
The Burden of COVID-19 in Children and Its Prevention by Vaccination: A Joint Statement of the Israeli Pediatric Association and the Israeli Society for Pediatric Infectious Diseases

 , , , ,
, , , ,
Abstract
:1. The Burden of COVID-19
1.1. The Epidemiology of SARS-CoV-2 Infection in Children and Adolescents
1.2. COVID-19 Morbidity and Mortality among Children and Adolescents, Including Risk Factors for Severe COVID-19
2. Long-Term Complications of COVID-19 Infection
2.1. Myocarditis as a Complication of COVID-19
2.2. Multisystem Inflammatory Syndrome in Children (MIS-C)
2.3. Long COVID in Children and Adolescents
2.4. Possible Long-Term Sequelae of COVID-19
3. Infectivity and Transmission among Children and Adolescents
3.1. Infectivity of Children and Adolescents
3.2. The Role of Children in Household Transmission of COVID-19
3.3. The Role of Children in the Transmission of COVID-19 in Educational Institutions
4. Indirect Effects of COVID-19 on Children
The Importance of School Routine
5. Vaccine Efficacy
5.1. The Efficacy of the Messenger Ribonucleic Acid (mRNA) COVID-19 Vaccine
5.2. The Efficacy of the mRNA COVID-19 Vaccine among Children Aged 5–11 Years
5.3. The Efficacy of the mRNA COVID-19 Vaccine among Children Aged ≥12 Years
5.4. The Effectiveness of the mRNA COVID-19 Vaccine in Preventing Transmission of Infection
5.5. The Importance of Vaccination against Emerging SARS-CoV-2 Variants
5.6. The Expected Benefit of Immunization in Reducing the Burden of COVID-19 Complications (Long COVID and MIS-C) in Children and Adolescents
5.7. COVID-19 Immunization and Prevention of MIS-C
5.8. COVID-19 Vaccination of Recovered Children
6. Vaccine Safety
6.1. Safety of the mRNA COVID-19 Vaccine according to Research and Real-World Data
6.2. Safety of the mRNA COVID-19 Vaccine among Children Aged 5–11 Years
6.3. Myocarditis following COVID-19 Vaccination
6.4. COVID-19 Vaccines Show No Signs of Harming Female or Male Fertility
6.5. Lack of Correlation between Increased Menstrual Bleeding and Female Infertility
7. Summary and Recommendations
8. Recommendations
- Vaccination against COVID-19 is recommended for children aged 5 years or older while providing full information to the parents, children and vaccinated adolescents regarding the effectiveness of the vaccine, the importance of disease prevention and the safety of the vaccine.
- Development of anaphylaxis or myocarditis following mRNA COVID-19 vaccination should serve as a contraindication for additional doses of the vaccine.
- A comprehensive vaccine safety follow-up program will be conducted by the Ministry of Health in Israel.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Israeli Ministry of Health Corona Dashboard. Available online: https://datadashboard.health.gov.il/COVID-19/ (accessed on 29 March 2021).
- Campbell, F.; Archer, B.; Laurenson-Schafer, H.; Jinnai, Y.; Konings, F.; Batra, N.; Pavlin, B.; Vandemaele, K.; Van Kerkhove, M.D.; Jombart, T.; et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Euro Surveill. 2021, 26, 2100509. [Google Scholar] [CrossRef]
- Public Health Services The COVID-19 Vaccine in the 5–11 Age Group. Available online: https://www.gov.il/BlobFolder/news/03112021-04/he/NEWS_Corona_public-health-services-5-11-vaccine.pdf (accessed on 29 November 2021).
- Home—COVID 19 Scenario Model Hub. Available online: https://covid19scenariomodelinghub.org/viz.html (accessed on 24 June 2021).
- Liguoro, I.; Pilotto, C.; Bonanni, M.; Ferrari, M.E.; Pusiol, A.; Nocerino, A.; Vidal, E.; Cogo, P. SARS-COV-2 infection in children and newborns: A systematic review. Eur. J. Pediatr. 2020, 179, 1029–1046. [Google Scholar] [CrossRef]
- Ben-Shimol, S.; Livni, G.; Megged, O.; Greenberg, D.; Danino, D.; Youngster, I.; Shachor-Meyouhas, Y.; Dabaja-Younis, H.; Scheuerman, O.; Mor, M.; et al. COVID-19 in a Subset of Hospitalized Children in Israel. J. Pediatr. Infect. Dis. Soc. 2021, 10, 757–765. [Google Scholar] [CrossRef]
- Havers, F.P.; Whitaker, M.; Self, J.L.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; Kawasaki, B.; Meek, J.; Yousey-Hindes, K.; Anderson, E.J.; et al. Hospitalization of Adolescents Aged 12-17 Years with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 1, 2020–April 24, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 851–857. [Google Scholar] [CrossRef]
- Daniels, C.J.; Rajpal, S.; Greenshields, J.T.; Rosenthal, G.L.; Chung, E.H.; Terrin, M.; Jeudy, J.; Mattson, S.E.; Law, I.H.; Borchers, J.; et al. Prevalence of Clinical and Subclinical Myocarditis in Competitive Athletes With Recent SARS-CoV-2 Infection: Results From the Big Ten COVID-19 Cardiac Registry. JAMA Cardiol. 2021, 6, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Oliver, S. EtR Framework: Pfizer-BioNTech COVID-19 vaccine in children aged 5–11 years 2021. In Proceedings of the CDC ACIP Meeting, Atlanta, GA, USA, 2 November 2021. [Google Scholar]
- Feldstein, L.R.; Tenforde, M.W.; Friedman, K.G.; Newhams, M.; Rose, E.B.; Dapul, H.; Soma, V.L.; Maddux, A.B.; Mourani, P.M.; Bowens, C.; et al. Characteristics and Outcomes of US Children and Adolescents with Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA 2021, 325, 1074–1087. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, M.S.; Bertolino, L.; Zampino, R.; Durante-Mangoni, E. Monaldi Hospital Cardiovascular Infection Study Group Cardiac sequelae after coronavirus disease 2019 recovery: A systematic review. Clin. Microbiol. Infect. 2021, 27, 1250–1261. [Google Scholar] [CrossRef]
- Giacalone, M.; Scheier, E.; Shavit, I. Multisystem inflammatory syndrome in children (MIS-C): A mini-review. Int J Emerg Med 2021, 14, 50. [Google Scholar] [CrossRef] [PubMed]
- Hoste, L.; Van Paemel, R.; Haerynck, F. Multisystem inflammatory syndrome in children related to COVID-19: A systematic review. Eur. J. Pediatr. 2021, 180, 2019–2034. [Google Scholar] [CrossRef] [PubMed]
- Sananez, I.; Raiden, S.C.; Algieri, S.C.; Uranga, M.; Grisolía, N.A.; Filippo, D.; De Carli, N.; Lalla, S.D.; Cairoli, H.; Chiolo, M.J.; et al. A poor and delayed anti-SARS-CoV2 IgG response is associated to severe COVID-19 in children. EBioMedicine 2021, 72, 103615. [Google Scholar] [CrossRef] [PubMed]
- Davies, P.; Evans, C.; Kanthimathinathan, H.K.; Lillie, J.; Brierley, J.; Waters, G.; Johnson, M.; Griffiths, B.; du Pré, P.; Mohammad, Z.; et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: A multicentre observational study. Lancet Child Adolesc. Health 2020, 4, 669–677. [Google Scholar] [CrossRef]
- CDC COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/#mis-national-surveillance (accessed on 24 October 2021).
