

Lercanidipine’s Antioxidative Effect Prevents Noise-Induced Hearing Loss

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Cell Culture and Treatment
2.3. Cell Viability Assay
2.4. Culture of Cochlear Explant and DRUG Treatment
2.5. Real-Time PCR
2.6. Noise Exposure
2.7. Auditory Brainstem Response (ABR) Measurements
2.8. Cochlear Tissue Preparation and Fluorescent Labeling
2.9. Statistical Analysis
3. Results
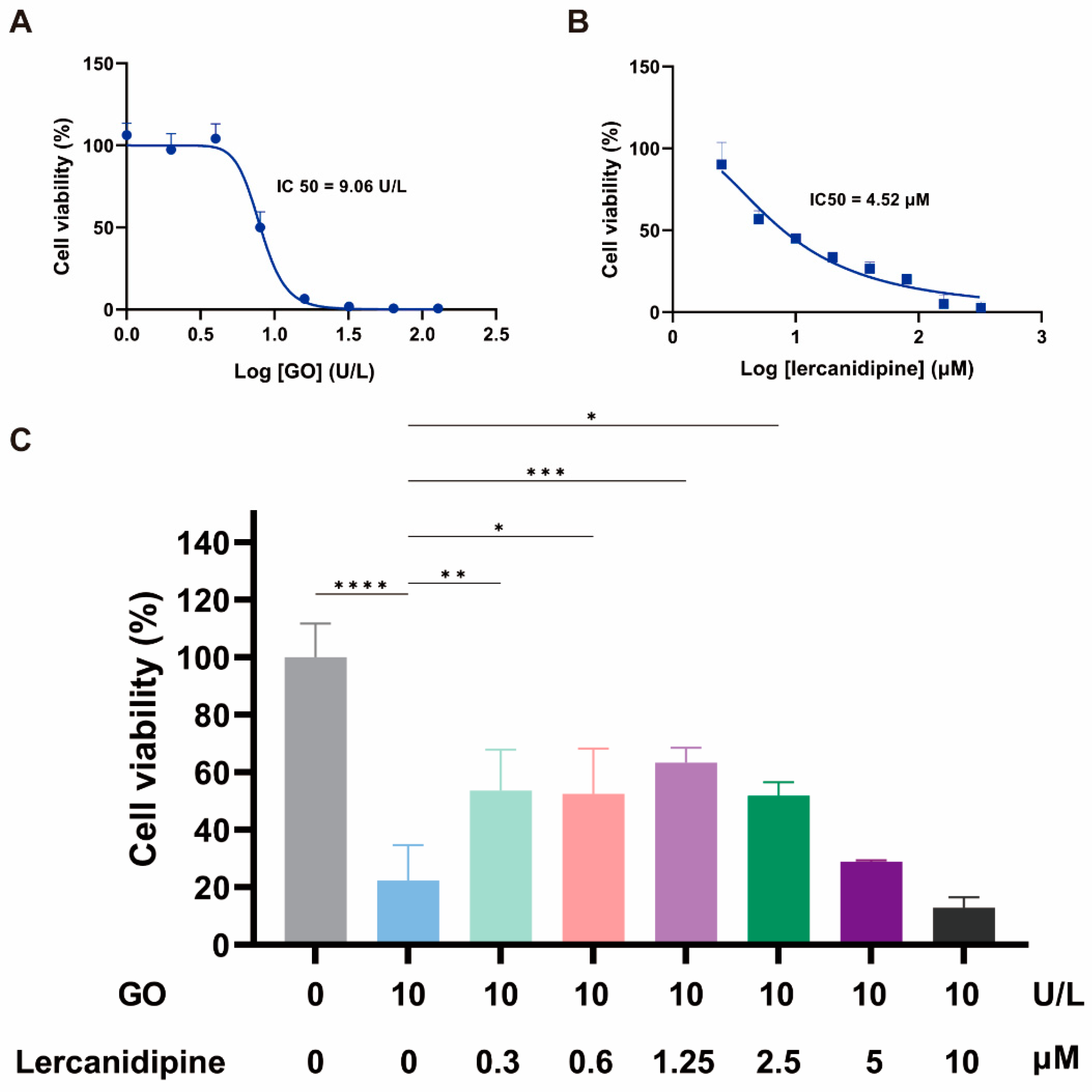
3.1. Lercanidipine Alleviates the Adverse Effect of GO on the OC-1 Cell Viability
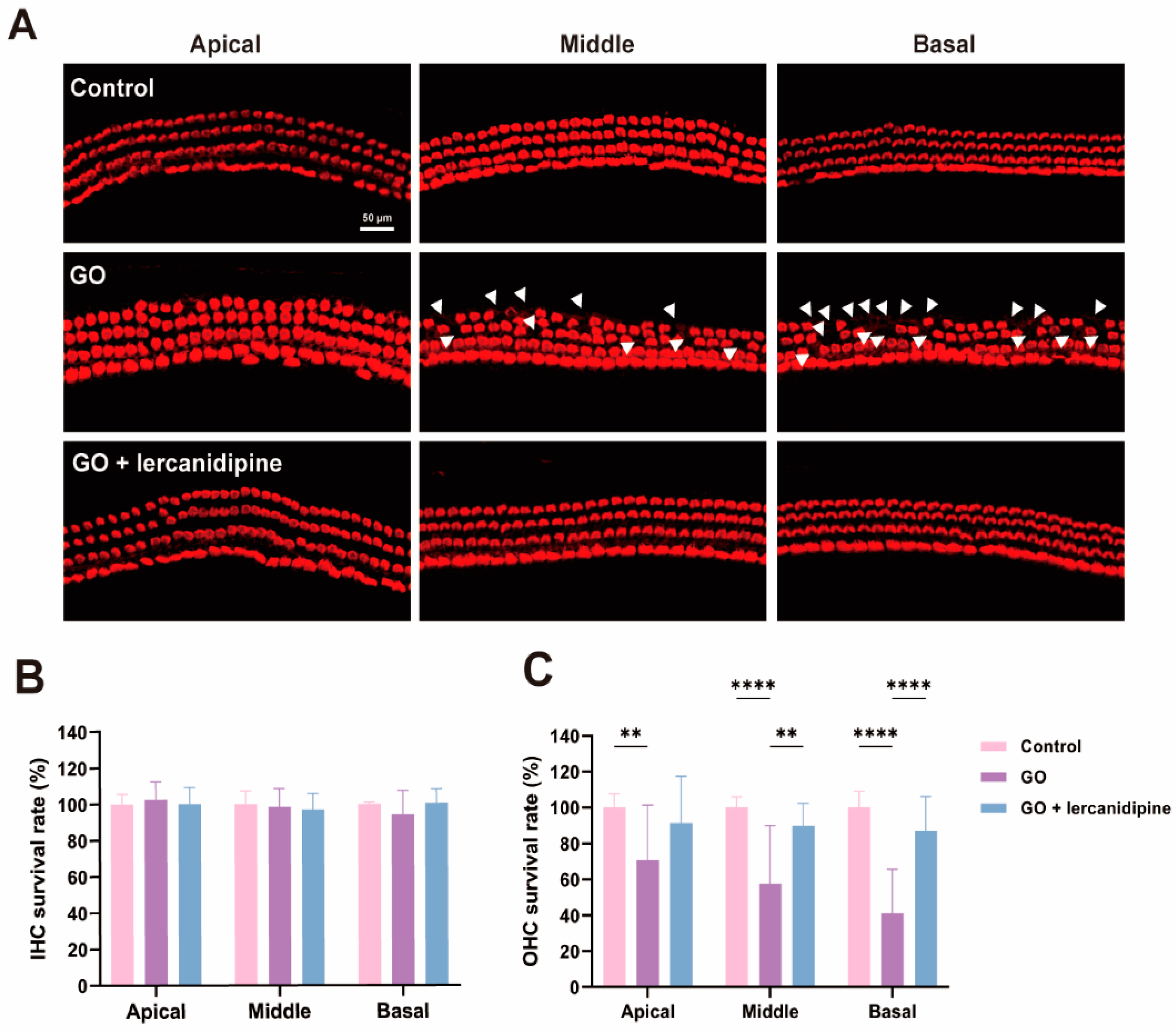
3.2. Lercanidipine Reverses the Damaging Effects of GO on the Cochlear Explant
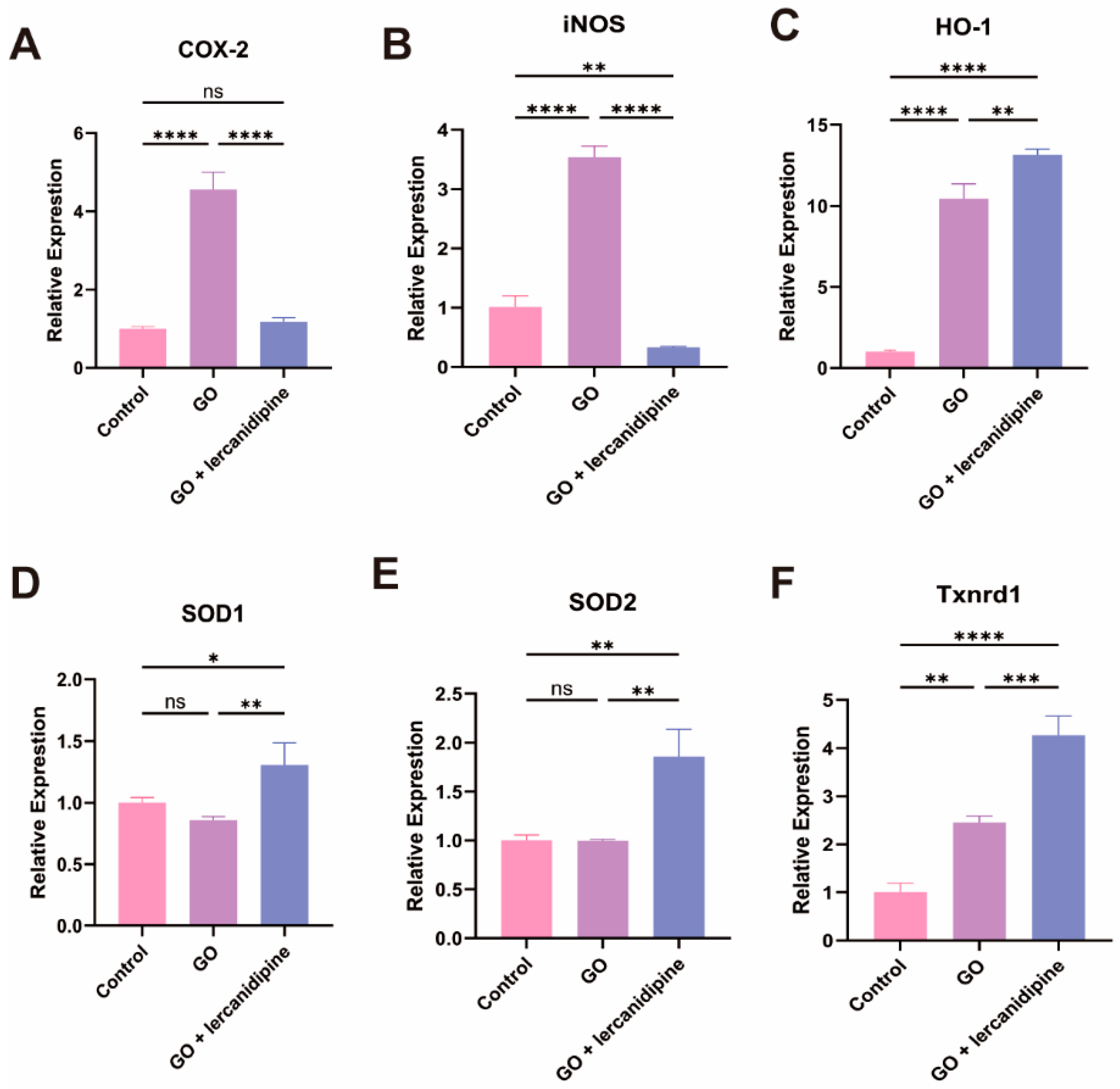
3.3. Lercanidipine Inhibits Oxidative and Promotes Antioxidative Enzyme Gene mRNA Expression after GO Treatment of Cochlea Explant
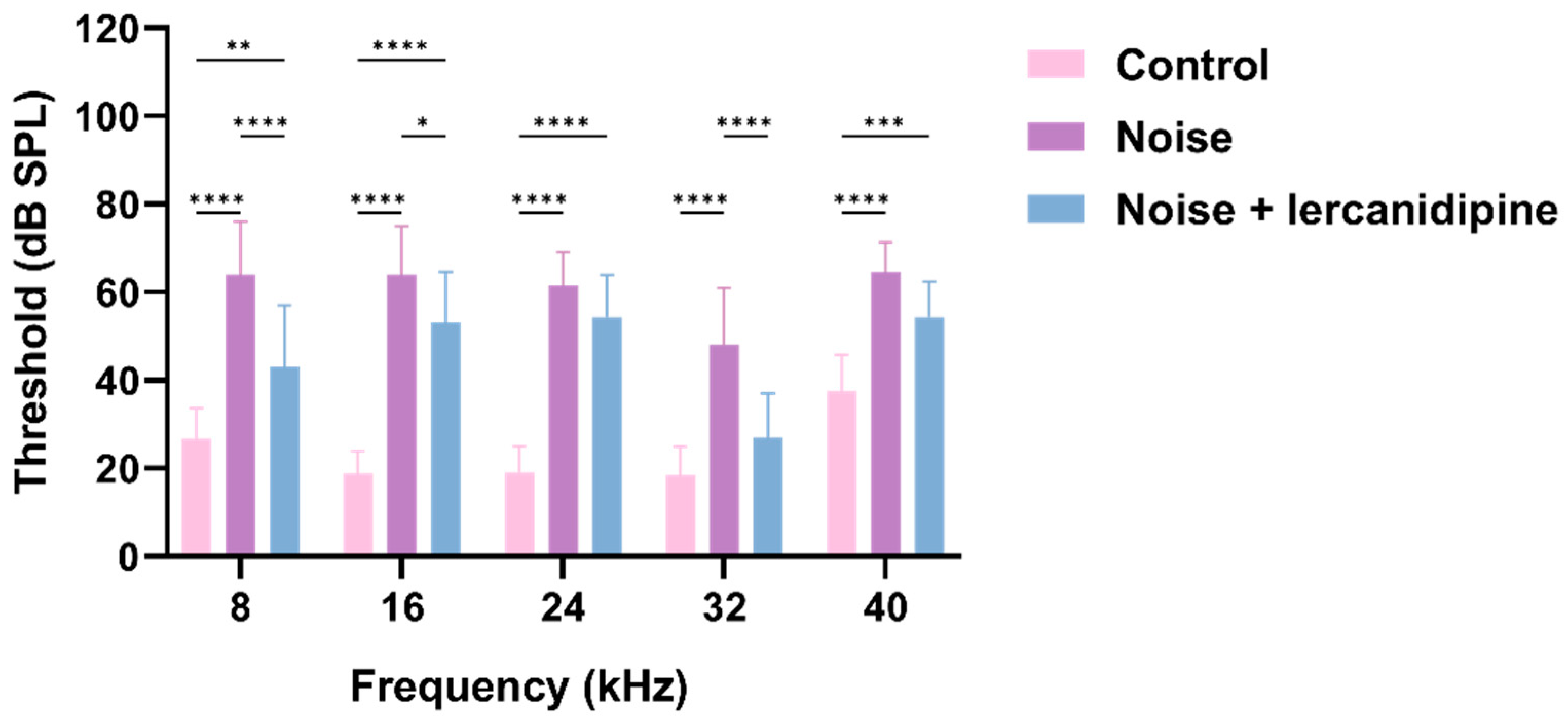
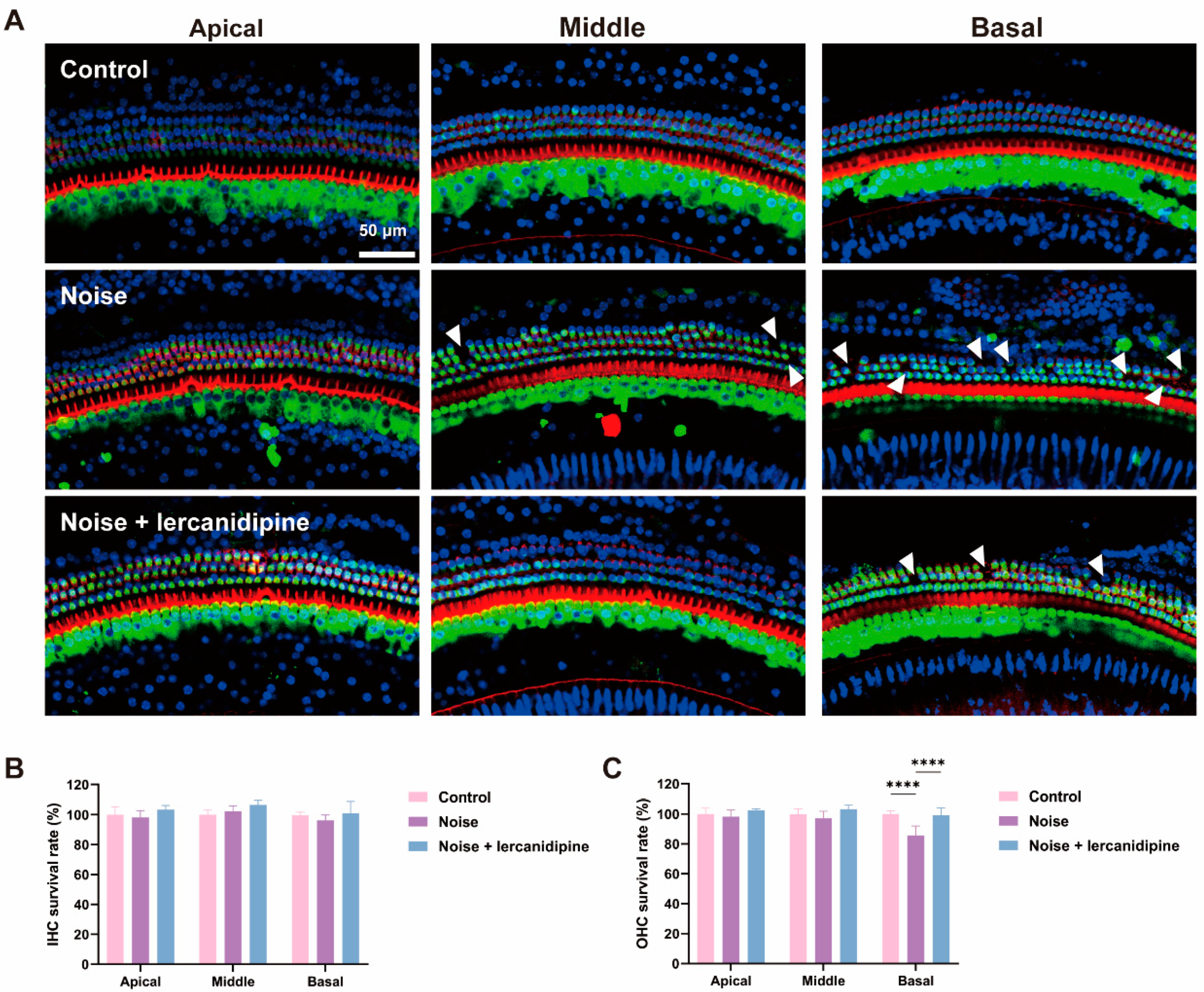
3.4. Lercanidipine Attenuates NIHL and Hair Cell Loss
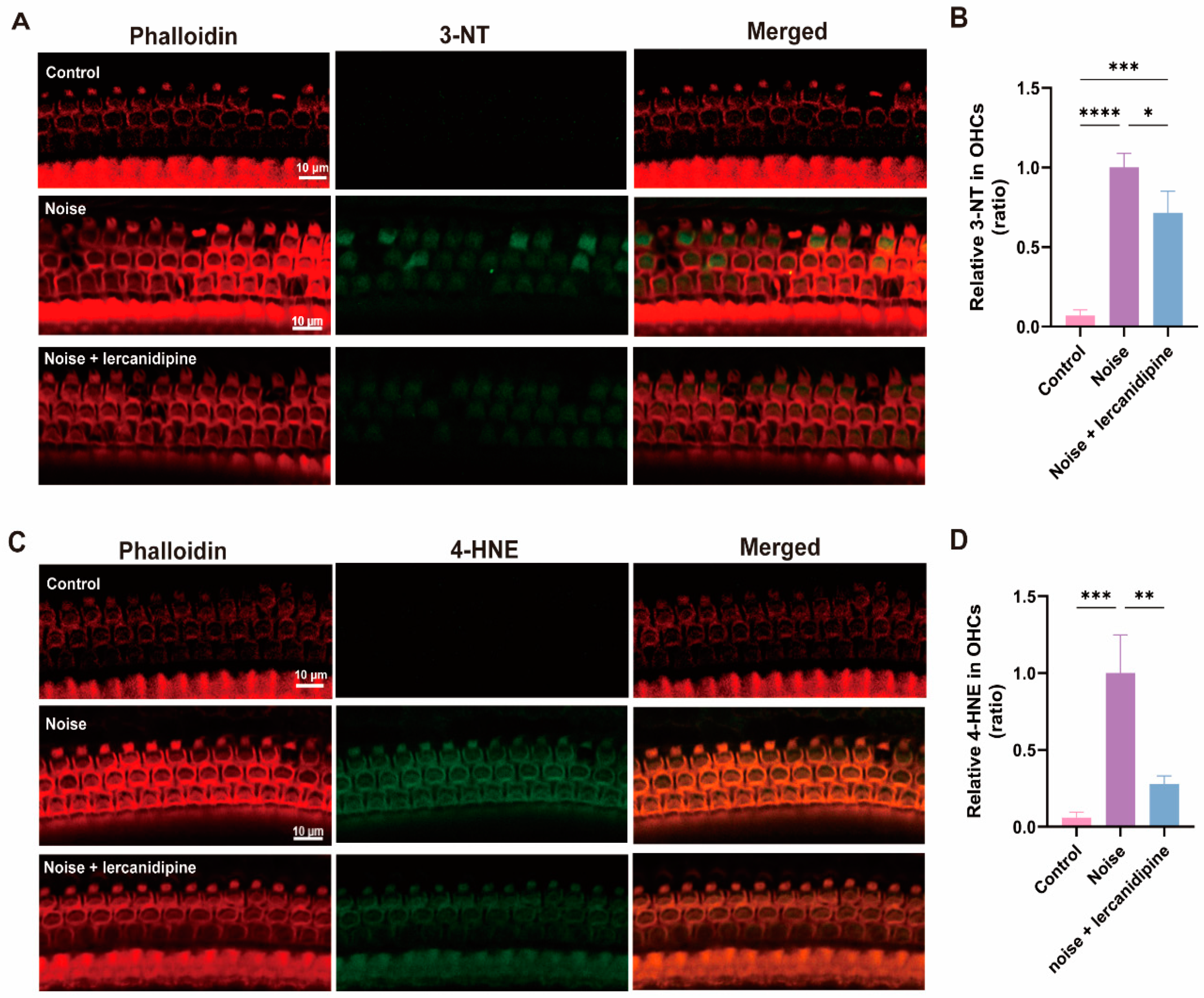
3.5. Lercanidipine Reduces Noise-Induced Oxidative Stress in OHCs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheffield, A.M.; Smith, R.J.H. The Epidemiology of Deafness. Cold Spring Harb. Perspect. Med. 2019, 9, 1–15. [Google Scholar] [CrossRef]
- Uy, J.; Forciea, M.A. In the Clinic. Hearing Loss. Ann. Intern. Med. 2013, 158, ITC4-1, quiz ITC4-16. [Google Scholar] [CrossRef]
- Park, S.N.; Back, S.A.; Park, K.H.; Seo, J.H.; Noh, H.I.; Akil, O.; Lustig, L.R.; Yeo, S.W. Comparison of Functional and Morphologic Characteristics of Mice Models of Noise-Induced Hearing Loss. Auris Nasus Larynx 2013, 40, 11–17. [Google Scholar] [CrossRef]
