Colon: the elongated sigmoid colon was elongated with fecal impaction.
- -
- Kidneys: slight diffuse glomerulosclerosis and arterio-sclerosis, renal cortical scars (up to 10 mm in diameter), bilateral mild active nephritis and urocystitis as well as evidence of shock kidney disorder.
- -
- Liver: slight lipofuscinosis.
- -
- Spleen: mild acute splenitis.
- -
- Stomach: mild diffuse gastric mucosal bleeding.
- -
- Thyroid gland: bilateral nodular goiter with chocolate cysts (up to 0.5 cm in diameter).
- -
- Prostate gland: benign nodular prostatic hyperplasia and chronic persistent prostatitis.
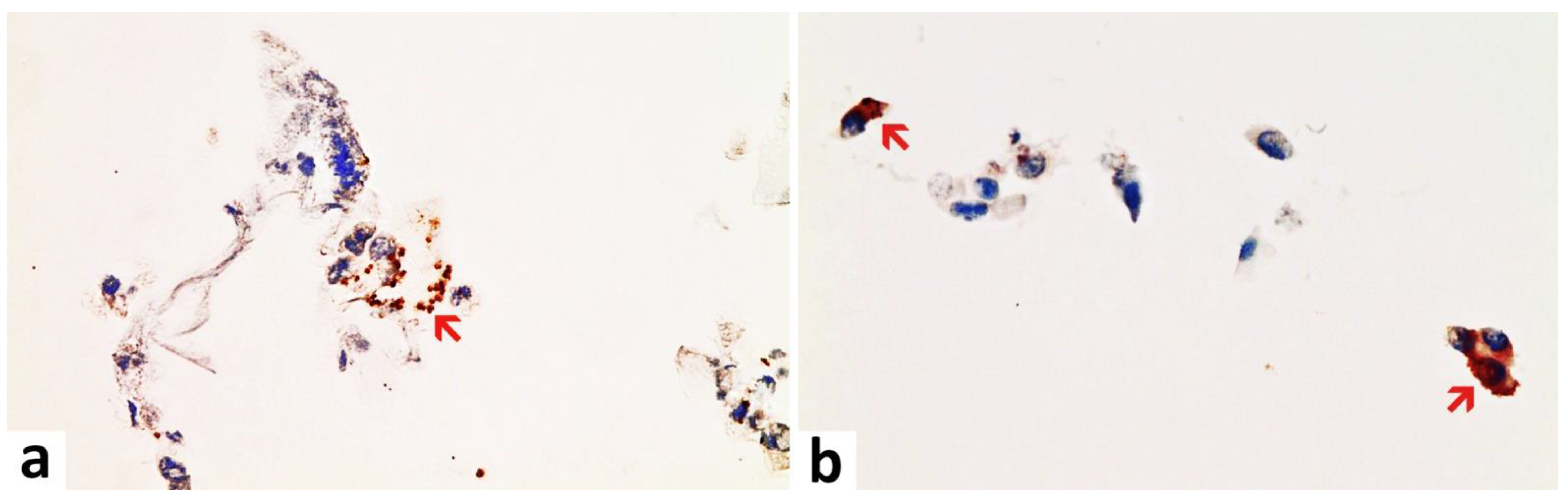
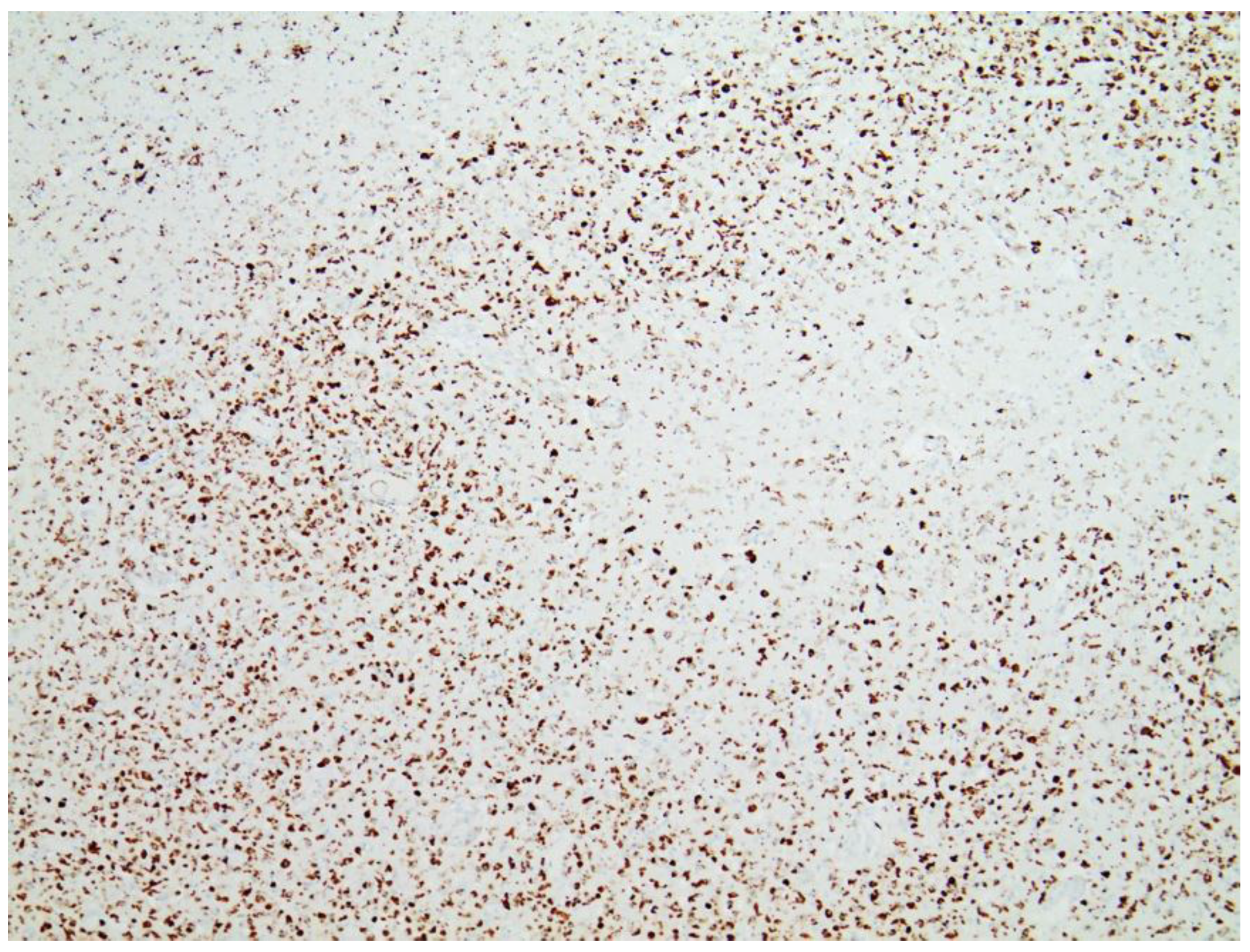
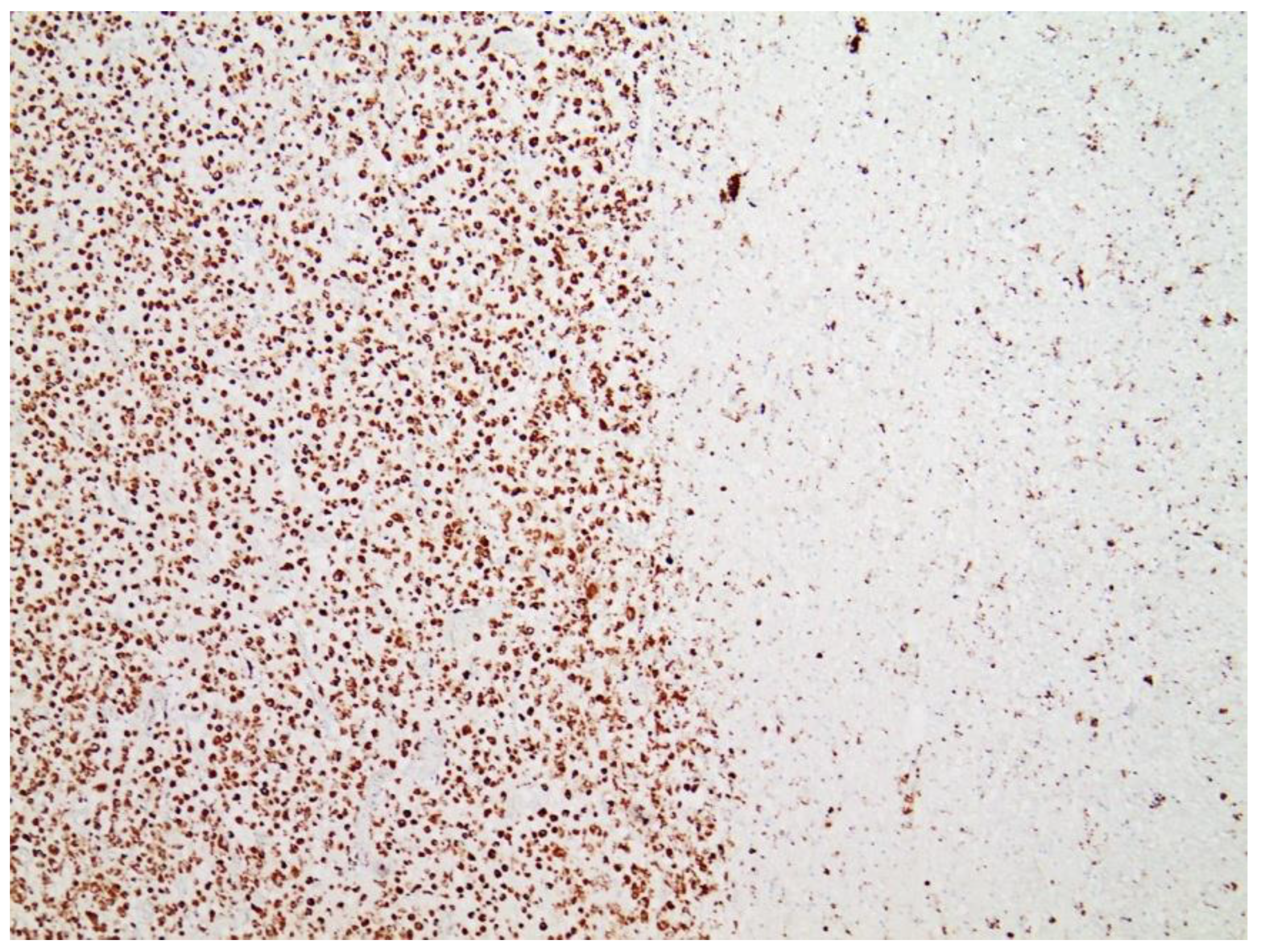
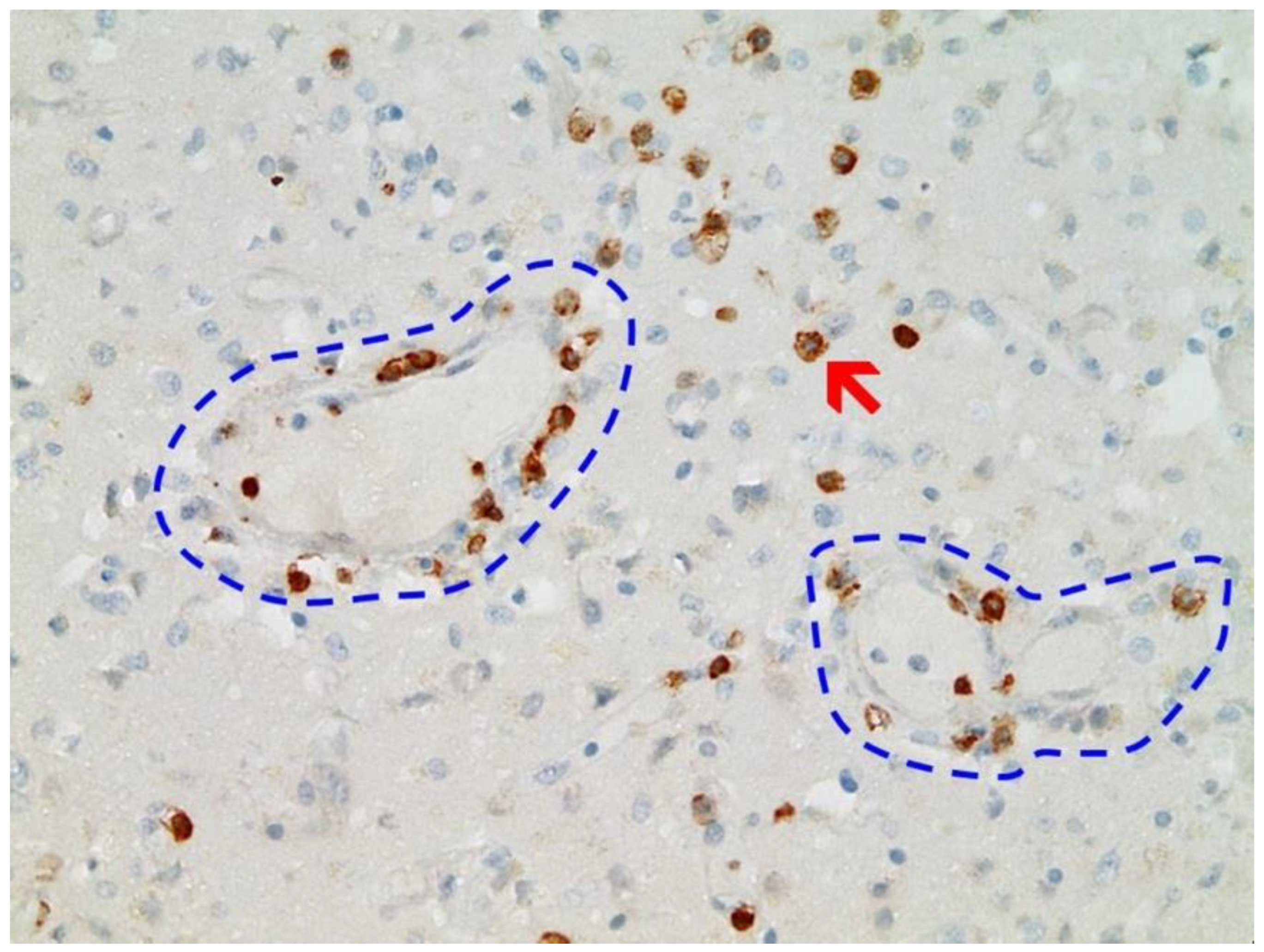
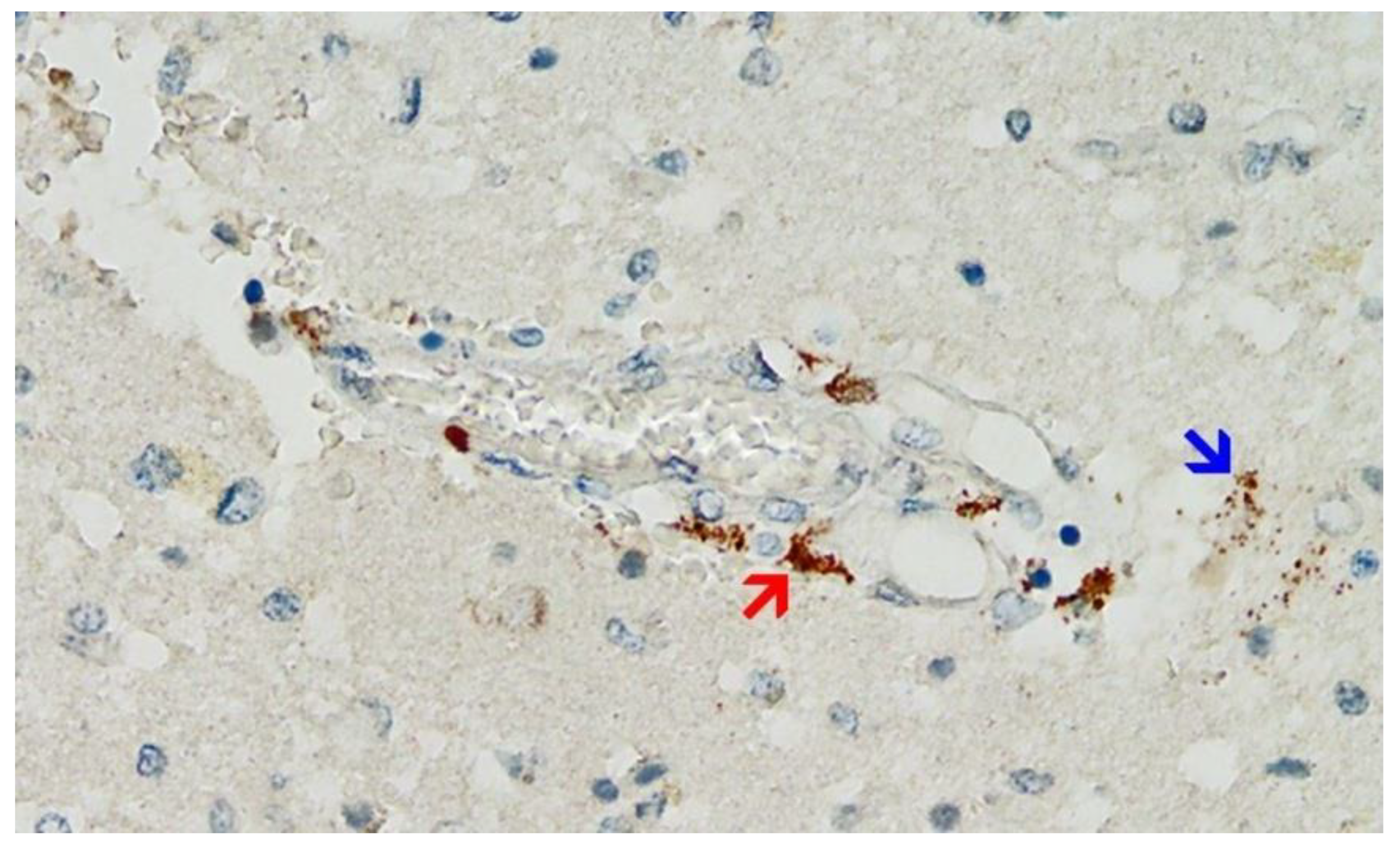
