Anti-Inflammatory, Anti-Arthritic and Anti-Nociceptive Activities of Nigella sativa Oil in a Rat Model of Arthritis

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Nigella sativa Oil Preparation
2.3. Quantitative Analysis of Fatty Acids and Tocopherols in Nigella sativa Oil
2.4. Animals
2.5. Acute Toxicity Study
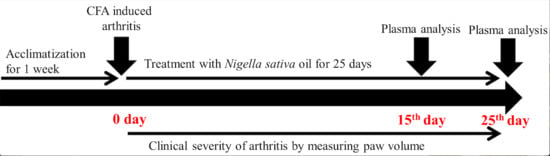
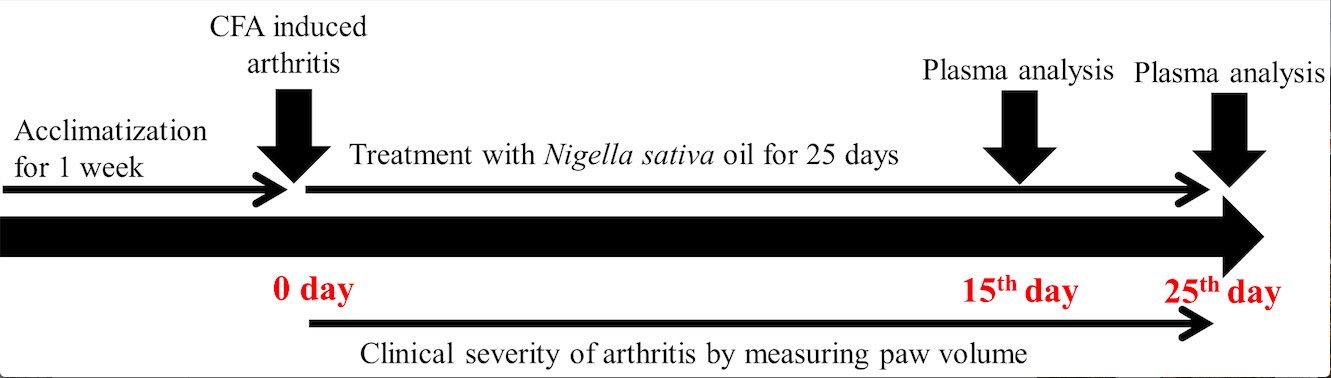
2.6. CFA-Induced Arthritis Model
2.7. Body Weight Assessment
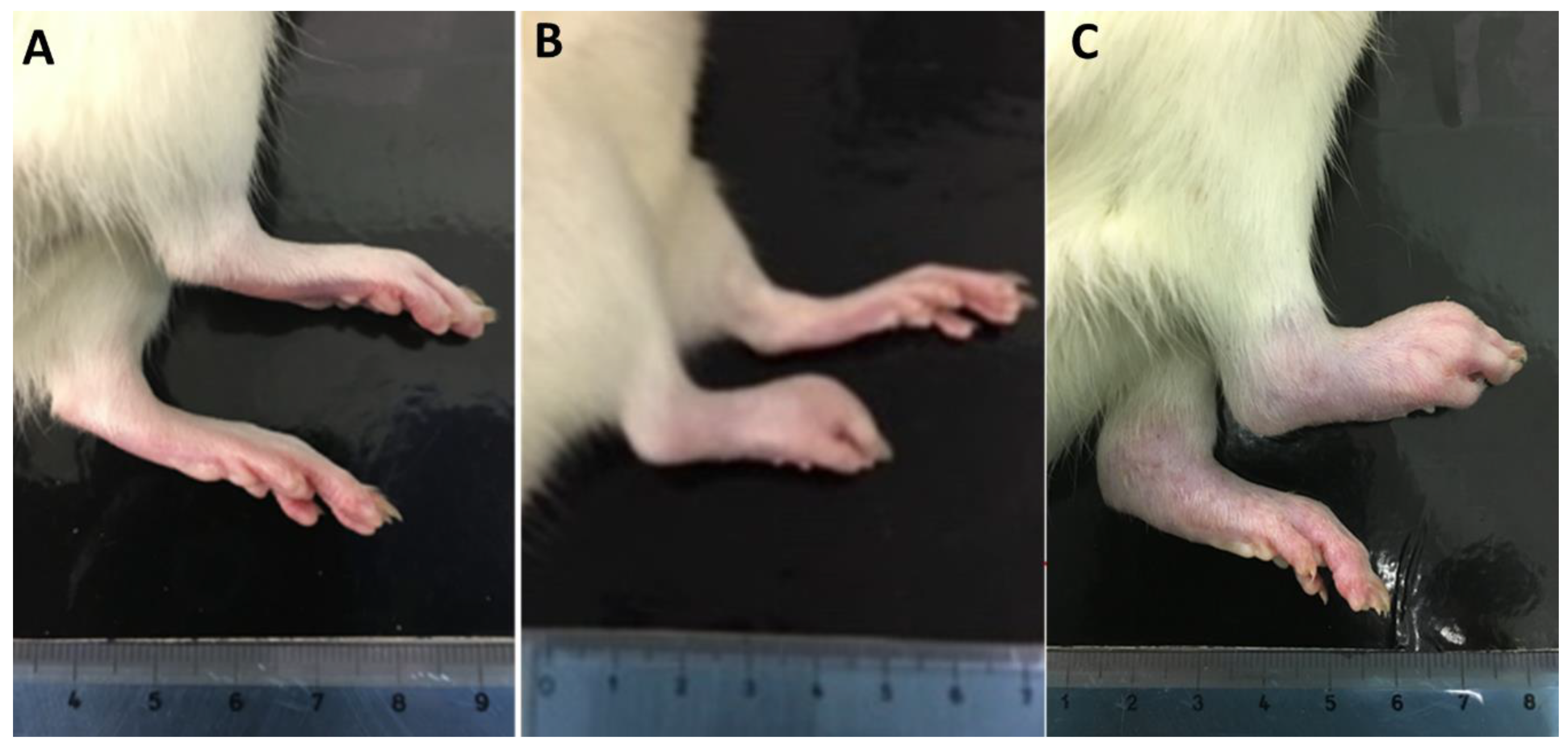
2.8. Hind Paw Volume Assessment
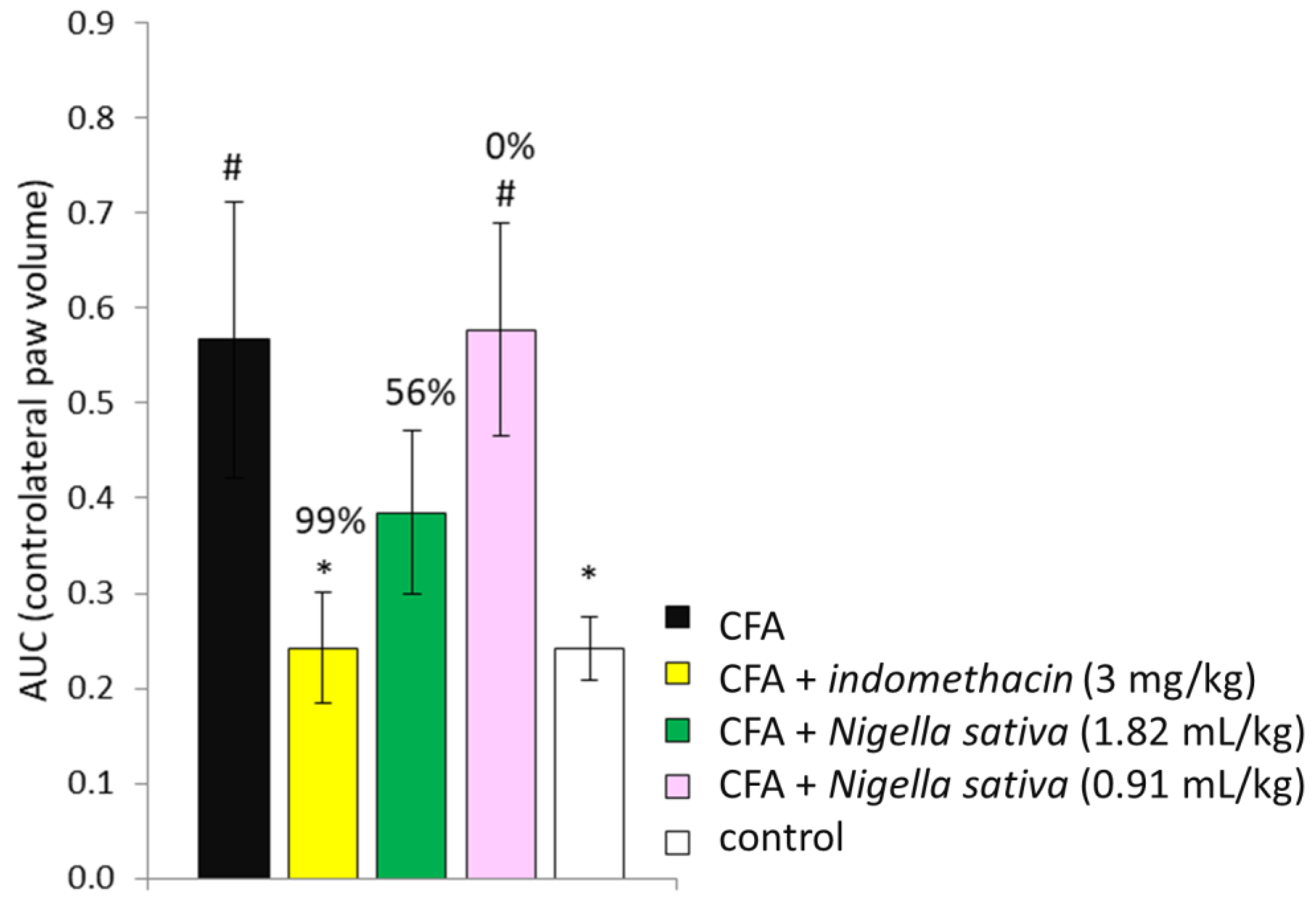
2.9. Percentage Inhibition of Paw Edema
2.10. Arthritis Score
2.11. Spontaneous Locomotor Activity
2.12. Mechanical Allodynia
2.13. Plasma IL-6, CRP, Albumin and TC Analysis
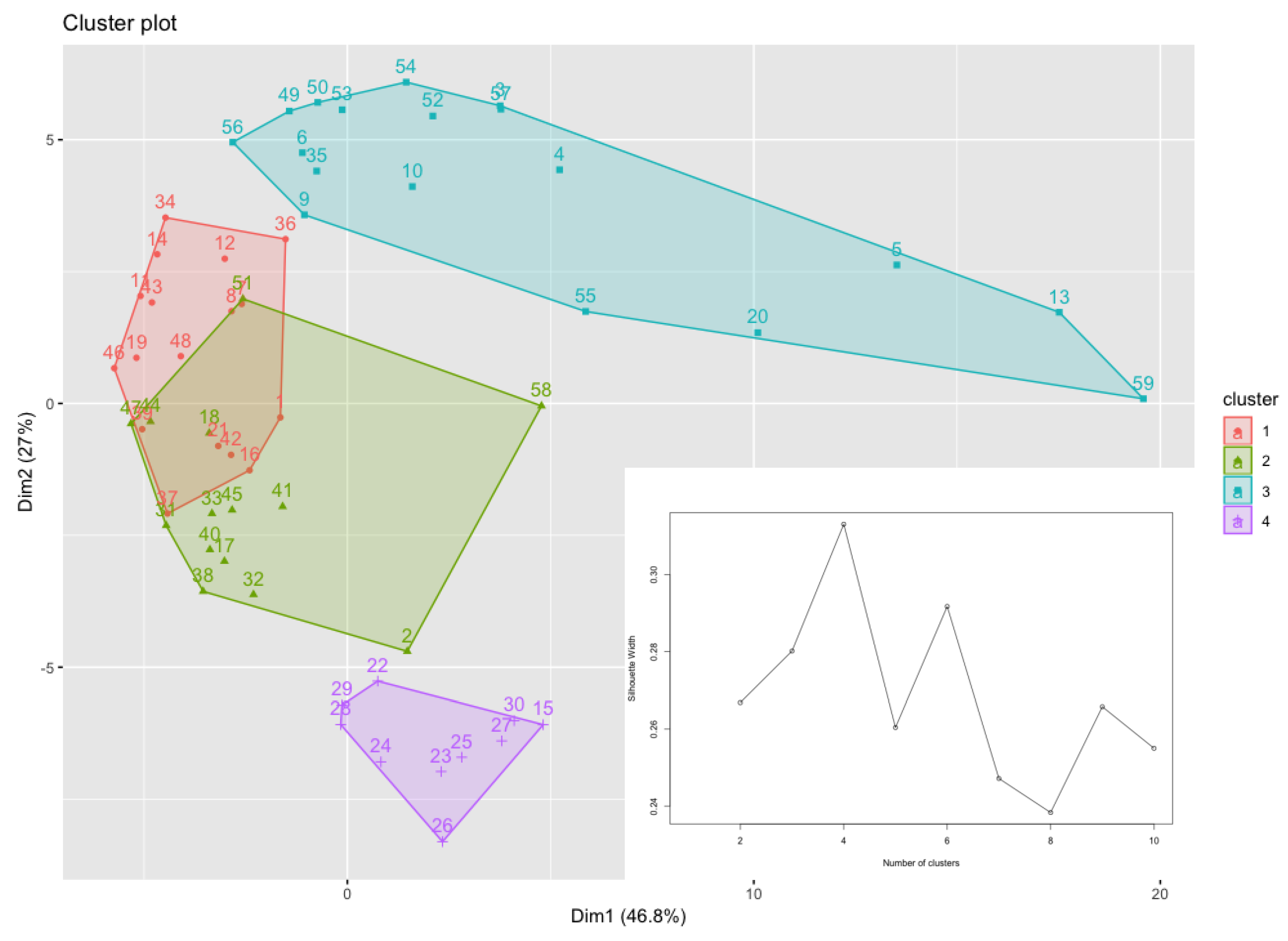
2.14. Clustering Analysis of Haematological Parameters
2.15. Statistical Analysis
3. Results
3.1. Fatty Acids and Tocopherols Levels in Nigella sativa Oil
3.2. Safety Profile of Nigella sativa Oil in Rats
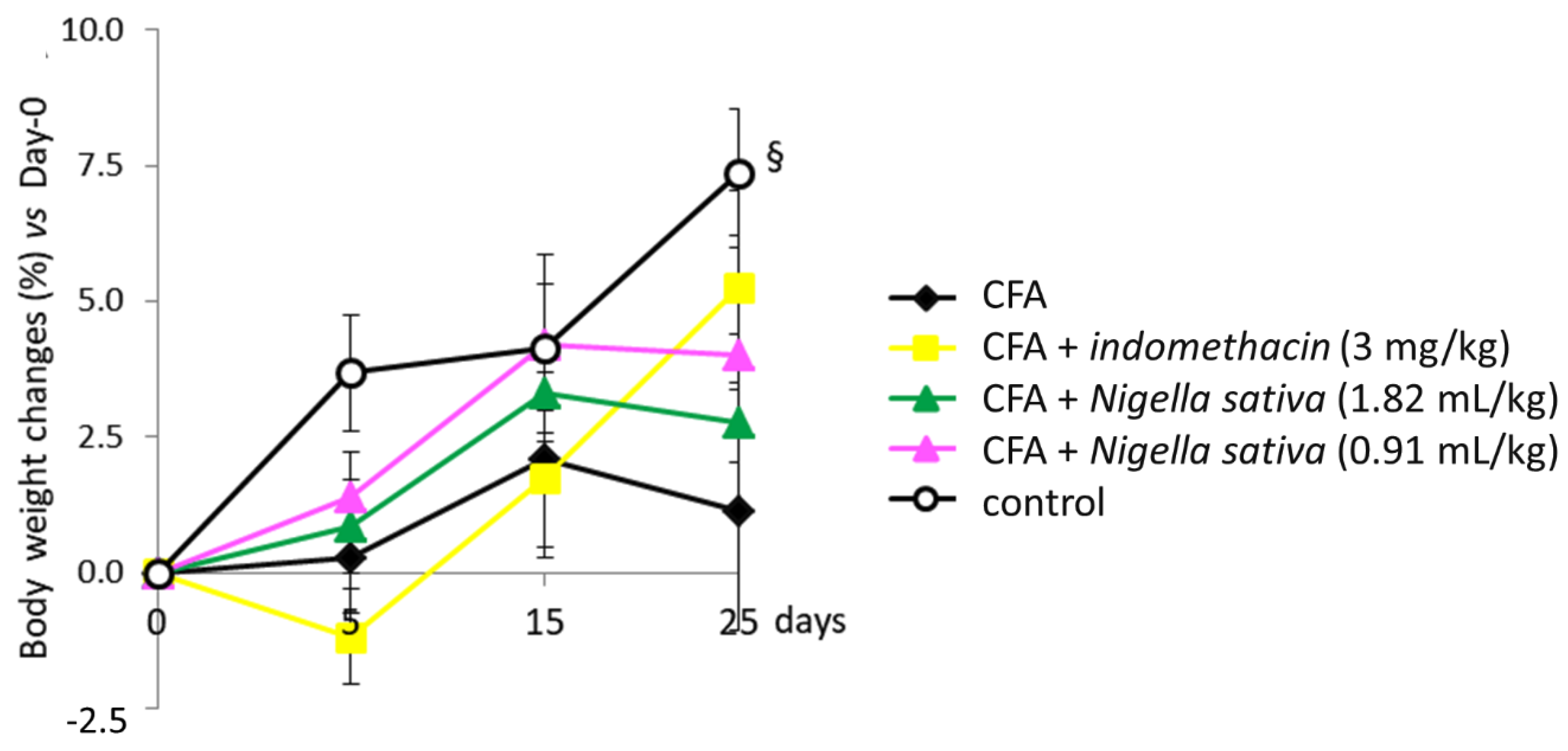
3.3. Body Weight Changes in CFA-Induced Arthritic Rats
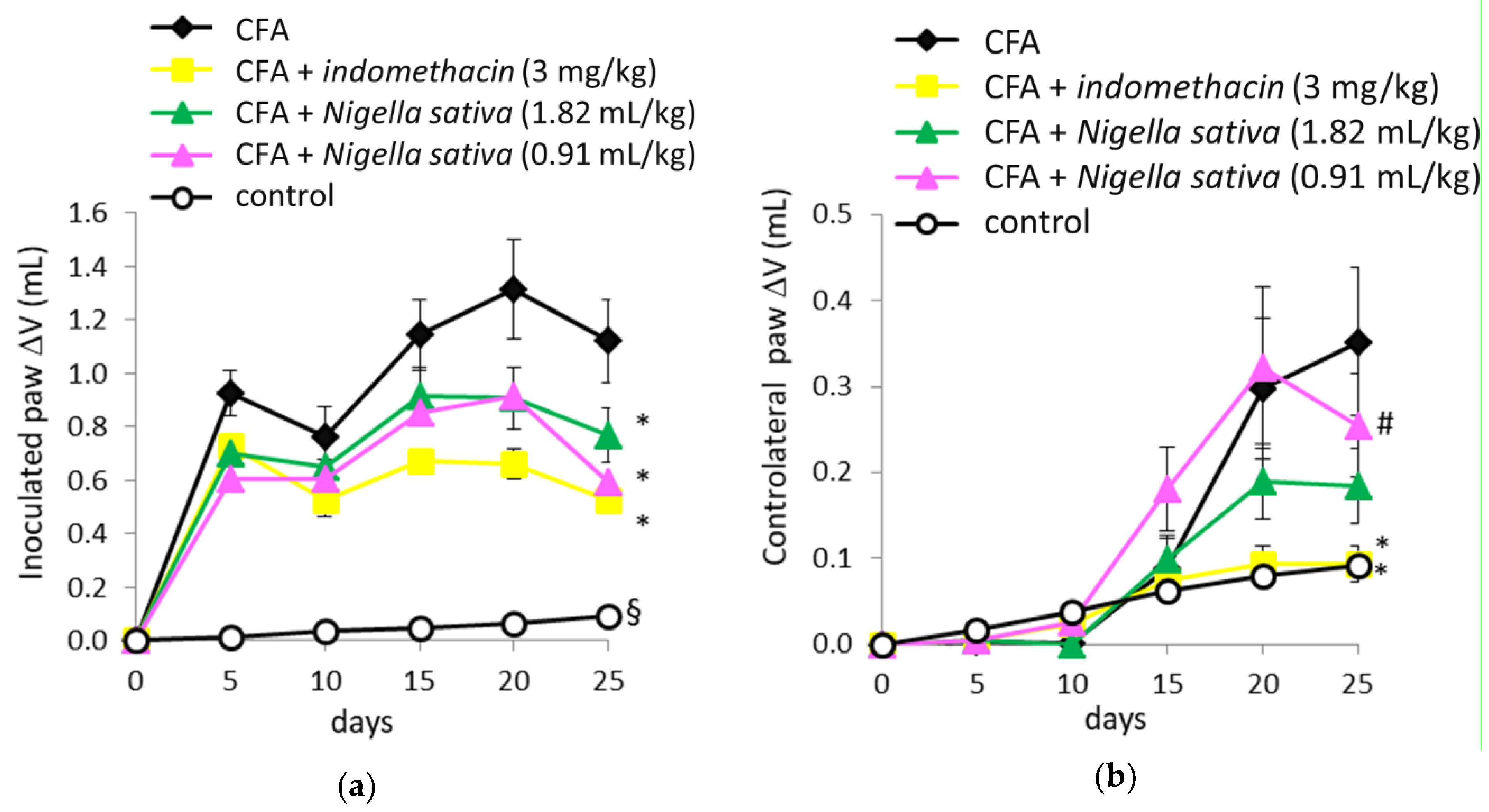
3.4. Anti-Inflammatory Activity of Nigella sativa Oil in CFA-Induced Arthritic Rats
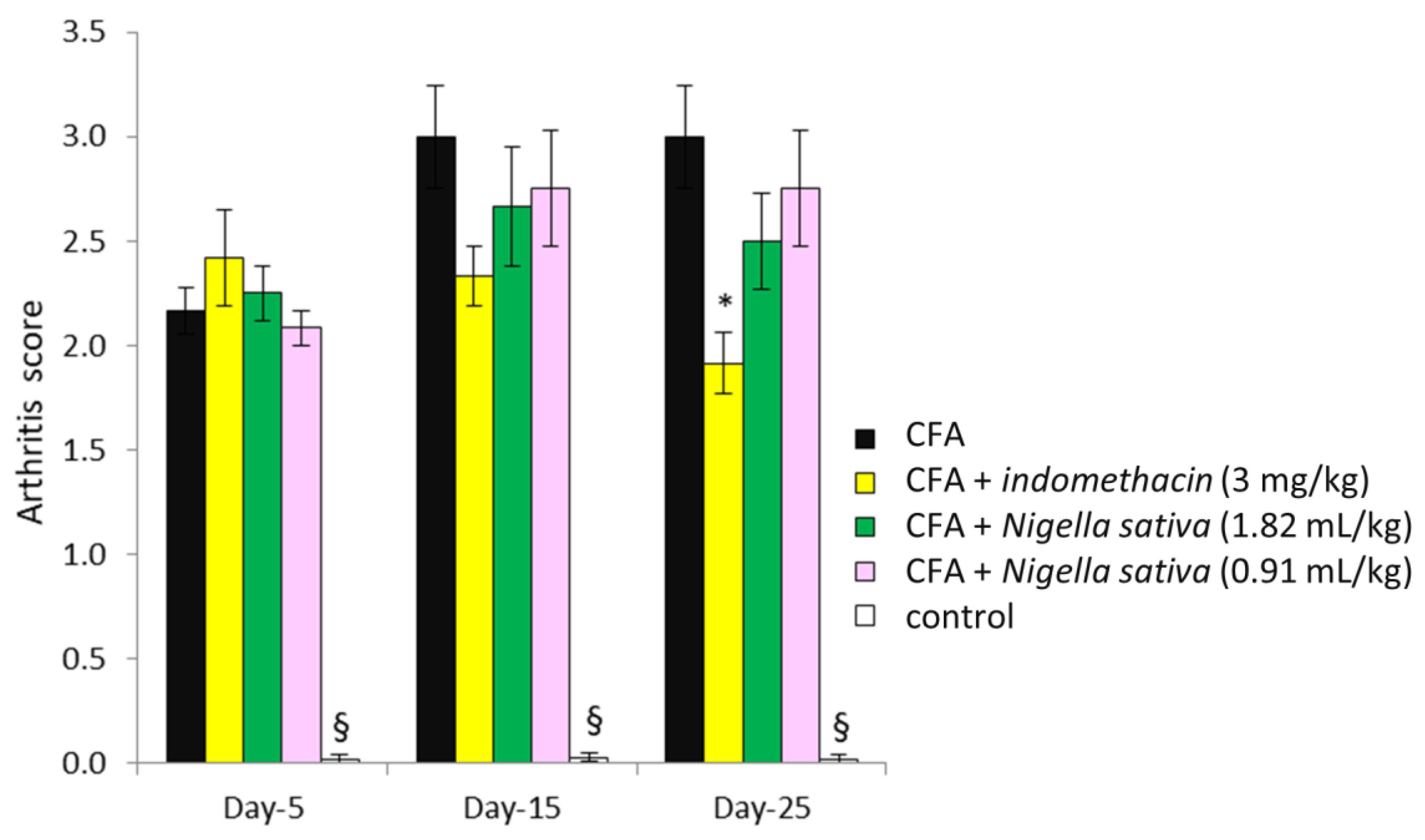
3.5. Effect of Nigella sativa Oil on the Arthritis Score in CFA-Induced Arthritic Rats
3.6. Effect of Nigella sativa Oil on Spontaneous Locomotor Activity in CFA-Induced Arthritic Rats
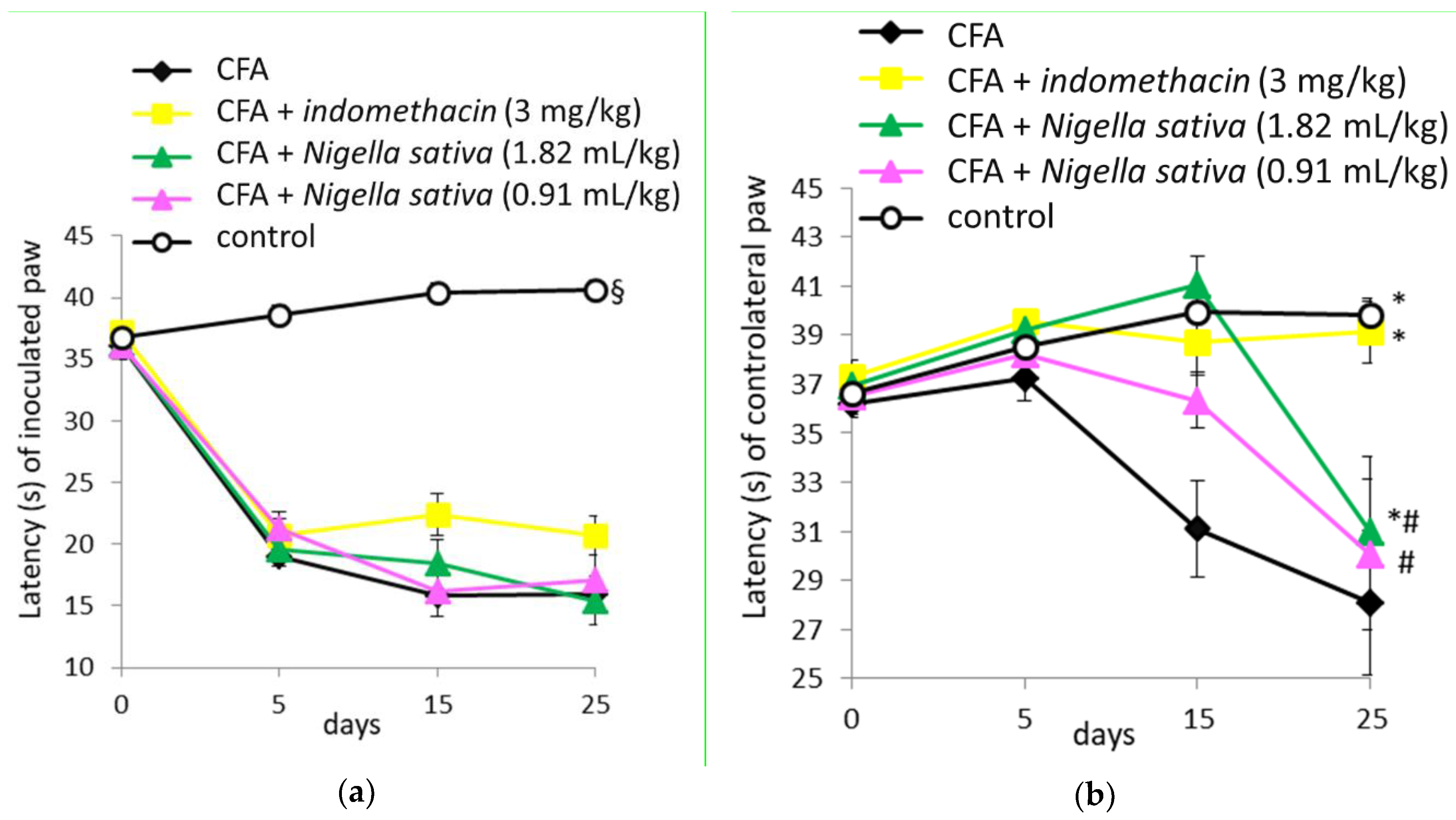
3.7. Anti-Nociceptive Activity of Nigella sativa Oil in CFA-Induced Arthritic Rats
3.8. Effect of Nigella sativa Oil on Plasma IL-6, CRP, Albumin and TC Levels in CFA-Induced Arthritic Rats
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References and Note
- Calabresi, E.; Petrelli, F.; Bonifacio, A.F.; Puxeddu, I.; Alunno, A. One year in review 2018: Pathogenesis of rheumatoid arthritis. Clin. Exp. Rheumatol. 2018, 36, 175–184. [Google Scholar] [PubMed]
