
Association between the Composite Dietary Antioxidant Index and Atherosclerotic Cardiovascular Disease in Postmenopausal Women: A Cross-Sectional Study of NHANES Data, 2013–2018


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Participants
2.3. Outcome Ascertainment
2.4. CDAI Measurement
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Population Characteristics
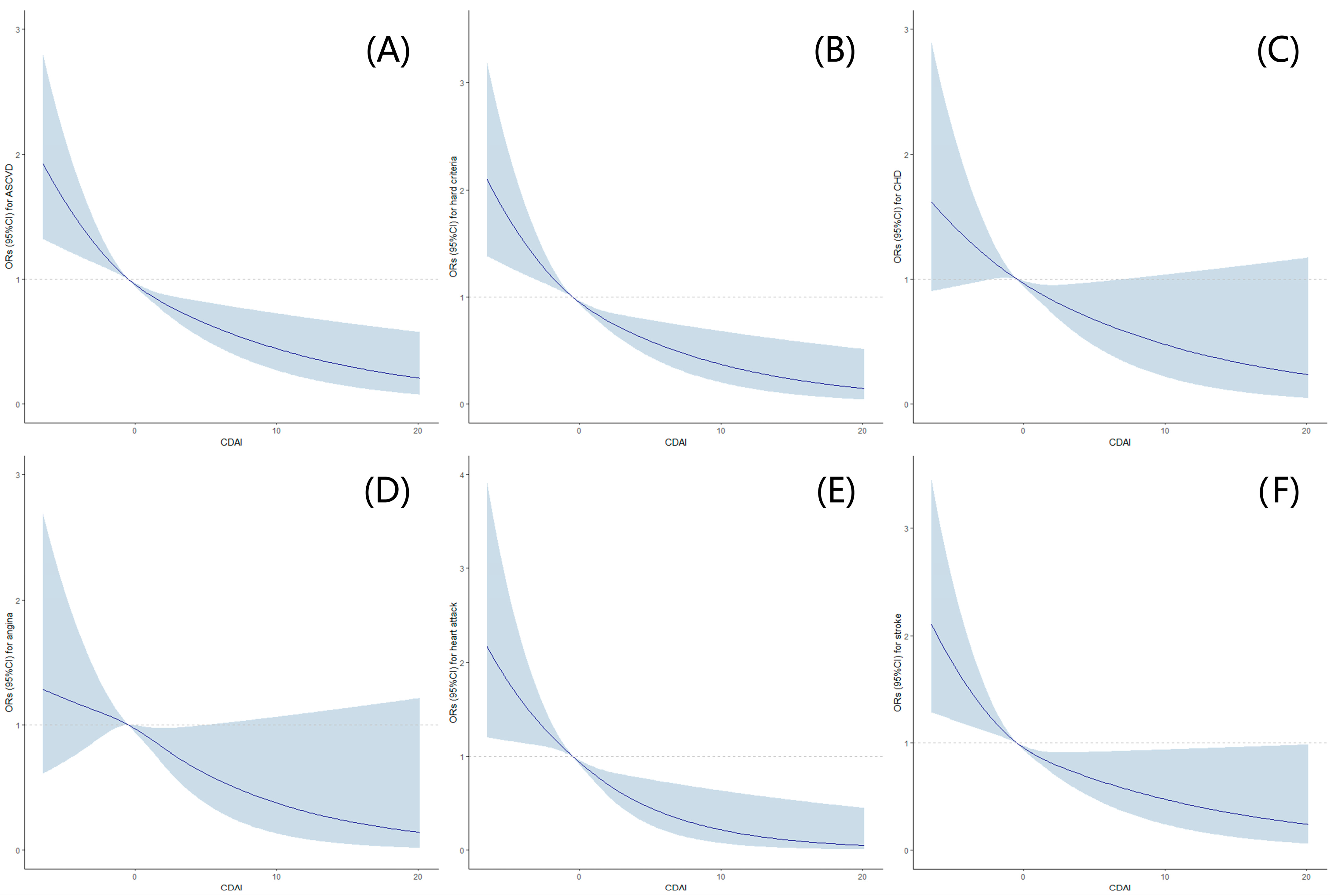
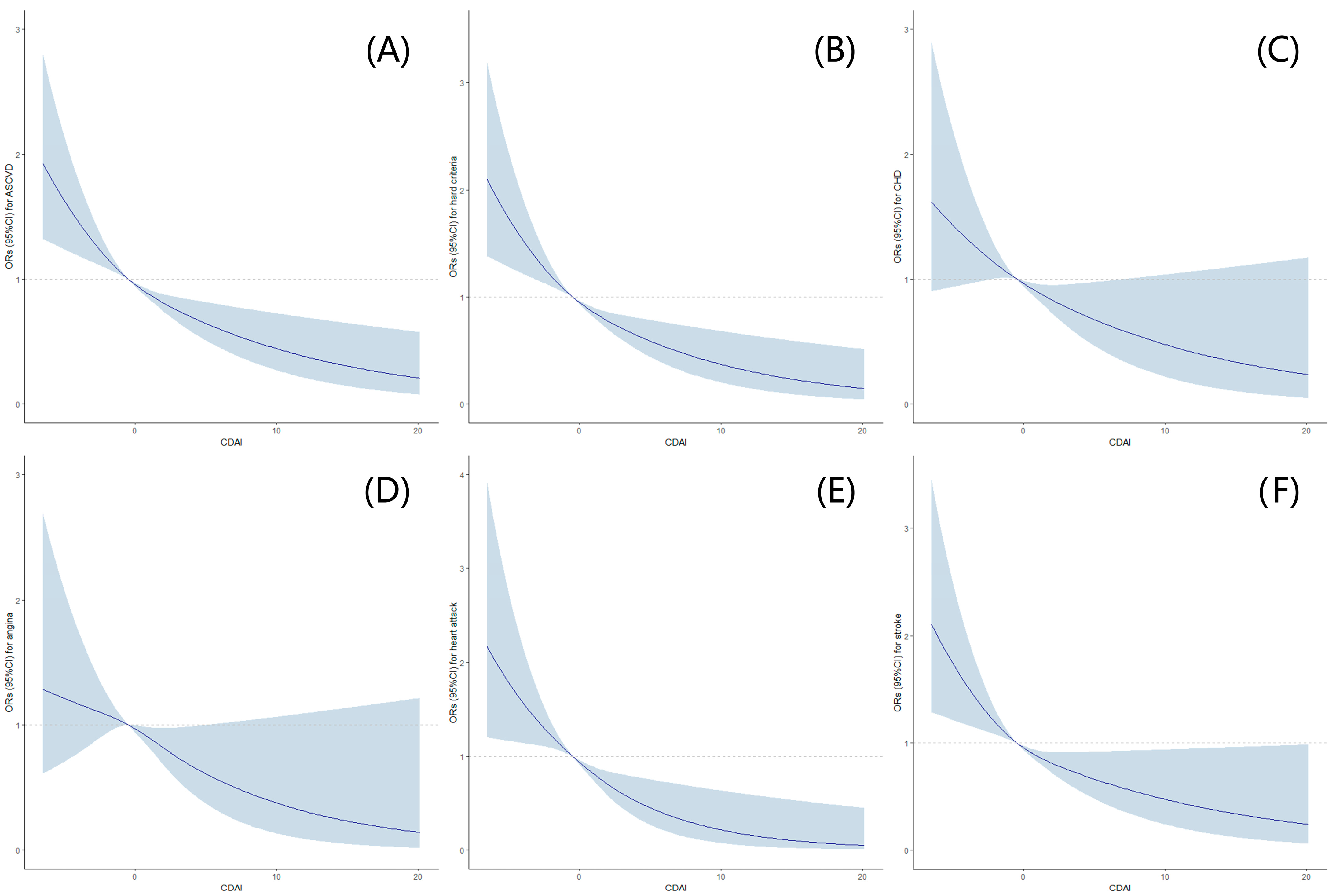
3.2. Associations between CDAI Levels and Risks of ASCVD and Hard Criteria
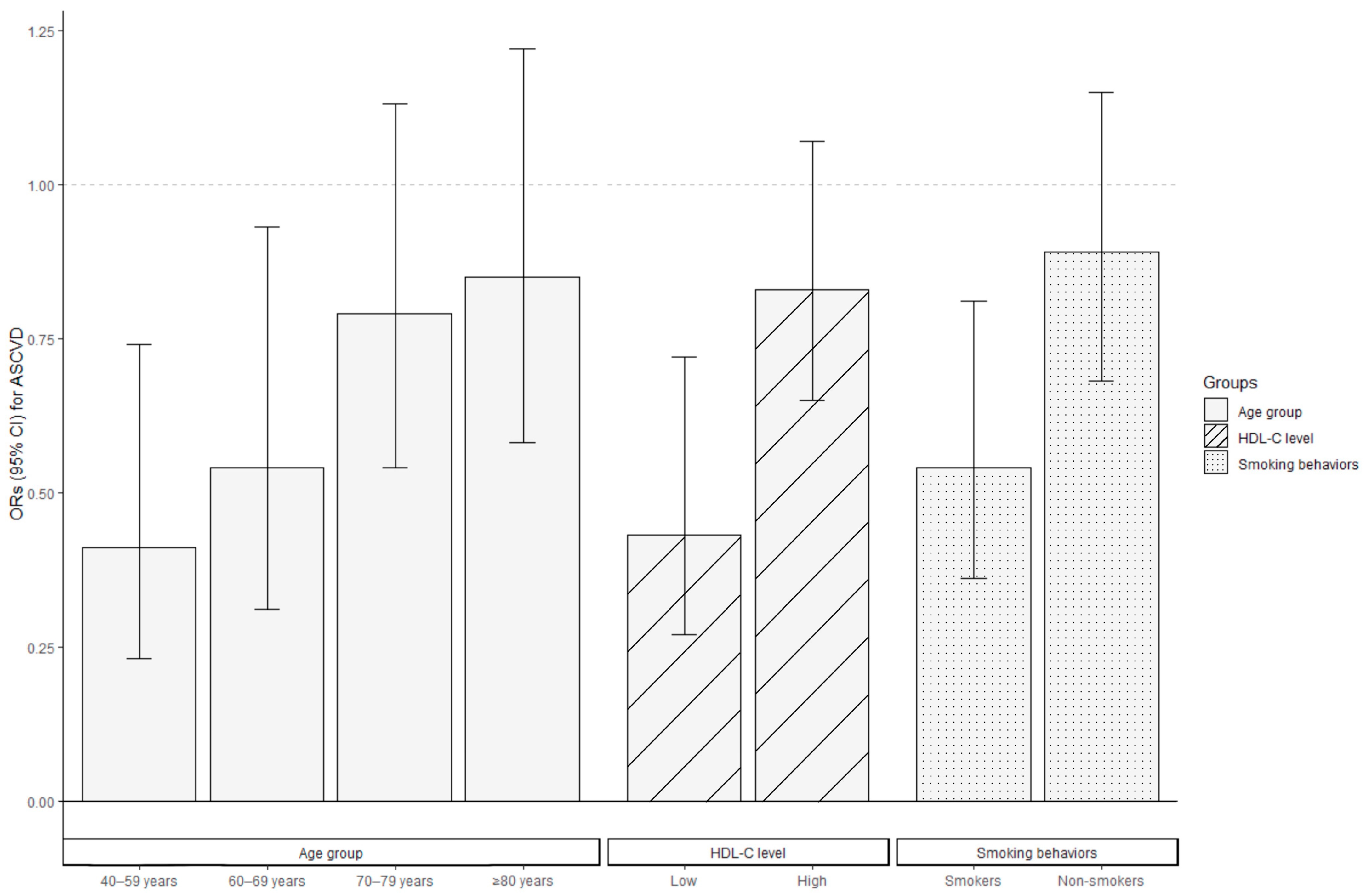
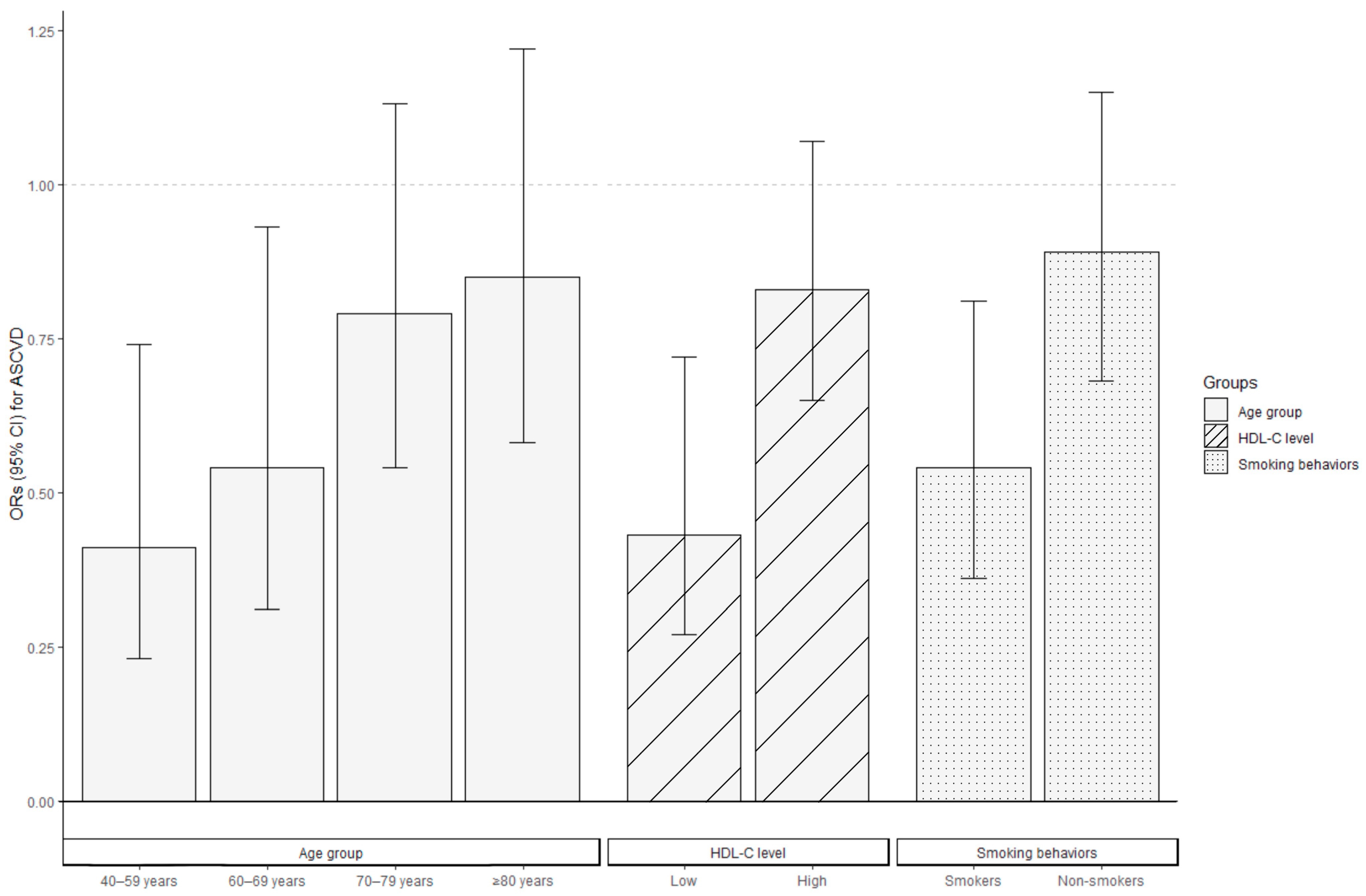
3.3. Stratified Analyses by Potential Effect Modifiers
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cowan, A.E.; Jun, S.; Gahche, J.J.; Tooze, J.A.; Dwyer, J.T.; Eicher-Miller, H.A.; Bhadra, A.; Guenther, P.M.; Potischman, N.; Dodd, K.W.; et al. Dietary Supplement Use Differs by Socioeconomic and Health-Related Characteristics among U.S. Adults, NHANES 2011–2014. Nutrients 2018, 10, 1114. