
Treatment with PCSK9 Inhibitor Evolocumab Improves Vascular Oxidative Stress and Arterial Stiffness in Hypercholesterolemic Patients with High Cardiovascular Risk
 ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals
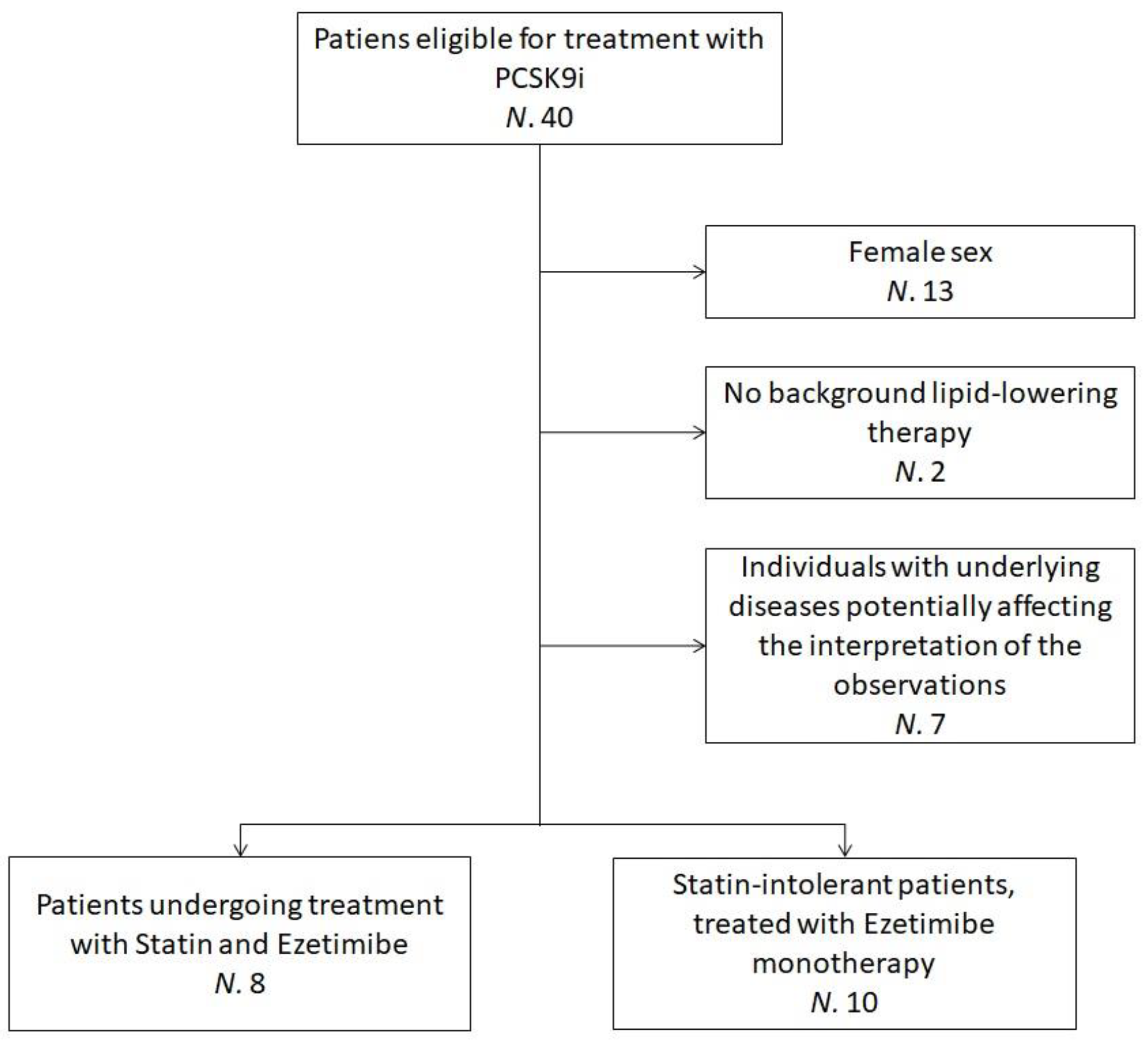
2.2. Study Population
2.3. Treatment
2.4. Assessments
2.4.1. Clinical Assessments
2.4.2. Biochemical Analyses
2.4.3. Blood Pressure Measurements
2.4.4. Non-Invasive Vascular Tests
2.5. H2O2Bioassay Procedure
2.5.1. PBMCs Collection
2.5.2. Quantification of Intracellular H2O2 in PBMCs
2.6. Cell Viability Assay
2.7. Data Analysis
3. Results and Discussion
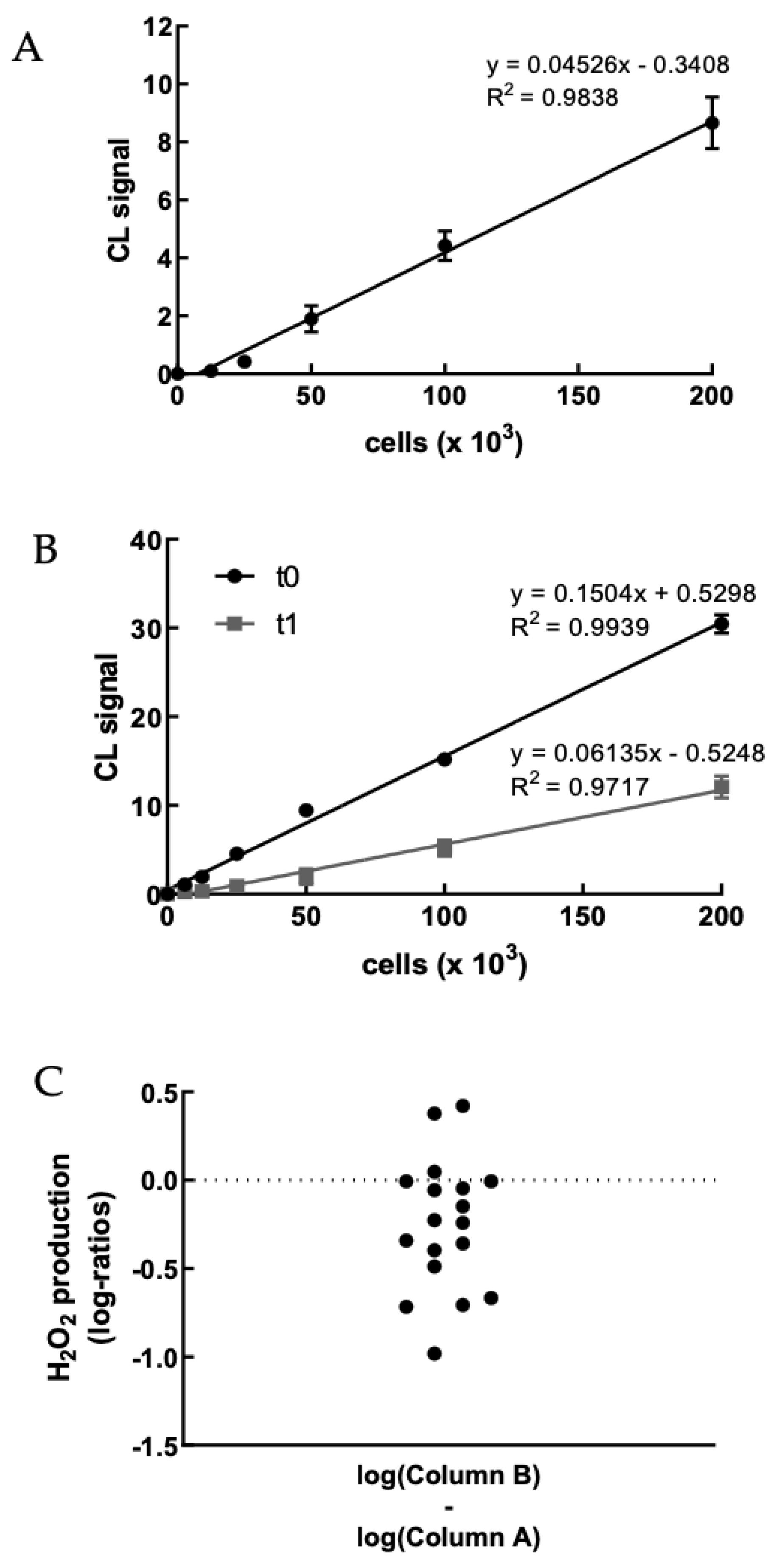
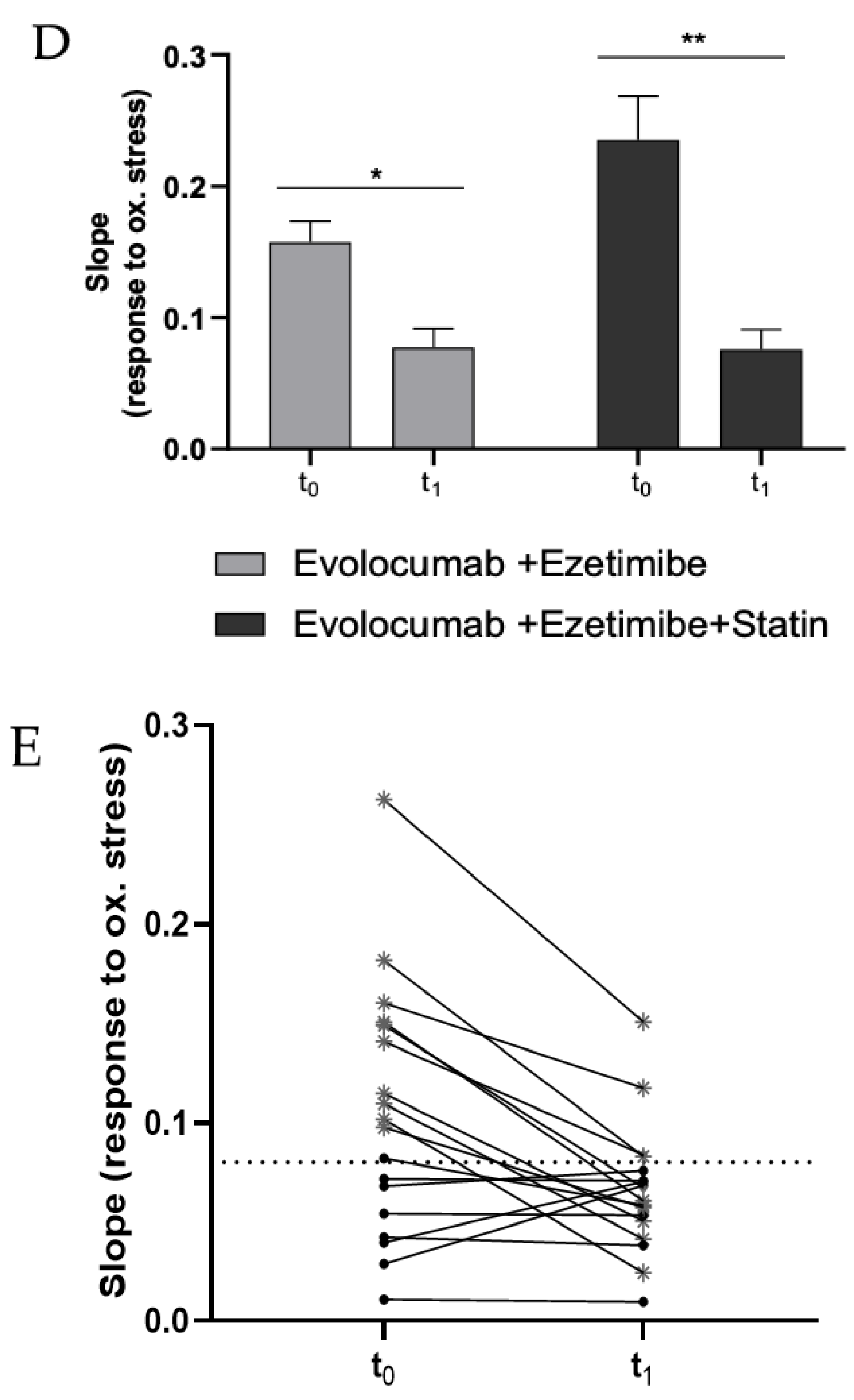
3.1. Evolocumab Treatment Decreases Intracellular H2O2Production in PBMCs
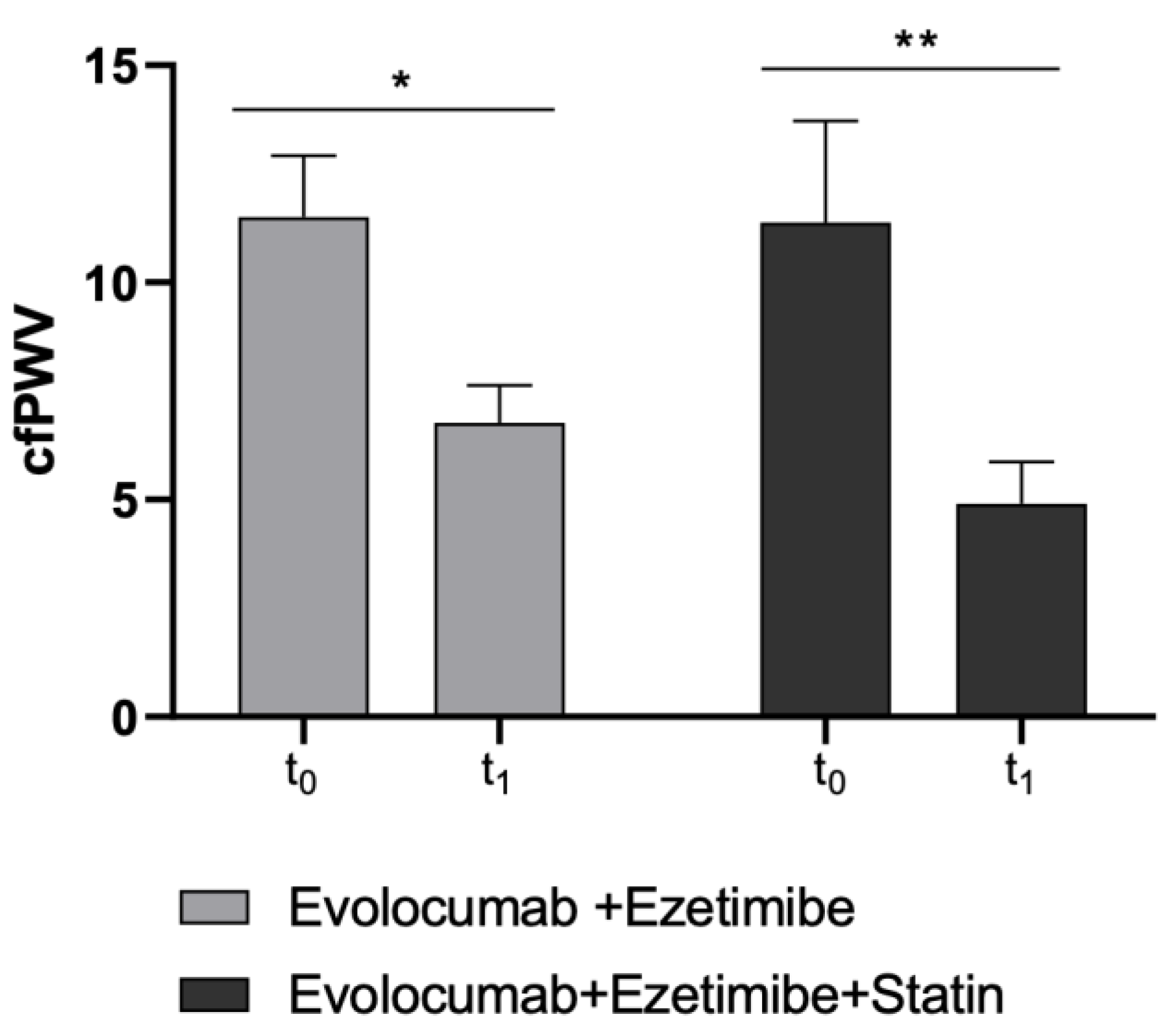
3.2. Plasma Lipids and Arterial Stiffness Improvement after Treatment with Evolocumab
3.3. H2O2 Decrease Correlates with Arterial Stiffness Improvement
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Touyz, R.M.; Rios, F.J.; Alves-Lopes, R.; Neves, K.B.; Camargo, L.L.; Montezano, A.C. Oxidative Stress: A Unifying Paradigm in Hypertension. Can. J. Cardiol. 2020, 36, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart Disease and Stroke Statistics—2012 Update. Circulation 2012, 125, e2–e220. [Google Scholar] [CrossRef]
- Martin-Ventura, J.; Rodrigues-Diez, R.; Martinez-Lopez, D.; Salaices, M.; Blanco-Colio, L.; Briones, A. Oxidative Stress in Human Atherothrombosis: Sources, Markers and Therapeutic Targets. Int. J. Mol. Sci. 2017, 18, 2315. [Google Scholar] [CrossRef]
