
Induction of Nitric Oxide and Its Role in Otitis Media



Abstract
1. Introduction
1.1. Otitis Media
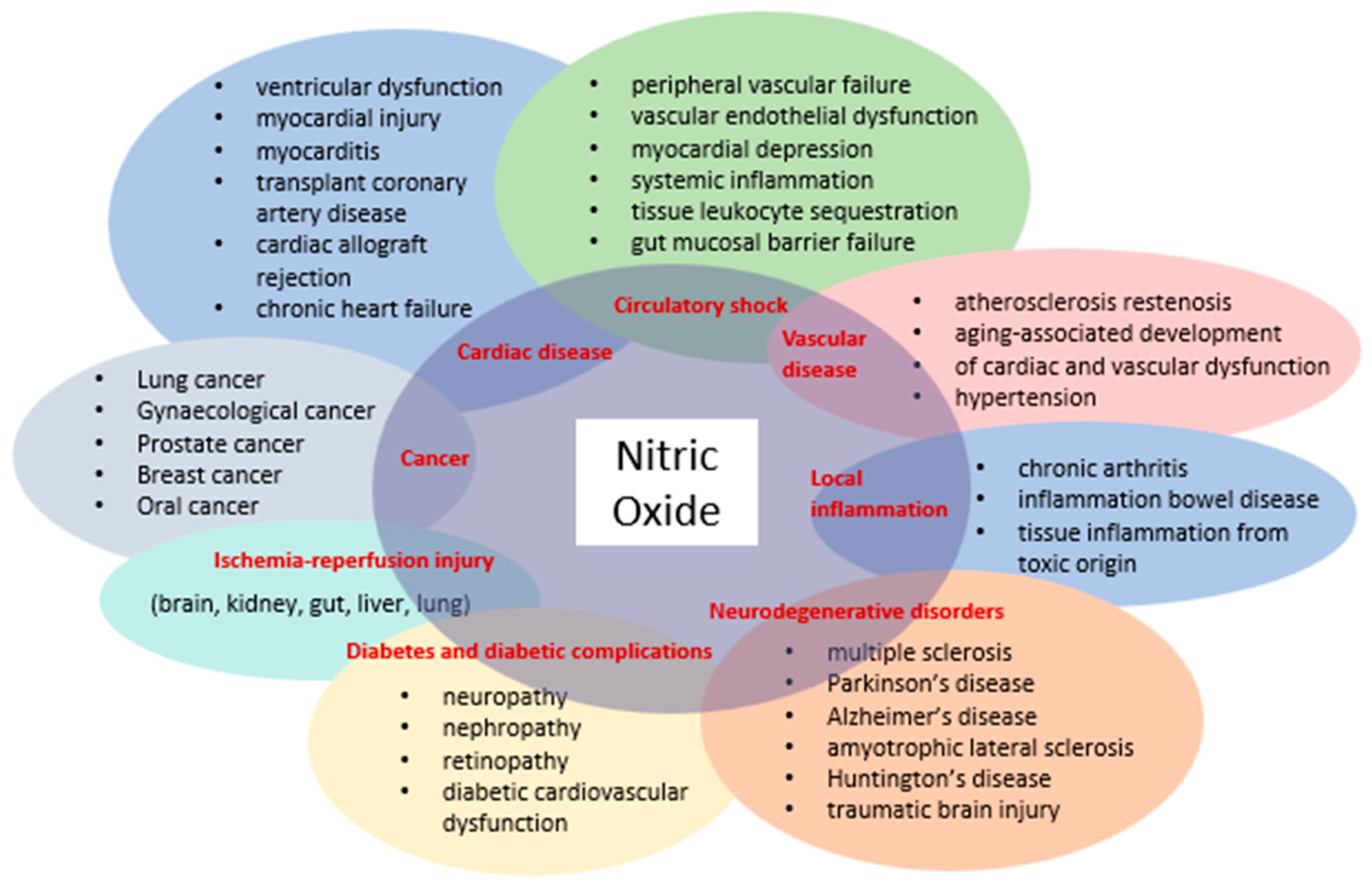
1.2. Nitric Oxide
2. Research Methods
3. Studies on the Role of NO in Otitis Media
3.1. Nitric Oxide (NO)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author [Reference] | Study Design | Species and/or Sample | Types of Otitis Media | Detection Method | Target Gene(s) or Pathway(s) Associated with NOS | Results/Conclusions |
|---|---|---|---|---|---|---|
| Allan et al. (2016) [37] | Biofilm experiment, human study | 11 pediatric patients | Otitis media caused by S. pneumoniae | CLSM, SEM, iTRAQ labeling, mass spectrometry, peak list generation, database searching | NO | Treatment with the NO donor SNP reduced the viability of planktonic cells and decreased the cell population within in vitro biofilms. Adjunctive NO treatment of in vitro pneumococcal biofilms increased the effectiveness of antibiotics. The combination of antibiotics and NO treatment improved the ex vivo eradication of S. pneumoniae on adenoid tissue. These findings imply that at lower concentrations, NO disrupts the metabolism of pneumococcal biofilms, while at higher concentrations, NO becomes toxic to S. pneumoniae. Targeted adjunctive NO treatment could be a promising novel therapy for reducing biofilm tolerance by pneumococci. |
| Granath et al. (2010) [40] | Human study | 12 children with OME and 14 children with adenoid hypertrophy (control) | Otitis media with effusion | Real time PCR, immunohistochemical staining of adenoid tissue | iNOS, eNOS | The children with OME showed lower levels of iNOS compared to the controls without middle ear disease, while no difference was observed for eNOS. These proteins were primarily located in association with the surface epithelium. The local induction of iNOS in adenoids may play a crucial role in preventing the development of OME. |
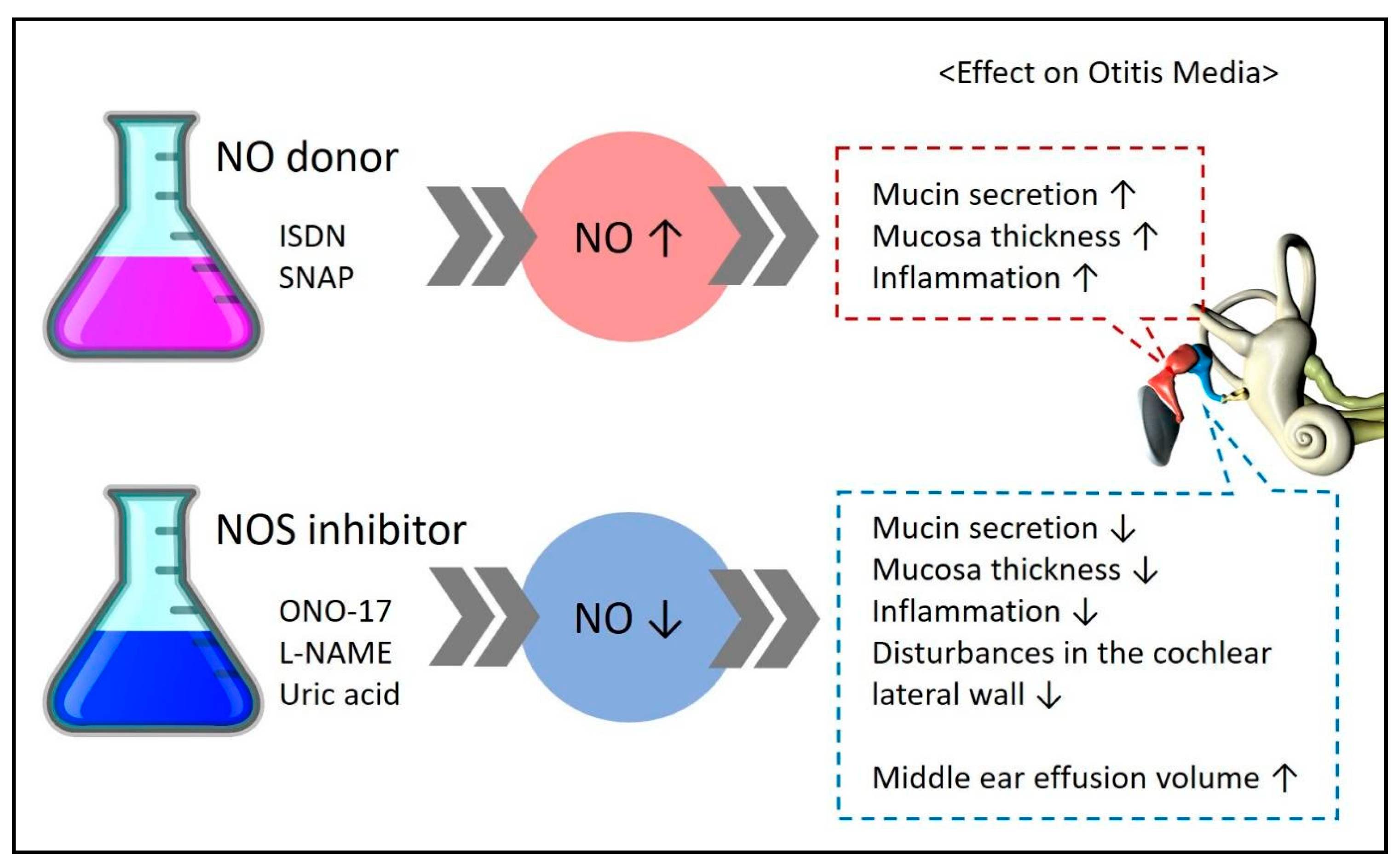
3.2. NO Metabolites and NO Donors
3.3. Nitric Oxide Synthase (NOS)
3.3.1. NOS
3.3.2. iNOS
3.3.3. Polymorphisms
3.3.4. NO and NOS
3.4. NO Stimulants or Inhibitors, NO Metabolites, NO Biomarkers
3.4.1. Steroids
3.4.2. Steroids and Tacrolimus
3.4.3. L-LAA
3.4.4. MDA
3.4.5. LPS and L-NAME
3.4.6. MPO, 4HNE, and L-NAME
3.4.7. NO, MPO, and CAT
3.5. Clinical Implications of NO
3.6. Synthesis of NO in Otitis Media
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yeo, S.G. Acute Otitis Media. In Korean Society of Otorhinolaryngology−Head and Neck Surgery; KoonJa: Seoul, Republic of Korea, 2018; Volume 3, pp. 363–383. [Google Scholar]
- Gates, G.A. Acute Otitis Media and Otitis Media with Effusion. Otolaryngology, Head and Neck Surgery, 3rd ed.; Mosby: St Louis, MO, USA, 1998. [Google Scholar]
- Jang, J.H. Acute Otitis Media. Korean Otol. Soc. 2022, 27, 433–441. [Google Scholar]
- Jang, J.W. Otitis Media with Effusion. Korean Otol. Soc. 2022, 28, 443–460. [Google Scholar]
- Bluestone, C.D.; Klein, J.O. Otitis Media and Eustachian Tube Dysfunction. Pediatr. Otolaryngol. 2003, 4, 474. [Google Scholar]
- Gleeson, M.; Clarke, R. Scott-Brown’s Otorhinolaryngology, Head and Neck Surgery; CRC Press: Boca Raton, FL, USA, 2008; Volume 7. [Google Scholar]
- Park, Y.H. Chronic Otitis Media. Korean Otol. Soc. 2022, 30, 469–480. [Google Scholar]
- Verhoeff, M.; van der Veen, E.L.; Rovers, M.M.; Sanders, E.A.M.; Schilder, A.G.M. Chronic Suppurative Otitis Media: A Review. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1–12. [Google Scholar] [CrossRef]
- Bhutta, M.F.; Thornton, R.B.; Kirkham, L.-A.S.; Kerschner, J.E.; Cheeseman, M.T. Understanding the Aetiology and Resolution of Chronic Otitis Media from Animal and Human Studies. Dis. Model. Mech. 2017, 10, 1289–1300. [Google Scholar] [CrossRef]
