
The Impact of Antioxidants on Vitiligo and Melasma: A Scoping Review and Meta-Analysis



Abstract
:1. Introduction
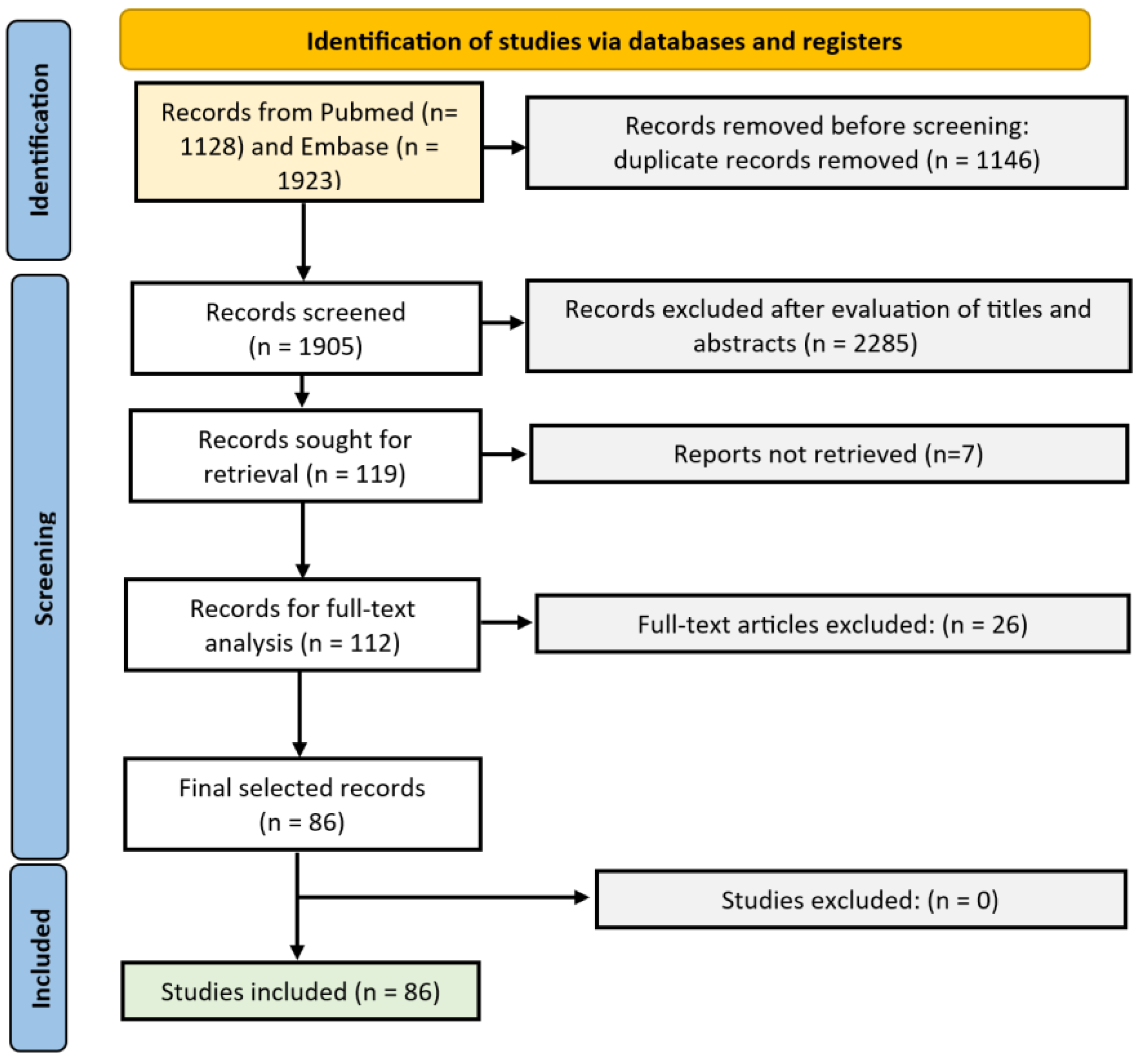
2. Materials and Methods
3. Results
3.1. Results in Vitiligo (Table 1)
3.1.1. Catalase/Superoxide Dismutase
3.1.2. Polypodium Leucotomos
3.1.3. Vitamin E
3.1.4. Vitamin B12
3.1.5. Ginkgo Biloba
3.1.6. α-Lipoic Acid
3.1.7. Other

{kind=link}
{kind=link}
{kind=link}
| Antioxidant | (P)lacebo/No Treatment; (O)ther; (N)o Comparison | (T)opical or (O) Oral | Author | UV | Study Design | (B)etween/(W)ithin | # Pts | Weeks | Outcome | |
|---|---|---|---|---|---|---|---|---|---|---|
| Catalase/superoxide dismutase (SOD) | ||||||||||
| Oral gliadin-protected SOD | (P) Placebo | O | Fontas et al., 2021 [15] | Y | RCT | B | 25/25 | 24 | ↑ | I: improvement VES:19.9% (SE:4.6); VES30:6 (24%); VES50:4 (16%) C: improvement VES:8.8% (SE 4.7); VES30:3 (12%); VES50:1 (4%) |
| Pseudocatalase | (P) Nothing | T | Schallreuter et al., 2008 [35] | Y | Uncontrolled, retrospect. | B | 71/10 | 32–52 w | ↑ | I: repigmentation: 100%: 28/71 (39.4%); >75%: 38/71 (53.2); 0%: 5/71 (7%); C: repigmentation: 50%: 1 (face); none in all other |
| Pseudocatalase | (P) Placebo | T | Schallreuter et al., 2002 [36] | Y | Random., prosp. | B | 39/20 | 3 w | ↑ | I: Significantly more follicular repigmentation in the face compared to controls; 100% cessation of spread |
| SOD, copper, zinc, vit.B12, calcium pantothenate | (P) Nothing | T | Soliman et al., 2014 [37] | Y | Open label, prosp. | W | 30 | 12 w | ↑ | I: response excellent = 20%; good = 26.7%; moderate = 22.2%; poor = 22.2%; none = 8.9%. C: response: 48.9% moderate; 42.2% poor; 8.9% none. |
| Vitix gel | (P) Nothing | T | Yuksel et al., 2009 [38] | Y | Open | B | 15/15 | 24 w | ↗ | I: Repigmentation: n = 1 (>75%); n = 4 (51–75%); n = 10 (26–50%); n = 6 (≤25%) C: Repigmentation: n = 0 (>75%); n = 2 (51–75%); n = 8 (26–50%); n = 11 (≤25%) |
| Pseudocatalase/SOD gel (+ tacrolimus) | (P) Nothing (+tacrolimus) | T | Alshijab et al., 2020 [39] | N | RCT | B | 25/24 | 36 w | = | Percentages of pigmentation on 3, 6, and 9 months: group 1= 23.9%, 40.4%, and 60% vs. group 2 = 23.2%, 40.7%, and 62.4%. |
| Pseudocatalase | (P) Placebo | T | Bakis et al., 2009 [40] | Y | RCT | B | 14/18 | 24 w | = | N.S. |
| Pseudocatalase/SOD | (P) Placebo | T | Naini et al., 2012 [41] | N | RCT | W | 23 | 6 m | = | N.S. |
| Catalase/SOD | (O) 0.05% betamethason | T | Sanclemente et al., 2008 [14] | N | RCT | B | 25 | 40 w | ↘ | I: repigmentation: 12.4% ± 59 C: repigmentation: 18.5% ± 93 |
| Catalase and SOD | (N) | T | Kostović et al., 2007 [42] | Y | Prosp., 1 arm | N | 19 | 6 m | / | Repigmentation: >50%: 11/19 (57.9%); >75%: 3/19 (15.79%); 26–50%: 6/19 (31.58%); 1–25%: 1/19 (5.26%); none: 1/19 (5.26%); No new lesions |