- Benn, M.; Watts, G.F.; Tybjærg-Hansen, A.; Nordestgaard, B.G. Mutations Causative of Familial Hypercholesterolaemia: Screening of 98098 Individuals from the Copenhagen General Population Study Estimated a Prevalence of 1 in 217. Eur. Heart J. 2016, 37, 1384–1394. [Google Scholar] [CrossRef]
- Presta, V.; Figliuzzi, I.; Miceli, F.; Coluccia, R.; Fogacci, F.; Cicero, A.F.G.; Ferrucci, A.; Borghi, C.; Volpe, M.; Tocci, G.; et al. Achievement of Low Density Lipoprotein (LDL) Cholesterol Targets in Primary and Secondary Prevention: Analysis of a Large Real Practice Database in Italy. Atherosclerosis 2019, 285, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, D. The LDL Modification Hypothesis of Atherogenesis: An Update. J. Lipid Res. 2009, 50, S376–S381. [Google Scholar] [CrossRef] [PubMed]
- Mollazadeh, H.; Carbone, F.; Montecucco, F.; Pirro, M.; Sahebkar, A. Oxidative Burden in Familial Hypercholesterolemia. J. Cell. Physiol. 2018, 233, 5716–5725. [Google Scholar] [CrossRef] [PubMed]
- Marks, D.; Thorogood, M.; Neil, H.A.W.; Humphries, S.E. A Review on the Diagnosis, Natural History, and Treatment of Familial Hypercholesterolaemia. Atherosclerosis 2003, 168, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, M.D.; Tavori, H.; Fazio, S. PCSK9. Circ. Res. 2018, 122, 1420–1438. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Raal, F.J.; Stein, E.A.; Dufour, R.; Turner, T.; Civeira, F.; Burgess, L.; Langslet, G.; Scott, R.; Olsson, A.G.; Sullivan, D.; et al. PCSK9 Inhibition with Evolocumab (AMG 145) in Heterozygous Familial Hypercholesterolaemia (RUTHERFORD-2): A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2015, 385, 331–340. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Toth, P.P.; Fogacci, F.; Virdis, A.; Borghi, C. Improvement in Arterial Stiffness after Short-Term Treatment with PCSK9 Inhibitors. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 527–529. [Google Scholar] [CrossRef]
- Mandraffino, G.; Scicali, R.; Rodríguez-Carrio, J.; Savarino, F.; Mamone, F.; Scuruchi, M.; Cinquegrani, M.; Imbalzano, E.; di Pino, A.; Piro, S.; et al. Arterial Stiffness Improvement after Adding on PCSK9 Inhibitors or Ezetimibe to High-Intensity Statins in Patients with Familial Hypercholesterolemia: A Two–Lipid Center Real-World Experience. J. Clin. Lipidol. 2020, 14, 231–240. [Google Scholar] [CrossRef]
- Punch, E.; Klein, J.; Diaba-Nuhoho, P.; Morawietz, H.; Garelnabi, M. Effects of PCSK9 Targeting: Alleviating Oxidation, Inflammation, and Atherosclerosis. J. Am. Heart Assoc. 2022, 11, e023328. [Google Scholar] [CrossRef]
- Tang, Z.-H.; Peng, J.; Ren, Z.; Yang, J.; Li, T.-T.; Li, T.-H.; Wang, Z.; Wei, D.-H.; Liu, L.-S.; Zheng, X.-L.; et al. New Role of PCSK9 in Atherosclerotic Inflammation Promotion Involving the TLR4/NF-ΚB Pathway. Atherosclerosis 2017, 262, 113–122. [Google Scholar] [CrossRef]