- Cho, S.I. Cholesteatomatous Otitis Media. Korean Otol. Soc. 2022, 31, 481–494. [Google Scholar]
- van der Toom, H.F.E.; van der Schroeff, M.P.; Pauw, R.J. Single-Stage Mastoid Obliteration in Cholesteatoma Surgery and Recurrent and Residual Disease Rates: A Systematic Review. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 440–446. [Google Scholar] [CrossRef]
- Jovanovic, I.; Zivkovic, M.; Djuric, T.; Stojkovic, L.; Jesic, S.; Stankovic, A. Perimatrix of Middle Ear Cholesteatoma: A Granulation Tissue with a Specific Transcriptomic Signature. Laryngoscope 2020, 130, E220–E227. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Kim, S.-K. Nitric Oxide and Dental Pulp. J. Korean Acad. Conserv. Dent. 2002, 27, 543. [Google Scholar] [CrossRef]
- Yim, C.Y. Nitric Oxide and Cancer. Korean J. Intern. Med. 2010, 78, 430–436. [Google Scholar]
- Blaise, G.A.; Gauvin, D.; Gangal, M.; Authier, S. Nitric Oxide, Cell Signaling and Cell Death. Toxicology 2005, 208, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Kröncke, K.D.; Fehsel, K.; Kolb-Bachofen, V. Nitric Oxide: Cytotoxicity versus Cytoprotection—How, Why, When, and Where? Nitric Oxide 1997, 1, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Pacher, P.; Beckman, J.S.; Liaudet, L. Nitric Oxide and Peroxynitrite in Health and Disease. Physiol. Rev. 2007, 87, 315–424. [Google Scholar] [CrossRef]
- Oh, Y.J.; Yon, D.K.; Choi, Y.S.; Lee, J.; Yeo, J.H.; Kim, S.S.; Lee, J.M.; Yeo, S.G. Induction of Nitric Oxide and Its Role in Facial Nerve Regeneration According to the Method of Facial Nerve Injury. Antioxidants 2024, 13, 741. [Google Scholar] [CrossRef]
- Fan, W.; Li, X.; Xu, H.; Zhao, L.; Zhao, J.; Li, W. Relationship of T Lymphocytes, Cytokines, Immunoglobulin E and Nitric Oxide with Otitis Media with Effusion in Children and Their Clinical Significances. Rev. Assoc. Med. Bras. 2019, 65, 971–976. [Google Scholar] [CrossRef]
- John, E.O.; Russell, P.T.; Nam, B.H.; Jinn, T.H.; Jung, T.T. Concentration of Nitric Oxide Metabolites in Middle Ear Effusion. Int. J. Pediatr. Otorhinolaryngol. 2001, 60, 55–58. [Google Scholar] [CrossRef]
- Capper, R.; Guo, L.; Pearson, J.P.; Birchall, J.P. Effect of Nitric Oxide Donation on Mucin Production in Vitro. Clin. Otolaryngol. Allied Sci. 2003, 28, 51–54. [Google Scholar] [CrossRef]
- Martin, P.; Choi, D.-J.; Jinn, T.-H.; Cohen, J.G.; John, E.O.; Moorehead, M.T.; Kaura, C.S.; Kaura, S.H.; Jung, T.T. k Effect of Nitric Oxide on Mucin Production in Experimental Otitis Media. Otolaryngol. Head Neck Surg. 2004, 130, 249–254. [Google Scholar] [CrossRef]
- Lee, H.Y.; Chung, J.H.; Lee, S.K.; Byun, J.Y.; Kim, Y.I.; Yeo, S.G. Toll-like Receptors, Cytokines & Nitric Oxide Synthase in Patients with Otitis Media with Effusion. Indian J. Med. Res. 2013, 138, 523–530. [Google Scholar]
- Başoğlu, M.S.; Eren, E.; Aslan, H.; Kolatan, H.E.; Ozbay, C.; Inan, S.; Karaca, F.; Oztürkcan, S.; Katılmış, H. Increased Expression of VEGF, INOS, IL-1β, and IL-17 in a Rabbit Model of Gastric Content-Induced Middle Ear Inflammation. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Long, J.P.; Tong, H.H.; Shannon, P.A.; DeMaria, T.F. Differential Expression of Cytokine Genes and Inducible Nitric Oxide Synthase Induced by Opacity Phenotype Variants of Streptococcus pneumoniae during Acute Otitis Media in the Rat. Infect. Immun. 2003, 71, 5531–5540. [Google Scholar] [CrossRef] [PubMed]
- Forséni, M.; Bagger-Sjöbäck, D.; Hultcrantz, M. A Study of Inflammatory Mediators in the Human Tympanosclerotic Middle Ear. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.; Uslu, C.; Akyuz, M. Nitric Oxide Synthase Activity and Nitric Oxide Level in Erythrocytes of Guinea Pigs with Experimental Otitis Media with Effusion. Cell. Biochem. Funct. 2006, 24, 471–473. [Google Scholar] [CrossRef]
