Sex Differences in Glutathione Peroxidase Activity and Central Obesity in Patients with Type 2 Diabetes at High Risk of Cardio-Renal Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Biochemical Assessments
2.2. Antioxidant Defense Assessment
2.3. Body Adiposity Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gomez-Marcos, M.A.; Recio-Rodriguez, J.I.; Gomez-Sanchez, L.; Agudo-Conde, C.; Rodríguez-Sanchez, E.; Maderuelo-Fernandez, J.; Gomez-Sanchez, M.; García-Ortiz, L. LOD-DIABETES Group. Sex differences in the progression of target organ damage in patients with increased insulin resistance: The LOD-DIABETES study. Cardiovasc. Diabetol. 2015, 14, 132–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huxley, R.; Barzi, F.; Woodward, M. Excess risk of fatal coronary heart disease associated with diabetes in men and women: Meta-analysis of 37 prospective cohort studies. BMJ 2006, 332, 73–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kardassis, D.; Karason, K.; Narbro, K.; Lystig, T. Female obesity appears to reverse sex differences in cardiovascular disease incidence. Int. J. Cardiol. 2007, 119, S11. [Google Scholar] [CrossRef]
- Goh, L.G.H.; Dhaliwal, S.S.; Welborn, T.A.; Lee, A.H.; Della, P.R. Anthropometric measurements of general and central obesity and the prediction of cardiovascular disease risk in women: A cross-sectional study. BMJ 2014, 4, e004138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef]
- Couillard, C.; Ruel, G.; Archer, W.R.; Pomerleau, S.; Bergeron, J.; Couture, P.; Lamarche, B.; Bergeron, N. Circulating levels of oxidative stress markers and endothelial adhesion molecules in men with abdominal obesity. J. Clin. Endocrinol. Metab. 2005, 90, 6454–6459. [Google Scholar] [CrossRef] [Green Version]
- Pou, K.M.; Massaro, J.M.; Hoffmann, U.; Vasan, R.S.; Maurovich-Horvat, P.; Larson, M.G.; Keaney, J.F., Jr.; Meigs, J.B.; Lipinska, I.; Kathiresan, S.; et al. Visceral and subcutaneous adipose tissue volumes are cross-sectionally related to markers of inflammation and oxidative stress: The Framingham Heart Study. Circulation 2007, 116, 1234–1241. [Google Scholar] [CrossRef] [Green Version]
- Stanton, R.C. Oxidative stress and diabetic kidney disease. Curr. Diab. Rep. 2011, 11. [Google Scholar] [CrossRef]
- Popolo, A.; Autore, G.; Pinto, A.; Marzocco, S. Oxidative stress in patients with cardiovascular disease and chronic renal failure. Free Radic. Res. 2013, 47, 346–356. [Google Scholar] [CrossRef]
- Patel, R.S.; Al Mheid, I.; Morris, A.A.; Ahmed, Y.; Kavtaradze, N.; Ali, S.; Dabhadkar, K.; Brigham, K.; Hooper, W.C.; Alexander, R.W.; et al. Oxidative stress is associated with impaired arterial elasticity. Atherosclerosis 2011, 2018, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Correia, M.L.G.; Haynes, W.G. Arterial compliance and endothelial function. Curr. Diab. Rep. 2007, 7, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Khera, R.; Corrales-Medina, V.F.; Townsend, R.R.; Chirinos, J.A. Review: Inflammation and arterial stiffness in humans. Atherosclerosis 2014, 237, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Cherney, D.Z.I.; Scholey, J.W.; Sochett, E.B. Sex differences in renal responses to hyperglycemia, l-Arginine, and l-NMMA in humans with uncomplicated Type 1 Diabetes. Diabetes Care 2013, 36, 1290–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rask-Madsen, C.; King, G.L. Vascular complications of diabetes: Mechanisms of injury and protective factors. Cell Metab. 2013, 17, 20–33. [Google Scholar] [CrossRef] [Green Version]
- Forbes, J.M.; Coughlan, M.T.; Cooper, M. Oxidative stress as a major culprit in kidney disease in diabetes. Diabetes 2008, 57, 1446–1454. [Google Scholar] [CrossRef] [Green Version]