- Cammisotto, V.; Baratta, F.; Simeone, P.G.; Barale, C.; Lupia, E.; Galardo, G.; Santilli, F.; Russo, I.; Pignatelli, P. Proprotein Convertase Subtilisin Kexin Type 9 (PCSK9) Beyond Lipids: The Role in Oxidative Stress and Thrombosis. Antioxidants 2022, 11, 569. [Google Scholar] [CrossRef]
- Safaeian, L.; Mirian, M.; Bahrizadeh, S. Evolocumab, a PCSK9 Inhibitor, Protects Human Endothelial Cells against H2O2 -Induced Oxidative Stress. Arch. Physiol. Biochem. 2022, 128, 1681–1686. [Google Scholar] [CrossRef] [PubMed]
- Swirski, F.K.; Nahrendorf, M. Leukocyte Behavior in Atherosclerosis, Myocardial Infarction, and Heart Failure. Science (1979) 2013, 339, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Rubattu, S.; Forte, M.; Raffa, S. Circulating Leukocytes and Oxidative Stress in Cardiovascular Diseases: A State of the Art. Oxid. Med. Cell. Longev. 2019, 2019, 2650429. [Google Scholar] [CrossRef] [PubMed]
- De Mello, V.D.F.; Kolehmanien, M.; Schwab, U.; Pulkkinen, L.; Uusitupa, M. Gene Expression of Peripheral Blood Mononuclear Cells as a Tool in Dietary Intervention Studies: What Do We Know so Far? Mol. Nutr. Food Res. 2012, 56, 1160–1172. [Google Scholar] [CrossRef]
- Shirakawa, R.; Yokota, T.; Nakajima, T.; Takada, S.; Yamane, M.; Furihata, T.; Maekawa, S.; Nambu, H.; Katayama, T.; Fukushima, A.; et al. Mitochondrial Reactive Oxygen Species Generation in Blood Cells Is Associated with Disease Severity and Exercise Intolerance in Heart Failure Patients. Sci. Rep. 2019, 9, 14709. [Google Scholar] [CrossRef]