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: A systematic review and dose-response meta-analysis of prospective studies. Am. J. Clin. Nutr. 2018, 108, 1069–1091. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 2018, 13, 757–772. [Google Scholar] [CrossRef] [PubMed]
- Siti, H.N.; Kamisah, Y.; Kamsiah, J. The role of oxidative stress, antioxidants and vascular inflammation in cardiovascular disease (a review). Vasc. Pharmacol. 2015, 71, 40–56. [Google Scholar] [CrossRef]
- Firuzi, O.; Miri, R.; Tavakkoli, M.; Saso, L. Antioxidant therapy: Current status and future prospects. Curr. Med. Chem. 2011, 18, 3871–3888. [Google Scholar] [CrossRef]
- O’Connor, E.A.; Evans, C.V.; Ivlev, I.; Rushkin, M.C.; Thomas, R.G.; Martin, A.; Lin, J.S. Vitamin and Mineral Supplements for the Primary Prevention of Cardiovascular Disease and Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2022, 327, 2334–2347. [Google Scholar] [CrossRef]
- Mangione, C.M.; Barry, M.J.; Nicholson, W.K.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Jaén, C.R.; et al. Vitamin, Mineral, and Multivitamin Supplementation to Prevent Cardiovascular Disease and Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2022, 327, 2326–2333. [Google Scholar] [CrossRef]
- Yu, Y.C.; Paragomi, P.; Wang, R.; Jin, A.; Schoen, R.E.; Sheng, L.T.; Pan, A.; Koh, W.P.; Yuan, J.M.; Luu, H.N. Composite dietary antioxidant index and the risk of colorectal cancer: Findings from the Singapore Chinese Health Study. Int. J. Cancer 2022, 150, 1599–1608. [Google Scholar] [CrossRef]
- Zhao, L.; Sun, Y.; Cao, R.; Wu, X.; Huang, T.; Peng, W. Non-linear association between composite dietary antioxidant index and depression. Front. Public Health 2022, 10, 988727. [Google Scholar] [CrossRef]
- Luu, H.N.; Wen, W.; Li, H.; Dai, Q.; Yang, G.; Cai, Q.; Xiang, Y.B.; Gao, Y.T.; Zheng, W.; Shu, X.O. Are dietary antioxidant intake indices correlated to oxidative stress and inflammatory marker levels? Antioxid. Redox Signal. 2015, 22, 951–959. [Google Scholar] [CrossRef]
- Wang, L.; Yi, Z. Association of the Composite dietary antioxidant index with all-cause and cardiovascular mortality: A prospective cohort study. Front. Cardiovasc. Med. 2022, 9, 993930. [Google Scholar] [CrossRef] [PubMed]
- Matthews, K.A.; Crawford, S.L.; Chae, C.U.; Everson-Rose, S.A.; Sowers, M.F.; Sternfeld, B.; Sutton-Tyrrell, K. Are changes in cardiovascular disease risk factors in midlife women due to chronological aging or to the menopausal transition? J. Am. Coll. Cardiol. 2009, 54, 2366–2373. [Google Scholar] [CrossRef] [PubMed]
- Xiang, D.; Liu, Y.; Zhou, S.; Zhou, E.; Wang, Y. Protective Effects of Estrogen on Cardiovascular Disease Mediated by Oxidative Stress. Oxid. Med. Cell. Longev. 2021, 2021, 5523516. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.L.; Xu, J.; Kochanek, K.D.; Arias, E. Mortality in the United States, 2017; NCHS Data Brief; National Center for Health Statistics: Hyattsville, MD, USA, 2018. [Google Scholar]
- World Health Organization. Menopause. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/menopause (accessed on 8 July 2023).