- Sone, M.; Hayashi, H.; Yamamoto, H.; Tominaga, M.; Nakashima, T. A Comparative Study of Intratympanic Steroid and NO Synthase Inhibitor for Treatment of Cochlear Lateral Wall Damage Due to Acute Otitis Media. Eur. J. Pharmacol. 2003, 482, 313–318. [Google Scholar] [CrossRef]
- Pudrith, C.; Martin, D.; Kim, Y.H.; Jahng, P.; Kim, B.; Wall, M.; Jung, T. Glucocorticoids Reduce Nitric Oxide Concentration in Middle Ear Effusion from Lipopolysaccharide Induced Otitis Media. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 384–386. [Google Scholar] [CrossRef]
- Hebda, P.A.; Burckar, G.J.; Alper, C.M.; Swarts, J.D.; Moody-Antonio, S.; Zeevi, A.; Doyle, W.J. Effect of 10 Pharmacologic Probes on MRNA Levels of Inducible Nitric Oxide Synthetase and Selected Inflammatory Cytokines in a Rat Model of Acute Otitis Media. Acta Otolaryngol. 2002, 122, 255–261. [Google Scholar] [CrossRef]
- Karlidağ, T.; Ilhan, N.; Kaygusuz, I.; Keleş, E.; Yalçin, S. Comparison of Free Radicals and Antioxidant Enzymes in Chronic Otitis Media with and without Tympanosclerosis. Laryngoscope 2004, 114, 85–89. [Google Scholar] [CrossRef]
- Rose, A.S.; Prazma, J.; Randell, S.H.; Baggett, H.C.; Lane, A.P.; Pillsbury, H.C. Nitric Oxide Mediates Mucin Secretion in Endotoxin-Induced Otitis Media with Effusion. Otolaryngol. Head Neck Surg. 1997, 116, 308–316. [Google Scholar] [CrossRef]
- Jeon, E.; Park, Y.-S.; Lee, S.K.; Yeo, S.-W.; Park, S.N.; Chang, K.-H. Effect of Nitric Oxide and Peroxynitrite on Mucociliary Transport Function of Experimental Otitis Media. Otolaryngol. Head Neck Surg. 2006, 134, 126–131. [Google Scholar] [CrossRef]
- Garça, M.F.; Aslan, M.; Tuna, B.; Kozan, A.; Cankaya, H. Serum Myeloperoxidase Activity, Total Antioxidant Capacity and Nitric Oxide Levels in Patients with Chronic Otitis Media. J. Membr. Biol. 2013, 246, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Sagiroglu, S.; Ates, S.; Tolun, F.; Oztarakci, H. Evaluation of Oxidative Stress and Antioxidants Effect on Turning Process Acute Otitis Media to Chronic Otitis Media with Effusion. Niger. J. Clin. Pr. 2019, 22, 375. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.H.; Chen, Y.; Liu, X.; DeMaria, T.F. Differential expression of cytokine genes and iNOS induced by nonviable nontypeable Haemophilus influenzae or its LOS mutants during acute otitis media in the rat. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Allan, R.N.; Morgan, S.; Brito-Mutunayagam, S.; Skipp, P.; Feelisch, M.; Hayes, S.M.; Hellier, W.; Clarke, S.C.; Stoodley, P.; Burgess, A.; et al. Low Concentrations of Nitric Oxide Modulate Streptococcus Pneumoniae Biofilm Metabolism and Antibiotic Tolerance. Antimicrob. Agents Chemother. 2016, 60, 2456–2466. [Google Scholar] [CrossRef]
- Yuan, M.; Sun, T.; Wu, J.; Fei, Y.; Yang, Y.; Ling, Y.; Zhang, Y.; Huang, Z. The Insights and Perspectives of Nitric Oxide-mediated Biofilm Eradication. Curr. Top. Med. Chem. 2021, 21, 2213–2229. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tang, J. Fe-based Fenton-like catalysts for water treatment: Catalytic mechanisms and applications. J. Mol. Liq. 2021, 332, 115755. [Google Scholar]
- Granath, A.; Norrby-Teglund, A.; Uddman, R.; Cardell, L.-O. Reduced INOS Expression in Adenoids from Children with Otitis Media with Effusion. Pediatr. Allergy Immunol. 2010, 21, 1151–1156. [Google Scholar] [CrossRef]
- Winterbourn, C.C. Toxicity of iron and hydrogen peroxide: The Fenton reaction. Toxicol. Lett. 1995, 82–83, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Aktan, B.; Taysi, S.; Gümüştekin, K.; Uçüncü, H.; Memişoğullari, R.; Save, K.; Bakan, N. Effect of Macrolide Antibiotics on Nitric Oxide Synthase and Xanthine Oxidase Activities, and Malondialdehyde Level in Erythrocyte of the Guinea Pigs with Experimental Otitis Media with Effusion. Pol. J. Pharmacol. 2003, 55, 1105–1110. [Google Scholar]