- Alfatni, A.; Riou, M.; Charles, A.-L.; Meyer, A.; Barnig, C.; Andres, E.; Lejay, A.; Talha, S.; Geny, B. Peripheral Blood Mononuclear Cells and Platelets Mitochondrial Dysfunction, Oxidative Stress, and Circulating MtDNA in Cardiovascular Diseases. J. Clin. Med. 2020, 9, 311. [Google Scholar] [CrossRef]
- Wenzel, P.; Knorr, M.; Kossmann, S.; Stratmann, J.; Hausding, M.; Schuhmacher, S.; Karbach, S.H.; Schwenk, M.; Yogev, N.; Schulz, E.; et al. Lysozyme M–Positive Monocytes Mediate Angiotensin II–Induced Arterial Hypertension and Vascular Dysfunction. Circulation 2011, 124, 1370–1381. [Google Scholar] [CrossRef]
- Forte, M.; Nocella, C.; de Falco, E.; Palmerio, S.; Schirone, L.; Valenti, V.; Frati, G.; Carnevale, R.; Sciarretta, S. The Pathophysiological Role of NOX2 in Hypertension and Organ Damage. High Blood Press. Cardiovasc. Prev. 2016, 23, 355–364. [Google Scholar] [CrossRef]
- Catapano, A.L.; Graham, I.; de Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Rev. Esp. Cardiol. (Engl. Ed.) 2017, 70, 115. [Google Scholar] [CrossRef] [PubMed]
- AIFA (Italian Medicines Agency). Classificazione del Medicinale per uso Umano «Repatha», ai Sensi dell’art. 8, Comma 10, Della Legge 24 Dicembre 1993, n. 537. (Determina n. 172/2017). Available online: https://www.gazzettaufficiale.it/eli/id/2017/02/07/17A01047/s#:~:text=%C2%ABRepatha%C2%BB%20e’%20indicato%20nei,C%20target%20con%20la%20dose (accessed on 2 December 2022).