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef]
- Wright, M.E.; Mayne, S.T.; Stolzenberg-Solomon, R.Z.; Li, Z.; Pietinen, P.; Taylor, P.R.; Virtamo, J.; Albanes, D. Development of a comprehensive dietary antioxidant index and application to lung cancer risk in a cohort of male smokers. Am. J. Epidemiol. 2004, 160, 68–76. [Google Scholar] [CrossRef]
- Koene, R.J.; Prizment, A.E.; Blaes, A.; Konety, S.H. Shared Risk Factors in Cardiovascular Disease and Cancer. Circulation 2016, 133, 1104–1114. [Google Scholar] [CrossRef]
- Murray, C.J.; Atkinson, C.; Bhalla, K.; Birbeck, G.; Burstein, R.; Chou, D.; Dellavalle, R.; Danaei, G.; Ezzati, M.; Fahimi, A.; et al. The state of US health, 1990-2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 310, 591–608. [Google Scholar] [CrossRef]
- Peñalvo, J.L.; Cudhea, F.; Micha, R.; Rehm, C.D.; Afshin, A.; Whitsel, L.; Wilde, P.; Gaziano, T.; Pearson-Stuttard, J.; O’Flaherty, M.; et al. The potential impact of food taxes and subsidies on cardiovascular disease and diabetes burden and disparities in the United States. BMC Med. 2017, 15, 208. [Google Scholar] [CrossRef]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean diet, its components, and cardiovascular disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Rev. Española De Cardiol. 2022, 75, 429. [Google Scholar] [CrossRef]
- Villaverde, P.; Lajous, M.; MacDonald, C.J.; Fagherazzi, G.; Bonnet, F.; Boutron-Ruault, M.C. High dietary total antioxidant capacity is associated with a reduced risk of hypertension in French women. Nutr. J. 2019, 18, 31. [Google Scholar] [CrossRef]
- Hermsdorff, H.H.; Puchau, B.; Volp, A.C.; Barbosa, K.B.; Bressan, J.; Zulet, M.; Martínez, J.A. Dietary total antioxidant capacity is inversely related to central adiposity as well as to metabolic and oxidative stress markers in healthy young adults. Nutr. Metab. 2011, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Syddall, H.E.; Phillips, D.I.; Sayer, A.A.; Dennison, E.M.; Cooper, C.; Robinson, S.M. Dietary total antioxidant capacity is related to glucose tolerance in older people: The Hertfordshire Cohort Study. Nutr. Metab. Cardiovasc. Dis. NMCD 2014, 24, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Parohan, M.; Anjom-Shoae, J.; Nasiri, M.; Khodadost, M.; Khatibi, S.R.; Sadeghi, O. Dietary total antioxidant capacity and mortality from all causes, cardiovascular disease and cancer: A systematic review and dose-response meta-analysis of prospective cohort studies. Eur. J. Nutr. 2019, 58, 2175–2189. [Google Scholar] [CrossRef]
- Kim, K.; Vance, T.M.; Chen, M.H.; Chun, O.K. Dietary total antioxidant capacity is inversely associated with all-cause and cardiovascular disease death of US adults. Eur. J. Nutr. 2018, 57, 2469–2476. [Google Scholar] [CrossRef] [PubMed]
- Zujko, M.E.; Waśkiewicz, A.; Witkowska, A.M.; Szcześniewska, D.; Zdrojewski, T.; Kozakiewicz, K.; Drygas, W. Dietary Total Antioxidant Capacity and Dietary Polyphenol Intake and Prevalence of Metabolic Syndrome in Polish Adults: A Nationwide Study. Oxid. Med. Cell. Longev. 2018, 2018, 7487816. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, H.; Daneshzad, E.; Surkan, P.J.; Azadbakht, L. Dietary Total Antioxidant Capacity and Cardiovascular Disease Risk Factors: A Systematic Review of Observational Studies. J. Am. Coll. Nutr. 2018, 37, 533–545. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Moradi, F.; Najafi, M.; Jafarabadi, M.A. 10-year survival in coronary artery bypass grafting surgery patients in Tehran heart center, coronary outcome measurement study: Predictive power of dietary inflammatory index and dietary antioxidant quality. Nutrition 2019, 63–64, 22–28. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, M.; Lee, S.G.; Davis, C.G.; Koo, S.I.; Fernandez, M.L.; Volek, J.S.; Chun, O.K. Diets high in total antioxidant capacity improve risk biomarkers of cardiovascular disease: A 9-month observational study among overweight/obese postmenopausal women. Eur. J. Nutr. 2014, 53, 1363–1369. [Google Scholar] [CrossRef]
