
Obesity and Skin Carotenoid Score in Children from Center–Southern Italian Regions

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Anthropometric Parameters
2.3. Adherence to the Mediterranean Diet Using the KIDMED Questionnaire
2.4. Measurement of Skin Carotenoid Content
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
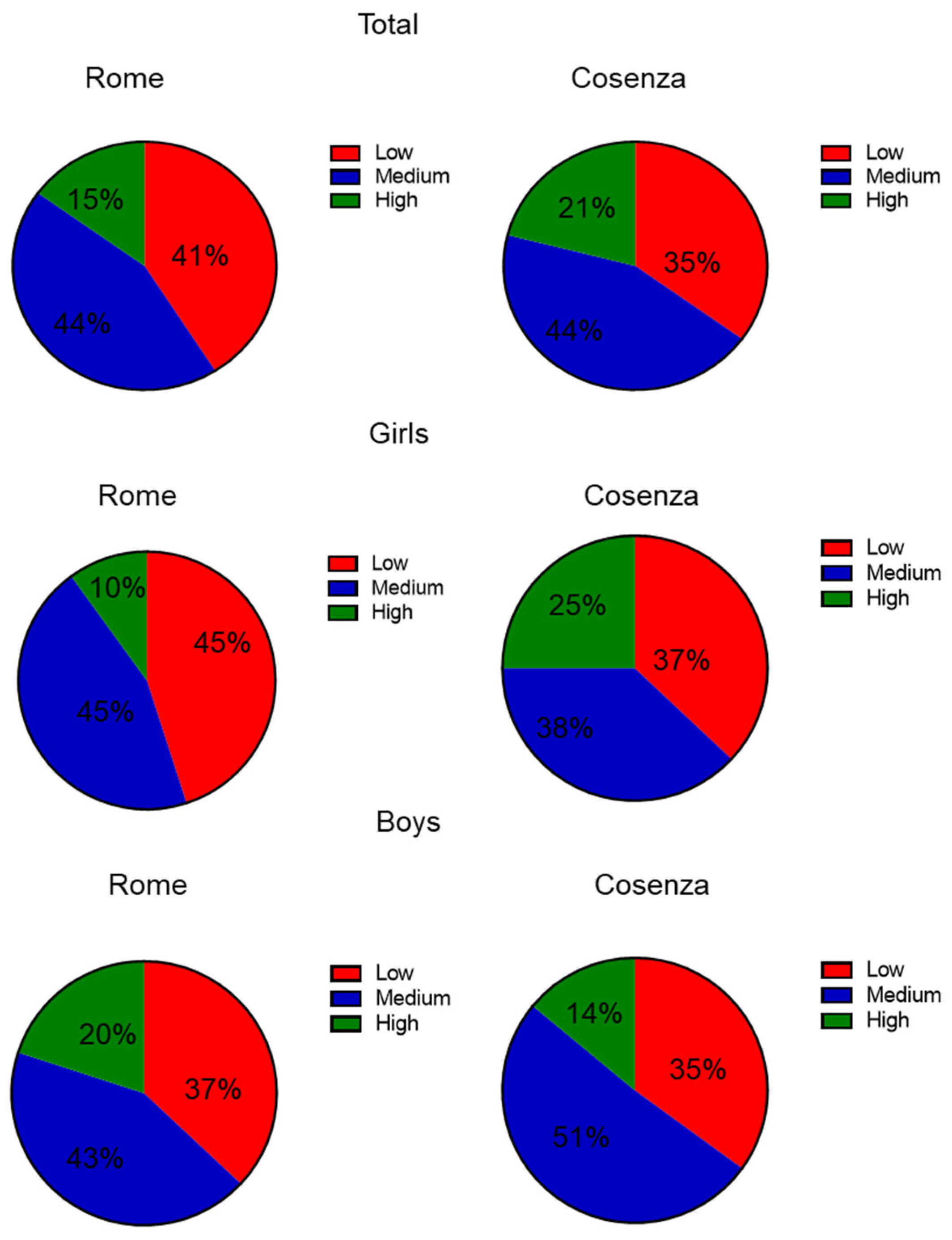
3.2. Adherence to the Mediterranean Diet in the Sample Population
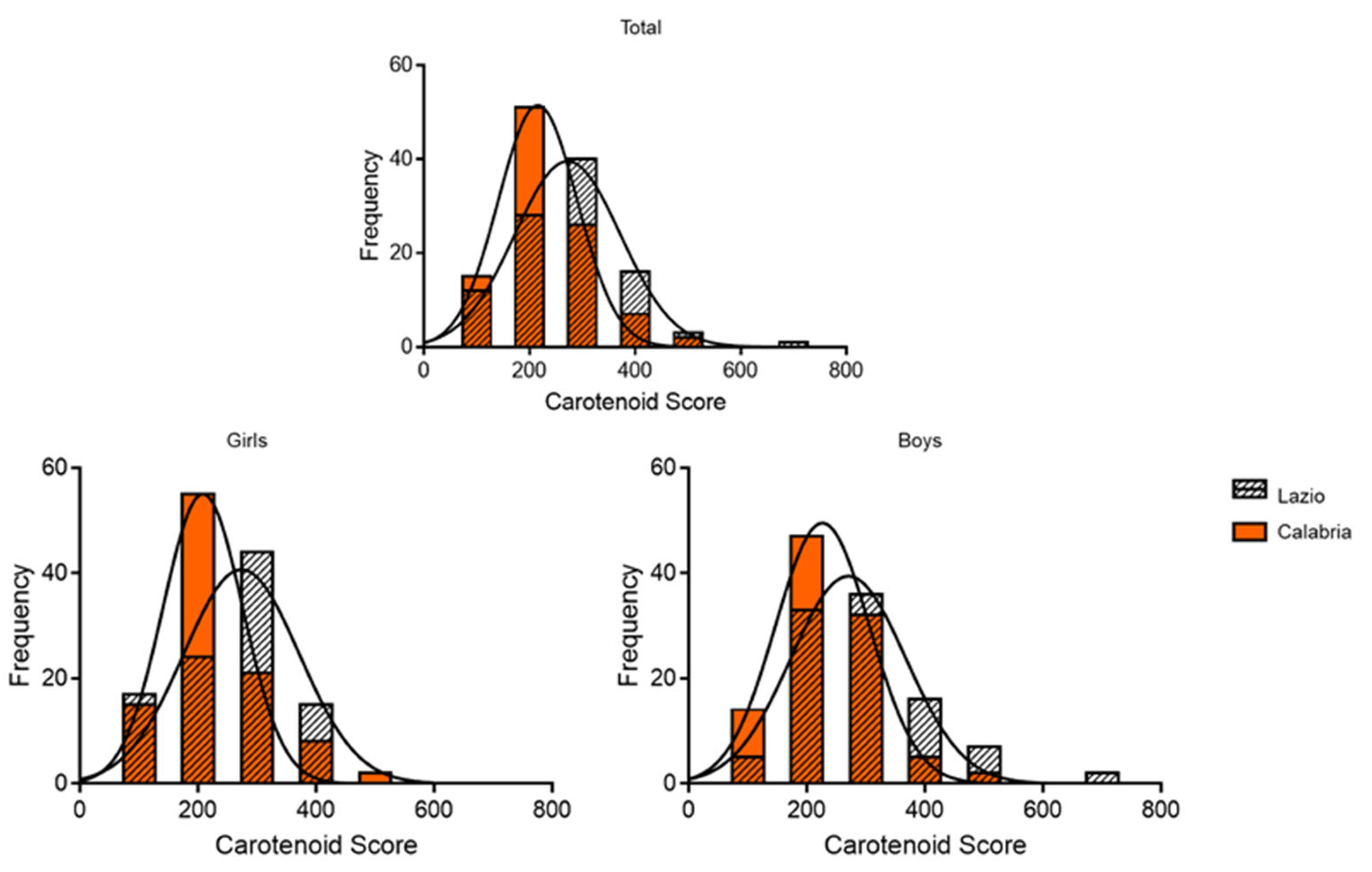
3.3. Carotenoid Score in the Sample Population
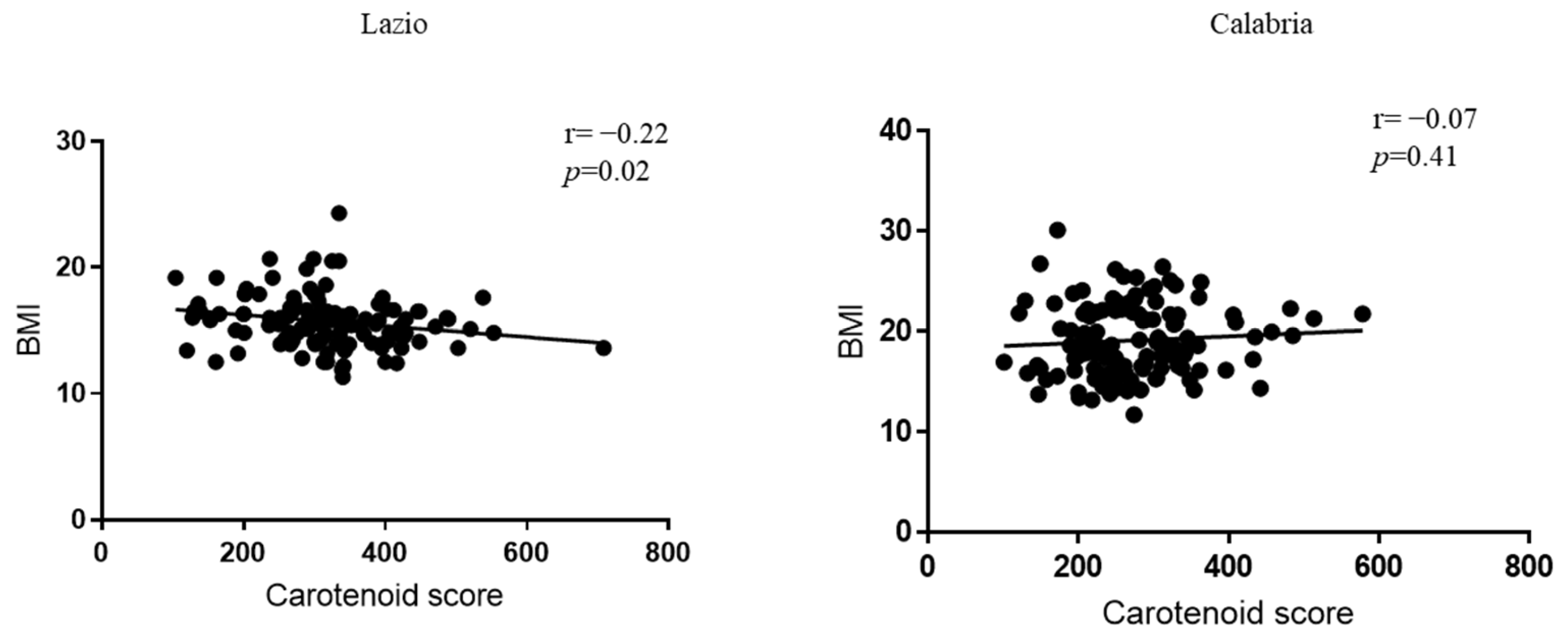
3.4. Correlation Between Carotenoid Score and Different Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| FV | Fruits and Vegetables |
| MD | Mediterranean Diet |
| NCDs | Non-Communicable Diseases |
References
- Available online: https://www.who.int/europe/initiatives/who-european-childhood-obesity-surveillance-initiative-(cosi) (accessed on 12 December 2024).
- Available online: https://www.epicentro.iss.it/okkioallasalute/ (accessed on 12 December 2024).