- Markenson, J.A. Worldwide trends in the socioeconomic impact and long-term prognosis of rheumatoid arthritis. Semin. Arthritis Rheum. 1991, 21, 4–12. [Google Scholar] [CrossRef]
- Bendele, A. Animal models of rheumatoid arthritis. J. Musculoskelet. Neuronal Interact. 2001, 1, 377–385. [Google Scholar] [PubMed]
- Bolon, B.; Stolina, M.; King, C.; Middleton, S.; Gasser, J.; Zack, D.; Feige, U. Rodent preclinical models for developing novel antiarthritic molecules: Comparative biology and preferred methods for evaluating efficacy. J. Biomed. Biotechnol. 2011, 2011, 569068. [Google Scholar] [CrossRef] [PubMed]
- Bevaart, L.; Vervoordeldonk, M.J.; Tak, P.P. Evaluation of therapeutic targets in animal models of arthritis: How does it relate to rheumatoid arthritis? Arthritis Rheum. 2010, 62, 2192–2205. [Google Scholar] [CrossRef] [PubMed]
- Szekanecz, Z.; Halloran, M.M.; Volin, M.V.; Woods, J.M.; Strieter, R.M.; Kenneth Haines, G., 3rd; Kunkel, S.L.; Burdick, M.D.; Koch, A.E. Temporal expression of inflammatory cytokines and chemokines in rat adjuvant-induced arthritis. Arthritis Rheum. 2000, 43, 1266–1277. [Google Scholar] [CrossRef]
- Gaffo, A.; Saag, K.G.; Curtis, J.R. Treatment of rheumatoid arthritis. Am. J. Health Syst. Pharm. 2006, 63, 2451–2465. [Google Scholar] [CrossRef] [PubMed]
- Gholamnezhad, Z.; Havakhah, S.; Boskabady, M.H. Preclinical and clinical effects of Nigella sativa and its constituent, thymoquinone: A review. J. Ethnopharmacol. 2016, 190, 372–386. [Google Scholar] [CrossRef]
- Ikhsan, M.; Hiedayati, N.; Maeyama, K.; Nurwidya, F. Nigella sativa as an anti-inflammatory agent in asthma. BMC Res. Notes 2018, 11, 744. [Google Scholar] [CrossRef]
- Bordoni, L.; Fedeli, D.; Nasuti, C.; Maggi, F.; Papa, F.; Wabitsch, M.; De Caterina, R.; Gabbianelli, R. Antioxidant and anti-inflammatory properties of Nigella sativa oil in human pre-adipocytes. Antioxidants 2019, 8, 51. [Google Scholar] [CrossRef]