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Dufort, E.M.; Koumans, E.H.; Chow, E.J.; Rosenthal, E.M.; Muse, A.; Rowlands, J.; Barranco, M.A.; Maxted, A.M.; Rosenberg, E.S.; Easton, D.; et al. Multisystem inflammatory syndrome in children in new york state. N. Engl. J. Med. 2020, 383, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Roessler, M.; Tesch, F.; Batram, M.; Jacob, J.; Loser, F.; Weidinger, O.; Wende, D.; Vivirito, A.; Toepfner, N.; Seifert, M.; et al. Post COVID-19 in children, adolescents, and adults: Results of a matched cohort study including more than 150,000 individuals with COVID-19. medRxiv 2021. [Google Scholar] [CrossRef]
- What Has Been the Impact of COVID-19 across the UK Countries? The Nuffield Trust. Available online: https://www.nuffieldtrust.org.uk/news-item/what-has-been-the-impact-of-covid-19-across-the-uk-countries?gclid=CjwKCAjw2vOLBhBPEiwAjEeK9kgnV4oYYe8fHM1eOVUEF4SyWRdb7vElgYcO3bAiwjHBId2KAxahwhoCoVEQAvD_BwE (accessed on 31 October 2021).
- Stephenson, T.; Stephenson, T.; Pereira, S.P.; Shafran, R.; De Stavola, B.; Rojas, N.; McOwat, K.; Simmons, R.; Zavala, M.; O’Mahoney, L.; et al. Long COVID—The physical and mental health of children and non-hospitalised young people 3 months after SARS-CoV-2 infection; a national matched cohort study (The CLoCk) Study. Res. Sq. 2021, 11, e052838. [Google Scholar] [CrossRef]
- Radtke, T.; Ulyte, A.; Puhan, M.A.; Kriemler, S. Long-term Symptoms After SARS-CoV-2 Infection in Children and Adolescents. JAMA 2021, 326, 869–871. [Google Scholar] [CrossRef]
- Blankenburg, J.; Wekenborg, M.K.; Reichert, J.; Kirsten, C.; Kahre, E.; Haag, L.; Schumm, L.; Czyborra, P.; Berner, R.; Armann, J.P. Mental Health of Adolescents in the Pandemic: Long-COVID-19 or Long-Pandemic Syndrome? SSRN J. 2021. [Google Scholar] [CrossRef]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes, R.C.; Antonelli, M.; Murray, B.; Kläser, K.; Kerfoot, E.; Chen, L.; et al. Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2. Lancet Child Adolesc. Health 2021, 5, 708–718. [Google Scholar] [CrossRef]
- Osmanov, I.M.; Spiridonova, E.; Bobkova, P.; Gamirova, A.; Shikhaleva, A.; Andreeva, M.; Blyuss, O.; El-Taravi, Y.; DunnGalvin, A.; Comberiati, P.; et al. Risk factors for long covid in previously hospitalised children using the ISARIC Global follow-up protocol: A prospective cohort study. Eur. Respir. J. 2021. [Google Scholar] [CrossRef]
- Buonsenso, D.; Munblit, D.; De Rose, C.; Sinatti, D.; Ricchiuto, A.; Carfi, A.; Valentini, P. Preliminary Evidence on Long COVID in children. medRxiv 2021. [Google Scholar] [CrossRef]
- Miller, F.; Nguyen, V.; Navaratnam, A.M.; Shrotri, M.; Kovar, J.; Hayward, A.C.; Fragaszy, E.; Aldridge, R.W.; Hardelid, P. Prevalence of persistent symptoms in children during the COVID-19 pandemic: Evidence from a household cohort study in England and Wales. medRxiv 2021. [Google Scholar] [CrossRef]
- Ashkenazi-Hoffnung, L.; Shmueli, E.; Ehrlich, S.; Ziv, A.; Bar-On, O.; Birk, E.; Lowenthal, A.; Prais, D. Long COVID in children: Observations from A designated pediatric clinic. Pediatr. Infect. Dis. J. 2021, 40, e509. [Google Scholar] [CrossRef] [PubMed]
- Prevalence of Ongoing Symptoms Following Coronavirus (COVID-19) Infection in the UK—Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/7october2021 (accessed on 31 October 2021).
- Results of the Long-COVID Survey Among Children in Israel|Ministry of Health. Available online: https://www.gov.il/en/departments/news/13092021-01 (accessed on 3 November 2021).