- Yamane, H.; Nakai, Y.; Takayama, M.; Iguchi, H.; Nakagawa, T.; Kojima, A. Appearance of Free Radicals in the Guinea Pig Inner Ear after Noise-Induced Acoustic Trauma. Eur. Arch. Oto-Rhino-Laryngol. 1995, 252, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Ohlemiller, K.K.; Wright, J.S.; Dugan, L.L. Early Elevation of Cochlear Oxygen Species Following Reactive Noise Exposure. Audiol. Neuro-Otol. 1999, 4, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, D.; Jiang, H.Y.; Schacht, J.; Miller, J.M. Delayed Production of Free Radicals Following Noise Exposure. Brain Res. 2004, 1019, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Ohinata, Y.; Yamasoba, T.; Schacht, J.; Miller, J.M. Glutathione Limits Noise-Induced Hearing Loss. Hear. Res. 2000, 146, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.C.M.; Meech, R.P.; Klemens, J.J.; Gerberi, M.T.; Dyrstad, S.S.W.; Larsen, D.L.; Mitchell, D.L.; El-Azizi, M.; Verhulst, S.J.; Hughes, L.F. Prevention of Noise- and Drug-Induced Hearing Loss with d-Methionine. Hear. Res. 2007, 226, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Bielefeld, E.C.; Kopke, R.D.; Jackson, R.L.; Coleman, J.K.M.; Liu, J.; Henderson, D. Noise Protection with N-Acetyl-l-Cysteine (NAC) Using a Variety of Noise Exposures, NAC Doses, and Routes of Administration. Acta Otolaryngol. 2007, 127, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Flieger, J.; Flieger, W.; Baj, J.; Maciejewski, R. Antioxidants: Classification, Natural Sources, Activity/Capacity Measurements, and Usefulness for the Synthesis of Nanoparticles. Materials 2021, 14, 4135. [Google Scholar] [CrossRef] [PubMed]
- Kramer, S.; Dreisbach, L.; Lockwood, J.; Baldwin, K.; Kopke, R.; Scranton, S.; O’Leary, M. Efficacy of the Antioxidant N-Acetylcysteine (NAC) in Protecting Ears Exposed to Loud Music. J. Am. Acad. Audiol. 2006, 17, 265–278. [Google Scholar] [CrossRef]
- Farah, R.; Shurtz-Swirski, R. The Combined Effect of Calcium Channel Blocker Lercanidipine and Antioxidants on Low-Grade Systemic Inflammation Parameters in Essential Hypertension Patients. Minerva Cardioangiol. 2008, 56, 467–476. [Google Scholar] [PubMed]