| Pseudocatalase | (N) | T | Patel et al., 2002 [43] | Y | Prosp., 1 arm | N | 32 | 24 w | / | No obvious improvement; 10/26 with at least some improvement of either the hands or face |
| Pseudocatalase and calcium | (N) | O | Schallreuter et al., 1995 [16] | Y | Prosp. 1-arm | N | 33 | 36 m | / | Excellent repigmentation of the face and dorsum of the hands in 90%. Focal vitiligo: 90–100% repigmentation in all cases; No new lesions |
| Cucumis melo extract | (N) | T | Schallreuter et al., 2011 [44] | N | Retrosp., one-arm | N | 53 | 1–24 w | / | No repigmentation without phototherapy Repigmentation in 3/9 with 311 nm phototherapy |
| Polypodium leucotomos (PLE) | ||||||||||
| PLE | Placebo | O | Pacifico et al., 2021 [17] | Y | RCT, assessor-blinded | B | 23/21 | 6 m | ↑ | I: repigmentation: head/neck: excellent = 85%; trunk: moderate-excellent = 92%; extremities: moderate = 83%; C: repigmentation: head/neck: excellent = 25%; trunk: moderate-excellent = 44%; extremities: moderate = 12%; |
| PLE | Placebo | O | Reyes et al., 2005 [18] | Y | RCT | B | 10/9 | 12 w | ↑ | I: >50% repigmentation significantly higher compared to placebo |
| PLE | Placebo | O | Middelkamp et al., 2007 [19] | Y | RCT | B | 25/24 | 26 w | ↗ | I: trend towards more repigmentation compared with the placebo group |
| PLE | Placebo | O | Salazar et al., 2013 [20] | Y | RCT | B | 4/4 | 24 w | ↘ | I: depigmentation: Baseline: 35 ± 21%; FU: 16 ± 17%. C: depigmentation: Baseline: 26 ± 13%; FU: 6 ± 4%. |
| PLE | / | O | Mohammad et al., 1989 [45] | N | Prosp. 1-arm | / | 22 | 5 m | / | 100% cured of the disease. This successful treatment coincided with the hottest months of the year. |
| Vitamin E | ||||||||||
| Phyllanthus emblica fruit extracts, vitamin E, carotenoids | Nothing | O | Colucci et al., 2014 [22] | Y | Random | B | 65/65 | 24 | ↑ | I: significant mild repigmentation in the head and neck (p = 0.019) and on the trunk (p = 0.051), a higher but not significant repigmentation for each body site, and higher stable disease (p = 0.065). |
| a-lipoic acid, vit C, vit E, polyunsat. fatty acids, cysteine | Placebo | O | Dell’Anna et al., 2007 [21] | Y | RCT | B | 14/11 | 24 w | ↑ | I: repigmentation: >75% in 8/17(47%; p < 0.05 vs. placebo);0–75%; 4/17 (23.5) C: repigmentation: >50% in 2/11(18%) |
| Vitamin E | Nothing | O | Elgoweini et al., 2009 [46] | Y | Prosp. Random | B | 12/12 | 6 m | ↑ | I: Marked to excellent repigmentation in 8/11 (72.7%); No new lesions C: Marked to excellent repigmentation in 5/9 (55.6%); No new lesions |
| Vit E, beta-carotene, vit C, selenium, copper, zinc, manganese | Nothing | O | Jayanth et al., 2002 [23] | Y | Random., not blinded | B | 15/15 | 12 | = | N.S. |