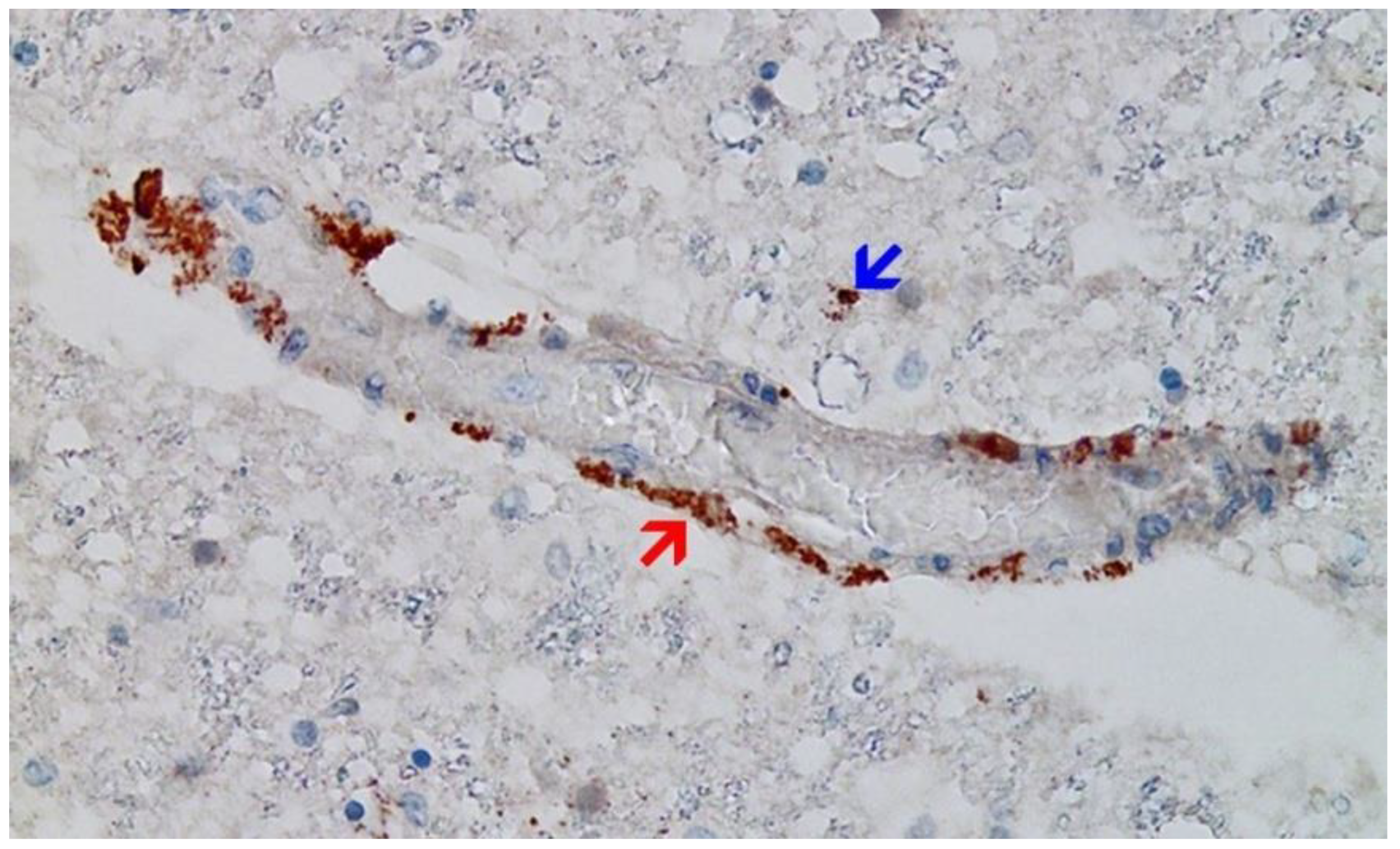
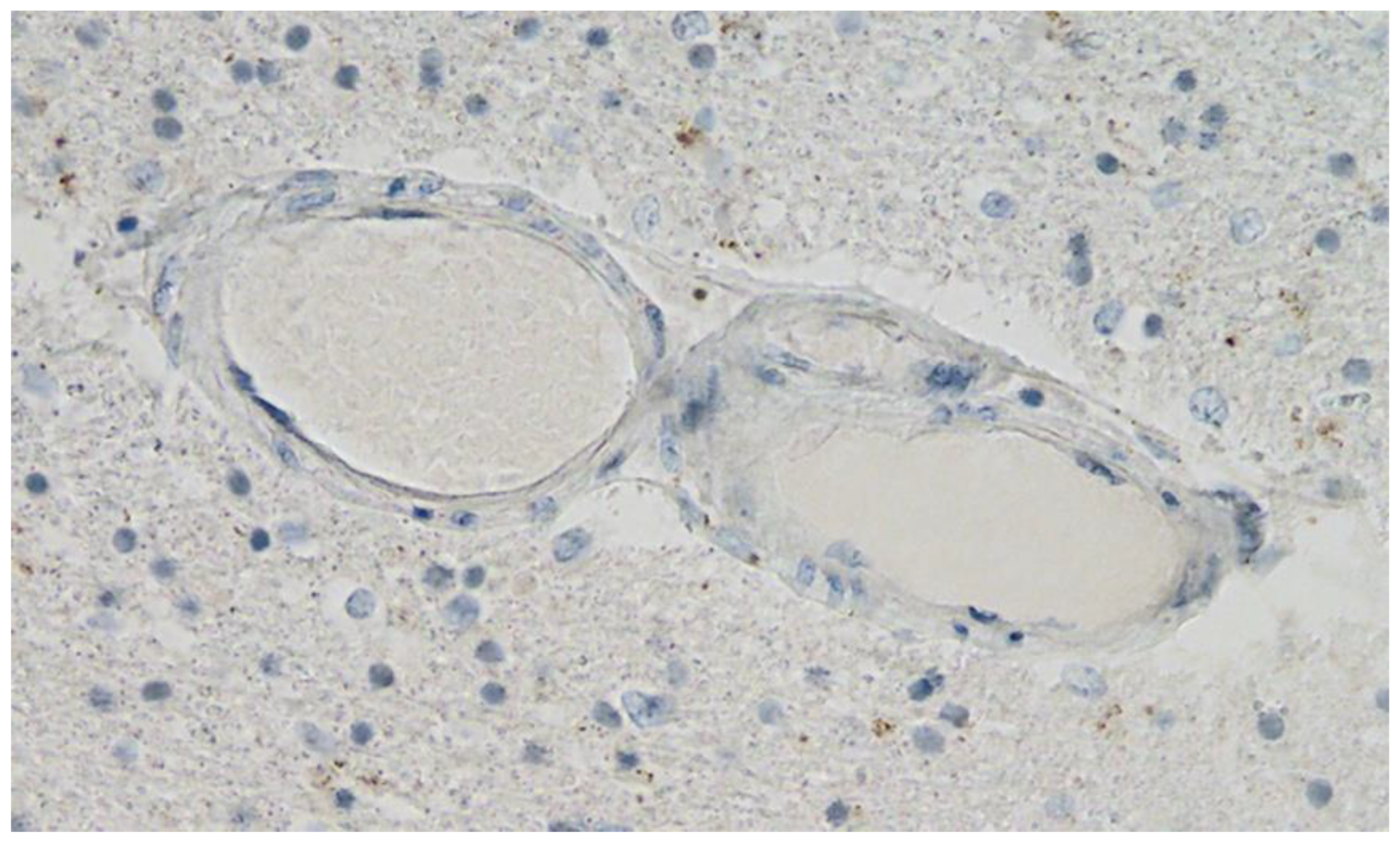
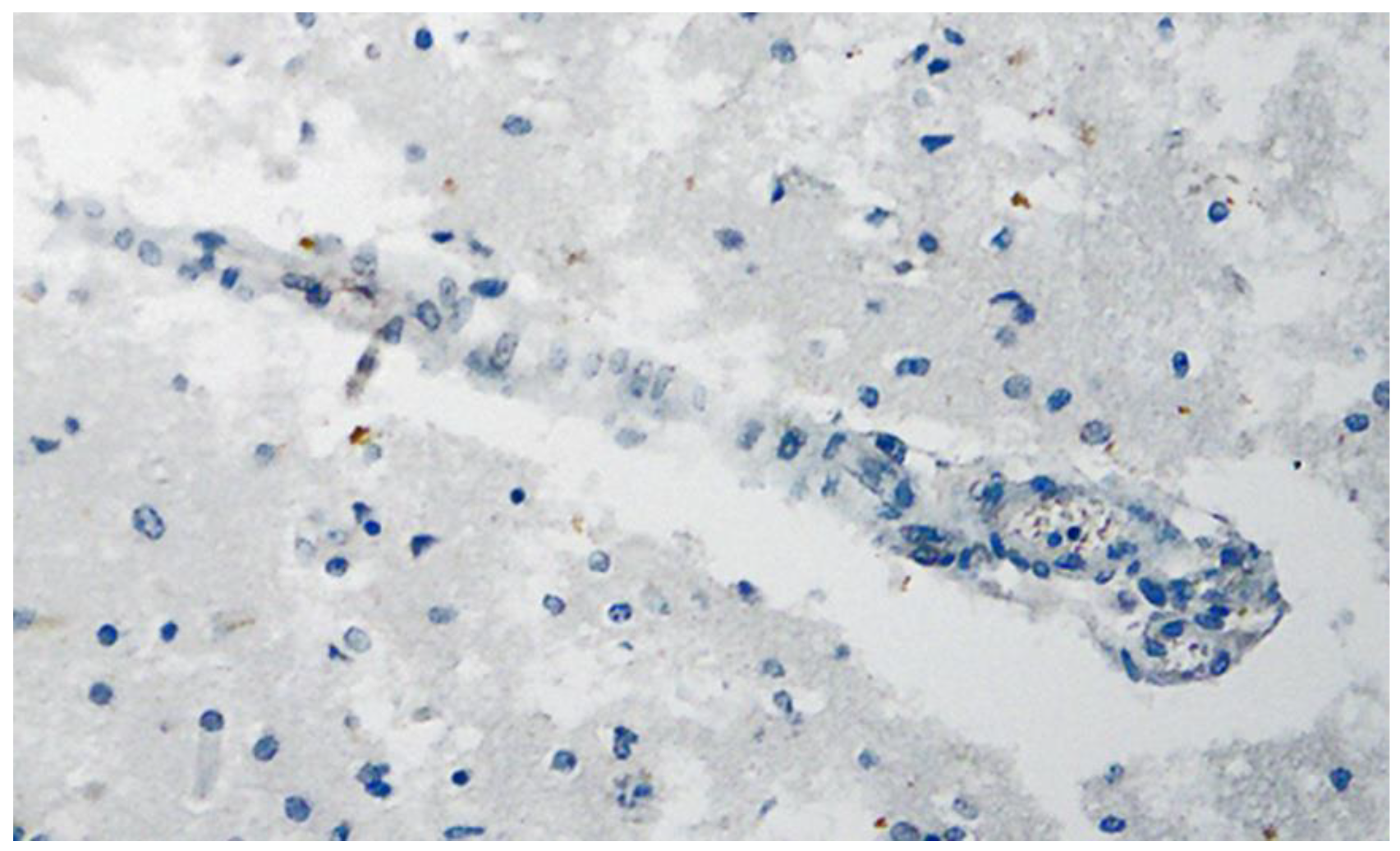
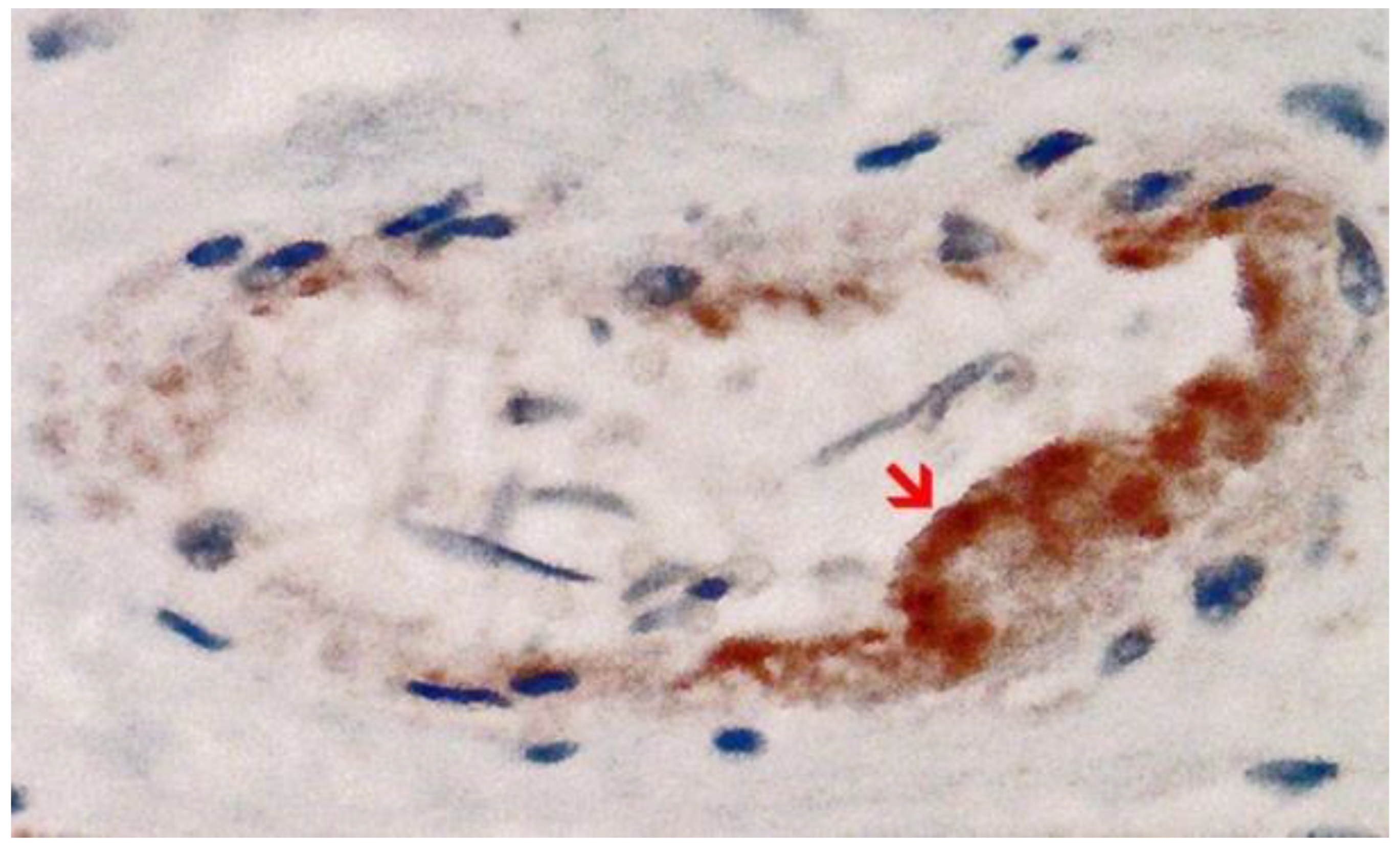
3.3. Immunohistochemical Analyses
3.4. Autopsy-Based Diagnosis
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, W.-H.; Strych, U.; Hotez, P.J.; Bottazzi, M.E. The SARS-CoV-2 Vaccine Pipeline: An Overview. Curr. Trop. Med. Rep. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Sultana, J.; Mazzaglia, G.; Luxi, N.; Cancellieri, A.; Capuano, A.; Ferrajolo, C.; de Waure, C.; Ferlazzo, G.; Trifirò, G. Potential effects of vaccinations on the prevention of COVID-19: Rationale, clinical evidence, risks, and public health considerations. Expert Rev. Vaccines 2020, 19, 919–936. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 2 June 2022).