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12, 698169. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; Jbabdi, S.; et al. Brain imaging before and after COVID-19 in UK Biobank. medRxiv 2021. [Google Scholar] [CrossRef]
- Wenzel, J.; Lampe, J.; Müller-Fielitz, H.; Schuster, R.; Zille, M.; Müller, K.; Krohn, M.; Körbelin, J.; Zhang, L.; Özorhan, Ü.; et al. The SARS-CoV-2 main protease Mpro causes microvascular brain pathology by cleaving NEMO in brain endothelial cells. Nat. Neurosci. 2021, 24, 1522–1533. [Google Scholar] [CrossRef] [PubMed]
- Jeong, M.; Ocwieja, K.E.; Han, D.; Wackym, P.A.; Zhang, Y.; Brown, A.; Moncada, C.; Vambutas, A.; Kanne, T.; Crain, R.; et al. Direct SARS-CoV-2 infection of the human inner ear may underlie COVID-19-associated audiovestibular dysfunction. Commun Med. 2021, 1, 44. [Google Scholar] [CrossRef] [PubMed]
- Baggio, S.; L’Huillier, A.G.; Yerly, S.; Bellon, M.; Wagner, N.; Rohr, M.; Huttner, A.; Blanchard-Rohner, G.; Loevy, N.; Kaiser, L.; et al. SARS-CoV-2 viral load in the upper respiratory tract of children and adults with early acute COVID-19. Clin. Infect. Dis. 2020, 73, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Hurst, J.H.; Heston, S.M.; Chambers, H.N.; Cunningham, H.M.; Price, M.J.; Suarez, L.; Crew, C.G.; Bose, S.; Aquino, J.N.; Carr, S.T.; et al. SARS-CoV-2 Infections Among Children in the Biospecimens from Respiratory Virus-Exposed Kids (BRAVE Kids) Study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Yonker, L.M.; Neilan, A.M.; Bartsch, Y.; Patel, A.B.; Regan, J.; Arya, P.; Gootkind, E.; Park, G.; Hardcastle, M.; St John, A.; et al. Pediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses. J. Pediatr. 2020, 227, 45–52.e5. [Google Scholar] [CrossRef]
- Heald-Sargent, T.; Muller, W.J.; Zheng, X.; Rippe, J.; Patel, A.B.; Kociolek, L.K. Age-Related Differences in Nasopharyngeal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Levels in Patients With Mild to Moderate Coronavirus Disease 2019 (COVID-19). JAMA Pediatr. 2020, 174, 902–903. [Google Scholar] [CrossRef]
- Li, X.; Xu, W.; Dozier, M.; He, Y.; Kirolos, A.; Lang, Z.; Song, P.; Theodoratou, E. UNCOVER The role of children in the transmission of SARS-CoV2: Updated rapid review. J. Glob. Health 2020, 10, 021101. [Google Scholar] [CrossRef] [PubMed]
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A Review of Viral, Host, and Environmental Factors. Ann. Intern. Med. 2020, 174, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Mallapaty, S. How do children spread the coronavirus? The science still isn’t clear. Nature 2020, 581, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Raszka, W.V. COVID-19 Transmission and Children: The Child Is Not to Blame. Pediatrics 2020, 146. [Google Scholar] [CrossRef]
- Director of public health services Ministry of Health COVID-19 in children in Israel. In COVID-19 in Children in Israel; Israeli Ministry of Health: Jerusalem, Israel, 2020; pp. 1–24.
- Szablewski, C.M.; Chang, K.T.; McDaniel, C.J.; Chu, V.T.; Yousaf, A.R.; Schwartz, N.G.; Brown, M.; Winglee, K.; Paul, P.; Cui, Z.; et al. SARS-CoV-2 Transmission Dynamics in a Sleep-Away Camp. Pediatrics 2021, 147, e2020046524. [Google Scholar] [CrossRef]
- Pray, I.W.; Gibbons-Burgener, S.N.; Rosenberg, A.Z.; Cole, D.; Borenstein, S.; Bateman, A.; Pevzner, E.; Westergaard, R.P. COVID-19 Outbreak at an Overnight Summer School Retreat—Wisconsin, July-August 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1600–1604. [Google Scholar] [CrossRef]
- Stein-Zamir, C.; Abramson, N.; Shoob, H.; Libal, E.; Bitan, M.; Cardash, T.; Cayam, R.; Miskin, I. A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Euro Surveill. 2020, 25, 2001352. [Google Scholar] [CrossRef]
- Goldstein, E.; Lipsitch, M.; Cevik, M. On the Effect of Age on the Transmission of SARS-CoV-2 in Households, Schools, and the Community. J. Infect. Dis. 2021, 223, 362–369. [Google Scholar] [CrossRef]
- Szablewski, C.M.; Chang, K.T.; Brown, M.M.; Chu, V.T.; Yousaf, A.R.; Anyalechi, N.; Aryee, P.A.; Kirking, H.L.; Lumsden, M.; Mayweather, E.; et al. SARS-CoV-2 Transmission and Infection Among Attendees of an Overnight Camp—Georgia, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1023–1025. [Google Scholar] [CrossRef]
- Park, Y.J.; Choe, Y.J.; Park, O.; Park, S.Y.; Kim, Y.-M.; Kim, J.; Kweon, S.; Woo, Y.; Gwack, J.; Kim, S.S.; et al. Contact Tracing during Coronavirus Disease Outbreak, South Korea, 2020. Emerg. Infect. Dis. 2020, 26, 2465–2468. [Google Scholar] [CrossRef]
- Posfay-Barbe, K.M.; Wagner, N.; Gauthey, M.; Moussaoui, D.; Loevy, N.; Diana, A.; L’Huillier, A.G. COVID-19 in Children and the Dynamics of Infection in Families. Pediatrics 2020, 146. [Google Scholar] [CrossRef]
- Kim, J.; Choe, Y.J.; Lee, J.; Park, Y.J.; Park, O.; Han, M.S.; Kim, J.-H.; Choi, E.H. Role of children in household transmission of COVID-19. Arch. Dis. Child. 2021, 106, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Bloxham, C.J.; Hulme, K.D.; Sinclair, J.E.; Tong, Z.W.M.; Steele, L.E.; Noye, E.C.; Lu, J.; Xia, Y.; Chew, K.Y.; et al. A Meta-analysis on the Role of Children in Severe Acute Respiratory Syndrome Coronavirus 2 in Household Transmission Clusters. Clin. Infect. Dis. 2021, 72, e1146–e1153. [Google Scholar] [CrossRef]
- Soriano-Arandes, A.; Gatell, A.; Serrano, P.; Biosca, M.; Campillo, F.; Capdevila, R.; Fàbrega, A.; Lobato, Z.; López, N.; Moreno, A.M.; et al. Household severe acute respiratory syndrome coronavirus 2 transmission and children: A network prospective study. Clin. Infect. Dis. 2021, 73, e1261–e1269. [Google Scholar] [CrossRef]
- Pitman-Hunt, C.; Leja, J.; Jiwani, Z.M.; Rondot, D.; Ang, J.; Kannikeswaran, N. SARS-CoV-2 Transmission in an Urban Community: The Role of Children and Household Contacts. J. Pediatr. Infect. Dis. Soc. 2020, 10, 919–992. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.A.; Daneman, N.; Schwartz, K.L.; Science, M.; Brown, K.A.; Whelan, M.; Chan, E.; Buchan, S.A. Association of Age and Pediatric Household Transmission of SARS-CoV-2 Infection. JAMA Pediatr. 2021, 175, 1151–1158. [Google Scholar] [CrossRef]