- Roblin, L. Childhood obesity: Food, nutrient, and eating-habit trends and influences. Appl. Physiol. Nutr. Metab. 2007, 32, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Kuzbicka, K.; Rachon, D. Bad eating habits as the main cause of obesity among children. Pediatr. Endocrinol. Diabetes Metab. 2013, 19, 106–110. [Google Scholar] [PubMed]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Muller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef]
- Ruel, G.; Shi, Z.; Zhen, S.; Zuo, H.; Kroger, E.; Sirois, C.; Levesque, J.F.; Taylor, A.W. Association between nutrition and the evolution of multimorbidity: The importance of fruits and vegetables and whole grain products. Clin. Nutr. 2014, 33, 513–520. [Google Scholar] [CrossRef]
- Wallace, T.C.; Bailey, R.L.; Blumberg, J.B.; Burton-Freeman, B.; Chen, C.O.; Crowe-White, K.M.; Drewnowski, A.; Hooshmand, S.; Johnson, E.; Lewis, R.; et al. Fruits, vegetables, and health: A comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake. Crit. Rev. Food Sci. Nutr. 2020, 60, 2174–2211. [Google Scholar] [CrossRef]
- Folkvord, F.; Naderer, B.; Coates, A.; Boyland, E. Promoting Fruit and Vegetable Consumption for Childhood Obesity Prevention. Nutrients 2021, 14, 157. [Google Scholar] [CrossRef]
- Smith, L.; Lopez Sanchez, G.F.; Veronese, N.; Soysal, P.; Oh, H.; Barnett, Y.; Keyes, H.; Butler, L.; Allen, P.; Kostev, K.; et al. Fruit and Vegetable Intake and Non-Communicable Diseases among Adults Aged >/=50 Years in Low- and Middle-Income Countries. J. Nutr. Health Aging 2022, 26, 1003–1009. [Google Scholar] [CrossRef]
- Library of Evidence for Nutrition Actions (eLENA). Available online: https://www.who.int/tools/elena/interventions/ (accessed on 5 February 2025).
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef]
- Marti, R.; Rosello, S.; Cebolla-Cornejo, J. Tomato as a Source of Carotenoids and Polyphenols Targeted to Cancer Prevention. Cancers 2016, 8, 58. [Google Scholar] [CrossRef]
- Koklesova, L.; Liskova, A.; Samec, M.; Buhrmann, C.; Samuel, S.M.; Varghese, E.; Ashrafizadeh, M.; Najafi, M.; Shakibaei, M.; Busselberg, D.; et al. Carotenoids in Cancer Apoptosis-The Road from Bench to Bedside and Back. Cancers 2020, 12, 2425. [Google Scholar] [CrossRef] [PubMed]
- Di Mascio, P.; Kaiser, S.; Sies, H. Lycopene as the most efficient biological carotenoid singlet oxygen quencher. Arch. Biochem. Biophys. 1989, 274, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Stahl, W.; Sies, H. Antioxidant activity of carotenoids. Mol. Asp. Med. 2003, 24, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.H. Mechanisms involved in the intestinal absorption of dietary vitamin A and provitamin A carotenoids. Biochim. Biophys. Acta 2012, 1821, 70–77. [Google Scholar] [CrossRef]
- Rodriguez-Concepcion, M.; Avalos, J.; Bonet, M.L.; Boronat, A.; Gomez-Gomez, L.; Hornero-Mendez, D.; Limon, M.C.; Meléndez-Martínez, A.J.; Olmedilla-Alonso, B.; Palou, A.; et al. A global perspective on carotenoids: Metabolism, biotechnology, and benefits for nutrition and health. Prog. Lipid Res. 2018, 70, 62–93. [Google Scholar] [CrossRef]
- Meléndez-Martínez, A.J. An Overview of Carotenoids, Apocarotenoids, and Vitamin A in Agro-Food, Nutrition, Health, and Disease. Mol. Nutr. Food Res. 2019, 63, e1801045. [Google Scholar] [CrossRef]
- Longevity Link Corporation. The Veggie Meter®: Non-Invasive Optical Biomarker for Personal Health. Available online: http://www.longevitylinkcorporation.com (accessed on 5 February 2025).