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing COVID-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Diagnostics Laboratory Emergency Use Listing. Available online: https://www.who.int/teams/regulation-prequalification/eul (accessed on 2 June 2022).
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, P. A phase III study to investigate a vaccine against COVID-19. ISRCTN 2020. [Google Scholar] [CrossRef]
- Polak, S.B.; Van Gool, I.C.; Cohen, D.; von der Thüsen, J.H.; van Paassen, J. A systematic review of pathological findings in COVID-19: A pathophysiological timeline and possible mechanisms of disease progression. Mod. Pathol. 2020, 33, 2128–2138. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Lee, S.; Seo, J.-W.; Kim, M.-J.; Jeon, Y.H.; Park, J.H.; Lee, J.K.; Yeo, N.S. Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J. Korean Med. Sci. 2021, 36, e286. [Google Scholar] [CrossRef]
- Fillon, A.; Sautenet, B.; Barbet, C.; Moret, L.; Thillard, E.M.; Jonville-Béra, A.P.; Halimi, J.M. De novo and relapsing necrotizing vasculitis after COVID-19 vaccination. Clin. Kidney J. 2022, 15, 560–563. [Google Scholar] [CrossRef]
- Gao, J.-J.; Tseng, H.-P.; Lin, C.-L.; Hsu, R.-F.; Lee, M.-H.; Liu, C.-H. Acute encephalitis after COVID-19 vaccination: A case report and literature review. Hum. Vaccines Immunother. 2022, 2082206. [Google Scholar] [CrossRef]
- Jarius, S.; Bieber, N.; Haas, J.; Wildemann, B. MOG encephalomyelitis after vaccination against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2): Case report and comprehensive review of the literature. J. Neurol. 2022, 269, 5198–5212. [Google Scholar] [CrossRef] [PubMed]
- Oshida, S.; Akamatsu, Y.; Matsumoto, Y.; Suzuki, T.; Sasaki, T.; Kondo, Y.; Fujiwara, S.; Kashimura, H.; Kubo, Y.; Ogasawara, K. Intracranial aneurysm rupture within three days after receiving mRNA anti-COVID-19 vaccination: Three case reports. Surg. Neurol. Int. 2022, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Won, J.H.; Byun, S.J.; Oh, B.-M.; Park, S.J.; Seo, H.G. Risk and mortality of aspiration pneumonia in Parkinson’s disease: A nationwide database study. Sci. Rep. 2021, 11, 6597. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Sengoku, R.; Saito, Y.; Kakuta, Y.; Murayama, S.; Imafuku, I. Sudden death in Parkinson’s disease: A retrospective autopsy study. J. Neurol. Sci. 2014, 343, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.-T.; Lin, Y.-Y.; Chiang, W.-F.; Lin, C.-Y.; Chen, M.-H.; Wu, K.-A.; Chan, J.-S.; Kao, Y.-H.; Shyu, H.-Y.; Hsiao, P.-J. COVID-19 vaccine-induced encephalitis and status epilepticus. QJM Mon. J. Assoc. Physicians 2022, 115, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.D.; Ugolini, C.; Jha, P. Two Cases of Post-Moderna COVID-19 Vaccine Encephalopathy Associated with Nonconvulsive Status Epilepticus. Cureus 2021, 13, e16172. [Google Scholar] [CrossRef]
- Werner, J.; Brandi, G.; Jelcic, I.; Galovic, M. New-onset refractory status epilepticus due to autoimmune encephalitis after vaccination against SARS-CoV-2: First case report. Front. Neurol. 2022, 13, 946644. [Google Scholar] [CrossRef]
- Kim, D.; Bresette, C.; Liu, Z.; Ku, D.N. Occlusive thrombosis in arteries. APL Bioeng. 2019, 3, 041502. [Google Scholar] [CrossRef]
- Ludewig, B.; Zinkernagel, R.M.; Hengartner, H. Arterial inflammation and atherosclerosis. Trends Cardiovasc. Med. 2002, 12, 154–159. [Google Scholar] [CrossRef]
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The vascular endothelium: The cornerstone of organ dysfunction in severe SARS-CoV-2 infection. Crit. Care Lond. Engl. 2020, 24, 353. [Google Scholar] [CrossRef]
- Dörschug, A.; Frickmann, H.; Schwanbeck, J.; Yilmaz, E.; Mese, K.; Hahn, A.; Groß, U.; Zautner, A.E. Comparative Assessment of Sera from Individuals after S-Gene RNA-Based SARS-CoV-2 Vaccination with Spike-Protein-Based and Nucleocapsid-Based Serological Assays. Diagnostics 2021, 11, 426. [Google Scholar] [CrossRef]
- Magen, E.; Mukherjee, S.; Bhattacharya, M.; Detroja, R.; Merzon, E.; Blum, I.; Livoff, A.; Shlapobersky, M.; Baum, G.; Talisman, R.; et al. Clinical and Molecular Characterization of a Rare Case of BNT162b2 mRNA COVID-19 Vaccine-Associated Myositis. Vaccines 2022, 10, 1135. [Google Scholar] [CrossRef] [PubMed]
- Röltgen, K.; Nielsen, S.C.A.; Silva, O.; Younes, S.F.; Zaslavsky, M.; Costales, C.; Yang, F.; Wirz, O.F.; Solis, D.; Hoh, R.A.; et al. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell 2022, 185, 1025–1040.e14. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Zhang, J.; Schiavon, C.R.; He, M.; Chen, L.; Shen, H.; Zhang, Y.; Yin, Q.; Cho, Y.; Andrade, L.; et al. SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE2. bioRxiv 2020. bioRxiv:2020.12.04.409144. [Google Scholar] [CrossRef]