- Sacks, D.; Baxter, B.; Campbell, B.C.V.; Carpenter, J.S.; Cognard, C.; Dippel, D.; Eesa, M.; Fischer, U.; Hausegger, K.; Hirsch, J.A.; et al. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Lin, X.; Pornprasert, S.; Lü, X.; Ran, B.; Lin, Y. L-Type Calcium Channel Blockers Decrease the Iron Overload-Mediated Oxidative Stress in Renal Epithelial Cells by Reducing Iron Accumulation. Eur. J. Pharmacol. 2020, 886, 173513. [Google Scholar] [CrossRef]
- He, Z.H.; Zou, S.Y.; Li, M.; Liao, F.L.; Wu, X.; Sun, H.Y.; Zhao, X.Y.; Hu, Y.J.; Li, D.; Xu, X.X.; et al. The Nuclear Transcription Factor FoxG1 Affects the Sensitivity of Mimetic Aging Hair Cells to Inflammation by Regulating Autophagy Pathways. Redox Biol. 2020, 28, 101364. [Google Scholar] [CrossRef]
- Rivolta, M.N.; Holley, M.C. Cell Lines in Inner Ear Research. J. Neurobiol. 2002, 53, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Liu, Z.; Dong, D.; Schacht, J.; Arya, D.; Sha, S.H. Histone Deacetylase Inhibitors Are Protective in Acute but Not in Chronic Models of Ototoxicity. Front. Cell. Neurosci. 2017, 11, 1–9. [Google Scholar] [CrossRef]
- Bai, X.; Chen, S.; Xu, K.; Jin, Y.; Niu, X.; Xie, L.; Qiu, Y.; Liu, X.; Sun, Y. N-Acetylcysteine Combined with Dexamethasone Treatment Improves Sudden Sensorineural Hearing Loss and Attenuates Hair Cell Death Caused by ROS Stress. Front. Cell Dev. Biol. 2021, 9, 659486. [Google Scholar] [CrossRef]
- Xu, K.; Chen, S.; Xie, L.; Qiu, Y.; Liu, X.Z.; Bai, X.; Jin, Y.; Wang, X.H.; Sun, Y. The Protective Effects of Systemic Dexamethasone on Sensory Epithelial Damage and Hearing Loss in Targeted Cx26-Null Mice. Cell Death Dis. 2022, 13, 545. [Google Scholar] [CrossRef]
- Ohlemiller, K.K.; Wright, J.S.; Heidbreder, A.F. Vulnerability to Noise-Induced Hearing Loss in “middle-Aged” and Young Adult Mice: A Dose-Response Approach in CBA, C57BL, and BALB Inbred Strains. Hear. Res. 2000, 149, 239–247. [Google Scholar] [CrossRef]