- Ates, M.; Cevik, C.; Dokuyucu, R.; Berber, O.; Colak, S.; Izmirli, M. The Endothelial Nitric Oxide Synthase (ENOS) Polymorphism in Otitis Media with Effusion (OME). Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2017, 134, 3–5. [Google Scholar] [CrossRef]
- Ryan, A.F.; Bennett, T. Nitric Oxide Contributes to Control of Effusion in Experimental Otitis Media. Laryngoscope 2001, 111, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Wand, Z.; Jin, A.; Yang, Z.; Huang, W. Advanced Nitric Oxide Generating Nanomedicine for Therapeutic Applications. ACS Nano 2023, 17, 8935–8965. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ignarro, L.J. Nitric Oxide: Biology and Pathobiology; Academic Press: Cambridge, MA, USA, 2000. [Google Scholar]
- Hou, J.; Pan, Y.; Zhu, D.; Fan, Y.; Feng, G.; Wei, Y.; Wang, H.; Qin, K.; Zhao, T.; Yang, Q.; et al. Targeted delivery of nitric oxide via a ‘bump-and-hole’-based enzyme-prodrug pair. Nat. Chem. Biol. 2019, 15, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Lerner, E. Nitric oxide inhibition strategies. Future Sci. OA 2015, 1, FSO35. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, X.M.; Hu, C.P.; Li, Y.J.; Jiang, J.L. Cardiovascular risk in autoimmune disorders: Role of asymmetric dimethylarginine. Eur. J. Pharmacol. 2012, 696, 5–11. [Google Scholar] [CrossRef]
- Baylis, C. NOS derangements and hypertension in kidney disease. Curr. Opin. Nephrol. Hypertens. 2012, 21, 1–6. [Google Scholar] [CrossRef]
- Schwedhelm, E.; Boger, R.H. The role of asymmetric and symmetric dimethylarginines in renal disease. Nat. Rev. Nephrol. 2011, 7, 275–285. [Google Scholar] [CrossRef]
- Avontuur, J.A.; Boomsma, F.; Van Den Meiracker, A.H.; DEJong, F.H.; Bruining, H.A. Endothelin-1 and blood pressure after inhibition of nitric oxide synthesis in human septic shock. Circulation 1999, 99, 271–275. [Google Scholar] [CrossRef]
- Jadeski, L.C.; Hum, K.O.; Chakraborty, C.; Lala, P.K. Nitric oxide promotes murine mammary tumour growth and metastasis by stimulating tumour cell migration, invasiveness and angiogenesis. Int. J. Cancer 2000, 86, 30–39. [Google Scholar] [CrossRef]
- Banach, M.; Piskorska, B.J.; Czuczwar, S.K.; Borowicz, K. Nitric oxide, epileptic seizures, and action of antiepileptic drugs. CNS Neurol. Disord. Drug Targets 2011, 10, 808–819. [Google Scholar] [CrossRef]
- Hoffman, R.A.; Nüssler, N.C.; Gleixner, S.L.; Zhang, G.; Ford, H.R.; Langrehr, J.M.; Demetris, A.J.; Simmons, R.L. Attenuation of lethal graft-versus-host disease by inhibition of, N.O.S. Transplantation 1997, 63, 94–100. [Google Scholar] [CrossRef]


| NOS | NOS Isoform | Alternative Description | Human Chromosome | Molecular Mass (kDa) | Distinctive Properties | Subcellular Localization | Tissue Expression | Features | Primary Site | Main Function |
|---|---|---|---|---|---|---|---|---|---|---|
| NOS-I (nNOS) | Neuronal | Type I nNOS ncNOS bNOS | 12 | 160 | Ca++-dependent, constitutively expressed | Binds to specific proteins via an N-terminal PDZ domain | Neuronal cells Skeletal muscle | Constitutive, Ca++/CaM-dependent | 1. Neuronal tissues 2. Skeletal muscle 3. Lung epithelium | 1. Neurotransmission 2. Relaxation of vascular and non-vascular smooth muscle |
| NOS-II (iNOS) | Inducible | Type II iNOS macNOS | 17 | 130 | Ca++-independent, induced by inflammatory stimuli (cytokines, LPS) | Soluble? | Macrophages Hepatocytes Astrocytes Smooth muscle cells (and many more) | Inducible, Ca++-independent | 1. Astrocytes 2. Chondrocytes 3. Dendritic cells 4. Epithelial cells 5. Fibroblasts 6. Macrophages 7. Osteoclasts 8. Various cancer cells | 1. Cytotoxicity 2. Host defense |
