
The Anti-Inflammatory and Antioxidant Impact of Dietary Fatty Acids in Cardiovascular Protection in Older Adults May Be Related to Vitamin C Intake

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design and Measurements
2.3. Statistical Analysis
3. Results
3.1. Baseline Group Characteristics
3.2. Nutritional Characteristics
3.3. C-Reactive Protein of Saliva, and Plasma and Salivary Antioxidant Parameters
3.4. Correlations for Fatty Acids Intake, and Plasma and Salivary Antioxidant Parameters
3.4.1. Antioxidant Parameters vs. Fatty Acid Intake in the Study Group (n = 80)
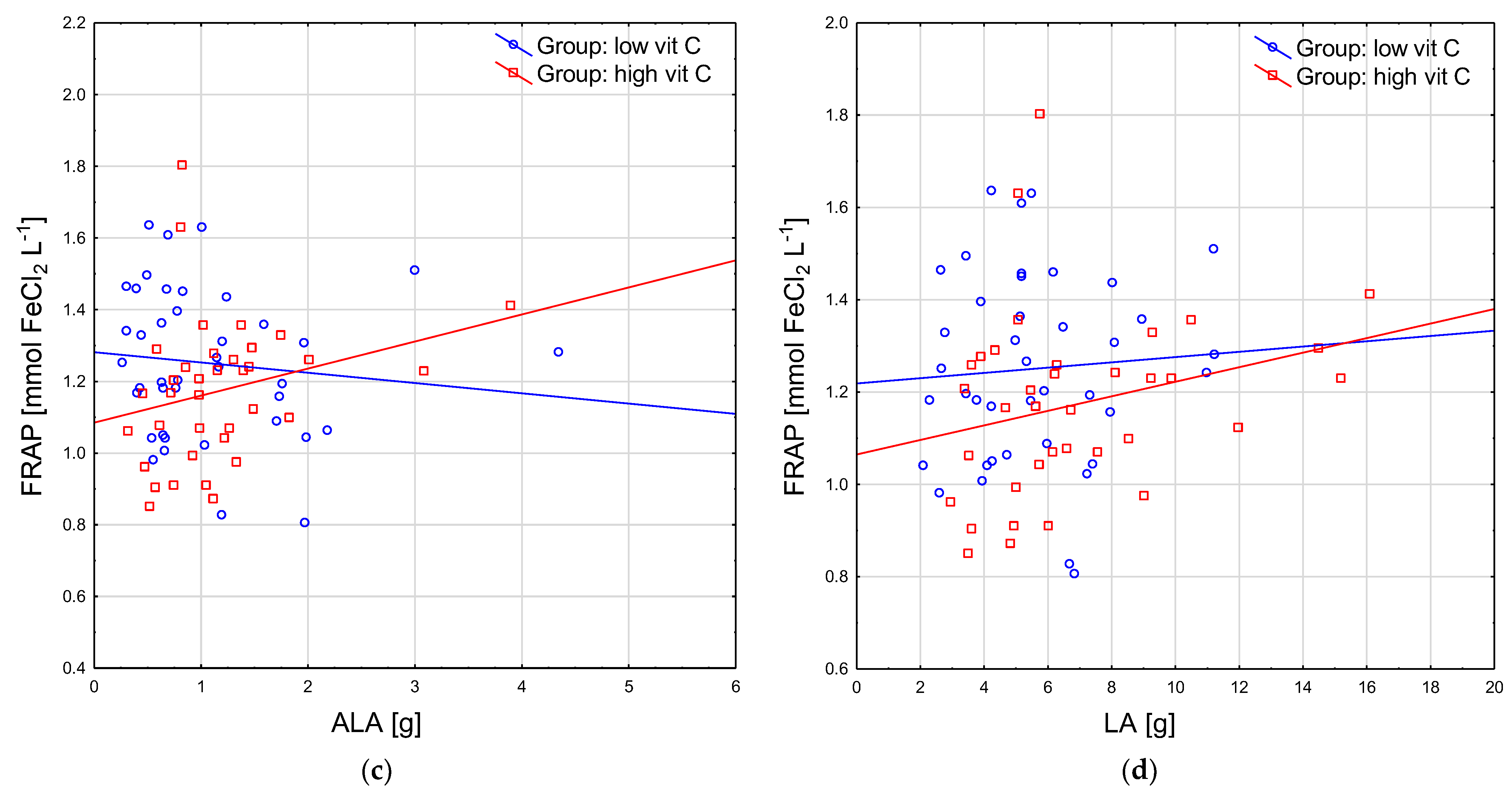
3.4.2. Plasma Antioxidant Parameters vs. Fatty Acid Intake in Groups with High and Low Vitamin C Intake
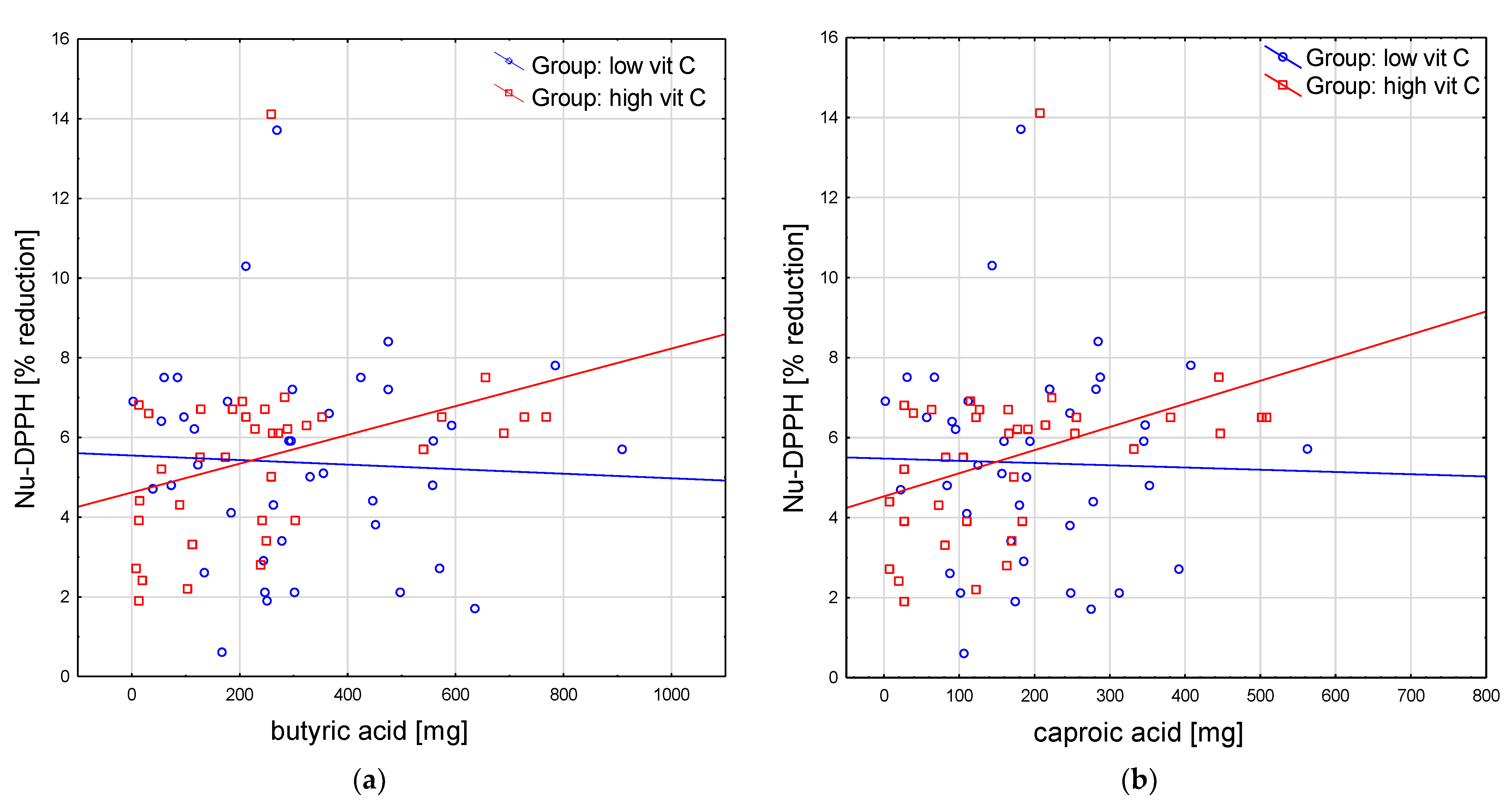
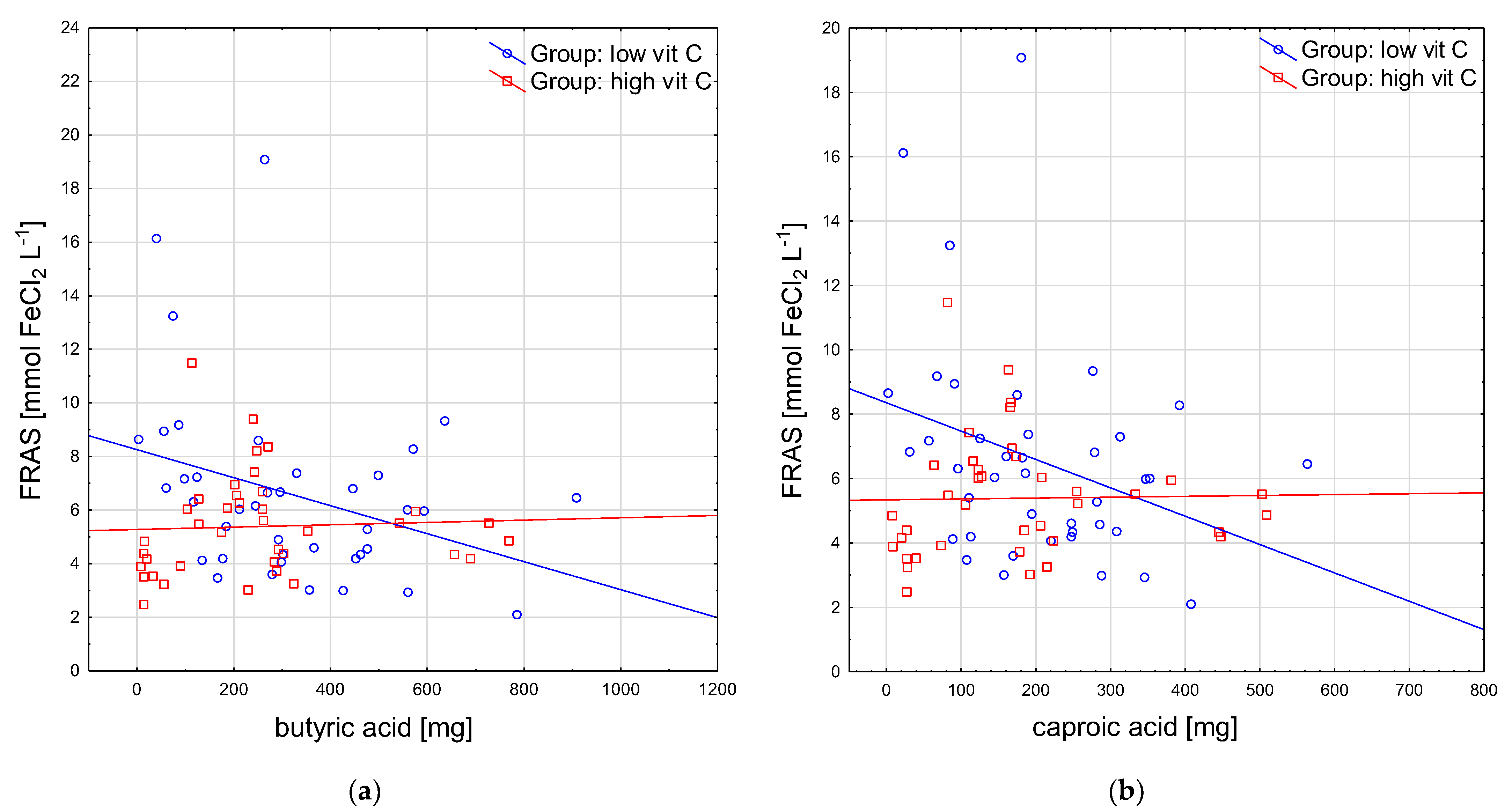
3.4.3. Salivary Antioxidant Parameters vs. Fatty Acid Intake in the Groups with High and Low Vitamin C Intake
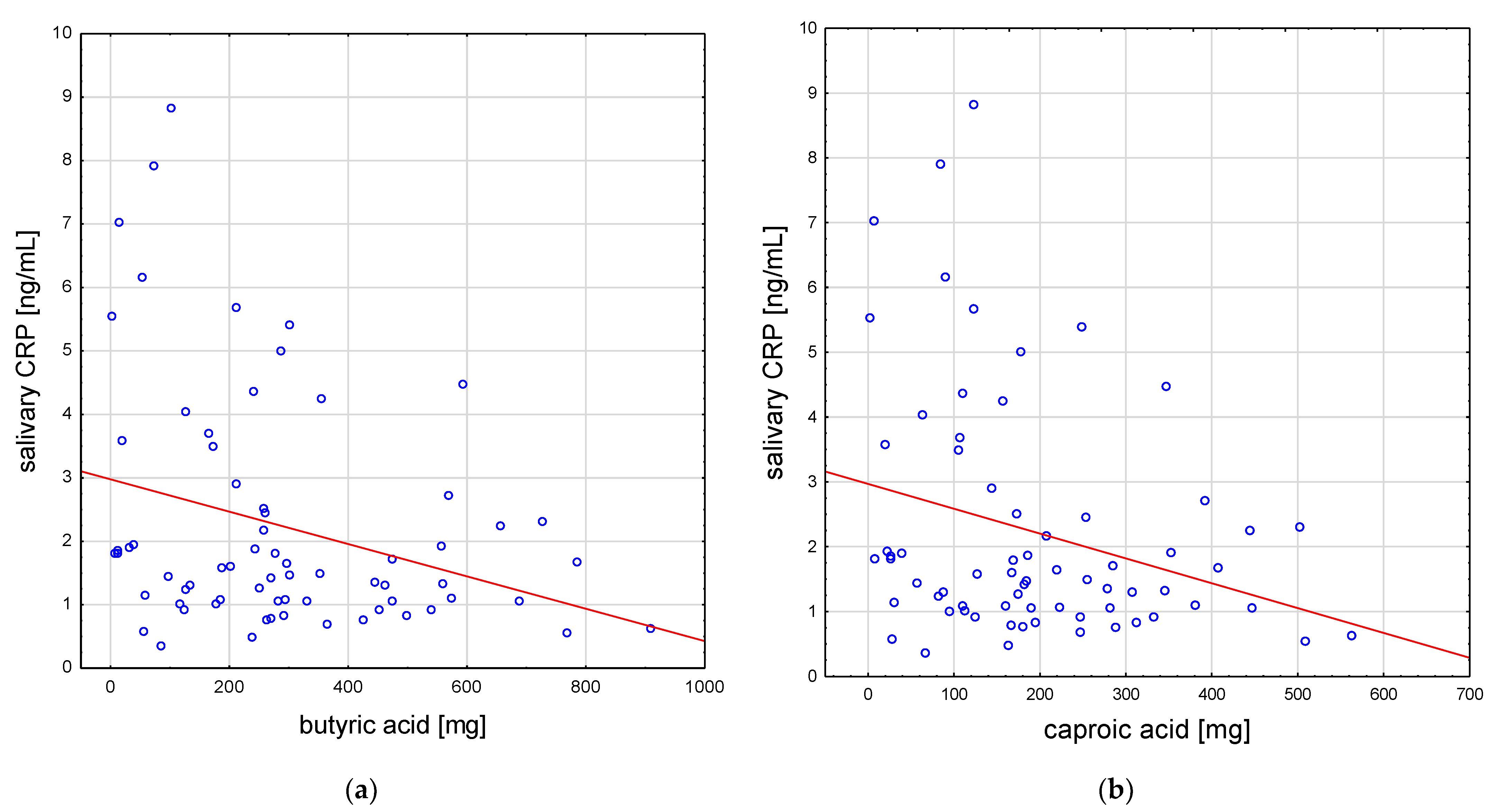
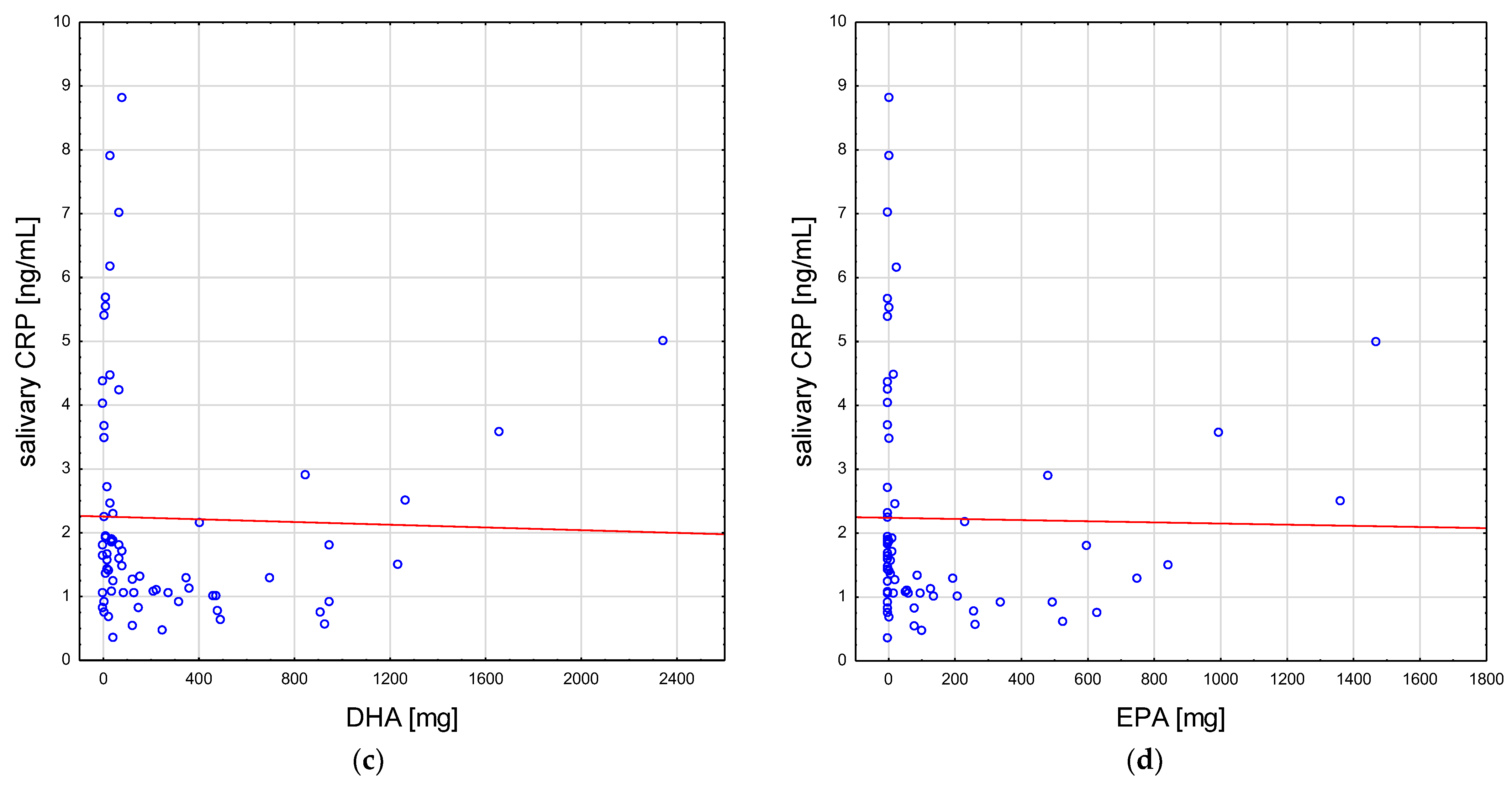
3.5. Correlations of Fatty Acid Intake and Salivary CRP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Djuricic, I.; Calder, P.C. Beneficial Outcomes of Omega-6 and Omega-3 Polyunsaturated Fatty Acids on Human Health: An Update for 2021. Nutrients 2021, 13, 2421. [Google Scholar] [CrossRef]
- Balta, I.; Stef, L.; Pet, I.; Iancu, T.; Stef, D.; Corcionivoschi, N. Essential Fatty Acids as Biomedicines in Cardiac Health. Biomedicines 2021, 9, 1466. [Google Scholar] [CrossRef]
- Tribulova, N.; Szeiffova Bacova, B.; Egan Benova, T.; Knezl, V.; Barancik, M.; Slezak, J. Omega-3 Index and Anti-Arrhythmic Potential of Omega-3 PUFAs. Nutrients 2017, 9, 1191. [Google Scholar] [CrossRef] [PubMed]