- Zhou, X.X.; Chen, S.; Xie, L.; Ji, Y.Z.; Wu, X.; Wang, W.W.; Yang, Q.; Yu, J.T.; Sun, Y.; Lin, X.; et al. Reduced Connexin26 in the Mature Cochlea Increases Susceptibility to Noise-Induced Hearing Lossin Mice. Int. J. Mol. Sci. 2016, 17, 301. [Google Scholar] [CrossRef]
- Yuan, H.; Wang, X.; Hill, K.; Chen, J.; Lemasters, J.; Yang, S.M.; Sha, S.H. Autophagy Attenuates Noise-Induced Hearing Loss by Reducing Oxidative Stress. Antioxid. Redox Signal. 2015, 22, 1308–1324. [Google Scholar] [CrossRef] [PubMed]
- Fetoni, A.R.; Paciello, F.; Rolesi, R.; Paludetti, G.; Troiani, D. Targeting Dysregulation of Redox Homeostasis in Noise-Induced Hearing Loss: Oxidative Stress and ROS Signaling. Free Radic. Biol. Med. 2019, 135, 46–59. [Google Scholar] [CrossRef]
- Böttger, E.C.; Schacht, J. The Mitochondrion: A Perpetrator of Acquired Hearing Loss. Hear. Res. 2013, 303, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Gentilin, E.; Cani, A.; Simoni, E.; Chicca, M.; Di Paolo, M.L.; Martini, A.; Astolfi, L. Hydrogen Peroxide Toxicity on Auditory Cells: An in Vitro Study. Chem. Biol. Interact. 2021, 345, 109575. [Google Scholar] [CrossRef]
- Baker, K.; Staecker, H. Low Dose Oxidative Stress Induces Mitochondrial Damage in Hair Cells. Anat. Rec. 2012, 295, 1868–1876. [Google Scholar] [CrossRef]
- Ying, Y.L.M.; Balaban, C.D. Regional Distribution of Manganese Superoxide Dismutase 2 (Mn SOD2) Expression in Rodent and Primate Spiral Ganglion Cells. Hear. Res. 2009, 253, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Sha, S.H.; Schacht, J. Emerging Therapeutic Interventions against Noise-Induced Hearing Loss. Expert Opin. Investig. Drugs 2017, 26, 85–96. [Google Scholar] [CrossRef]
- Ohinata, Y.; Miller, J.M.; Altschuler, R.A.; Schacht, J. Intense Noise Induces Formation of Vasoactive Lipid Peroxidation Products in the Cochlea. Brain Res. 2000, 878, 163–173. [Google Scholar] [CrossRef]