- Avolio, E.; Carrabba, M.; Milligan, R.; Kavanagh Williamson, M.; Beltrami, A.P.; Gupta, K.; Elvers, K.T.; Gamez, M.; Foster, R.R.; Gillespie, K.; et al. The SARS-CoV-2 Spike protein disrupts human cardiac pericytes function through CD147 receptor-mediated signalling: A potential non-infective mechanism of COVID-19 microvascular disease. Clin. Sci. 2021, 135, 2667–2689. [Google Scholar] [CrossRef]
- Bansal, S.; Perincheri, S.; Fleming, T.; Poulson, C.; Tiffany, B.; Bremner, R.M.; Mohanakumar, T. Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer-BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines. J. Immunol. Baltim. Md. 1950 2021, 207, 2405–2410. [Google Scholar] [CrossRef]
- Baumeier, C.; Aleshcheva, G.; Harms, D.; Gross, U.; Hamm, C.; Assmus, B.; Westenfeld, R.; Kelm, M.; Rammos, S.; Wenzel, P.; et al. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. Int. J. Mol. Sci. 2022, 23, 6940. [Google Scholar] [CrossRef]
- Yamamoto, M.; Kase, M.; Sano, H.; Kamijima, R.; Sano, S. Persistent varicella zoster virus infection following mRNA COVID-19 vaccination was associated with the presence of encoded spike protein in the lesion. J. Cutan. Immunol. Allergy 2022. [Google Scholar] [CrossRef]
- TGA Therapeutic Goods Administration. Australian Government 2021: Non Clinical Evaluation Report of BNT162b2 [mRNA] COVID-19 vaccine (COMIRNATY™) Submission No: PM-2020-05461-1-2 Sponsor: Pfizer Australia Pty Ltd. Available online: https://www.tga.gov.au/sites/default/files/foi-2389-06.pdf (accessed on 2 June 2022).
- Ancau, M.; Liesche-Starnecker, F.; Niederschweiberer, J.; Krieg, S.M.; Zimmer, C.; Lingg, C.; Kumpfmüller, D.; Ikenberg, B.; Ploner, M.; Hemmer, B.; et al. Case Series: Acute Hemorrhagic Encephalomyelitis After SARS-CoV-2 Vaccination. Front. Neurol. 2021, 12, 820049. [Google Scholar] [CrossRef]
- Poli, K.; Poli, S.; Ziemann, U. Multiple Autoimmune Syndromes Including Acute Disseminated Encephalomyelitis, Myasthenia Gravis, and Thyroiditis Following Messenger Ribonucleic Acid-Based COVID-19 Vaccination: A Case Report. Front. Neurol. 2022, 13, 913515. [Google Scholar] [CrossRef]
- Scorza, F.A.; Fiorini, A.C.; Scorza, C.A.; Finsterer, J. Cardiac abnormalities in Parkinson’s disease and Parkinsonism. J. Clin. Neurosci. 2018, 53, 1–5. [Google Scholar] [CrossRef]
- Piqueras-Flores, J.; López-García, A.; Moreno-Reig, Á.; González-Martínez, A.; Hernández-González, A.; Vaamonde-Gamo, J.; Jurado-Románet, A. Structural and functional alterations of the heart in Parkinson’s disease. Neurol. Res. 2018, 40, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Burstein, B.; Barbosa, R.S.; Samuel, M.; Kalfon, E.; Philippon, F.; Birnie, D.; Mangat, I.; Redfearn, D.; Sandhu, R.; Macle, L.; et al. Prevention of venous thrombosis after electrophysiology procedures: A survey of national practice. J. Interv. Card. Electrophysiol. 2018, 53, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.K.; Rhodes, C.; Rivers, E.; Thornton, C.P.; Rodney, T. Prevalence of Mental Health Disorders Among Undergraduate University Students in the United States: A Review. J. Psychosoc. Nurs. Ment. Health Serv. 2021, 59, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.G.; Sobieszczyk, P.S.; Bhatt, D.L. Acute Myocardial Infarction Within 24 Hours After COVID-19 Vaccination. Am. J. Cardiol. 2021, 156, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Li, S.; Ma, Y.; Li, Z.; Liu, G.; Liu, Y.; Jiao, J.; Zhu, C.; Song, B.; Jin, J.; et al. Risk factors associated with deep venous thrombosis in patients with different bed-rest durations: A multi-institutional case-control study. Int. J. Nurs. Stud. 2021, 114, 103825. [Google Scholar] [CrossRef]
- Walter, A.; Kraemer, M. A neurologist’s rhombencephalitis after comirnaty vaccination. A change of perspective. Neurol. Res. Pract. 2021, 3, 56. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Antigen | Manufacturer | Clone | Dilution | Incubation Time |
|---|---|---|---|---|
| CD3 (expressed by T-Lymphocytes) | cytomed | ZM-45 | 1:200 | 30 min |
| CD68 (expressed by monocytic cells) | DAKO | PG-M1 | 1:100 | 30 min |
| SARS-CoV-2-Spike subunit 1 | ProSci | 9083 | 1:500 | 30 min |
| SARS-CoV-2-Nucleocapsid | ProSci | 35–720 | 1:500 | 30 min |
| Item | Measure |
|---|---|
| Body weight | 60 kg |
| Hight | 175 cm |
| Heart weight | 410 g |
| Brain weight | 1560 g |
| Liver weight | 1500 g |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mörz, M. A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines 2022, 10, 1651. https://doi.org/10.3390/vaccines10101651
Mörz M. A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines. 2022; 10(10):1651. https://doi.org/10.3390/vaccines10101651
Chicago/Turabian StyleMörz, Michael. 2022. "A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19" Vaccines 10, no. 10: 1651. https://doi.org/10.3390/vaccines10101651
APA StyleMörz, M. (2022). A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines, 10(10), 1651. https://doi.org/10.3390/vaccines10101651