| NOS-III (eNOS) | Endothelial | Type III eNOS ecNOS | 7 | 134 | Ca++-dependent, constitutively expressed | Targets to the Golgi and the caveolae via N-terminal myristoylation and palmitoylation | Endothelial cells Epithelial cells Cardiomyocytes | Constitutive, Ca++/CaM-dependent, membrane-associated | 1. Endothelial cells 2. Cardiac myocytes 3. Hippocampal pyramidal cells | 1. Platelet aggregation 2. Vascular tone maintenance 3. Angiogenesis 4. Corpora cavernosa relaxation 5. Smooth muscle proliferation control |
| Author [Reference] | Study Design | Species and/or Sample | Types of Otitis Media | Detection Method | Target gene(s) or Pathway(s) Associated with NOS | Results/Conclusions |
|---|---|---|---|---|---|---|
| Fan et al. (2019) [19] | Human study | 50 children with OME and 50 controls | Otitis media with effusion | NO levels were determined using ELISA (enzyme-linked immunosorbent assay) | NO | In the observation group, the percentage of NO levels in peripheral blood was significantly greater than that in the control group (p < 0.01). Furthermore, within the observation group, NO levels in the MEE were markedly higher than those found in peripheral blood (p < 0.01). In children with OME, there is an elevation in peripheral blood NO levels. These measurements offer valuable insights for diagnosing OME in pediatric patients. |
| John et al. (2001) [20] | Human study | 55 patients | Otitis media with effusion | Colorimetric assay (Griess method) | NO | In human MEE, the concentrations of NO₂⁻/ NO₃⁻ were found to be highest in cases of mucoid otitis media, followed by serous and then purulent otitis media. Many children who continue to have effusion after acute OM treatment progress to MOM, which is considered the most advanced stage within the OME spectrum. The elevated NO levels observed in MOM further imply that NO might play a role in mediating mucin secretion during the development of MOM. |
| Capper et al. (2003) [21] | Human cell line study | HT-29MTX goblet cells | Otitis media with effusion | Mucin analysis (ELISA assay) | NO | When ISDN, an NO donor, is added to the cell culture medium containing the goblet cell line HT29-MTX, there is an observed increase in the production of human MUC5AC mucin. The peak stimulation is achieved after 1 h of NO donor exposure, resulting in a 30% increase in mucus production compared to baseline levels. Additionally, the increase in mucus production is dose-dependent on the concentration of ISDN. The administration of NO via ISDN leads to an increase in mucus production that is related to both dose and time. This finding further supports an inflammatory model for mucus secretion in OME. |
| Martin et al. (2004) [22] | Animal study | 22 chinchillas | Mucoid otitis media (MOM) | Auditory brainstem response, histopathologic study, mucin analysis (periodic acid–Schiff method) | NO | Mucin levels were significantly elevated in the LPS + SNAP (NO donor) group compared to the group treated with LPS alone. After 96 h, both the LPS and LPS + SNAP groups showed thickened mucosa accompanied by subepithelial edema, focal hemorrhage, and hyperemia. These findings bolster the hypothesis that exogenous NO can enhance mucin production in LPS-induced OM and exacerbate the severity of inflammation in the middle ear mucosa. The study indicates that NO may play a role in the progression of MOM from SOM in the pathogenesis of OM. |
| Lee et al. (2013) [23] | Human study | 96 children with OME | Otitis media with effusion | The level of iNOS mRNA in middle ear effusion was assessed using real-time polymerase chain reaction | iNOS | Overall, the patients who were culture-positive exhibited higher levels of NOS mRNAs compared to those who were culture-negative. However, this difference did not reach statistical significance. NOS plays a cooperative role in the innate immune response and is closely linked to OME. |