- Thalmann, R.; Miyoshi, T.; Thalmann, I. The Influence of Ischemia upon the Energy Reserves of Inner Ear Tissues. Laryngoscope 1972, 82, 2249–2272. [Google Scholar] [CrossRef]
- Mom, T.; Bon, P.; Gilain, L.; Avan, P. Vulnerability of the Gerbil Cochlea to Sound Exposure during Reversible Ischemia. Hear. Res. 1999, 136, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.J.T.; Thorne, P.R.; Vlajkovic, S.M. Characterisation of Cochlear Inflammation in Mice Following Acute and Chronic Noise Exposure. Histochem. Cell Biol. 2016, 146, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Tornabene, S.V.; Sato, K.; Pham, L.; Billings, P.; Keithley, E.M. Immune Cell Recruitment Following Acoustic Trauma. Hear. Res. 2006, 222, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Mason, R.P. Mechanisms of Plaque Stabilization for the Dihydropyridine Calcium Channel Blocker Amlodipine: Review of the Evidence. Atherosclerosis 2002, 165, 191–199. [Google Scholar] [CrossRef]
- Yamane, H.; Nakai, Y.; Takayama, M.; Konishi, K.; Iguchi, H.; Nakagawa, T.; Shibata, S.; Kato, A.; Sunami, K.; Kawakatsu, C. The Emergence of Free Radicals after Acoustic Trauma and Strial Blood Flow. Acta Otolaryngol. 1995, 115, 87–92. [Google Scholar] [CrossRef]
- Meredith, P.A. Lercanidipine: A Novel Lipophilic Dihydropyridine Calcium Antagonist with Long Duration of Action and High Vascular Selectivity. Expert Opin. Investig. Drugs 1999, 8, 1043–1062. [Google Scholar] [CrossRef]
- Goldwyn, B.G.; Quirk, W.S. Calcium Channel Blockade Reduces Noise-Induced Vascular Permeability in Cochlear Stria Vascularis. Laryngoscope 1997, 107, 1112–1116. [Google Scholar] [CrossRef]