- Maugeri, A.; Hruskova, J.; Jakubik, J.; Kunzova, S.; Sochor, O.; Barchitta, M.; Agodi, A.; Bauerova, H.; Medina-Inojosa, J.R.; Vinciguerra, M. Dietary antioxidant intake decreases carotid intima media thickness in women but not in men: A cross-sectional assessment in the Kardiovize study. Free Radic. Biol. Med. 2019, 131, 274–281. [Google Scholar] [CrossRef]
- Zujko, M.E.; Waśkiewicz, A.; Witkowska, A.M.; Cicha-Mikołajczyk, A.; Zujko, K.; Drygas, W. Dietary Total Antioxidant Capacity-A New Indicator of Healthy Diet Quality in Cardiovascular Diseases: A Polish Cross-Sectional Study. Nutrients 2022, 14, 3219. [Google Scholar] [CrossRef]
- Witkowska, A.M.; Waśkiewicz, A.; Zujko, M.E.; Szcześniewska, D.; Pająk, A.; Stepaniak, U.; Drygas, W. Dietary Polyphenol Intake, but Not the Dietary Total Antioxidant Capacity, Is Inversely Related to Cardiovascular Disease in Postmenopausal Polish Women: Results of WOBASZ and WOBASZ II Studies. Oxid. Med. Cell. Longev. 2017, 2017, 5982809. [Google Scholar] [CrossRef] [PubMed]
- SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [CrossRef] [PubMed]
- SCORE2-OP risk prediction algorithms: Estimating incident cardiovascular event risk in older persons in four geographical risk regions. Eur. Heart J. 2021, 42, 2455–2467. [CrossRef] [PubMed]
- Tomas Luiz, A.; Martin Pozuelo, G.; Gonzalez Navarro, I.; Elvira Torales, L.; Ponce, H.; Gonzalez Barrio, R.; Garcia Alonso, J.; Periago, M.J. Influence of dietary carotenoids on biomarkers of cardiometabolic risk in peri- and post-menopausal women. Nutr. Hosp. 2021, 38, 993–1001. [Google Scholar] [CrossRef]
- McSorley, P.T.; Young, I.S.; Bell, P.M.; Fee, J.P.H.; McCance, D.R. Vitamin C improves endothelial function in healthy estrogen-deficient postmenopausal women. Climacteric 2003, 6, 238–247. [Google Scholar] [CrossRef]
- Naziroglu, M.; Simsek, M.; Simsek, H.; Aydilek, N.; Ozcan, Z.; Atilgan, R. The effects of hormone replacement therapy combined with vitamins C and E on antioxidants levels and lipid profiles in postmenopausal women with Type 2 diabetes. Clin. Chim. Acta 2004, 344, 63–71. [Google Scholar] [CrossRef]
- Koh, W.P.; Yuan, J.M.; Wang, R.; Lee, Y.P.; Lee, B.L.; Yu, M.C.; Ong, C.N. Plasma carotenoids and risk of acute myocardial infarction in the Singapore Chinese Health Study. Nutr. Metab. Cardiovasc. Dis. NMCD 2011, 21, 685–690. [Google Scholar] [CrossRef]
- Carr, B.R.; Khan, N.; Adams-Huet, B.; Kakarla, N.; Havelock, J.C.; Gell, J. Effect of vitamin E supplementation with and without hormone therapy on circulatory inflammatory markers in postmenopausal women. Fertil. Steril. 2006, 85, 667–673. [Google Scholar] [CrossRef]
- Riccioni, G.; D’Orazio, N.; Salvatore, C.; Franceschelli, S.; Pesce, M.; Speranza, L. Carotenoids and vitamins C and E in the prevention of cardiovascular disease. Int. J. Vitam. Nutr. Res. 2012, 82, 15–26. [Google Scholar] [CrossRef]
- Alves Luzia, L.; Mendes Aldrighi, J.; Teixeira Damasceno, N.R.; Rodrigues Sampaio, G.; Aparecida Manolio Soares, R.; Tande Silva, I.; De Queiroz Mello, A.P.; Ferreira Carioca, A.A.; Ferraz da Silva Torres, E.A. Fish Oil and Vitamin E Change Lipid Profiles and Anti-Ldl-Antibodies in Two Different Ethnic Groups of Women Transitioning Through Menopause. Nutr. Hosp. 2015, 32, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Rasool, A.H.; Rehman, A.; Wan Yusuf, W.N.; Rahman, A.R. Vitamin E and its effect on arterial stiffness in postmenopausal women--a randomized controlled trial. Int. J. Clin. Pharmacol. Ther. 2003, 41, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Salonen, J.T.; Nyyssönen, K.; Salonen, R.; Lakka, H.M.; Kaikkonen, J.; Porkkala-Sarataho, E.; Voutilainen, S.; Lakka, T.A.; Rissanen, T.; Leskinen, L.; et al. Antioxidant Supplementation in Atherosclerosis Prevention (ASAP) study: A randomized trial of the effect of vitamins E and C on 3-year progression of carotid atherosclerosis. J. Intern. Med. 2000, 248, 377–386. [Google Scholar] [CrossRef]