- Commission Delegated Regulation (EU) 2015/1830 of 8 July 2015 amending Regulation (EEC) No 2568/91 on the characteristics of olive oil and olive residue oil and on the relevant methods of analysis.
- Esposto, S.; Taticchi, A.; Di Maio, I.; Urbani, S.; Veneziani, G.; Selvaggini, R.; Servili, M. Effect of an olive phenolic extract on the quality of vegetable oils during frying. Food Chem. 2015, 176, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Organization for Economic Co-operation and Development (OECD) Guideline No. 423, Acute Oral Toxicity in Animals, OECD/OCDE No. 423. Adopted 17 December 2001. Available online: http://www.ntp.niehs.nih.gov/iccvam/suppdocs/feddocs/oecd/oecd_gl423.pdf (accessed on 17 December 2001).
- Abbadie, C.; Besson, J.M.; Calvino, B. c-Fos expression in the spinal cord and pain-related symptoms induced by chronic arthritis in the rat are prevented by pretreatment with Freund adjuvant. J. Neurosci. 1994, 14, 5865–5871. [Google Scholar] [CrossRef] [PubMed]
- Contó, M.B.; de Carvalho, J.G.; Benedito, M.A. Behavioral differences between subgroups of rats with high and low threshold to clonic convulsions induced by DMCM, a benzodiazepine inverse agonist. Pharmacol. Biochem. Behav. 2005, 82, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Nasuti, C.; Carloni, M.; Fedeli, D.; Gabbianelli, R.; Di Stefano, A.; Cerasa, L.S.; Silva, I.; Domingues, V.; Ciccocioppo, R. Effects of early life permethrin exposure on spatial working memory and on monoamine levels in different brain areas of pre-senescent rats. Toxicology 2013, 303, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, J.E. Automated serum albumin determination by use of the immediate reaction with bromcresol green reagent. Clin. Chem. 1978, 24, 369–373. [Google Scholar] [PubMed]