- Chu, V.T.; Yousaf, A.R.; Chang, K.; Schwartz, N.G.; McDaniel, C.J.; Lee, S.H.; Szablewski, C.M.; Brown, M.; Drenzek, C.L.; Dirlikov, E.; et al. Household Transmission of SARS-CoV-2 from Children and Adolescents. N. Engl. J. Med. 2021, 385, 954–956. [Google Scholar] [CrossRef]
- Grijalva, C.G.; Rolfes, M.A.; Zhu, Y.; McLean, H.Q.; Hanson, K.E.; Belongia, E.A.; Halasa, N.B.; Kim, A.; Reed, C.; Fry, A.M.; et al. Transmission of SARS-COV-2 Infections in Households—Tennessee and Wisconsin, April-September 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1631–1634. [Google Scholar] [CrossRef] [PubMed]
- Coffin, S.E.; Rubin, D. Yes, children can transmit COVID, but we need not fear. JAMA Pediatr. 2021, 175, 1110. [Google Scholar] [CrossRef]
- Lee, B.; Raszka, W.V. COVID-19 in Children: Looking Forward, Not Back. Pediatrics 2021, 147. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, C.V.; Martin, L.M.; Kim, S.S.; Kirmse, B.M.; Haynie, L.; McGraw, S.; Byers, P.; Taylor, K.G.; Patel, M.M.; Flannery, B.; et al. Factors Associated with Positive SARS-CoV-2 Test Results in Outpatient Health Facilities and Emergency Departments Among Children and Adolescents Aged <18 Years—Mississippi, September-November 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1925–1929. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.S.; Hill, M.; Antezano, J.; Vilven, D.; Rutner, T.; Bogdanow, L.; Claflin, C.; Kracalik, I.T.; Fields, V.L.; Dunn, A.; et al. Transmission Dynamics of COVID-19 Outbreaks Associated with Child Care Facilities—Salt Lake City, Utah, April-July 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Danis, K.; Epaulard, O.; Bénet, T.; Gaymard, A.; Campoy, S.; Botelho-Nevers, E.; Bouscambert-Duchamp, M.; Spaccaferri, G.; Ader, F.; Mailles, A.; et al. Cluster of Coronavirus Disease 2019 (COVID-19) in the French Alps, February 2020. Clin. Infect. Dis. 2020, 71, 825–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heavey, L.; Casey, G.; Kelly, C.; Kelly, D.; McDarby, G. No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020. Euro Surveill. 2020, 25, 2000903. [Google Scholar] [CrossRef]
- Ehrhardt, J.; Ekinci, A.; Krehl, H.; Meincke, M.; Finci, I.; Klein, J.; Geisel, B.; Wagner-Wiening, C.; Eichner, M.; Brockmann, S.O. Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools after their reopening in May 2020, Baden-Württemberg, Germany. Euro Surveill. 2020, 25, 2001587. [Google Scholar] [CrossRef]
- Link-Gelles, R.; DellaGrotta, A.L.; Molina, C.; Clyne, A.; Campagna, K.; Lanzieri, T.M.; Hast, M.A.; Palipudi, K.; Dirlikov, E.; Bandy, U. Limited Secondary Transmission of SARS-CoV-2 in Child Care Programs—Rhode Island, June 1-July 31, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1170–1172. [Google Scholar] [CrossRef]
- Yung, C.F.; Kam, K.-Q.; Nadua, K.D.; Chong, C.Y.; Tan, N.W.H.; Li, J.; Lee, K.P.; Chan, Y.H.; Thoon, K.C.; Ng, K.C. Novel coronavirus 2019 transmission risk in educational settings. Clin. Infect. Dis. 2021, 72, 1055–1058. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.; Choi, G.-J.; Kim, J.Y.; Kim, K.-R.; Park, H.; Chun, J.K.; Kim, Y.-J. Childcare Exposure to Severe Acute Respiratory Syndrome Coronavirus 2 for 4-Year-Old Presymptomatic Child, South Korea. Emerg. Infect. Dis. 2021, 27, 341–347. [Google Scholar] [CrossRef]
- Kim, C.; McGee, S.; Khuntia, S.; Elnour, A.; Johnson-Clarke, F.; Mangla, A.; Iyengar, P.; Nesbitt, L. Characteristics of COVID-19 Cases and Outbreaks at Child Care Facilities—District of Columbia, July-December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 744–748. [Google Scholar] [CrossRef]
- van Loon, W.; Hommes, F.; Theuring, S.; von der Haar, A.; Körner, J.; Schmidt, M.; von Kalle, C.; Mall, M.A.; Seybold, J.; Kurth, T.; et al. Renewed Absence of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infections in the Day Care Context in Berlin, January 2021. Clin. Infect. Dis. 2021, 73, 1944–1945. [Google Scholar] [CrossRef]
- Lachassinne, E.; de Pontual, L.; Caseris, M.; Lorrot, M.; Guilluy, C.; Naud, A.; Dommergues, M.-A.; Pinquier, D.; Wannepain, E.; Hausherr, E.; et al. SARS-CoV-2 transmission among children and staff in daycare centres during a nationwide lockdown in France: A cross-sectional, multicentre, seroprevalence study. Lancet Child Adolesc. Health 2021, 5, 256–264. [Google Scholar] [CrossRef]
- Bourion-Bédès, S.; Tarquinio, C.; Batt, M.; Tarquinio, P.; Lebreuilly, R.; Sorsana, C.; Legrand, K.; Rousseau, H.; Baumann, C. Psychological impact of the COVID-19 outbreak on students in a French region severely affected by the disease: Results of the PIMS-CoV 19 study. Psychiatry Res. 2021, 295, 113559. [Google Scholar] [CrossRef]
- de Figueiredo, C.S.; Sandre, P.C.; Portugal, L.C.L.; Mázala-de-Oliveira, T.; da Silva Chagas, L.; Raony, Í.; Ferreira, E.S.; Giestal-de-Araujo, E.; Dos Santos, A.A.; Bomfim, P.O.-S. COVID-19 pandemic impact on children and adolescents’ mental health: Biological, environmental, and social factors. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 106, 110171. [Google Scholar] [CrossRef]
- Taub Center Opportunities and Risks to the Education System in the Time of the Coronavirus an Overview. Available online: http://taubcenter.org.il/he/opportunities-and-risks-to-the-education-system-in-the-time-of-the-coronavirus-an-overview/ (accessed on 11 April 2021).
- Central Bureau of Statistics Civil Resilience During the Coronavirus Crisis Among Persons Aged 21 and Over. Available online: https://www.cbs.gov.il/he/mediarelease/Pages/2020/%D7%AA%D7%9E%D7%95%D7%A0%D7%AA-%D7%9E%D7%A6%D7%91-%D7%A9%D7%9C-%D7%94%D7%97%D7%95%D7%A1%D7%9F-%D7%94%D7%90%D7%96%D7%A8%D7%97%D7%99-%D7%91%D7%AA%D7%A7%D7%95%D7%A4%D7%AA-%D7%9E%D7%A9%D7%91%D7%A8-%D7%94%D7%A7%D7%95%D7%A8%D7%95%D7%A0%D7%94.aspx (accessed on 11 April 2021).
- Bank of Israel Bank of Israel Periodical Report. Available online: https://www.boi.org.il/he/NewsAndPublications/RegularPublications/Pages/DochBankIsrael2020.aspx (accessed on 11 April 2021).