- Kurutas, E.B. The importance of antioxidants which play the role in cellular response against oxidative/nitrosative stress: Current state. Nutr. J. 2016, 15, 71. [Google Scholar] [CrossRef] [Green Version]
- Covas, M.I.; Flores-Mateo, G.; Carrillo-Santisteve, P.; Elosua, R.; Guallar, E.; Marrugat, J.; Bleys, J. Antioxidant enzyme activity and coronary heart disease: Meta-analyses of observational studies. Am. J. Epidemiol. 2009, 170, 135–147. [Google Scholar]
- Avissar, N.; Ornt, D.B.; Yagil, Y.; Horowitz, S.; Watkins, R.H.; Kerl, E.A.; Takahashi, K.; Palmer, I.S.; Cohen, H.J. Human kidney proximal tubules are the main source of plasma glutathione peroxidase. Am. J. Physiol. 1994, 266, C367–C375. [Google Scholar] [CrossRef]
- Maser, R.L.; Magenheimer, B.S.; Calvet, J.P. Mouse plasma glutathione peroxidase. Cdna sequence analysis and renal proximal tubular expression and secretion. J. Biol. Chem. 1994, 269, 27066–27073. [Google Scholar]
- Yoshimura, S.; Watanabe, K.; Suemizu, H.; Onozawa, T.; Mizoguchi, J.; Tsuda, K.; Hatta, H.; Moriuchi, T. Tissue specific expression of the plasma glutathione peroxidase gene in rat kidney. J. Biochem. 1991, 109, 918–923. [Google Scholar] [CrossRef]
- Lee, Y.S.; Kim, A.Y.; Choi, J.W.; Kim, M.; Yasue, S.; Son, H.J.; Masuzaki, H.; Park, K.S.; Kim, J.B. Dysregulation of adipose glutathione peroxidase 3 in obesity contributes to local and systemic oxidative stress. Mol. Endocrinol. 2008, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceballos-Picot, I.; Witko-Sarsat, V.; Merad-Boudia, M.; Nguyen, A.T.; Thévenin, M.; Jaudon, M.C.; Zingraff, J.; Verger, C.; Jungers, P.; Descamps-Latscha, B. Glutathione antioxidant system as a marker of oxidative stress in chronic renal failure. Free Radic. Biol. Med. 1996, 21, 845–853. [Google Scholar] [CrossRef]
- Crawford, A.; Fassett, R.G.; Coombes, J.S.; Kunde, D.A.; Ahuja, K.D.; Robertson, I.K.; Ball, M.J.; Geraghty, D.P. Glutathione peroxidase, superoxide dismutase and catalase genotypes and activities and the progression of chronic kidney disease. Nephrol. Dial. Transplant. 2011, 26, 2806–2813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassalle, C.; Maffei, S.; Boni, C.; Zucchelli, G.C. Gender-related differences in oxidative stress levels among elderly patients with coronary artery disease. Fertil Steril. 2008, 89, 608–613. [Google Scholar] [CrossRef]
- Earle, K.A.; Zitouni, K.; Pepe, J.; Karaflou, M.; Godbold, J.R. Modulation of endogenous antioxidant defense and progression of kidney disease in multi-heritage groups of patients with type 2 diabetes: Prospective Evaluation of Early Nephropathy and its Treatment (PREVENT). J. Transl. Med. 2016, 14, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A. Estimating GFR Using the CKD Epidemiology Collaboration (CKD-EPI) Creatinine Equation: More Accurate GFR Estimates, Lower CKD Prevalence Estimates, and Better Risk Predictions. Am. J. Kidney Dis. 2010, 55, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Zitouni, K.; Nourooz-Zadeh, J.; Harry, D.; Kerry, S.M.; Betteridge, D.J.; Cappuccio, F.P.; Earle, K.A. Race-specific differences in antioxidant enzyme activity in patients with type 2 diabetes. Diabetes Care 2005, 28, 1698–1703. [Google Scholar] [CrossRef] [Green Version]
- Sloth, J.; Larsen, E. The application of ICP dynamic reaction cell mass spectrometry for measurement of selenium isotopes, isotope ratios and chromatographic detection of selenoamino acids. J. Anal. At. Spectrom. 2000, 15, 669–672. [Google Scholar] [CrossRef]
- Sieniawska, C.; Mensikov, R.; Delves, H.T. Determination of total selenium in serum, whole blood and erythrocytes by ICP-MS. J. Anal. At. Spectrom. 1999, 14, 109–112. [Google Scholar] [CrossRef]
- Available online: https://www.idf.org/webdata/docs/MetSyndrome_FINAL.pdf (accessed on 1 November 2016).