- Allain, C.C.; Poon, L.S.; Chan, C.S.; Richmond, W.; Fu, P.C. Enzymatic determination of total serum cholesterol. Clin. Chem. 1974, 20, 470–475. [Google Scholar] [PubMed]
- Kaufman, L.; Rousseeuw, P.J. Partitioning around medoids (program PAM). In Finding Groups in Data; Wiley: Hoboken, NJ, USA, 2008; pp. 68–125. [Google Scholar]
- Gharby, S.; Harhar, H.; Guillaume, D.; Roudani, A.; Boulbaroud, S.; Ibrahimi, M.; Ahmad, M.; Sultana, S.; Ben Haddah, T.; Chafchaouni-Moussaouii, I.; et al. Chemical investigation of Nigella sativa L. seed oil produced in Morocco. J. Saudi Soc. Agric. Sci. 2015, 14, 172–177. [Google Scholar] [CrossRef]
- Matthaus, B.; Ozcan, M.M. Fatty acids, tocopherol, and sterol contents of some Nigella species seed oil. Czech J. Food Sci. 2011, 29, 145–150. [Google Scholar] [CrossRef]
- Umar, S.; Zargan, J.; Umar, K.; Ahmad, S.; Katiyar, C.K.; Khan, H.A. Modulation of the oxidative stress and inflammatory cytokine response by thymoquinone in the collagen induced arthritis in Wistar rat. Chem. Biol. Interact. 2012, 197, 40–46. [Google Scholar] [CrossRef]
- Amin, B.; Hosseinzadeh, H. Black Cumin (Nigella sativa) and Its Active Constituent, Thymoquinone: An Overview on the Analgesic and Anti-inflammatory Effects. Planta Med. 2016, 82, 8–16. [Google Scholar] [CrossRef]
- Zaoui, A.; Cherrah, Y.; Mahassini, N.; Alaoui, K.; Amarouch, H.; Hassar, M. Acute and chronic toxicity of Nigella sativa fixed oil. Phytomedicine 2002, 9, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Ali, B.H.; Blunden, G. Pharmacological and toxicological properties of Nigella sativa. Phytother. Res. 2003, 17, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Granado, M.; Priego, T.; Martín, A.I.; Villanúa, M.A.; López-Calderón, A. Ghrelin receptor agonist GHRP-2 prevents arthritis-induced increase in E3 ubiquitin-ligating enzymes MuRF1 and MAFbx gene expression in skeletal muscle. Am. J. Physiol. Endocrinol. Metab. 2005, 289, E1007–E1014. [Google Scholar] [CrossRef] [PubMed]