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Tessier, E.; Groves, N.; Dabrera, G.; Myers, R.; et al. Effectiveness of COVID-19 vaccines against the B.1.617.2 variant. medRxiv 2021. [Google Scholar] [CrossRef]
- FDA. EUA Amendment Request for Pfizer-BioNTech COVID-19 Vaccine for Use in Children 5 through 11 Years of Age; FDA: Silver Spring, MD, USA, 2021.
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Nationwide Vaccination Campaign with BNT162b2 in Israel Demonstrates High Vaccine Effectiveness and Marked Declines in Incidence of SARS-CoV-2 Infections and COVID-19 Cases, Hospitalizations, and Deaths. 2021. Available online: https://ssrn.com/abstract=3811387 (accessed on 29 December 2021).
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Frenck, R.W.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.M.; Newhams, M.M.; Halasa, N.B.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Irby, K.; Walker, T.C.; Schwartz, S.P.; Pannaraj, P.S.; et al. Effectiveness of Pfizer-BioNTech mRNA Vaccination Against COVID-19 Hospitalization Among Persons Aged 12-18 Years—United States, June-September 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1483–1488. [Google Scholar] [CrossRef]
- Tang, L.; Hijano, D.R.; Gaur, A.H.; Geiger, T.L.; Neufeld, E.J.; Hoffman, J.M.; Hayden, R.T. Asymptomatic and Symptomatic SARS-CoV-2 Infections After BNT162b2 Vaccination in a Routinely Screened Workforce. JAMA 2021, 325, 2500–2502. [Google Scholar] [CrossRef] [PubMed]
- Lumley, S.F.; Rodger, G.; Constantinides, B.; Sanderson, N.; Chau, K.K.; Street, T.L.; O’Donnell, D.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; et al. An observational cohort study on the incidence of SARS-CoV-2 infection and B.1.1.7 variant infection in healthcare workers by antibody and vaccination status. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Andrejko, K.L.; Pry, J.; Myers, J.F.; Jewell, N.P.; Openshaw, J.; Watt, J.; Jain, S.; Lewnard, J.A. California COVID-19 Case-Control Study Team Prevention of COVID-19 by mRNA-based vaccines within the general population of California. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Pouwels, K.B.; Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Vihta, K.-D.; House, T.; Hay, J.; Bell, J.I.; Newton, J.N.; et al. Effect of Delta variant on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. Nat. Med. 2021, 2127–2135. [Google Scholar] [CrossRef]
- Elliott, P.; Haw, D.; Wang, H.; Eales, O.; Walters, C.E.; Ainslie, K.E.C.; Atchison, C.; Fronterre, C.; Diggle, P.J.; Page, A.J.; et al. REACT-1 round 13 final report: Exponential growth, high prevalence of SARS-CoV-2 and vaccine effectiveness associated with Delta variant in England during May to July 2021. medRxiv 2021. [Google Scholar] [CrossRef]
- Reis, B.Y.; Barda, N.; Leshchinsky, M.; Kepten, E.; Hernán, M.A.; Lipsitch, M.; Dagan, N.; Balicer, R.D. Effectiveness of BNT162b2 Vaccine against Delta Variant in Adolescents. N. Engl. J. Med. 2021, 385, 2101–2103. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.; Walker, A.S.; Peto, T.E. The impact of SARS-CoV-2 vaccination on Alpha and Delta variant transmission. medRxiv 2021. [Google Scholar] [CrossRef]
- Chia, P.Y.; Ong, S.; Chiew, C.J.; Ang, L.W.; Chavatte, J.G.; Mak, T.M.; Cui, L.; Kalimuddin, S.; Chia, W.N.; Tan, C.W.; et al. Virological and serological kinetics of SARS-CoV-2 Delta variant vaccine-breakthrough infections: A multi-center cohort study. medRxiv 2021. [Google Scholar] [CrossRef]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Allen, H.; Vusirikala, A.; Flannagan, J.; Twohig, K.A.; Zaidi, A.; Chudasama, D.; Lamagni, T.; Groves, N.; Turner, C.; Rawlinson, C.; et al. Household transmission of COVID-19 cases associated with SARS-CoV-2 delta variant (B.1.617.2): National case-control study. Lancet Reg. Health Eur. 2022, 12, 100252. [Google Scholar] [CrossRef] [PubMed]
- de Gier, B.; Andeweg, S.; Backer, J.A.; RIVM COVID-19 surveillance and epidemiology team; Hahné, S.J.M.; van den Hof, S.; de Melker, H.E.; Knol, M.J. Vaccine effectiveness against SARS-CoV-2 transmission to household contacts during dominance of Delta variant (B.1.617.2), August-September 2021, the Netherlands. medRxiv 2021. [Google Scholar] [CrossRef]
- Strategy to Achieve Global Covid-19 Vaccination by mid-2022—World|ReliefWeb. Available online: https://reliefweb.int/report/world/strategy-achieve-global-covid-19-vaccination-mid-2022 (accessed on 18 December 2021).
- SARS-CoV-2 Variants of Concern as of 16 December 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 18 December 2021).
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 18 December 2021).
- Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 18 December 2021).
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—14 December 2021. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---14-december-2021 (accessed on 18 December 2021).
- Gardner, B.J.; Kilpatrick, A.M. Estimates of reduced vaccine effectiveness against hospitalization, infection, transmission and symptomatic disease of a new SARS-CoV-2 variant, Omicron (B.1.1.529), using neutralizing antibody titers. medRxiv 2021. [Google Scholar] [CrossRef]
- Pfizer and BioNTech Provide Update on Omicron Variant|Business Wire. Available online: https://www.businesswire.com/news/home/20211208005542/en/Pfizer-and-BioNTech-Provide-Update-on-Omicron-Variant (accessed on 18 December 2021).
- Wilhelm, A.; Widera, M.; Grikscheit, K.; Toptan, T.; Schenk, B.; Pallas, C.; Metzler, M.; Kohmer, N.; Hoehl, S.; Helfritz, F.A.; et al. Reduced Neutralization of SARS-CoV-2 Omicron Variant by Vaccine Sera and monoclonal antibodies. medRxiv 2021. [Google Scholar] [CrossRef]
- Tuite, A.R.; Zhu, L.; Fisman, D.N.; Salomon, J.A. Alternative Dose Allocation Strategies to Increase Benefits From Constrained COVID-19 Vaccine Supply. Ann. Intern. Med. 2021, 174, 570–572. [Google Scholar] [CrossRef] [PubMed]
- Overview of the Implementation of COVID-19 Vaccination Strategies and Deployment Plans in the EU/EEA. Available online: https://www.ecdc.europa.eu/en/publications-data/overview-implementation-covid-19-vaccination-strategies-and-deployment-plans (accessed on 18 December 2021).
- UK to Offer Booster Shots to All Adults, Just 3 Months after Their Second Dose—CNN. Available online: https://edition.cnn.com/2021/11/29/uk/uk-booster-vaccine-expansion-omicron-gbr-intl/index.html (accessed on 19 December 2021).