- Gurzov, E.N.; Tran, M.; Fernandez-Rojo, M.A.; Merry, T.L.; Zhang, X.; Xu, Y.; Fukushima, A.; Waters, M.J.; Watt, M.J.; Andrikopoulos, S.; et al. Hepatic oxidative stress promotes insulin-STAT-5 signaling and obesity by inactivating protein tyrosine phosphatase N2. Cell Metab. 2014, 20, 85–102. [Google Scholar] [CrossRef] [Green Version]
- Amirkhizi, F.; Fereydoun, S.; Mahmoud, D.; Soudabeh, H.S. Impaired enzymatic antioxidant defense in erythrocytes of women with general and abdominal obesity. Obes. Res. Clin. Pract. 2014, 8, e26–e34. [Google Scholar] [CrossRef] [PubMed]
- Mutakin, M.; Meiliana, A.; Wijaya, A.; Kobayashi, K.; Yamazaki, C.; Kameo, S.; Nakazawa, M.; Koyama, H. Association between selenium nutritional status and metabolic risk factors in men with visceral obesity. J. Trace Elem. Med. Biol. 2013, 27, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R.; Singhai, M.; Faizy, A.F. Glutathione peroxidase activity in obese and non-obese diabetic patients and role of hyperglycaemia in oxidative stress. J. Midlife Health 2011, 2, 72–76. [Google Scholar] [PubMed]
- Galougahi, K.K.; Antoniades, C.; Nicholls, S.J.; Channon, K.M.; Figtree, G.A. Redox biomarkers in cardiovascular medicine. Eur. Heart J. 2015, 36, 1576–1582. [Google Scholar] [CrossRef] [Green Version]
- Touat-Hamici, Z.; Legrain, Y.; Bulteau, A.L.; Chavatte, L. Selective up-regulation of human selenoproteins in response to oxidative stress. J. Biol. Chem. 2014, 289. [Google Scholar] [CrossRef] [Green Version]
- Pendergrass, K.D.; Rafferty, K.; Davis, M.E. H2O2 Acutely Upregulates Glutathione Peroxidase and Catalase mRNA levels in Cardiac Progenitor Cells. FASEB J. 2011, 25, 826.3. [Google Scholar]
- Holley, A.; Pitman, J.; Miller, J.; Harding, S.; Larsen, P. Glutathione peroxidase activity and expression levels are significantly increased in acute coronary syndromes. J. Investig. Med. 2017, 65, 919–925. [Google Scholar] [CrossRef]
- Bierl, C.; Voetsch, B.; Jin, R.C.; Handy, D.E.; Loscalzo, J. Determinants of human plasma glutathione peroxidase (GPx-3) expression. J. Biol. Chem. 2004, 279, 26839–26845. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Bonet, B.; Gillenwater, H.; Knopp, R.H. Opposing effects of estrogen and progestins on LDL oxidation and vascular wall cytotoxicity: Implications for atherogenesis. Proc. Soc. Exp. Biol. Med. 1999, 222, 214–221. [Google Scholar] [CrossRef]