- Caparello, G.; Ceraudo, F.; Meringolo, F.; Augimeri, G.; Morino, G.; Bonofiglio, D. Eating habits and carotenoid skin content among children based on their attendance at the school meals: A cross-sectional pilot study. J. Clin. Transl. Endocrinol. 2024, 38, 100378. [Google Scholar] [CrossRef]
- Morelli, C.; Avolio, E.; Galluccio, A.; Caparello, G.; Manes, E.; Ferraro, S.; De Rose, D.; Santoro, M.; Barone, I.; Catalano, S.; et al. Impact of Vigorous-Intensity Physical Activity on Body Composition Parameters, Lipid Profile Markers, and Irisin Levels in Adolescents: A Cross-Sectional Study. Nutrients 2020, 12, 742. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; Garcia, A.; Perez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Kim, J.; Lim, H. Nutritional Management in Childhood Obesity. J. Obes. Metab. Syndr. 2019, 28, 225–235. [Google Scholar] [CrossRef]
- Liberali, R.; Kupek, E.; Assis, M.A.A. Dietary Patterns and Childhood Obesity Risk: A Systematic Review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Lassale, C.; Fito, M.; Morales-Suarez-Varela, M.; Moya, A.; Gomez, S.F.; Schroder, H. Mediterranean diet and adiposity in children and adolescents: A systematic review. Obes. Rev. 2022, 23 (Suppl. S1), e13381. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.R.; Oliveira, A. Dietary Interventions to Prevent Childhood Obesity: A Literature Review. Nutrients 2021, 13, 3447. [Google Scholar] [CrossRef] [PubMed]
- Acito, M.; Valentino, R.; Rondini, T.; Fatigoni, C.; Moretti, M.; Villarini, M. Mediterranean Diet Adherence in Italian Children: How much do Demographic Factors and Socio-Economic Status Matter? Matern. Child Health J. 2024, 28, 1861–1869. [Google Scholar] [CrossRef]
- Cardamone, E.; Di Benedetto, R.; Lorenzoni, G.; Gallipoli, S.; Ghidina, M.; Zobec, F.; Iacoponi, F.; Gregori, D.; Silano, M. Adherence to Mediterranean diet in Italy (ARIANNA) cross-sectional survey: Study protocol. BMJ Open 2023, 13, e067534. [Google Scholar] [CrossRef]
- Garcia-Conesa, M.T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef]
- Caparello, G.; Galluccio, A.; Giordano, C.; Lofaro, D.; Barone, I.; Morelli, C.; Sisci, D.; Catalano, S.; Ando, S.; Bonofiglio, D. Adherence to the Mediterranean diet pattern among university staff: A cross-sectional web-based epidemiological study in Southern Italy. Int. J. Food Sci. Nutr. 2020, 71, 581–592. [Google Scholar] [CrossRef]
- Augimeri, G.; Soto, M.; Ceraudo, F.; Caparello, G.; Villegas Figueroa, M.; Cesario, M.; Caputi, L.S.; Calderon, B.; Bonofiglio, D. Differences of skin carotenoids and adherence to the Mediterranean Diet pattern in adults from Southern Italy and Dominican Republic. J. Transl. Med. 2024, 22, 424. [Google Scholar] [CrossRef]
- Nardone, P.; Ciardullo, S.; Mandolini, D.; Salvatore, M.A.; Spinelli, A. Lo Stato Ponderale dei Bambini e delle Bambine OKkio alla SALUTE: Rilevazione Dati 2023. Centro Nazionale di Prevenzione delle Malattie e Promozione della Salute, Istituto Superiore di Sanità, 10 May 2024 Roma, Italy. Available online: https://www.epicentro.iss.it/okkioallasalute/pdf2024/convegno-2024/Conv.10-Mag%2010.40%20-%20Lo%20stato%20ponderale%20dei%20bambini%20e%20delle%20bambine%20-%20Nardone%20Ciardullo.pdf (accessed on 5 February 2025).