- France Brings forward Third COVID-19 Vaccine Shot|Reuters. Available online: https://www.reuters.com/world/europe/france-reduces-delay-get-third-covid-19-booster-shot-four-months-2021-12-17/ (accessed on 19 December 2021).
- S.Korea to Cut COVID-19 Booster Shot Interval Again as Infections Rise Reuters. Available online: https://www.reuters.com/world/asia-pacific/skorea-cut-covid-19-booster-shot-interval-again-infections-rise-2021-12-10/ (accessed on 19 December 2021).
- Denmark Cuts Interval Between Covid Second Dose and Booster Shot To 4.5 Months. Available online: https://www.ndtv.com/world-news/denmark-cuts-covid-19-booster-shot-interval-to-4-5-months-2648932 (accessed on 19 December 2021).
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. Effectiveness of COVID-19 vaccines against the Omicron (B.1.1.529) variant of concern. medRxiv 2021. [Google Scholar] [CrossRef]
- Wang, X.; Powell, C.A. How to translate the knowledge of COVID-19 into prevention of Omicron variants. Clin. Transl. Discov. 2021, 1. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Wallace, M. COVID19 mRNA vaccines in adolescents and young adults: Benefitrisk discussion 2021. In Proceedings of the ACIP Meeting, online, 23 June 2021. [Google Scholar]
- CDC Encourages Vaccination of Children to Prevent MIS-C, a Rare Illness Linked to Coronavirus|Health News|US News. Available online: https://www.usnews.com/news/health-news/articles/2021-06-17/cdc-encourages-vaccination-of-children-to-prevent-mis-c-a-rare-illness-linked-to-coronavirus (accessed on 1 November 2021).
- Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight Against Pandemic|FDA. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use (accessed on 3 June 2021).
- The MHRA Concludes Positive Safety Profile for Pfizer/BioNTech Vaccine in 12- to 15-Year-Olds—GOV.UK. Available online: https://www.gov.uk/government/news/the-mhra-concludes-positive-safety-profile-for-pfizerbiontech-vaccine-in-12-to-15-year-olds (accessed on 5 June 2021).
- First COVID-19 Vaccine Approved for Children Aged 12 to 15 in EU|European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/first-covid-19-vaccine-approved-children-aged-12-15-eu (accessed on 5 June 2021).
- GRADE: Pfizer-BioNTech COVID-19 Vaccine Age 12–15 Years|CDC. Available online: https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-pfizer-biontech-vaccine-12-15-years.html (accessed on 3 June 2021).
- Tom Shimabukuro Advisory Committee on Immunization Practices (ACIP) Safty Updates 23 June 2021. Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-10-20-21/06-COVID-Shimabukuro-508.pdf (accessed on 23 June 2021).
- Interim Statement on COVID-19 Vaccination for Children and Adolescents. Available online: https://www.who.int/news/item/24-11-2021-interim-statement-on-covid-19-vaccination-for-children-and-adolescents (accessed on 21 December 2021).
- National Advisory Committee on Immunization National Advisory Committee on Immunization (NACI) Statement: Recommendation on the Use of the Pfizer-BioNTech COVID-19 Vaccine (10 mcg) in Children 5 to 11 Years of Age. Available online: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/recommendations-use-covid-19-vaccines/pfizer-biontech-10-mcg-children-5-11-years-age.html (accessed on 21 December 2021).
- European Centre for Disease Prevention and Control. Interim Public Health Considerations for COVID-19 Vaccination of Children Aged 5-11 Years; ECDC: Stockholm, Swedish, 2021.
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N.; et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 2140–2149. [Google Scholar] [CrossRef]
- Israel Ministry of Health. Summary of Corona Myocarditis Events Following the COVID Vaccine, December 2020–May 2021; Israel Ministry of Health: Jerusalem, Israel, 2021; pp. 1–16.
- Vaccines and Related Biological Products Advisory Committee June 10, 2021 Meeting Presentation. Available online: https://www.fda.gov/media/149935/download (accessed on 10 June 2021).
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.E.; Taub, I.B.; Kaelber, D.C. Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis. medRxiv 2021. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Balicer, R.D. Adverse Effects after BNT162b2 Vaccine and SARS-CoV-2 Infection, According to Age and Sex. N. Engl. J. Med. 2021, 385, 2299. [Google Scholar] [CrossRef]
- Vasudeva, R.; Bhatt, P.; Lilje, C.; Desai, P.; Amponsah, J.; Umscheid, J.; Parmar, N.; Bhatt, N.; Adupa, R.; Pagad, S.; et al. Trends in Acute Myocarditis Related Pediatric Hospitalizations in the United States, 2007-2016. Am. J. Cardiol. 2021, 149, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D.; et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef]
- Lee, G.M.; Hopkins, R.H. COVID-19 Vaccine Safety Technical (VaST) Work Group 2021. Available online: https://www.cdc.gov/vaccines/acip/work-groups-vast/index.html (accessed on 30 August 2021).
- Patel, T.; Kelleman, M.; West, Z.; Peter, A.; Dove, M.; Butto, A.; Oster, M.E. Comparison of MIS-C Related Myocarditis, Classic Viral Myocarditis, and COVID-19 Vaccine related Myocarditis in Children. medRxiv 2021. [Google Scholar] [CrossRef]
- Yang, H. Benefits-Risks of Pfizer-BioNTech COVID-19 Vaccine for Ages 5 to 11 Years 2021; FDA VRBPAC: Silver Spring, MD, USA, 2021.