- Shwaery, G.T.; Vita, J.A.; Keaney, J.F. Antioxidant protection of LDL by physiological concentrations of 17 beta-estradiol. Requirement for estradiol modification. Circulation 1997, 95, 1378–1385. [Google Scholar] [CrossRef]
- Ozacmak, V.H.; Sayan, H. The effects of 17beta estradiol, 17alpha estradiol and progesterone on oxidative stress biomarkers in ovariectomized female rat brain subjected to global cerebral ischemia. Physiol. Res. 2009, 58, 909–912. [Google Scholar] [PubMed]
- Ha, B.J. Oxidative stress in ovariectomy menopause and role of chondroitin sulfate. Arch. Pharm. Res. 2004, 27, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Sack, M.N.; Rader, D.J.; Cannon, R.O. Oestrogen and inhibition of oxidation of low-density lipoproteins in postmenopausal women. Lancet 1994, 343, 269–270. [Google Scholar] [CrossRef]
- Cervellati, C.; Bergamini, C.M. Oxidative damage and the pathogenesis of menopause related disturbances and diseases. Clin. Chem. Lab. Med. 2016, 54, 739–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundholm, L.; Putnik, M.; Otsuki, M.; Andersson, S.; Ohlsson, C.; Gustafsson, J.A.; Dahlman-Wright, K. Effects of estrogen on gene expression profiles in mouse hypothalamus and white adipose tissue: Target genes include glutathione peroxidase 3 and cell death-inducing DNA fragmentation factor, alpha-subunit-like effector A. J. Endocrinol. 2008, 196, 547–557. [Google Scholar] [CrossRef] [Green Version]
- Blankenberg, S.; Rupprecht, H.J.; Bickel, C.; Torzewski, M.; Hafner, G.; Tiret, L.; Smieja, M.; Cambien, F.; Meyer, J.; Lackner, K.J. AtheroGene Investigators. Glutathione peroxidase 1 activity and cardiovascular events in patients with coronary artery disease. N. Engl. J. Med. 2003, 349, 1605–1613. [Google Scholar] [CrossRef] [Green Version]
- Borrás, C.; Gambini, J.; Gómez-Cabrera, M.C.; Sastre, J.; Pallardó, F.V.; Mann, G.E.; Viña, J. 17beta-oestradiol up-regulates longevity-related, antioxidant enzyme expression via the ERK1 and ERK2[MAPK]/NFkappaB cascade. Aging Cell 2005, 4, 113–118. [Google Scholar] [CrossRef]
- Viña, J.; Sastre, J.; Pallardó, F.; Borrás, C. Mitochondrial theory of aging: Importance to explain why females live longer than males. Antioxid. Redox Signal. 2003, 5, 549–556. [Google Scholar] [CrossRef]
- Akl, M.G.; Fawzy, E.; Deif, M.; Farouk, A.; Elshorbagy, A.K. Perturbed adipose tissue hydrogen peroxide metabolism in centrally obese men: Association with insulin resistance. PLoS ONE 2005, 12, e0177268. [Google Scholar] [CrossRef] [Green Version]