- Umemura, K.; Kohno, Y.; Asai, Y.; Uematsu, T.; Nakashima, M. Effect of a Ca2+ Entry Blocker, Nilvadipine, on Hearing Disturbances and Equilibrium Dysfunction Caused by Microcirculatory Disorders of the Rat Inner Ear. Eur. J. Pharmacol. 1993, 239, 17–21. [Google Scholar] [CrossRef]
- Liu, J.; Niu, Y.G.; Li, W.X.; Yuan, Y.Y.; Han, W.J.; Yu, N.; Yang, S.M.; Li, X.Q. Interaction of a Calcium Channel Blocker with Noise in Cochlear Function in Guinea Pig. Acta Otolaryngol. 2012, 132, 1140–1144. [Google Scholar] [CrossRef]
- Velena, A.; Zarkovic, N.; Gall Troselj, K.; Bisenieks, E.; Krauze, A.; Poikans, J.; Duburs, G. 1,4-Dihydropyridine Derivatives: Dihydronicotinamide Analogues—Model Compounds Targeting Oxidative Stress. Oxid. Med. Cell. Longev. 2016, 2016, 1892412. [Google Scholar] [CrossRef] [PubMed]
- Clifford, R.E.; Coleman, J.K.M.; Balough, B.J.; Liu, J.; Kopke, R.D.; Jackson, R.L. Low-Dose D-Methionine and N-Acetyl-L-Cysteine for Protection from Permanent Noise-Induced Hearing Loss in Chinchillas. Otolaryngol. Head Neck Surg. 2011, 145, 999–1006. [Google Scholar] [CrossRef]
- Yeh, J.L.; Hsu, J.H.; Liang, J.C.; Chen, I.J.; Liou, S.F. Lercanidipine and Labedipinedilol-A Attenuate Lipopolysaccharide/Interferon-γ-Induced Inflammation in Rat Vascular Smooth Muscle Cells through Inhibition of HMGB1 Release and MMP-2, 9 Activities. Atherosclerosis 2013, 226, 364–372. [Google Scholar] [CrossRef]
- Wu, J.; Liou, S.; Lin, S.; Chai, C.; Dai, Z.; Liang, J.; Chen, I.; Yeh, J. Lercanidipine Inhibits Vascular Smooth Muscle Cell Proliferation and Neointimal Formation via Reducing Intracellular Reactive Oxygen Species and Inactivating Ras-ERK1/2 Signaling. Pharmacol. Res. 2009, 59, 48–56. [Google Scholar] [CrossRef]
- Omboni, S.; Zanchetti, A. Antihypertensive Efficacy of Lercanidipine at 2.5, 5 and 10 Mg in Mild to Moderate Essential Hypertensives Assessed by Clinic and Ambulatory Blood Pressure Measurements. Multicenter Study Investigators. J. Hypertens. 1998, 16, 1831–1838. [Google Scholar] [CrossRef]