- Orvieto, R.; Noach-Hirsh, M.; Segev-Zahav, A.; Haas, J.; Nahum, R.; Aizer, A. Does mRNA SARS-CoV-2 vaccine influence patients’ performance during IVF-ET cycle? Reprod. Biol. Endocrinol. 2021, 19, 69. [Google Scholar] [CrossRef]
- Bentov, Y.; Beharier, O.; Moav-Zafrir, A.; Kabessa, M.; Godin, M.; Greenfield, C.S.; Ketzinel-Gilad, M.; Ash Broder, E.; Holzer, H.E.G.; Wolf, D.; et al. Ovarian follicular function is not altered by SARS-CoV-2 infection or BNT162b2 mRNA COVID-19 vaccination. Hum. Reprod. 2021, 36, 2506–2513. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, E.O.; Haapala, J.; DeSilva, M.; Vazquez-Benitez, G.; Vesco, K.K.; Naleway, A.L.; Lipkind, H.S. Spontaneous Abortion Following COVID-19 Vaccination During Pregnancy. JAMA 2021, 326, 1629–1631. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.S. SARS-CoV-2 spike protein seropositivity from vaccination or infection does not cause sterility. F&S Rep. 2021, 2, 253–255. [Google Scholar] [CrossRef]
- Zauche, L.H.; Wallace, B.; Smoots, A.N.; Olson, C.K.; Oduyebo, T.; Kim, S.Y.; Petersen, E.E.; Ju, J.; Beauregard, J.; Wilcox, A.J.; et al. Receipt of mRNA Covid-19 Vaccines and Risk of Spontaneous Abortion. N. Engl. J. Med. 2021, 385, 1533–1535. [Google Scholar] [CrossRef]
- Magnus, M.C.; Gjessing, H.K.; Eide, H.N.; Wilcox, A.J.; Fell, D.B.; Håberg, S.E. Covid-19 Vaccination during Pregnancy and First-Trimester Miscarriage. N. Engl. J. Med. 2021, 385, 2008–2010. [Google Scholar] [CrossRef]
- Safrai, M.; Rottenstreich, A.; Herzberg, S.; Imbar, T.; Reubinoff, B.; Ben-Meir, A. Stopping the misinformation: BNT162b2 COVID-19 vaccine has no negative effect on women’s fertility. medRxiv 2021. [Google Scholar] [CrossRef]
- Gonzalez, D.C.; Nassau, D.E.; Khodamoradi, K.; Ibrahim, E.; Blachman-Braun, R.; Ory, J.; Ramasamy, R. Sperm Parameters Before and After COVID-19 mRNA Vaccination. JAMA 2021, 326, 273–274. [Google Scholar] [CrossRef]
- Safrai, M.; Reubinoff, B.; Ben-Meir, A. BNT162b2 mRNA Covid-19 vaccine does not impair sperm parameters. medRxiv 2021. [Google Scholar] [CrossRef]
- Male, V. Menstrual changes after covid-19 vaccination. BMJ 2021, 374, n2211. [Google Scholar] [CrossRef] [PubMed]
- RCOG/FSRH Respond to Reports of 30,000 Women’s Periods Affected after COVID-19 Vaccine. Available online: https://www.rcog.org.uk/en/news/rcogfsrh-responds-to-reports-of-30000-womens-periods-affected-after-covid-19-vaccine/ (accessed on 2 November 2021).
- Comirnaty COVID-19 Vaccine: EMA Recommends Approval for Children Aged 5 to 11|European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/comirnaty-covid-19-vaccine-ema-recommends-approval-children-aged-5-11 (accessed on 21 December 2021).
- Coronavirus Vaccine—Weekly Summary of Yellow Card Reporting—GOV.UK. Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 15 November 2021).
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
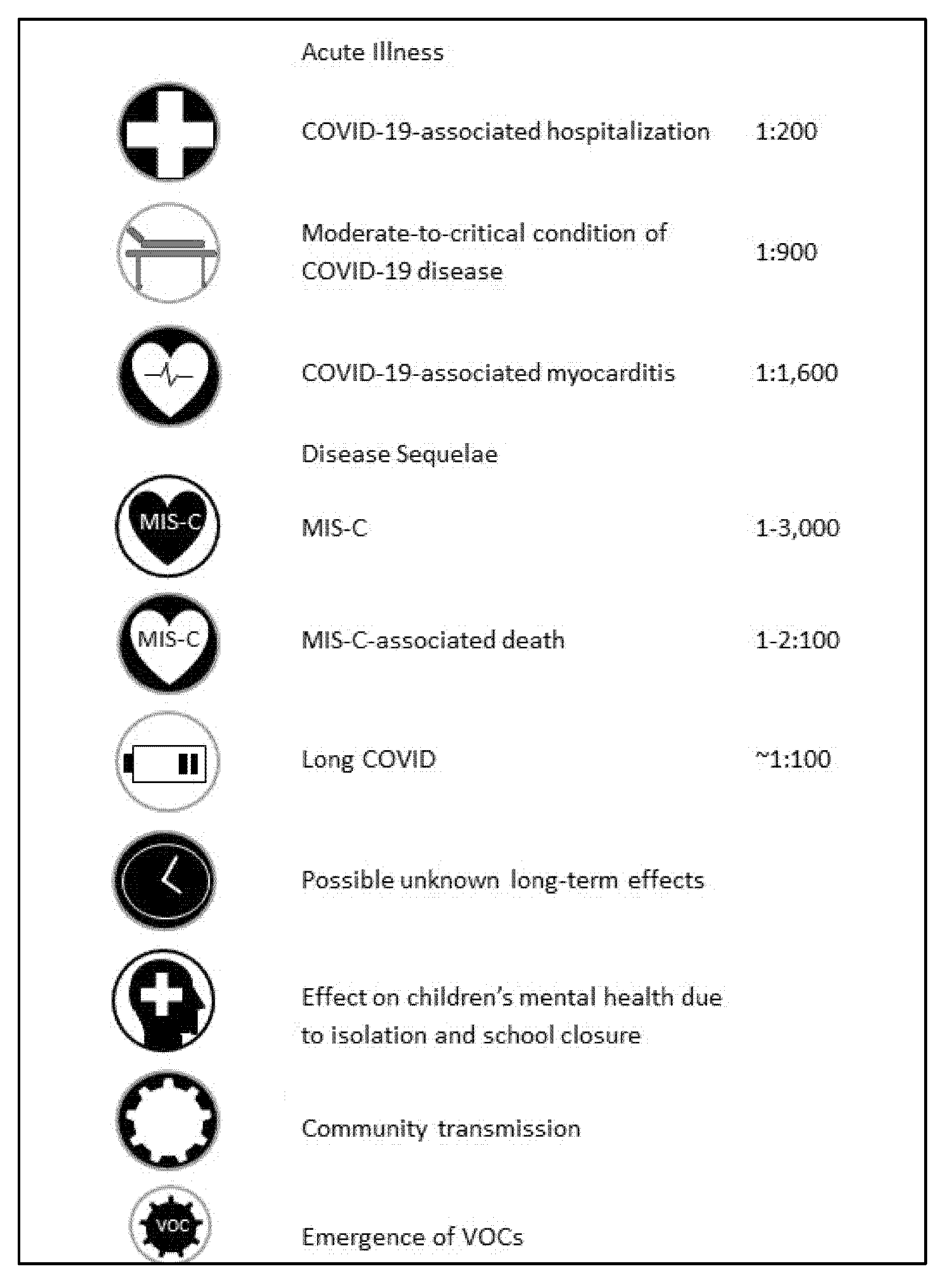
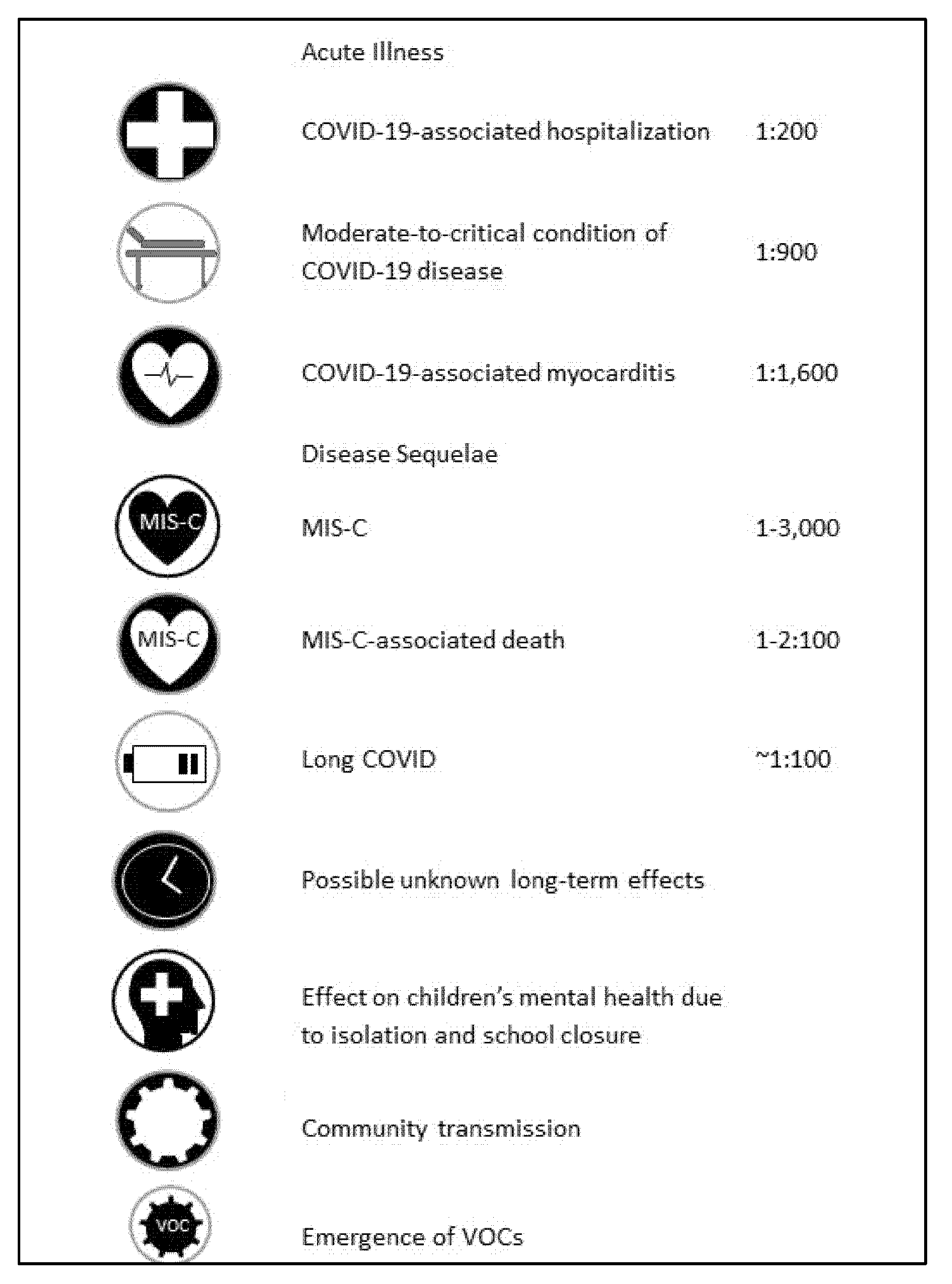