- Fogacci, F.; Giovannini, M.; Grandi, E.; Imbalzano, E.; Degli Esposti, D.; Borghi, C.; Cicero, A.F.G. Management of High-Risk Hypercholesterolemic Patients and PCSK9 Inhibitors Reimbursement Policies: Data from a Cohort of Italian Hypercholesterolemic Outpatients. J. Clin. Med. 2022, 11, 4701. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Veronesi, M.; Strocchi, E.; Grandi, E.; Rizzoli, E.; Poli, A.; Marangoni, F.; Borghi, C. A Randomized Placebo-Controlled Clinical Trial to Evaluate the Medium-Term Effects of Oat Fibers on Human Health: The Beta-Glucan Effects on Lipid Profile, Glycemia and InTestinal Health (BELT) Study. Nutrients 2020, 12, 686. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Giovannini, M.; Grandi, E.; D’Addato, S.; Borghi, C. Interaction between Low-Density Lipoprotein-Cholesterolaemia, Serum Uric Level and Incident Hypertension. J. Hypertens. 2019, 37, 728–731. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; de Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.S.; Protogerou, A.D.; et al. Expert Consensus Document on the Measurement of Aortic Stiffness in Daily Practice Using Carotid-Femoral Pulse Wave Velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef]
- Marque, V.; van Essen, H.; Struijker-Boudier, H.A.J.; Atkinson, J.; Lartaud-Idjouadiene, I. Determination of Aortic Elastic Modulus by Pulse Wave Velocity and Wall Tracking in a Rat Model of Aortic Stiffness. J. Vasc. Res. 2001, 38, 546–550. [Google Scholar] [CrossRef]
- Hirata, K.; Kawakami, M.; O’Rourke, M.F. Pulse Wave Analysis and Pulse Wave Velocity A Review of Blood Pressure Interpretation 100 Years After Korotkov. Circulation 2006, 70, 1231–1239. [Google Scholar] [CrossRef] [PubMed]
- Hickson, S.S.; Butlin, M.; Broad, J.; Avolio, A.P.; Wilkinson, I.B.; McEniery, C.M. Validity and Repeatability of the Vicorder Apparatus: A Comparison with the SphygmoCor Device. Hypertens. Res. 2009, 32, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.R.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and Interpretation of the Ankle-Brachial Index. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [PubMed]
- Samba, H.; Guerchet, M.; Ndamba-Bandzouzi, B.; Kehoua, G.; Mbelesso, P.; Desormais, I.; Aboyans, V.; Preux, P.-M.; Lacroix, P. Ankle Brachial Index (ABI) Predicts 2-Year Mortality Risk among Older Adults in the Republic of Congo: The EPIDEMCA-FU Study. Atherosclerosis 2019, 286, 121–127. [Google Scholar] [CrossRef]
- Bua, G.; Manaresi, E.; Bonvicini, F.; Gallinella, G. Parvovirus B19 Replication and Expression in Differentiating Erythroid Progenitor Cells. PLoS ONE 2016, 11, e0148547. [Google Scholar] [CrossRef]
- Hananya, N.; Shabat, D. Recent Advances and Challenges in Luminescent Imaging: Bright Outlook for Chemiluminescence of Dioxetanes in Water. ACS Cent. Sci. 2019, 5, 949–959. [Google Scholar] [CrossRef]
- Green, O.; Gnaim, S.; Blau, R.; Eldar-Boock, A.; Satchi-Fainaro, R.; Shabat, D. Near-Infrared Dioxetane Luminophores with Direct Chemiluminescence Emission Mode. J. Am. Chem. Soc. 2017, 139, 13243–13248. [Google Scholar] [CrossRef]
- Caliceti, C.; Rizzo, P.; Ferrari, R.; Fortini, F.; Aquila, G.; Leoncini, E.; Zambonin, L.; Rizzo, B.; Calabria, D.; Simoni, P.; et al. Novel Role of the Nutraceutical Bioactive Compound Berberine in Lectin-like OxLDL Receptor 1-Mediated Endothelial Dysfunction in Comparison to Lovastatin. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 552–563. [Google Scholar] [CrossRef]
- Calabria, D.; Guardigli, M.; Mirasoli, M.; Punzo, A.; Porru, E.; Zangheri, M.; Simoni, P.; Pagnotta, E.; Ugolini, L.; Lazzeri, L.; et al. Selective Chemiluminescent TURN-ON Quantitative Bioassay and Imaging of Intracellular Hydrogen Peroxide in Human Living Cells. Anal. Biochem. 2020, 600, 113760. [Google Scholar] [CrossRef]
- ClinLab Navigator. HemoLink Blood Collection Device. Available online: http://www.clinlabnavigator.com/hemolink-blood-collection-device.html (accessed on 24 December 2022).