| Başoğlu et al. (2011) [24] | Animal study | 16 rabbits | Gastric content-induced middle ear inflammation | Histochemical staining, immunohistochemical staining, H&E staining, light microscopy | iNOS, eNOS | The expression level of iNOS showed a significant difference between the experimental and control groups, whereas the expression level of eNOS did not differ significantly between these groups. This study illustrates that middle ear inflammation induced by gastroesophageal reflux is linked to an increased expression of iNOS. |
| Long et al. (2003) [25] | Animal study | 55 Sprague–Dawley rats | Pneumococcal otitis media | Real-time PCR, ELISA | iNOS | The transparent variant of S. pneumoniae is a stronger inducer of inflammation, leading to the accumulation of more inflammatory cells and significantly higher increases in the expression and production of inflammatory mediators. The opacity variants of S. pneumoniae affect the timing of mRNA expression for inflammatory mediators in the middle ear. |
| Forséni et al. (2001) [26] | Human study | 9 biopsy specimens from children with secretory otitis media, 11 biopsy specimens from patients with chronic otitis media and tympanosclerosis | Secretory otitis media, chronic otitis media | Immunohistochemical technique | iNOS | Biopsy specimens from the children with secretory otitis media exhibited more positive staining for macrophages, B cells, and IL-6 compared to those from patients with chronic otitis media and tympanosclerosis. Conversely, biopsy specimens from the patients with chronic otitis media and tympanosclerosis more frequently showed positive staining for iNOS than those from secretory otitis media. In patients with secretory otitis media, an early phase of the disease, macrophages, B cells, and IL-6 were labeled more frequently. In contrast, iNOS was more frequently observed in patients with tympanosclerosis, indicating a later phase of the disease. |
| Yilmaz et al. (2006) [27] | Animal study | 12 guinea pigs (6 with experimental OME and 6 controls) | Otitis media with effusion | Erythrocyte sediments, NOS activity assay, erythrocyte NO levels measured using the Griess reagent | NOS, NO | In experimental otitis media with effusion, the NOS activity and NO levels were significantly higher compared to the control group. In guinea pigs with experimental OME, erythrocytes exhibit an increased NOS activity and elevated NO levels. These heightened NO levels may significantly contribute to cell and tissue damage associated with experimental otitis media with effusion. |
| Sone et al. (2003) [28] | Animal study | 16 Sprague–Dawley rats | Damage to the cochlear lateral wall induced by endotoxin (lipopolysaccharide)-induced otitis media | Measurement of the cochlear blood flow using a laser Doppler flowmeter, electron microscope examination | NO | ONO-1714, a NOS inhibitor, is significantly more effective than the steroid dexamethasone in combating LPS-induced disorders of the cochlear wall. In rats treated with ONO-1714, cochlear blood flow normalized and increased more following prostaglandin E1 application compared to those treated with PBS. These drugs can help protect the function of the spiral ligament during acute otitis media. The intratympanic administration of a NOS inhibitor proved effective in treating disturbances in the cochlear lateral wall caused by otitis media. |