| Potential Benefits and Risks of Childhood Vaccination against COVID-19 | ||
|---|---|---|
| Potential Benefits | Potential Risks | |
| Prevention of COVID-19-associated hospitalization | Local transient vaccine-related side effects | 7:10 |
| Protection against a moderate-to-critical condition of COVID-19 disease | Vaccine-associated myocarditis | 1:6600 *, mild in 95% |
| Protection against COVID-19-associated myocarditis | Vaccine-associated severe myocarditis | 1:300,000 ** |
| Protection against MIS-C | Transient menstrual bleeding irregularity | |
| Prevention of MIS-C-associated death | ||
| Protection against long COVID | ||
| Prevention of possible unknown long-term effects | ||
| Avoidance of isolation and school closure | ||
| Reducing community transmission | ||
| Reducing emergence of VOCs | ||
| We recommend the use of the Pfizer-BioNTech COVID-19 vaccine for children aged 5 years and older while providing accessible and transparent information to the parents, adolescents and children regarding the effectiveness of the vaccine, the importance of COVID-19 prevention and the safety of the vaccine. |
| The second dose of the Pfizer-BioNTech COVID-19 vaccination series should be deferred in children who experience anaphylaxis or myocarditis following the first dose of the Pfizer-BioNTech COVID-19 vaccine. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stein, M.; Ashkenazi-Hoffnung, L.; Greenberg, D.; Dalal, I.; Livni, G.; Chapnick, G.; Stein-Zamir, C.; Ashkenazi, S.; Hecht-Sagie, L.; Grossman, Z. The Burden of COVID-19 in Children and Its Prevention by Vaccination: A Joint Statement of the Israeli Pediatric Association and the Israeli Society for Pediatric Infectious Diseases. Vaccines 2022, 10, 81. https://doi.org/10.3390/vaccines10010081
Stein M, Ashkenazi-Hoffnung L, Greenberg D, Dalal I, Livni G, Chapnick G, Stein-Zamir C, Ashkenazi S, Hecht-Sagie L, Grossman Z. The Burden of COVID-19 in Children and Its Prevention by Vaccination: A Joint Statement of the Israeli Pediatric Association and the Israeli Society for Pediatric Infectious Diseases. Vaccines. 2022; 10(1):81. https://doi.org/10.3390/vaccines10010081
Chicago/Turabian StyleStein, Michal, Liat Ashkenazi-Hoffnung, David Greenberg, Ilan Dalal, Gilat Livni, Gil Chapnick, Chen Stein-Zamir, Shai Ashkenazi, Lior Hecht-Sagie, and Zachi Grossman. 2022. "The Burden of COVID-19 in Children and Its Prevention by Vaccination: A Joint Statement of the Israeli Pediatric Association and the Israeli Society for Pediatric Infectious Diseases" Vaccines 10, no. 1: 81. https://doi.org/10.3390/vaccines10010081
APA StyleStein, M., Ashkenazi-Hoffnung, L., Greenberg, D., Dalal, I., Livni, G., Chapnick, G., Stein-Zamir, C., Ashkenazi, S., Hecht-Sagie, L., & Grossman, Z. (2022). The Burden of COVID-19 in Children and Its Prevention by Vaccination: A Joint Statement of the Israeli Pediatric Association and the Israeli Society for Pediatric Infectious Diseases. Vaccines, 10(1), 81. https://doi.org/10.3390/vaccines10010081