- Narendhirakannan, R.T.; Subramanian, S.; Kandaswamy, M. Anti-inflammatory and lysosomal stability actions of Cleome gynandra L. studied in adjuvant induced arthritic rats. Food Chem. Toxicol. 2007, 45, 1001–1012. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, L.K.; Chandrul, K.K.; Sharma, U.S. Evaluation of Anti-arthritic activity of Ficus benghalensis Linn. root extracts on Freund’s adjuvant induced Arthritis in rats. J. Phytopharmacol. 2016, 5, 10–14. [Google Scholar]
- Al-Ghamdi, M.S. The anti-inflammatory, analgesic and antipyretic activity of Nigella sativa. J. Ethnopharmacol. 2001, 76, 45–48. [Google Scholar] [CrossRef]
- Tanko, Y.; Mohammed, A.; Okasha, M.A.; Shuaibu, A.; Magaji, M.G.; Yaro, A.H. Analgesic and anti-inflammatory activities of ethanol seed extract of Nigella sativa (black cumin) in mice and rats. Eur. J. Sci. Res. 2007, 18, 277–281. [Google Scholar]
- Philips, L.; Gegout-Pottie, P.; Guingamp, C.; Bordji, K.; Terlain, B.; Netter, P.; Gillet, P. Relations between functional, inflammatory, and degenerative parameters during adjuvant arthritis in rats. Am. J. Physiol. 1997, 273, R1550–R1556. [Google Scholar]
- Anderson, G.D.; Hauser, S.D.; McGarity, K.L.; Bremer, M.E.; Isakson, P.C.; Gregory, S.A. Selective inhibition of cyclooxygenase (COX)-2 reverses inflammation and expression of COX-2 and interleukin 6 in rat adjuvant arthritis. J. Clin. Investig. 1996, 97, 2672–2679. [Google Scholar] [CrossRef]
- Leisten, J.C.; Gaarde, W.A.; Scholz, W. Interleukin-6 serum levels correlate with footpad swelling in adjuvant-induced arthritic Lewis rats treated with cyclosporin A or indomethacin. Clin. Immunol. Immunopathol. 1990, 56, 108–115. [Google Scholar] [CrossRef]
- Thiesen-Popp, P.; Pape, H.; Muller-Peddinghaus, R. Interleukin-6 (IL-6) in adjuvant arthritis of rats and its pharmacological modulation. Int. J. Immunopharmacol. 1992, 14, 565–571. [Google Scholar] [CrossRef]