- Barrios, V.; Navarro, A.; Esteras, A.; Luque, M.; Romero, J.; Tamargo, J.; Prieto, L.; Carrasco, J.L.; Herranz, I.; Navarro-Cid, J.; et al. Antihypertensive Efficacy and Tolerability of Lercanidipine in Daily Clinical Practice. The ELYPSE Study. Eficacia de Lercanidipino y Su Perfil de Seguridad. Blood Press. 2002, 11, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Barrios, V.; Escobar, C.; De La Figuera, M.; Honorato, J.; Llisterri, J.L.; Segura, J.; Calderón, A. High Doses of Lercanidipine Are Better Tolerated than Other Dihydropyridines in Hypertensive Patients with Metabolic Syndrome: Results from the TOLERANCE Study. Int. J. Clin. Pract. 2008, 62, 723–728. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Becatti, M.; Marcucci, R.; Mannucci, A.; Gori, A.M.; Giusti, B.; Sofi, F.; Mannini, L.; Cellai, A.P.; Liotta, A.A.; Mugnaini, M.; et al. Erythrocyte Membrane Fluidity Alterations in Sudden Sensorineural Hearing Loss Patients: The Role of Oxidative Stress. Thromb. Haemost. 2017, 117, 2334–2345. [Google Scholar] [CrossRef] [PubMed]
- Teranishi, M.; Uchida, Y.; Nishio, N.; Kato, K.; Otake, H.; Yoshida, T.; Suzuki, H.; Sone, M.; Sugiura, S.; Ando, F.; et al. Polymorphisms in Genes Involved in Oxidative Stress Response in Patients with Sudden Sensorineural Hearing Loss and Ménière’s Disease in a Japanese Population. DNA Cell Biol. 2012, 31, 1555–1562. [Google Scholar] [CrossRef] [PubMed]
- Someya, S.; Xu, J.; Kondo, K.; Ding, D.; Salvi, R.J.; Yamasoba, T.; Rabinovitch, P.S. Age-Related Hearing Loss in C57BL/6J Mice Is Mediated by Bak-Dependent Mitochondrial Apoptosis. Proc. Natl. Acad. Sci. USA 2009, 106, 19432–19437. [Google Scholar] [CrossRef]
- Staecker, H.; Zheng, Q.Y.; Van De Water, T.R. Oxidative Stress in Aging in the C57B16/J Mouse Cochlea. Acta Otolaryngol. 2001, 121, 666–672. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene ID | Gene | Gene Location | Amplicon Size | Sequence (5′→3′) | CDS Location | Exon |