- Oppedisano, F.; Macrì, R.; Gliozzi, M.; Musolino, V.; Carresi, C.; Maiuolo, J.; Bosco, F.; Nucera, S.; Caterina Zito, M.; Guarnieri, L.; et al. The Anti-Inflammatory and Antioxidant Properties of n-3 PUFAs: Their Role in Cardiovascular Protection. Biomedicines 2020, 8, 306. [Google Scholar] [CrossRef]
- Oppedisano, F.; Mollace, R.; Tavernese, A.; Gliozzi, M.; Musolino, V.; Macrì, R.; Carresi, C.; Maiuolo, J.; Serra, M.; Cardamone, A.; et al. PUFA Supplementation and Heart Failure: Effects on Fibrosis and Cardiac Remodeling. Nutrients 2021, 13, 2965. [Google Scholar] [CrossRef]
- Liao, J.; Xiong, Q.; Yin, Y.; Ling, Z.; Chen, S. The Effects of Fish Oil on Cardiovascular Diseases: Systematical Evaluation and Recent Advance. Front. Cardiovasc. Med. 2021, 8, 802306. [Google Scholar] [CrossRef] [PubMed]
- Innes, J.K.; Calder, P.C. The Differential Effects of Eicosapentaenoic Acid and Docosahexaenoic Acid on Cardiometabolic Risk Factors: A Systematic Review. Int. J. Mol. Sci. 2018, 19, 532. [Google Scholar] [CrossRef]
- Salehi, B.; Martorell, M.; Arbiser, J.L.; Sureda, A.; Martins, N.; Maurya, P.K.; Sharifi-Rad, M.; Kumar, P.; Sharifi-Rad, J. Antioxidants: Positive or Negative Actors? Biomolecules 2018, 8, 124. [Google Scholar] [CrossRef]
- Richards, L.B.; Li, M.; van Esch, B.C.A.M.; Garssen, J.; Folkerts, G. The effects of short-chain fatty acids on the cardiovascular system. Pharma Nutr. 2016, 4, 68–111. [Google Scholar] [CrossRef]