- Pinto, R.E.; Bartley, W. The nature of the sex-linked differences in glutathione peroxidase activity and aerobic oxidation of glutathione in male and female rat liver. Biochem. J. 1969, 115, 449–456. [Google Scholar] [CrossRef] [Green Version]
- Lei, X.G.; Zhu, J.; Cheng, W.; Bao, Y.; Ho, Y.S.; Reddi, A.R.; Holmgren, A.; Arnér, E.S. Paradoxical Roles of antioxidant enzymes: Basic mechanisms and health implications. Physiol. Rev. 2016, 96, 307–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaede, P.; Poulsen, H.E.; Parving, H.H.; Pedersen, O. Double-blind, randomised study of the effect of combined treatment with vitamin C and E on albuminuria in Type 2 diabetic patients. Diabetes Med. 2001, 18, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Milman, U.; Blum, S.; Shapira, C.; Aronson, D.; Miller-Lotan, R.; Anbinder, Y.; Alshiek, J.; Bennett, L.; Kostenko, M.; Landau, M.; et al. Vitamin E supplementation reduces cardiovascular events in a subgroup of middle-aged individuals with both type 2 diabetes mellitus and the haptoglobin 2–2 genotype: A prospective double-blinded clinical trial. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Langhardt, J.; Flehmig, G.; Klöting, N.; Lehmann, S.; Ebert, T.; Kern, M.; Schön, M.R.; Gärtner, D.; Lohmann, T.; Dressler, M.; et al. Effects of Weight Loss on Glutathione Peroxidase 3 Serum Concentrations and Adipose Tissue Expression in Human Obesity. Obes. Facts 2018, 11, 475–490. [Google Scholar] [CrossRef]
- Baez-Duarte, B.G.; Mendoza-Carrera, F.; García-Zapién, A.; Flores-Martínez, S.E.; Sánchez-Corona, J.; Zamora-Ginez, I.; Torres-Rasgado, E.; León-Chávez, B.A.; Pérez-Fuentes, R. Multidisciplinary Research Group on Diabetes of the Instituto Mexicano del Seguro Social. Glutathione peroxidase 3 serum levels and GPX3 gene polymorphisms in subjects with metabolic syndrome. Arch. Med. Res. 2014, 45, 375–382. [Google Scholar] [CrossRef]


{kind=link}
| Demographic/Clinical Parameters | Male (n = 86) | Female (n = 85) | p |
|---|---|---|---|
| Age (years) | 59.87 ± 8.31 | 61.58 ± 6.96 | 0.15 |
| Diabetes duration (years) | 11.06 ± 8.04 | 9.46 ± 6.97 | 0.19 |
| Ethnicity: Caucasian (%) | 49 | 33 | |
| Smoking status: current-/Ex-/ or never-smoker (%) | 11/46/43 | 6/20/74 | 0.0001 |
| Systolic blood pressure (mmHg) | 141.3 ± 15.36 | 138.77 ± 17.11 | 0.31 |
| Diastolic blood pressure (mmHg) | 83.08 ± 9.61 | 81.05 ± 8.90 | 0.16 |