| Pudrith et al. (2010) [29] | Animal study | 53 chinchillas | Otitis media with effusion | Griess reagent | NO | In an LPS-induced experimental OME model in chinchillas, glucocorticoids reduced NO levels in middle ear effusion. While treatment with glucocorticoids at 0.1% concentrations did not consistently lead to significant reductions in NO, a 1% concentration of glucocorticoids significantly reduced NO concentration by 55.3%. Glucocorticoids have the potential to lower the levels of NO, a potentially ototoxic substance, in middle ear effusion. Nonetheless, further research, including clinical trials, is necessary to ascertain if this effect is applicable in clinical practice. |
| Hebda et al. (2002) [30] | Animal study | 72 Sprague–Dawley rats | Acute otitis media | RT-PCR | iNOS | During AOM, the expression of messages for cytokines and iNOS is downregulated by corticosteroid treatment. In rats with AOM, tacrolimus treatment led to decreased messenger levels for iNOS and the cytokines tested, with effects similar in magnitude to those seen with dexamethasone treatment. The extensive impact of dexamethasone and tacrolimus on cytokine and iNOS messenger expression indicates that these treatments may exert strong anti-inflammatory effects in AOM. |
| Karlıdağ et al. (2004) [31] | Human study | 65 patients | Chronic otitis media with and without tympanosclerosis | Griess reaction, modified cadmium reduction method, spectrophotometric method | NO, MDA | In specimens taken from the middle ear mucosa, tympanic membrane, and correspondingly from plasma, the NO and MDA levels were higher in group 1 (patients with tympanosclerotic plaques) compared to group 2 (patients without tympanosclerosis). Additionally, group 1 exhibited lower antioxidant activity levels (superoxide dismutase and catalase) in their erythrocytes than group 2. NO, free oxygen radicals, and catalase might play a role in the development of tympanosclerosis in patients with chronic otitis media. |
| Rose et al. (1996) [32] | Animal study | 20 Sprague–Dawley rats | Otitis media with effusion | ELISA, immunohistochemistry | NOS | After 7 days, the LPS-exposed ears had a significantly greater volume of effusion and amount of collected mucin compared to the controls. Additionally, antimucin immunostaining revealed mucous cell hyperplasia as a response to LPS exposure. Treatment with L-NAME inhibited the LPS-induced production of mucin and mucous cell hyperplasia in the ears. LPS triggers the hypersecretion of mucin in OME, and inhibiting NO synthesis prevents the LPS-induced production of mucin in middle ear effusion. |
| Jeon et al. (2006) [33] | Animal study | 20 guinea pigs | Otitis media with effusion | 5% Coomassie Brilliant Blue dye transfer time, light microscopy, immunohistochemistry | NO | In the LPS group, dye transfer time was significantly delayed compared to the control group; conversely, it was notably shortened in the groups treated with L-NAME (NOS inhibitor) or uric acid (peroxynitrite scavenger). Histopathological examination revealed reduced inflammation and mucosal thickening in these treated groups compared to the LPS group. NO plays a role in every stage of OM pathogenesis, and its harmful effects may be mediated through the formation of RNS. New therapeutic strategies could be developed to mitigate the potential role of NO and peroxynitrite. However, given their defensive role against invading organisms, the timing of administration must be carefully considered. |
| Garça et al. (2013) [34] | Human study | 61 patients with COM and 30 controls | Chronic otitis media, COM with cholesteatoma (CCOM) | Serum TAC levels were measured spectrophotometrically; serum NO levels were measured using the Griess reagent | Lipid peroxidation, MAD, MPO, NO, TAC | Our study revealed that the patients with COM had significantly elevated serum NO levels and reduced TAC levels compared to the healthy controls. Furthermore, serum NO levels were markedly higher in the patients with cholesteatoma than in those without, whereas TAC levels were significantly lower. Enhanced oxidative stress appears to be linked with reduced antioxidant levels in patients with COM, suggesting that increased oxidative stress may contribute to the pathogenesis of COM. |