- Yasunari, K.; Watanabe, T.; Nakamura, M. Reactive Oxygen Species Formation by Polymorphonuclear Cells and Mononuclear Cells as a Risk Factor of Cardiovascular Diseases. Curr. Pharm. Biotechnol. 2006, 7, 73–80. [Google Scholar] [CrossRef]
- Yasunari, K.; Maeda, K.; Nakamura, M.; Watanabe, T.; Yoshikawa, J. Benidipine, a Long-Acting Calcium Channel Blocker, Inhibits Oxidative Stress in Polymorphonuclear Cells in Patients with Essential Hypertension. Hypertens. Res. 2005, 28, 107–112. [Google Scholar] [CrossRef] [PubMed]
- IJsselmuiden, A.J.; Musters, R.J.; de Ruiter, G.; van Heerebeek, L.; Alderse-Baas, F.; van Schilfgaarde, M.; Leyte, A.; Tangelder, G.-J.; Laarman, G.J.; Paulus, W.J. Circulating White Blood Cells and Platelets Amplify Oxidative Stress in Heart Failure. Nat. Clin. Pract. Cardiovasc. Med. 2008, 5, 811–820. [Google Scholar] [CrossRef]
- Leu, H.-B.; Lin, C.-P.; Lin, W.-T.; Wu, T.-C.; Lin, S.-J.; Chen, J.-W. Circulating Mononuclear Superoxide Production and Inflammatory Markers for Long-Term Prognosis in Patients with Cardiac Syndrome X. Free Radic. Biol. Med. 2006, 40, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Song, B.; Li, T.; Chen, S.; Yang, D.; Luo, L.; Wang, T.; Han, X.; Bai, L.; Ma, A. Correlations between MTP and ROS Levels of Peripheral Blood Lymphocytes and Readmission in Patients with Chronic Heart Failure. Heart Lung Circ. 2016, 25, 296–302. [Google Scholar] [CrossRef]
- Wilking, M.; Ndiaye, M.; Mukhtar, H.; Ahmad, N. Circadian rhythm connections to oxidative stress: Implications for human health. Antioxid. Redox Signal. 2013, 19, 192–208. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Kataoka, Y.; Nissen, S.E.; Prati, F.; Windecker, S.; Puri, R.; Hucko, T.; Aradi, D.; Herrman, J.R.; Hermanides, R.S.; et al. Effect of Evolocumab on Coronary Plaque Phenotype and Burden in Statin-Treated Patients Following Myocardial Infarction. JACC Cardiovasc. Imaging 2022, 15, 1308–1321. [Google Scholar] [CrossRef] [PubMed]
- Maulucci, G.; Cipriani, F.; Russo, D.; Casavecchia, G.; di Staso, C.; di Martino, L.; Ruggiero, A.; di Biase, M.; Brunetti, N.D. Improved Endothelial Function after Short-Term Therapy with Evolocumab. J. Clin. Lipidol. 2018, 12, 669–673. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Terentes-Printzios, D.; Ioakeimidis, N.; Stefanadis, C. Prediction of Cardiovascular Events and All-Cause Mortality with Brachial-Ankle Elasticity Index. Hypertension 2012, 60, 556–562. [Google Scholar] [CrossRef]
- Yubero-Serrano, E.M.; Delgado-Lista, J.; Peña-Orihuela, P.; Perez-Martinez, P.; Fuentes, F.; Marin, C.; Tunez, I.; Tinahones, F.J.; Perez-Jimenez, F.; Roche, H.M.; et al. Oxidative stress is associated with the number of components of metabolic syndrome: LIPGENE study. Exp. Mol. Med. 2013, 45, e28. [Google Scholar] [CrossRef]
- Farinha, J.B.; Steckling, F.M.; Stefanello, S.T.; Cardoso, M.S.; Nunes, L.S.; Barcelos, R.P.; Duarte, T.; Kretzmann, N.A.; Mota, C.B.; Bresciani, G.; et al. Response of oxidative stress and inflammatory biomarkers to a 12-week aerobic exercise training in women with metabolic syndrome. Sports Med. Open 2015, 1, 19. [Google Scholar] [CrossRef] [PubMed]
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic Effects of Statins on the Cardiovascular System. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Statin and Ezetimibe (N = 8) | Ezetimibe (N = 10) |
|---|---|---|
| Age (years)—mean ± SD | 63.2 ± 7.3 | 69.4 ± 4.9 |
| Active smokers—% | 37.5 | 10 |
| Heterozygous FH—% | 62.5 | 30 |
| Primary cardiovascular prevention—% | 25 | 40 |
| Secondary cardiovascular prevention—% | 75 | 60 |
| Cardiovascular disease—% | 75 | 40 |
| Cerebrovascular disease—% | 0 | 10 |
| Peripheral obliterative arterial disease—% | 12.5 | 20 |
| Type 2 diabetes—% | 0 | 20 |
| Hypertension—% | 50 | 70 |
| History of statin intolerance—% | 50 | 80 |
| Low-dose * statin treatment—% | 50 | 0 |
| High-dose § statin treatment—% | 50 | 0 |
| n-3 PUFA treatment—% | 25 | 0 |
| Urate-lowering treatment—% | 12.5 | 10 |
| Parameters | Statin and Ezetimibe (N = 8) | Ezetimibe (N = 10) | ||