- Rhodes, B.; Furnrohr, B.G.; Vyse, T.J. C-reactive protein in rheumatology: Biology and genetics. Nat. Rev. Rheumatol. 2011, 7, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Wahba, M.G.; Messiha, B.A.; Abo-Saif, A.A. Protective effects of fenofibrate and resveratrol in an aggressive model of rheumatoid arthritis in rats. Pharm. Biol. 2016, 54, 1705–1715. [Google Scholar] [CrossRef] [PubMed]
- Abdel El-Gaphar, O.A.M.; Abo-Youssef, A.M.; Abo-Saif, A.A. Effect of losartan in complete freund’s adjuvant -induced arthritis in rats. Iran. J. Pharm. Res. 2018, 17, 1420–1430. [Google Scholar] [PubMed]
- Jurcovicova, J.; Svik, K.; Scsukova, S.; Bauerova, K.; Rovensky, J.; Stancikova, M. Methotrexate treatment ameliorated testicular suppression and anorexia related leptin reduction in rats with adjuvant arthritis. Rheumatol. Int. 2009, 29, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Hadi, V.; Kheirouri, S.; Alizadeh, M.; Khabbazi, A.; Hosseini, H. Effects of Nigella sativa oil extract on inflammatory cytokine response and oxidative stress status in patients with rheumatoid arthritis: A randomized, double-blind, placebo-controlled clinical trial. Avicenna J. Phytomed. 2016, 6, 34–43. [Google Scholar]
- Mahboubi, M.; Kashani, L.M.T.; Mahboubi, M. Nigella sativa fixed oil as alternative treatment in management of pain in arthritis rheumatoid. Phytomedicine 2018, 46, 69–77. [Google Scholar] [CrossRef]
- Sahebkar, A.; Beccuti, G.; Simental-Mendía, L.E.; Nobili, V.; Bo, S. Nigella sativa (black seed) effects on plasma lipid concentrations in humans: A systematic review and meta-analysis of randomized placebo-controlled trials. Pharmacol. Res. 2016, 106, 37–50. [Google Scholar] [CrossRef]