| Sagiroglu et al. (2018) [35] | Human study | 107 children | Chronic otitis media with effusion (COME), acute otitis media (AOM) | MPO activity was determined using the O-dianisidine method; CAT activity was assayed using Beutler’s method; NO levels were measured using the Griess reagent | MPO, CAT, NO | The levels of MPO, CAT, and NO were significantly elevated in the COME and AOM groups compared to the controls. CAT levels were slightly higher in the COME patients than in those with AOM. Serum levels of oxidative stress markers and antioxidant products actively contribute to the pathogenesis of COME and AOM. We believe these findings are crucial for the diagnosis and treatment of patients. |
| Tong et al. (2008) [36] | Animal study | 80 Sprague–Dawley rats | Acute otitis media | Real-time PCR, ELISA, H&E staining | NO | Nonviable NTHi (nontypeable Haemophilus influenza) 2019 parent strain induced a significant upregulation of iNOS gene expression compared to the B29 (NTHi LOS htrB gene mutant group) cohort. This study indicates that the disruption of the NTHi LOS htrB gene may impact the temporal mRNA expression of inflammatory mediators within the middle ear. |
| Author [Reference] | Study Design | Species and/or Sample | Types of Otitis Media | Detection Method | Target gene(s) or Pathway(s) Associated with NOS | Results/Conclusions |
|---|---|---|---|---|---|---|
| Ates et al. (2017) [43] | Animal study | 89 patients | Otitis media with effusion | Detection of the Clu298Asp polymorphism in eNOS was achieved by PCR-RFLP | eNOS | There was no statistically significant difference in genotypic distributions (Glu/Glu (G/G), Glu/Asp (G/T), Asp/Asp (T/T)). However, when comparing allele distributions, a significant relationship was found, with the G allele identified as a predisposing factor for genetic susceptibility to the development of OME. The G allele was identified as a predisposing factor for genetic susceptibility to the development of OME. Further comprehensive research is needed to explore new diagnostic and treatment modalities for OME, taking into account the eNOS polymorphism in pediatric patients. |
| Ryan et al. (2001) [44] | Animal study | 32 Hartley guinea pigs | Immune-mediated otitis media | Evaluation of effusion, H&E staining, light microscopy | NOS | Inhibition of NOS with NG-amino-L-arginine (L-NAA) led to a significant increase in middle ear effusion across all three time periods. This increase was prevented by adding excess L-arginine, which counteracts the inhibitory effects of L-NAA. The results indicate that NO plays a role in regulating the permeability of middle ear vasculature, the transudation of serum into the middle ear mucosa, and/or the movement of extracellular fluid across the middle ear mucosal epithelium. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, Y.J.; Lee, J.M.; Yeo, J.H.; Kim, S.S.; Yeo, S.G. Induction of Nitric Oxide and Its Role in Otitis Media. Antioxidants 2025, 14, 327. https://doi.org/10.3390/antiox14030327
Oh YJ, Lee JM, Yeo JH, Kim SS, Yeo SG. Induction of Nitric Oxide and Its Role in Otitis Media. Antioxidants. 2025; 14(3):327. https://doi.org/10.3390/antiox14030327
Chicago/Turabian StyleOh, Yeon Ju, Jae Min Lee, Joon Hyung Yeo, Sung Soo Kim, and Seung Geun Yeo. 2025. "Induction of Nitric Oxide and Its Role in Otitis Media" Antioxidants 14, no. 3: 327. https://doi.org/10.3390/antiox14030327
APA StyleOh, Y. J., Lee, J. M., Yeo, J. H., Kim, S. S., & Yeo, S. G. (2025). Induction of Nitric Oxide and Its Role in Otitis Media. Antioxidants, 14(3), 327. https://doi.org/10.3390/antiox14030327