- Lee, D.H.; Folsom, A.R.; Jacobs, D.R., Jr. Iron, zinc, and alcohol consumption and mortality from cardiovascular diseases: The Iowa Women’s Health Study. Am. J. Clin. Nutr. 2005, 81, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.; Wang, Y.; Zhou, F.; Ruan, J.; Duan, M.; Wang, X.; Yu, Q.; Yang, P.; Chen, W.; Meng, F. Reduced Serum Zinc Ion Concentration Is Associated with Coronary Heart Disease. Biol. Trace Elem. Res. 2021, 199, 4109–4118. [Google Scholar] [CrossRef]
- Dennehy, C.; Tsourounis, C. A review of select vitamins and minerals used by postmenopausal women. Maturitas 2010, 66, 370–380. [Google Scholar] [CrossRef]
- Stranges, S.; Marshall, J.R.; Trevisan, M.; Natarajan, R.; Donahue, R.P.; Combs, G.F.; Farinaro, E.; Clark, L.C.; Reid, M.E. Effects of selenium supplementation on cardiovascular disease incidence and mortality: Secondary analyses in a randomized clinical trial. Am. J. Epidemiol. 2006, 163, 694–699. [Google Scholar] [CrossRef]
- Rayman, M.P. Food-chain selenium and human health: Emphasis on intake. Br. J. Nutr. 2008, 100, 254–268. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (n = 3109) | ASCVD (n = 453) | Non-ASCVD (n = 2656) | p-Value |
|---|---|---|---|---|
| Weighted sample size | 44,737,249 | 5,814,546 | 38,922,703 | |
| Age (years) | 64.66 ± 9.06 | 69.27 ± 8.72 | 63.97 ± 8.91 | <0.001 |
| Age distribution (years), n (%) | <0.001 | |||
| 40–49 | 80 (3.1) | 3 (0.7) | 77 (3.4) | |
| 50–59 | 803 (30.1) | 65 (15.3) | 738 (32.3) | |
| 60–69 | 1188 (36.1) | 155 (32.1) | 1033 (36.7) | |
| 70–79 | 646 (20.2) | 121 (28.8) | 525 (19.0) | |
| ≥80 | 392 (10.5) | 109 (23.1) | 283 (8.6) | |
| Race, n (%) | 0.421 | |||
| Mexican American | 390 (4.7) | 40 (3.2) | 350 (4.9) | |
| Other Hispanic | 365 (4.4) | 52 (4.1) | 313 (4.4) | |
| Non-Hispanic White | 1359 (75.1) | 234 (75.1) | 1125 (75.1) | |
| Non-Hispanic Black | 624 (9.2) | 89 (10.0) | 535 (9.1) | |
| Other Race | 371 (6.7) | 38 (7.6) | 333 (6.5) | |
| Education level, n (%) | <0.001 | |||
| Less than high school | 686 (12.3) | 125 (16.3) | 561 (11.7) | |
| High school or equivalent | 763 (26.3) | 133 (33.5) | 630 (25.2) | |
| College or above | 1660 (61.4) | 195 (50.1) | 1465 (63.1) | |
| Marital status, n (%) | <0.001 | |||
| Married | 1470 (55.0) | 165 (42.4) | 1305 (56.9) | |
| Widowed | 651 (17.9) | 151 (33.4) | 500 (15.6) | |
| Divorced | 562 (17.1) | 68 (12.5) | 494 (17.8) | |
| Separated | 117 (2.2) | 22 (2.7) | 95 (2.1) | |
| Never married | 221 (4.9) | 34 (6.2) | 187 (4.7) | |
| Living with partner | 88 (2.9) | 13 (2.9) | 75 (2.9) | |
| Ratio of family income to poverty, n (%) | <0.001 | |||
| ≤1.00 | 640 (12.1) | 114 (15.7) | 526 (11.6) | |
| 1.01–3.00 | 1357 (36.1) | 239 (51.0) | 1118 (33.9) | |
| >3.00 | 1112 (51.8) | 100 (33.3) | 1012 (54.6) | |
| BMI (kg/m2) | 29.81 ± 7.30 | 30.61 ± 7.57 | 29.69 ± 7.25 | 0.109 |
| BMI (kg/m2), n (%) | 0.125 | |||
| <18.5 | 42 (1.6) | 10 (2.3) | 32 (1.4) | |
| 18.5–24.9 | 1297 (25.4) | 179 (21.6) | 1118 (25.9) | |
| 25.0–29.9 | 356 (29.7) | 43 (26.1) | 313 (30.2) | |
| ≥30.0 | 1414 (43.4) | 221 (49.9) | 1193 (42.4) | |
| Waist circumference (cm) | 99.00 [89.30, 110.50] | 102.42 [92.45, 114.90] | 98.50 [88.50, 109.80] | 0.004 |
| Alcohol use, n (%) | 1457 (56.0) | 189 (49.5) | 1268 (57.0) | 0.038 |
| Smoking—cigarette use, n (%) | 1208 (40.3) | 227 (51.7) | 981 (38.6) | <0.001 |
| Moderate to vigorous recreational activities, n (%) | 1179 (44.2) | 124 (33.8) | 1055 (45.7) | 0.013 |
| Sleep disorders, n (%) | 1197 (42.2) | 246 (56.8) | 951 (40.1) | <0.001 |