- Li, G.M.; Zhao, J.; Li, B.; Zhang, X.F.; Ma, J.X.; Ma, X.L.; Liu, J. The anti-inflammatory effects of statins on patients with rheumatoid arthritis: A systemic review and meta-analysis of 15 randomized controlled trials. Autoimmun. Rev. 2018, 17, 215–225. [Google Scholar] [CrossRef]
- Lakatos, J.; Hárságyi, A. Serum total, HDL, LDL cholesterol, and triglyceride levels in patients with rheumatoid arthritis. Clin. Biochem. 1988, 21, 93–96. [Google Scholar] [CrossRef]
- Lazarevic, M.B.; Vitic, J.; Myones, B.L.; Mladenovic, V.; Nanusevic, N.; Skosey, J.L.; Swedler, W.I. Antilipoprotein antibodies in rheumatoid arthritis. Semin. Arthritis Rheum. 1993, 22, 385–391. [Google Scholar] [CrossRef]
- Dursunoğlu, D.; Evrengül, H.; Polat, B.; Tanriverdi, H.; Cobankara, V.; Kaftan, A.; Kiliç, M. Lp(a) lipoprotein and lipids in patients with rheumatoid arthritis: Serum levels and relationship to inflammation. Rheumatol. Int. 2005, 25, 241–245. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fatty Acid and Tocopherol | Mean ± SD |
|---|---|
| Myristic acid (C14:0) | 0.16 ± 0.01 |
| Palmitic acid (C16:0) | 12.80 ± 0.21 |
| Palmitoleic acid (C16:1) | 0.18 ± 0.01 |
| Margaric acid (C17:0) | 0.08 ± 0.001 |
| Margaroleic acid (C17:1) | 0.06 ± 0.001 |
| Stearic acid (C18:0) | 3.39 ± 0.01 |
| Oleic acid (C18:1) | 24.65 ± 0.02 |
| Linoleic acid (18:2) | 57.92 ± 0.19 |
| Linolenic acid (C18:3) | 0.22 ± 0.002 |
| Arachidic acid (C20:0) | 0.24 ± 0.01 |
| Eicosenoic acid (C20:1) | 0.30 ± 0.02 |
| Saturated fatty acid (SFA) | 16.67 ± 0.21 |
| Monounsaturated fatty acid (MUFA) | 25.19 ± 0.03 |
| Polyunsaturated fatty acid (PUFA) | 58.14 ± 0.19 |
| α-Tocopherol | 26.60 ± 1.60 |
| γ-Tocopherol | 103.90 ± 5.90 |
| CFA n = 12 rats | CFA + Indomethacin (3 mg/kg) n = 12 rats | CFA + Nigella sativa (1.82 mL/kg) n = 12 rats | CFA + Nigella sativa (0.91 mL/kg) n = 12 rats | Control n = 11 rats | ||
|---|---|---|---|---|---|---|
| IL-6 | Day 15 | 465.12 ± 136.87 | 310.24 ± 100.10 * | 522.86 ± 148.47 # | 418.21 ± 25.98 # | 249.70 ± 26.02 * |