- Palm, C.L.; Nijholt, K.T.; Bakker, B.M.; Westenbrink, B.D. Short-Chain Fatty Acids in the Metabolism of Heart Failure—Rethinking the Fat Stigma. Front. Cardiovasc. Med. 2022, 9, 915102. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Wu, Q.; Yao, Q.; Jiang, K.; Yu, J.; Tang, Q. Short-chain fatty acid metabolism and multiple effects on cardiovascular diseases. Ageing Res. Rev. 2022, 81, 101706. [Google Scholar] [CrossRef] [PubMed]
- Gawron-Skarbek, A.; Prymont-Przymińska, A.; Sobczak, A.; Guligowska, A.; Kostka, T.; Nowak, D.; Szatko, F. A comparison of native and non-urate Total Antioxidant Capacity of fasting plasma and saliva among middle-aged and older subjects. Redox Rep. 2018, 23, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Stelmach, W.; Kaczmarczyk-Chalas, K.; Bielecki, W.; Drygas, W. The impact of income, education and health on lifestyle in a large urban population of Poland (Cindi programme). Int. J. Occup. Med. Environ. Health 2004, 17, 393–401. [Google Scholar] [PubMed]
- Benzie, I.F.; Strain, J.J. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: The FRAP assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef]
- Chrzczanowicz, J.; Gawron, A.; Zwolinska, A.; de Graft-Johnson, J.; Krajewski, W.; Krol, M.; Markowski, J.; Kostka, T.; Nowak, D. Simple method for determining human serum 2,2-diphenyl-1-picryl-hydrazyl (DPPH) radical scavenging activity—Possible application in clinical studies on dietary antioxidants. Clin. Chem. Lab. Med. 2008, 46, 342–349. [Google Scholar] [CrossRef]
- Schlesier, K.; Harwat, M.; Bohm, V.; Bitsch, R. Assessment of antioxidant activity by using different in vitro methods. Free. Radic. Res. 2002, 36, 177–187. [Google Scholar] [CrossRef]
- Gawron-Skarbek, A.; Chrzczanowicz, J.; Kostka, J.; Nowak, D.; Drygas, W.; Jegier, A.; Kostka, T. Cardiovascular risk factors and total serum antioxidant capacity in healthy men and in men with coronary heart disease. Biomed. Res. Int. 2014, 2014, 216964. [Google Scholar] [CrossRef]