- Jakobsen, D.D.; Brader, L.; Bruun, J.M. Association between Food, Beverages and Overweight/Obesity in Children and Adolescents-A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2023, 15, 764. [Google Scholar] [CrossRef]
- World Health Organization. Increasing Fruit and Vegetable Consumption to Reduce the Risk of Noncommunicable Diseases. Available online: https://www.who.int/tools/elena/interventions/fruit-vegetables-ncds (accessed on 5 February 2025).
- Spinelli, A.; Mandolini, D.; Salvatore, M.A. Gli stili di vita dei bambini e delle bambine. In Proceedings of the Stato Ponderale e Stili di Vita di Bambine e Bambini: I Dati Italiani della Sorveglianza “OKkio alla SALUTE 2023” e il Contributo dello Studio EPaS-ISS, Rome, Italy, 10 May 2024; Istituto Superiore di Sanità: Roma, Italy, 2024. [Google Scholar]
- Martinelli, S.; Acciai, F.; Tasevska, N.; Ohri-Vachaspati, P. Using the Veggie Meter in Elementary Schools to Objectively Measure Fruit and Vegetable Intake: A Pilot Study. Methods Protoc. 2021, 4, 33. [Google Scholar] [CrossRef]
- Augimeri, G.; Soto, M.; Ceraudo, F.; Caparello, G.; Villegas Figueroa, M.; Cesario, M.; Caputi, L.S.; Calderon, B.; Bonofiglio, D. Comparing the Dietary Habits and the Food Choices Between Italian and Dominican Adult Populations: Focus on Fruit and Vegetable Intakes and Their Association with Skin Carotenoid Levels. Foods 2024, 13, 3323. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.S. Carotenoids in Human Blood and Tissues. J. Nutr. 1989, 119, 101–104. [Google Scholar] [CrossRef]
- Kaplan, L.A.; Lau, J.M.; Stein, E.A. Carotenoid composition, concentrations, and relationships in various human organs. Clin. Physiol. Biochem. 1990, 8, 1–10. [Google Scholar] [PubMed]
- Madore, M.P.; Hwang, J.E.; Park, J.Y.; Ahn, S.; Joung, H.; Chun, O.K. A Narrative Review of Factors Associated with Skin Carotenoid Levels. Nutrients 2023, 15, 2156. [Google Scholar] [CrossRef] [PubMed]
- Seguin-Fowler, R.A.; Hanson, K.L.; Marshall, G.A.; Belarmino, E.H.; Jilcott Pitts, S.B.; Kolodinsky, J.; Sitaker, M.; Ammerman, A. Fruit and Vegetable Intake Assessed by Repeat 24 h Recalls, but Not by A Dietary Screener, Is Associated with Skin Carotenoid Measurements in Children. Nutrients 2021, 13, 980. [Google Scholar] [CrossRef]
- Fiedor, J.; Burda, K. Potential role of carotenoids as antioxidants in human health and disease. Nutrients 2014, 6, 466–488. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Lazio | Calabria | p-Value |
| Subjects (n) | 121 | 124 | |
| Girls (n, %) | 66, 54.54 | 66, 53.66 | |
| Boys (n, %) | 55, 45.45 | 58, 46.34 | |
| Weight (kg) | |||
| Total (Mean ± SD) | 26.2 ± 5.92 | 36.24 ± 9.49 | <0.0001 |
| Girls (Mean ± SD) | 26.06± 6.24 | 36.01 ± 9.05 | <0.0001 |