|---|---|---|---|---|
| Baseline (Mean ± SD) | Follow-Up (Mean ± SD) | Baseline (Mean ± SD) | Follow-Up (Mean ± SD) | |
| Fasting plasma glucose—mg/dL | 94.13 ± 5.08 | 93.4 ± 8 | 93.6 ± 10.04 | 99.6 ± 14.48 |
| Creatinine—mg/dL | 0.81 ± 0.13 | 0.78 ± 0.15 | 0.95 ± 0.16 | 1 ± 0.18 |
| eGFR—mL/min/1.73 m2 | 89.16 ± 17.11 | 90.63 ± 18.52 | 73.78 ± 15.34 | 68.11 ± 16.09 |
| Serum uric acid—mg/dL | 5.05 ± 0.93 | 4.61 ± 0.85 * | 5.86 ± 0.91 | 6 ± 0.98 |
| Total cholesterol—mg/dL | 212.88 ± 35.92 | 111.75 ± 12.15 * | 247.4 ± 85.19 | 138.3 ± 60.73 * |
| Triglyceride—mg/dL | 137.75 ± 93.23 | 106.5 ± 64.36 * | 138.7 ± 66.67 | 153 ± 150.69 |
| HDL-cholesterol—mg/dL | 58 ± 13.22 | 58 ± 11.87 | 56.2 ± 12.47 | 55.2 ± 13.58 |
| Non-HDL-cholesterol—mg/dL | 154.88 ± 32.99 | 53.75 ± 8.88 * | 191.2 ± 78.63 | 83.1 ± 52.84 * |
| LDL-cholesterol—mg/dL | 132.54 ± 35.94 | 33.4 ± 12.92 * | 163.46 ± 78.16 | 52.5 ± 55.33 * |
| VLDL-cholesterol—mg/dL | 28.03 ± 20.09 | 21.31 ± 13.9 * | 28.16 ± 14.07 | 32.07 ± 31.59 |
| Apolipoprotein-B—mg/dL | 147.2 ± 47.8 | 53 ± 20.48 * | 148 ± 41.12 | 53.63 ± 33.62 * |
| Lipoprotein(a)—mg/dL | 95.72 ± 92.62 | 67.06 ± 58.42 | 42.05 ± 54.45 | 30.79 ± 42.15 * |
| Total bilirubin—mg/dL | 0.5 ± 0.07 | 0.54 ± 0.12 | 0.64 ± 0.18 | 0.58 ± 0.21 |
| Direct bilirubin—mg/dL | 0.13 ± 0.04 | 0.16 ± 0.09 | 0.11 ± 0.03 | 0.13 ± 0.05 * |
| Indirect bilirubin—mg/dL | 0.37 ± 0.05 | 0.37 ± 0.06 | 0.54 ± 0.15 | 0.46 ± 0.17 |
| Aspartate aminotransferase—U/L | 25.71 ± 7.7 | 26.71 ± 8.73 | 33.2 ± 24.79 | 31.9 ± 26.59 |
| Alanine aminotransferase—U/L | 24.13 ± 10.26 | 23.5 ± 9.93 | 27.4 ± 14.97 | 24.6 ± 16.15 |
| Gamma-glutamyl transferase—U/L | 36 ± 51.8 | 45.13 ± 82.16 | 32.5 ± 23.63 | 29.8 ± 13.74 |
| Creatine phosphokinase—U/L | 125.25 ± 78.04 | 150.38 ± 95.58 | 393.8 ± 392.8 | 361.2 ± 398.3 |
| Thyroid-stimulating hormone—μU/mL | 1.92 ± 1.09 | 2.06 ± 1.2 | 2.44 ± 0.77 | 2.03 ± 0.38 |
| Parameters | Statin and Ezetimibe (N = 8) | Ezetimibe (N = 10) | ||
|---|---|---|---|---|
| Baseline (Mean ± SD) | Follow-Up (Mean ± SD) | Baseline (Mean ± SD) | Follow-Up (Mean ± SD) | |
| Heart rate—bpm | 67.13 ± 13 | 68.75 ± 8.19 | 62.8 ± 7.18 | 64.1 ± 10.04 |
| Systolic blood pressure—mmHg | 135.13 ± 14.29 | 148.13 ± 17.76 * | 142.3 ± 20.87 | 153 ± 14.31 |
| Diastolic blood pressure—mmHg | 70.5 ± 10.3 | 71.1 ± 10.5 | 70.1 ± 11.1 | 75.4 ± 8.1 |
| Pulse wave velocity—m/s | 11.39 ± 1.26 | 4.91 ± 2.7 ** | 11.5 ± 1.9 | 6.77 ± 2.71 * |
| Ankle–brachial index (right) | 1.06 ± 0.06 | 1.1 ± 0.15 | 0.91 ± 0.23 | 1.08 ± 0.07 |
| Ankle–brachial index (left) | 1.02 ± 0.18 | 1.06 ± 0.21 | 0.98 ± 0.19 | 1.1 ± 0.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silla, A.; Fogacci, F.; Punzo, A.; Hrelia, S.; Simoni, P.; Caliceti, C.; Cicero, A.F.G. Treatment with PCSK9 Inhibitor Evolocumab Improves Vascular Oxidative Stress and Arterial Stiffness in Hypercholesterolemic Patients with High Cardiovascular Risk. Antioxidants 2023, 12, 578. https://doi.org/10.3390/antiox12030578
Silla A, Fogacci F, Punzo A, Hrelia S, Simoni P, Caliceti C, Cicero AFG. Treatment with PCSK9 Inhibitor Evolocumab Improves Vascular Oxidative Stress and Arterial Stiffness in Hypercholesterolemic Patients with High Cardiovascular Risk. Antioxidants. 2023; 12(3):578. https://doi.org/10.3390/antiox12030578
Chicago/Turabian StyleSilla, Alessia, Federica Fogacci, Angela Punzo, Silvana Hrelia, Patrizia Simoni, Cristiana Caliceti, and Arrigo F. G. Cicero. 2023. "Treatment with PCSK9 Inhibitor Evolocumab Improves Vascular Oxidative Stress and Arterial Stiffness in Hypercholesterolemic Patients with High Cardiovascular Risk" Antioxidants 12, no. 3: 578. https://doi.org/10.3390/antiox12030578
APA StyleSilla, A., Fogacci, F., Punzo, A., Hrelia, S., Simoni, P., Caliceti, C., & Cicero, A. F. G. (2023). Treatment with PCSK9 Inhibitor Evolocumab Improves Vascular Oxidative Stress and Arterial Stiffness in Hypercholesterolemic Patients with High Cardiovascular Risk. Antioxidants, 12(3), 578. https://doi.org/10.3390/antiox12030578