- Jarosz, M.; Rychlik, E.; Stos, K.; Charzewska, J. Nutrition Standards for the Polish Population and Their Application; Narodowy Instytut Zdrowia Publicznego—Państwowy Zakład Higieny: Warszawa, Poland, 2020. [Google Scholar]
- Li, G.; Li, Y.; Xiao, B.; Cui, D.; Lin, Y.; Zeng, J.; Li, J.; Cao, M.J.; Liu, J. Antioxidant Activity of Docosahexaenoic Acid (DHA) and Its Regulatory Roles in Mitochondria. J. Agric. Food Chem. 2021, 69, 1647–1655. [Google Scholar] [CrossRef]
- Farzaneh-Far, R.; Harris, W.S.; Garg, S.; Na, B.; Whooley, M.A. Inverse association of erythrocyte n-3 fatty acid levels with inflammatory biomarkers in patients with stable coronary artery disease: The Heart and Soul Study. Atherosclerosis 2009, 205, 538–543. [Google Scholar] [CrossRef]
- Fontes, J.D.; Rahman, F.; Lacey, S.; Larson, M.G.; Vasan, R.S.; Benjamin, E.J.; Harris, W.S.; Robins, S.J. Red blood cell fatty acids and biomarkers of inflammation: A cross-sectional study in a community-based cohort. Atherosclerosis 2015, 240, 431–436. [Google Scholar] [CrossRef]
- Grenon, S.M.; Conte, M.S.; Nosova, E.; Alley, H.; Chong, K.; Harris, W.S.; Vittinghoff, E.; Owens, C.D. Association between n-3 polyunsaturated fatty acid content of red blood cells and inflammatory biomarkers in patients with peripheral artery disease. J. Vasc. Surg. 2013, 58, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- AbuMweis, S.; Jew, S.; Tayyem, R.; Agraib, L. Eicosapentaenoic acid and docosahexaenoic acid containing supplements modulate risk factors for cardiovascular disease: A meta-analysis of randomised placebo-control human clinical trials. J. Hum. Nutr. Diet. 2018, 31, 67–84. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.; Shi, J.J.; Li, Y.M.; Zhang, X.Y.; Chen, Y.; Calder, P.C.; Tang, L.J. What is the impact of n-3 PUFAs on inflammation markers in Type 2 diabetic mellitus populations?: A systematic review and meta-analysis of randomized controlled trials. Lipids Health Dis. 2016, 15, 133. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Sirtori, C.R.; Carugo, S.; Calder, P.C.; Corsini, A. Omega-3 and cardiovascular prevention—Is this still a choice? Pharmacol. Res. 2022, 182, 106342. [Google Scholar] [CrossRef]
- Zaloga, G.P. Narrative Review of n-3 Polyunsaturated Fatty Acid Supplementation upon Immune Functions, Resolution Molecules and Lipid Peroxidation. Nutrients 2021, 13, 662. [Google Scholar] [CrossRef]
- Cheng, C.; Li, H.; Liang, L.; Jin, T.; Zhang, G.; Bradley, J.L.; Peberdy, M.A.; Ornato, J.P.; Wijesinghe, D.S.; Tang, W. Effects of ω-3 PUFA and ascorbic acid combination on post-resuscitation myocardial function. Biomed. Pharmacother. 2021, 133, 110970. [Google Scholar] [CrossRef]
- Martindale, R.G.; Berlana, D.; Boullata, J.I.; Cai, W.; Calder, P.C.; Deshpande, G.H.; Evans, D.; Garcia-de-Lorenzo, A.; Goulet, O.J.; Li, A.; et al. Summary of Proceedings and Expert Consensus Statements From the International Summit “Lipids in Parenteral Nutrition”. JPEN J. Parenter. Enteral. Nutr. 2020, 44 (Suppl S1), S7–S20. [Google Scholar] [CrossRef]
- Bartolomaeus, H.; Balogh, A.; Yakoub, M.; Homann, S.; Markó, L.; Höges, S.; Tsvetkov, D.; Krannich, A.; Wundersitz, S.; Avery, E.G.; et al. Short-Chain Fatty Acid Propionate Protects From Hypertensive Cardiovascular Damage. Circulation 2019, 139, 1407–1421. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 80) | Low Vitamin C (n = 41) | High Vitamin C (n = 39) | p | |