| Boys (Mean ± SD) | 26.37 ± 5.55 | 36.5 ± 10.03 | <0.0001 |
| Height (cm) | |||
| Total (Mean ± SD) | 128.3 ± 9.06 | 136.9 ± 9.14 | <0.0001 |
| Girls (Mean ± SD) | 127.9 ± 9.46 | 136.9 ± 9.13 | <0.0001 |
| Boys (Mean ± SD) | 128.8 ± 8.62 | 136.9 ± 9.14 | 0.0004 |
| BMI (kg/m2) | |||
| Total (Mean ± SD) | 15.77 ± 2.02 | 19.14 ± 3.61 | <0.0001 |
| Girls (Mean ± SD) | 15.75 ± 2.03 | 19.13 ± 3.73 | <0.0001 |
| Boys (Mean ± SD) | 15.79 ± 2.04 | 19.17 ± 3.51 | <0.0001 |
| BMI Z-score | |||
| Total (Mean ± SD) | −0.23 ± 1.06 | 0.98 ± 1.26 | <0.0001 |
| Girls (Mean ± SD) | −0.21 ± 1.09 | 0.89 ± 1.37 | <0.0001 |
| Boys (Mean ± SD) | −0.24 ± 1.02 | 1.05 ± 1.16 | <0.0001 |
| Lazio | Calabria | p-Value | |
|---|---|---|---|
| BMI | |||
| Total | <0.0001 | ||
| Underweight–normal weight (%) | 88 | 48 | |
| Overweight (%) | 9 | 31 | |
| Obese (%) | 3 | 21 | |
| Girls | <0.0001 | ||
| Underweight–normal weight (%) | 85 | 50 | |
| Overweight (%) | 12 | 31 | |
| Obese (%) | 3 | 19 | |
| Boys | <0.0001 | ||
| Underweight–normal weight (%) | 91 | 46 | |
| Overweight (%) | 7 | 32 | |
| Obese (%) | 2 | 22 | |
| BMI Z-score | |||
| Total | <0.0001 | ||
| Underweight–normal weight (%) | 88 | 40 | |
| Overweight (%) | 11 | 30 | |
| Obese (%) | 1 | 30 | |
| Girls | <0.0001 | ||
| Underweight–normal weight (%) | 86 | 42 | |
| Overweight (%) | 14 | 29 | |
| Obese (%) | 0 | 29 | |
| Boys | <0.0001 | ||
| Underweight–normal weight (%) | 90 | 38 | |
| Overweight (%) | 8 | 31 | |
| Obese (%) | 2 | 31 |
| Total (Mean ± SD, n) | Girls (Mean ± SD, n) | Boys (Mean ± SD, n) | p-Value | |
|---|---|---|---|---|
| Lazio | 5.07 ± 2.25, 59 | 4.724 ± 2.186, 29 | 5.4 ± 2.298, 30 | 0.25 |
| Calabria | 5.47 ± 2.46, 121 | 5.515 ± 2.445, 65 | 5 ± 2.784, 56 | 0.27 |
| p-Value | 0.22 | 0.14 | 0.50 |
| Items | Lazio | Calabria | p-Value | ||
|---|---|---|---|---|---|
| % Inside | % Outside | % Inside | % Outside | ||
| Takes a fruit every day | 90 | 10 | 80 | 20 | 0.047 |
| Has a second fruit every day | 53 | 47 | 58 | 42 | |
| Has fresh or cooked vegetables regularly once per day | 80 | 20 | 76 | 24 | |
| Has fresh or cooked vegetables more than once per day | 49 | 51 | 44 | 56 | |
| Consumes fish regularly (at least 2–3 times per week) | 58 | 42 | 49 | 51 | |
| Likes pulses and eats them more than once per week | 64 | 36 | 79 | 21 | 0.02 |
| Consumes whole-grain pasta or whole-grain rice almost every day (5 or more times per week) | 95 | 5 | 63 | 37 | <0.0001 |
| Has whole cereals or whole-grains (whole-meal bread, etc.) for breakfast | 86 | 14 | 47 | 53 | <0.0001 |
| Consumes nuts regularly (at least 2–3 times per week) | 27 | 73 | 48 | 52 | 0.003 |
| Uses olive oil at home | 98 | 2 | 89 | 11 | 0.003 |