|---|---|---|---|---|---|---|
| 19225 | COX-2 | NC_000067.7 (149975851..149983978) | 271 | TTCAACACACTCTATCACTGGC AGAAGCGTTTGCGGTACTCAT | 1099–1120 1369–1349 | 8–9 |
| 18126 | iNOS | NC_000077.7 (78811613..78851052) | 127 | GTTCTCAGCCCAACAATACAAGA GTGGACGGGTCGATGTCAC | 103–125 229–211 | 1–3 |
| 15368 | HO-1 | NC_000074.7 (75820246..75827221) | 100 | AAGCCGAGAATGCTGAGTTCA GCCGTGTAGATATGGTACAAGGA | 80–100 179–157 | 2 |
| 20655 | SOD1 | NC_000082.7 (90017650..90023221) | 139 | AACCAGTTGTGTTGTCAGGAC CCACCATGTTTCTTAGAGTGAGG | 83–103 221–199 | 2–3 |
| 20656 | SOD2 | NC_000082.7 (90017650..90023221) | 113 | CAGACCTGCCTTACGACTATGG CTCGGTGGCGTTGAGATTGTT | 86–107 198–178 | 2 |
| 50493 | Txnrd1 | NC_000076.7 (82669785..82733558) | 134 | CCCACTTGCCCCAACTGTT GGGAGTGTCTTGGAGGGAC | 76–94 209–191 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Z.; Tian, E.; Chen, S.; Wang, J.; Chen, J.; Kong, W.; Crans, D.C.; Lu, Y.; Zhang, S. Lercanidipine’s Antioxidative Effect Prevents Noise-Induced Hearing Loss. Antioxidants 2024, 13, 327. https://doi.org/10.3390/antiox13030327
Guo Z, Tian E, Chen S, Wang J, Chen J, Kong W, Crans DC, Lu Y, Zhang S. Lercanidipine’s Antioxidative Effect Prevents Noise-Induced Hearing Loss. Antioxidants. 2024; 13(3):327. https://doi.org/10.3390/antiox13030327
Chicago/Turabian StyleGuo, Zhaoqi, E Tian, Sen Chen, Jun Wang, Jingyu Chen, Weijia Kong, Debbie C. Crans, Yisheng Lu, and Sulin Zhang. 2024. "Lercanidipine’s Antioxidative Effect Prevents Noise-Induced Hearing Loss" Antioxidants 13, no. 3: 327. https://doi.org/10.3390/antiox13030327
APA StyleGuo, Z., Tian, E., Chen, S., Wang, J., Chen, J., Kong, W., Crans, D. C., Lu, Y., & Zhang, S. (2024). Lercanidipine’s Antioxidative Effect Prevents Noise-Induced Hearing Loss. Antioxidants, 13(3), 327. https://doi.org/10.3390/antiox13030327