|---|---|---|---|---|---|
| Age (years) | 66 (64–69) | 66 (64–68) | 67 (63–69) | NS | |
| Sex (f/m) | 69/11 | 35/6 | 34/5 | NS | |
| BMI (kg∙m−2) | 28 (26–33) | 29 (26–34) | 27 (25–32) | NS | |
| Waist circumference (cm) | f | 89 (83–99) | 92 (84–100) | 88 (80–93) | NS |
| m | 99 (94–112) | 105 (99–112) | 94 (91–94) | NS | |
| WHR | f | 0.85 (0.80–0.90) | 0.87 (0.80–0.91) | 0.83 (0.78–0.88) | NS |
| m | 1.01 (0.96–1.04) | 1.03 (1.01–1.05) | 0.96 (0.86–0.96) | NS | |
| TCh (mg dL−1) | 187 (155–206) | 181 (151–200) | 190 (158–210) | NS | |
| LDL–Ch (mg dL−1) | 117 (86–135) | 112 (84- 127) | 127 (97–140) | NS | |
| HDL–Ch (mg dL−1) | 45 (34–54) | 42 (33–52) | 46 (43–57) | NS | |
| TG (mg dL−1) | 113 (77–170) | 138 (93–174) | 96 (73–149) | NS | |
| Variable | All (n = 80) | Low Vitamin C (n = 41) | High Vitamin C (n = 39) | p | ||
|---|---|---|---|---|---|---|
| Vitamin C (mg) | 114 (71–177) | 77 (38–101) | 177 (131–267) | <0.001 | ||
| Total fat (g) | 50 (36–64) | 48 (37–57) | 51 (36–66) | NS | ||
| Energy from fat (%) | 29 ± 7 | 30 ± 8 | 28 ± 7 | NS | ||
| Cholesterol (mg) | 298 ± 166 | 258 ± 125 | 340 ± 193 | 0.02 | ||
| SFA | Total (g) | 18 (13–23) | 17 (13–24) | 18 (12–23) | NS | |
| Energy from SFA (%) | 11 ± 3 | 11 ± 3 | 10 ± 3 | 0.04 | ||
| 4:0 (mg) | 255 (125–411) | 292 (167–462) | 240 (104–292) | NS | ||
| 6:0 (mg) | 170 (92–255) | 182 (107–282) | 166 (73–215) | NS | ||
| 12:0 (g) | 0.5 (0.2–0.6) | 0.5 (0.3–0.7) | 0.4 (0.2–0.6) | NS | ||
| 14:0 (g) | 1.9 ± 1.0 | 2.0 ± 0.9 | 1.8 ± 1.0 | NS | ||