| Has a dairy product for breakfast (yoghurt, milk, etc.) | 59 | 41 | 79 | 21 | 0.002 |
| Takes two yogurts and/or some cheese (40 g) daily | 22 | 78 | 64 | 36 | <0.0001 |
| Has commercially baked goods or pastries for breakfast | 58 | 42 | 35 | 65 | 0.001 |
| Goes to a fast-food (hamburger) restaurant more than once per week | 20 | 80 | 67 | 33 | <0.0001 |
| Has breakfast | 20 | 80 | 17 | 83 | |
| Takes sweets and candy several times every day | 29 | 71 | 53 | 47 | <0.0006 |
| Lazio (Mean ± SD) | Calabria (Mean ± SD) | p-Value | |
|---|---|---|---|
| Total | 315.3 ± 101.5 | 273.6 ± 83.03 | 0.0005 |
| Girls | 297.5 ± 94.2 | 269.3 ± 90.72 | 0.08 |
| Boys | 336.6 ± 106.6 | 278 ± 74.44 | 0.001 |
| p-Value | 0.03 | 0.56 |
| Lazio (Mean ± SD, n) | Calabria (Mean ± SD, n) | p-Value | |
|---|---|---|---|
| Item #1 | |||
| <2 servings/day | 266.1 ± 110.3, 28 | 252.7 ± 62.48, 51 | 0.49 |
| >2 servings/day | 323.8 ± 75.14, 31 | 289.2 ± 93.39, 69 | 0.07 |
| p-Value | 0.02 | 0.02 | |
| Item #2 | |||
| <2 servings/day | 297 ± 116.5, 31 | 268.8 ± 84.3, 69 | 0.17 |
| >2 servings/day | 299.6 ± 73.53, 29 | 280.4 ± 82.47, 51 | 0.30 |
| p-Value | 0.92 | 0.45 |
| β (95% CI) | SE | p-Value | |
|---|---|---|---|
| Gender [F] | −23.15 (−48.56; −2.27) | 12.88 | 0.07 |
| BMI | −0.73 (−4.78; 3.33) | 2.05 | 0.72 |
| >2 servings of fruit/day (>2 = 1) | 41.25 (14.56; 67.94) | 13.52 | 0.003 |
| >2 servings of vegetable/day (>2 = 1) | −1.62 (−27.55; 24.32) | 13.14 | 0.90 |
| Italian Region (Lazio = 1) | 23.19 (−6.66; 53.04) | 15.12 | 0.13 |
| Adj.R2 | 0.07 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augimeri, G.; Caparello, G.; Ceraudo, F.; Meringolo, F.; Mazzitelli, L.; Iovino, M.V.; Morino, G.; Bonofiglio, D. Obesity and Skin Carotenoid Score in Children from Center–Southern Italian Regions. Antioxidants 2025, 14, 448. https://doi.org/10.3390/antiox14040448
Augimeri G, Caparello G, Ceraudo F, Meringolo F, Mazzitelli L, Iovino MV, Morino G, Bonofiglio D. Obesity and Skin Carotenoid Score in Children from Center–Southern Italian Regions. Antioxidants. 2025; 14(4):448. https://doi.org/10.3390/antiox14040448
Chicago/Turabian StyleAugimeri, Giuseppina, Giovanna Caparello, Fabrizio Ceraudo, Francesca Meringolo, Ludovica Mazzitelli, Maria Vittoria Iovino, Giuseppe Morino, and Daniela Bonofiglio. 2025. "Obesity and Skin Carotenoid Score in Children from Center–Southern Italian Regions" Antioxidants 14, no. 4: 448. https://doi.org/10.3390/antiox14040448
APA StyleAugimeri, G., Caparello, G., Ceraudo, F., Meringolo, F., Mazzitelli, L., Iovino, M. V., Morino, G., & Bonofiglio, D. (2025). Obesity and Skin Carotenoid Score in Children from Center–Southern Italian Regions. Antioxidants, 14(4), 448. https://doi.org/10.3390/antiox14040448