| HbA1c % (mmol/mol) | 7.3 ± 3.8 (55.89 ± 18.26) | 7.6 ± 3.8 (59.07 ± 18.32) | 0.22 |
| eGFR CKD-EPI (mL/min/1.73 m2) | 88.76 ± 17.95 | 89.98 ± 16.24 | 0.64 |
| Total Cholesterol (mmol/L) | 3.89 ± 0.72 | 4.36 ± 0.92 | <0.0001 |
| Triglyceride (mmol/L) | 1.62 ± 0.89 | 1.52 ± 1.08 | 0.51 |
| HDL-cholesterol (mmol/L) | 1.19 ± 0.35 | 1.36 ± 0.35 | 0.002 |
| LDL-cholesterol (mmol/L) | 1.98 ± 0.63 | 2.34 ± 0.78 | 0.001 |
| Urinary ACR (mg:mol) | 5.48 ± 14.56 | 1.95 ± 3.06 | 0.03 |
| Bio-impedance (%) | 28.99 ± 7.68 | 40.41 ± 8.07 | <0.0001 |
| BMI (kg/m2) | 29.87 ± 4.88 | 31.02 ± 6.90 | 0.20 |
| Waist Circumference (cm) | 102.8 ± 11.7 | 101.3 ± 14.1] | 0.46 |
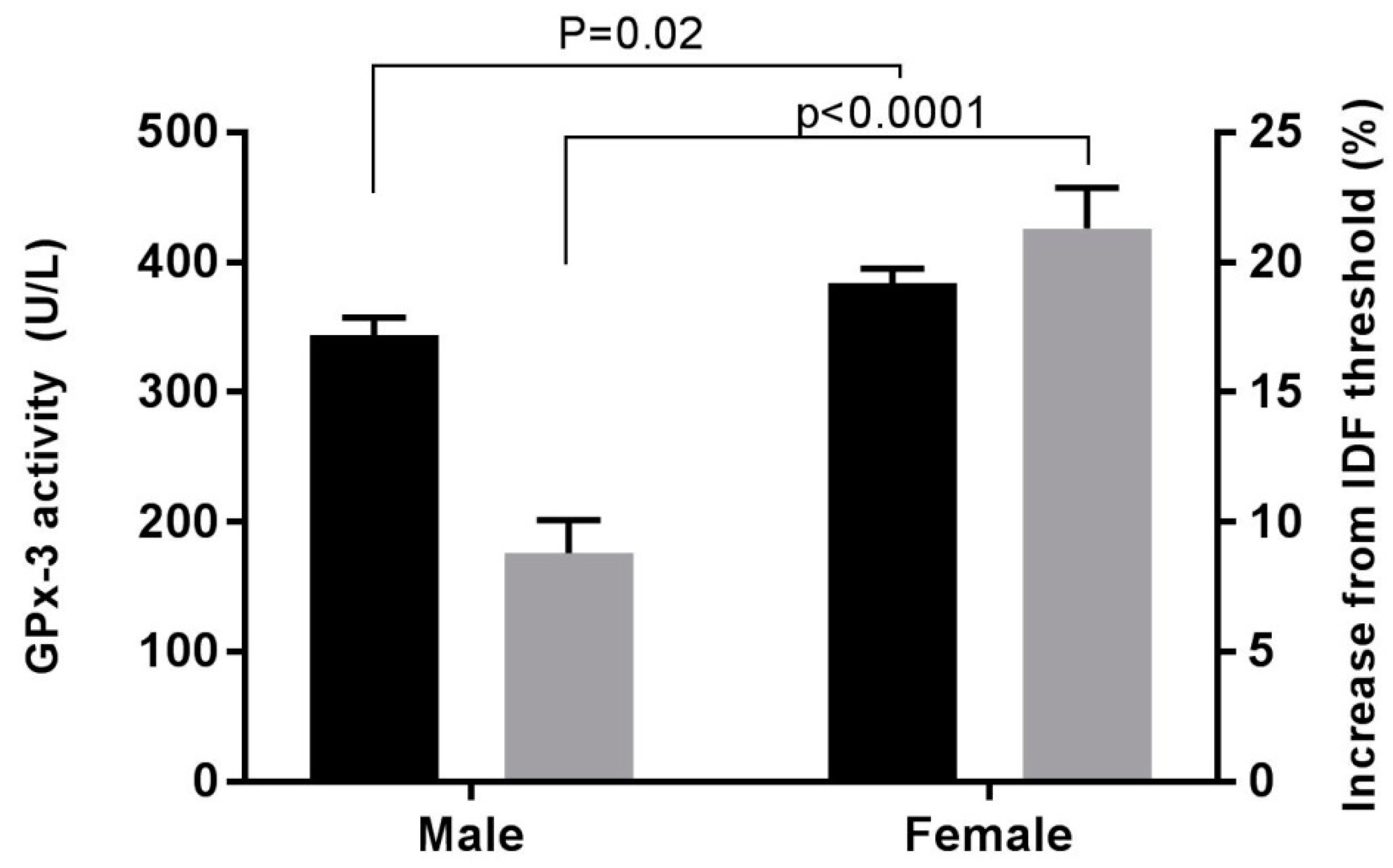
| Increase in waist circumference from IDF recommended threshold (%) | 8.9 ± 11.7 | 21.3 ± 14.1 | <0.0001 |
| Plasma Antioxidants | Male | Female | p |
|---|---|---|---|
| Vitamin E:Total-Cholesterol (µmol/mmol) | 8.95 ± 3.03 | 8.79 ± 2.54 | 0.72 |
| Selenium (µmol/L) | 1.25 ± 0.28 | 1.26 ± 0.24 | 0.73 |
| GPx-3 activity (U/L) | 343.3 ± 128.0 | 384.1 ± 99.7 | 0.02 |
| Variables | β | t | p | |
|---|---|---|---|---|
| Model A | Sex | 41.0 | 2.28 | 0.02 |
| Waist circumference | −1.48 | −2.13 | 0.04 | |
| Model B | Sex | 58.0 | 2.53 | 0.01 |
| Bioimpedance | −1.48 | −1.26 | 0.21 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steyn, M.; Zitouni, K.; Kelly, F.J.; Cook, P.; Earle, K.A. Sex Differences in Glutathione Peroxidase Activity and Central Obesity in Patients with Type 2 Diabetes at High Risk of Cardio-Renal Disease. Antioxidants 2019, 8, 629. https://doi.org/10.3390/antiox8120629
Steyn M, Zitouni K, Kelly FJ, Cook P, Earle KA. Sex Differences in Glutathione Peroxidase Activity and Central Obesity in Patients with Type 2 Diabetes at High Risk of Cardio-Renal Disease. Antioxidants. 2019; 8(12):629. https://doi.org/10.3390/antiox8120629
Chicago/Turabian StyleSteyn, Mia, Karima Zitouni, Frank J Kelly, Paul Cook, and Kenneth A Earle. 2019. "Sex Differences in Glutathione Peroxidase Activity and Central Obesity in Patients with Type 2 Diabetes at High Risk of Cardio-Renal Disease" Antioxidants 8, no. 12: 629. https://doi.org/10.3390/antiox8120629
APA StyleSteyn, M., Zitouni, K., Kelly, F. J., Cook, P., & Earle, K. A. (2019). Sex Differences in Glutathione Peroxidase Activity and Central Obesity in Patients with Type 2 Diabetes at High Risk of Cardio-Renal Disease. Antioxidants, 8(12), 629. https://doi.org/10.3390/antiox8120629