| 16:0 (g) | 9 (8–13) | 9 (8–13) | 10 (8–13) | NS | ||
| 18:0 (g) | 3.8 (2.7–5.4) | 3.9 (2.9–5.7) | 3.5 (2.5–5.3) | NS | ||
| MUFA | Total (g) | 19 (12–26) | 19 (13–26) | 20 (12–26) | NS | |
| Energy from MUFA (%) | 11 (9–14) | 11 (9–15) | 11 (8–13) | NS | ||
| 16:1 (g) | 1.1 (0.8–1.8) | 1.1 (0.8–1.7) | 1.1 (0.8–2.0) | NS | ||
| 18:1 (g) | 17 (11–22) | 17 (11–21) | 17 (11–22) | NS | ||
| PUFA | Total (g) | 7 (6–10) | 6 (5–9) | 7 (6–11) | 0.04 | |
| Energy from PUFA (%) | 4 (3–5) | 4 (3–5) | 4 (3–6) | NS | ||
| ω-3 | ALA (g) | 1.0 (0.6–1.4) | 1.0 (0.8–1.4) | 0.7 (0.6–1.5) | NS | |
| Energy from ALA (%) | 0.5 (0.4–0.8) | 0.4 (0.4–0.8) | 0.5 (0.4–0.8) | NS | ||
| EPA (mg) | 9 (0–181) | 5 (0–97) | 17 (0–260) | NS | ||
| DPA (mg) | 6 (0–50) | 10 (0–64) | 4 (0–48) | NS | ||
| DHA (mg) | 63 (16–358) | 35 (14–271) | 70 (33–404) | NS | ||
| EPA + DHA (mg) | 70 (21–592) | 47 (18–368) | 81 (35–732) | NS | ||
| ω-6 | LA (g) | 5.5 (4.0–7.5) | 5.2 (3.9–6.8) | 6.0 (4.7–9.0) | NS | |
| AA (mg) | 104 (49–192) | 104 (60–175) | 110 (42–238) | NS | ||
| Variable | All (n = 80) | Low Vitamin C (n = 41) | High Vitamin C (n = 39) | p | ||
|---|---|---|---|---|---|---|
| plasma | TAC, | FRAP (mmol FeCl2 L−1) | 1.2 ± 0.2 | 1.3 ± 0.2 | 1.2 ± 0.2 | NS |
| DPPH (% reduction) | 23 ± 6 | 24 ± 6 | 22 ± 5 | NS | ||
| Nu-FRAP (mmol FeCl2 L−1) | 0.40 (0.36–0.45) | 0.43 (0.37–0.52) | 0.38 (0.36–0.43) | 0.009 | ||
| Nu-DPPH (% reduction) | 6 (4–7) | 6 (4–7) | 6 (4–7) | NS | ||
| UA (mg dL−1), | 4.5 ± 1.2 | 4.5 ± 1.0 | 4.4 ± 1.3 | NS | ||
| CRP (mg L−1) | <3 | <3 | <3 | - | ||
| salivary | TAC, | FRAS (mmol FeCl2 L−1) | 5.5 (4.2–6.8) | 6.1 (4.3–7.3) | 5.2 (4.1–6.3) | NS |