| (pg/mL) | Day 25 | 241.67 ± 90.14 | 218.33 ± 77.76 | 254.05 ± 54.60 | 258.46 ± 44.22 | 243.17 ± 26.14 |
| CRP | Day 15 | 3.23 ± 1.63 | 2.45 ± 0.54 | 4.91 ± 0.90 ## | 4.49 ± 0.43 ## | 2.90 ± 1.36 |
| (mg/mL) | Day 25 | 3.29 ± 0.55 | 2.30 ± 1.02 | 2.80 ± 0.80 | 2.71 ± 0.58 | 2.91 ± 1.36 |
| Albumin | Day 15 | 2.06 ± 0.35 | 2.05 ± 0.44 | 2.24 ± 0.30 | 2.24 ± 0.28 | 2.81 ± 0.30 § |
| (g/dL) | Day 25 | 2.41 ± 0.29 | 2.19 ± 0.74 | 2.19 ± 0.25 | 2.21 ± 0.37 | 2.82 ± 0.30 § |
| TC | Day 15 | 58.05 ± 11.18 | 58.06 ± 12.05 | 59.69 ± 7.89 | 64.72 ± 8.05 | 60.00 ± 10.73 |
| (mg/dL) | Day 25 | 66.49 ± 12.13 | 62.73 ± 15.65 | 51.12 ± 10.55 * | 52.36 ± 9.53 * | 61.04 ± 10.74 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasuti, C.; Fedeli, D.; Bordoni, L.; Piangerelli, M.; Servili, M.; Selvaggini, R.; Gabbianelli, R. Anti-Inflammatory, Anti-Arthritic and Anti-Nociceptive Activities of Nigella sativa Oil in a Rat Model of Arthritis. Antioxidants 2019, 8, 342. https://doi.org/10.3390/antiox8090342
Nasuti C, Fedeli D, Bordoni L, Piangerelli M, Servili M, Selvaggini R, Gabbianelli R. Anti-Inflammatory, Anti-Arthritic and Anti-Nociceptive Activities of Nigella sativa Oil in a Rat Model of Arthritis. Antioxidants. 2019; 8(9):342. https://doi.org/10.3390/antiox8090342
Chicago/Turabian StyleNasuti, Cinzia, Donatella Fedeli, Laura Bordoni, Marco Piangerelli, Maurizio Servili, Roberto Selvaggini, and Rosita Gabbianelli. 2019. "Anti-Inflammatory, Anti-Arthritic and Anti-Nociceptive Activities of Nigella sativa Oil in a Rat Model of Arthritis" Antioxidants 8, no. 9: 342. https://doi.org/10.3390/antiox8090342
APA StyleNasuti, C., Fedeli, D., Bordoni, L., Piangerelli, M., Servili, M., Selvaggini, R., & Gabbianelli, R. (2019). Anti-Inflammatory, Anti-Arthritic and Anti-Nociceptive Activities of Nigella sativa Oil in a Rat Model of Arthritis. Antioxidants, 8(9), 342. https://doi.org/10.3390/antiox8090342