| Hypertension, n (%) b | 1827 (53.3) | 365 (77.5) | 1462 (49.7) | <0.001 |
| Diabetes, n (%) c | 833 (20.2) | 193 (35.9) | 640 (17.9) | <0.001 |
| A family history of heart attack, n (%) | 488 (17.1) | 119 (28.2) | 369 (15.4) | <0.001 |
| NLR | 1.93 [1.48, 2.62] | 2.18 [1.62, 3.02] | 1.89 [1.47, 2.57] | 0.001 |
| HDL-C (mg/dL) | 1.00 [0.00, 1.00] | 1.00 [0.00, 1.00] | 1.00 [0.00, 1.00] | 0.004 |
| Total cholesterol (mg/dL) | 202.17 [176.00, 228.00] | 184.00 [153.00, 216.00] | 205.00 [179.00, 230.00] | <0.001 |
| Total daily caloric intake (kcal, day), n (%) | 0.091 | |||
| <1550 | 1452 (42.1) | 254 (49.5) | 1198 (41.0) | |
| 1550–1972 | 719 (25.4) | 84 (24.0) | 635 (25.6) | |
| 1973–2554 | 580 (20.1) | 78 (17.4) | 502 (20.5) | |
| ≥2555 | 358 (12.4) | 37 (9.1) | 321 (12.9) | |
| Total daily polyunsaturated fatty acids intake (gm) | 15.02 [9.64, 22.02] | 14.37 [8.68, 21.88] | 15.11 [9.73, 22.04] | 0.136 |
| Female hormone use d, n (%) | 950 (30.8) | 144 (33.7) | 806 (30.4) | 0.263 |
| Antihypertensive medication use e, n (%) | 1596 (45.7) | 330 (69.8) | 1266 (42.1) | <0.001 |
| Lipid-lowering medication use f, n (%) | 1107 (36.0) | 257 (39.0) | 850 (35.5) | 0.304 |
| Antidiabetic medication use g, n (%) | 625 (13.4) | 149 (21.3) | 476 (12.2) | <0.001 |
| CDAI | −0.18 [−2.27, 2.46] | −1.14 [−3.05, 1.32] | −0.05 [−2.16, 2.56] | <0.001 |
| CDAI | Model A | Model B | Model C | |||
|---|---|---|---|---|---|---|
| ASCVD | Hard Criteria b | ASCVD | Hard Criteria b | ASCVD | Hard Criteria b | |
| As continuous (per SD) | 0.65 (0.53, 0.80) *** | 0.61 (0.50, 0.75) *** | 0.71 (0.58, 0.87) *** | 0.67 (0.54, 0.83) *** | 0.67 (0.51, 0.88) ** | 0.61 (0.46, 0.81) *** |
| By cut-off | ||||||
| Low | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| High | 0.60 (0.45, 0.80) *** | 0.57 (0.44, 0.73) *** | 0.68 (0.51, 0.90) ** | 0.65 (0.50, 0.83) ** | 0.71 (0.50, 0.98) * | 0.65 (0.48, 0.89) ** |
| Interquartile | ||||||
| Quartile 1 (−6.83–−1.04) | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Quartile 2 (−1.04–1.11) | 0.63 (0.43, 0.91) * | 0.69 (0.45, 1.06) | 0.65 (0.46, 0.93) * | 0.79 (0.49, 1.12) | 0.63 (0.44, 0.90) * | 0.70 (0.46, 1.08) |
| Quartile 3 (1.11–3.72) | 0.60 (0.41, 0.88) ** | 0.68 (0.46, 1.00) * | 0.69 (0.48, 1.00) * | 0.74 (0.54, 1.06) | 0.64 (0.42, 0.94) * | 0.70 (0.46, 1.02) |
| Quartile 4 (3.72–43.87) | 0.44 (0.26, 0.72) ** | 0.32 (0.18, 0.54) *** | 0.52 (0.31, 0.89) * | 0.38 (0.22, 0.68) ** | 0.51 (0.27, 0.97) * | 0.33 (0.16, 0.69) ** |
| p-trend | 0.002 | <0.001 | 0.022 | 0.002 | 0.042 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.; Lai, W.; Zhao, M.; Zhang, Y.; Hu, Y. Association between the Composite Dietary Antioxidant Index and Atherosclerotic Cardiovascular Disease in Postmenopausal Women: A Cross-Sectional Study of NHANES Data, 2013–2018. Antioxidants 2023, 12, 1740. https://doi.org/10.3390/antiox12091740
Liu C, Lai W, Zhao M, Zhang Y, Hu Y. Association between the Composite Dietary Antioxidant Index and Atherosclerotic Cardiovascular Disease in Postmenopausal Women: A Cross-Sectional Study of NHANES Data, 2013–2018. Antioxidants. 2023; 12(9):1740. https://doi.org/10.3390/antiox12091740
Chicago/Turabian StyleLiu, Chenning, Wenyu Lai, Meiduo Zhao, Yexuan Zhang, and Yuanjia Hu. 2023. "Association between the Composite Dietary Antioxidant Index and Atherosclerotic Cardiovascular Disease in Postmenopausal Women: A Cross-Sectional Study of NHANES Data, 2013–2018" Antioxidants 12, no. 9: 1740. https://doi.org/10.3390/antiox12091740
APA StyleLiu, C., Lai, W., Zhao, M., Zhang, Y., & Hu, Y. (2023). Association between the Composite Dietary Antioxidant Index and Atherosclerotic Cardiovascular Disease in Postmenopausal Women: A Cross-Sectional Study of NHANES Data, 2013–2018. Antioxidants, 12(9), 1740. https://doi.org/10.3390/antiox12091740