| DPPHS (% reduction) | 24 (16–35) | 22 (16–32) | 27 (16–37) | NS | ||
| Nu-FRAS (mmol FeCl2 L−1) | 1.29 (0.96–1.69) | 1.37 (1.08-–1.66) | 1.22 (0.96–1.74) | NS | ||
| Nu-DPPHS (% reduction) | 5 (4–7) | 4 (3–7) | 5 (4–8) | NS | ||
| UA (mg dL−1) | 8.7 (5.9–11.7) | 8.7 (6.5–11.5) | 8.5 (5.6–11.3) | NS | ||
| CRP (ng mL−1) | 1.6 (1.1–2.6) | 1.3 (1.0–1.9) | 1.8 (1.1–3.5) | NS | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gawron-Skarbek, A.; Guligowska, A.; Prymont-Przymińska, A.; Nowak, D.; Kostka, T. The Anti-Inflammatory and Antioxidant Impact of Dietary Fatty Acids in Cardiovascular Protection in Older Adults May Be Related to Vitamin C Intake. Antioxidants 2023, 12, 267. https://doi.org/10.3390/antiox12020267
Gawron-Skarbek A, Guligowska A, Prymont-Przymińska A, Nowak D, Kostka T. The Anti-Inflammatory and Antioxidant Impact of Dietary Fatty Acids in Cardiovascular Protection in Older Adults May Be Related to Vitamin C Intake. Antioxidants. 2023; 12(2):267. https://doi.org/10.3390/antiox12020267
Chicago/Turabian StyleGawron-Skarbek, Anna, Agnieszka Guligowska, Anna Prymont-Przymińska, Dariusz Nowak, and Tomasz Kostka. 2023. "The Anti-Inflammatory and Antioxidant Impact of Dietary Fatty Acids in Cardiovascular Protection in Older Adults May Be Related to Vitamin C Intake" Antioxidants 12, no. 2: 267. https://doi.org/10.3390/antiox12020267
APA StyleGawron-Skarbek, A., Guligowska, A., Prymont-Przymińska, A., Nowak, D., & Kostka, T. (2023). The Anti-Inflammatory and Antioxidant Impact of Dietary Fatty Acids in Cardiovascular Protection in Older Adults May Be Related to Vitamin C Intake. Antioxidants, 12(2), 267. https://doi.org/10.3390/antiox12020267