| Vitamin B12 | ||||||||||
| 2 groups (1) vit D and (2) vit D and vit B12 | Nothing | O | Iraji et al., 2017 [24] | Y | Open randomized | IB | 20/20/20 | 24 w | ? | N.S |
| Vit B12 and folic acid | Nothing | O | Tijoe et al., 2002 [25] | Y | Prosp., open | B | 14/3 | 1 y | = | No significant difference in repigmentation at any time point. |
| Vitamin C | ||||||||||
| Vit C, vit B12, folic acid | / | O | Don et al., 2006 [27] | Y | Prosp, 1-arm | / | 9 | 10 m | / | Significant repigmentation in all patients. Stop disease progression in 9/9 |
| Vit B12 and folic acid | / | O | Juhlin et al., 1997 [26] | Y | Prosp, 1-arm | / | 100 | / | Repigmentation in 52/100, Stop of disease progression in 64% | |
| Vit C, vit B12 | / | O | Sendrasoa et al., 2019 [28] | N | Prosp, 1-arm | / | 308 | 3–18 m | / | >76% repigmentation in 50 (65.7%) |
| Ginkgo biloba | ||||||||||
| Ginkgo biloba | Placebo | O | Parsad et al., 2003 [29] | N | RCT | B | 25/22 | 6 m | ↑ | I: Marked to complete repigmentation in 10 patients C: Marked to complete repigmentation in 2 patients Significant cessation of spread G. biloba (p = 0.006): 20/25 vs. 8/22 |
| Ginkgo biloba | Placebo | O | Abu-Raghif et al., 2013 [30] | Y | RCT., single blinded | B | 12/12 | 8 w | ↗ | I: VASI baseline: 6.42 ± 4.08; VASI FU: 6.17 ± 4.27; Difference: −0.25 C: VASI baseline: 3.75 ± 2.81; VASI FU: 3.88 ± 2.77; Difference: +0.13 |
| Ginkgo biloba | / | O | Szczurko et al., 2011 [31] | N | Prosp. open-label | / | 11 | 12 w | / | Mean percent improvement: 15%. Significant impact on arresting the spread of vitiligo: total spreading score from 2.7 to −1.1 (p ≤ 0.001) |
| α-lipoic acid | ||||||||||
| α-lipoic acid | Placebo | O | Li et al., 2015 [32] | Y | RCT | B | 26/24 | 6 m | ↗ | I: repigmentation ≥75% in 55%; 51–75% in 35% C: repigmentation ≥75% in 36.84%; 51–75% in 47.37%. |
| α-lipoic acid | Placebo | O | Sun et al., 2020 [47] | Y | RCT | B | 37/28 | 6 m | ↘ | I: >50% repigmentation: 37.8% (14/37) C: >50% repigmentation: 42.9% (12/28) |
| Other | ||||||||||
| Selenium | / | O | Tsiskarishvili et al., 2016 [33] | Y | ? | B | 17/18 | 5 w | ? | I: follicular repigmentation: 60.9%; C: follicular repigmentation: 29.1% |
| Turmeric | Placebo | T | Jalalmanesh et al., 2022 [34] | N | RCT | B | 24 | 4 m | ↑ | I: significant reduction in the size of the lesions following applying turmeric cream compared to placebo (independent-sample t-test, mean ± SE: 29.31 ± 5.31 for drug vs. −21.36 ± 11.00 for placebo, p < 0.05). |
3.2. Melasma (Table 2; Supplementary Table S1)
3.2.1. Vitamin C
3.2.2. Niacinamide
3.2.3. Cysteamine
3.2.4. Silymarin
3.2.5. Polypodium Leucotomos
3.2.6. Azelaic Acid
3.2.7. Tomato/Lycopene
3.2.8. Zinc Sulfate
3.2.9. Other
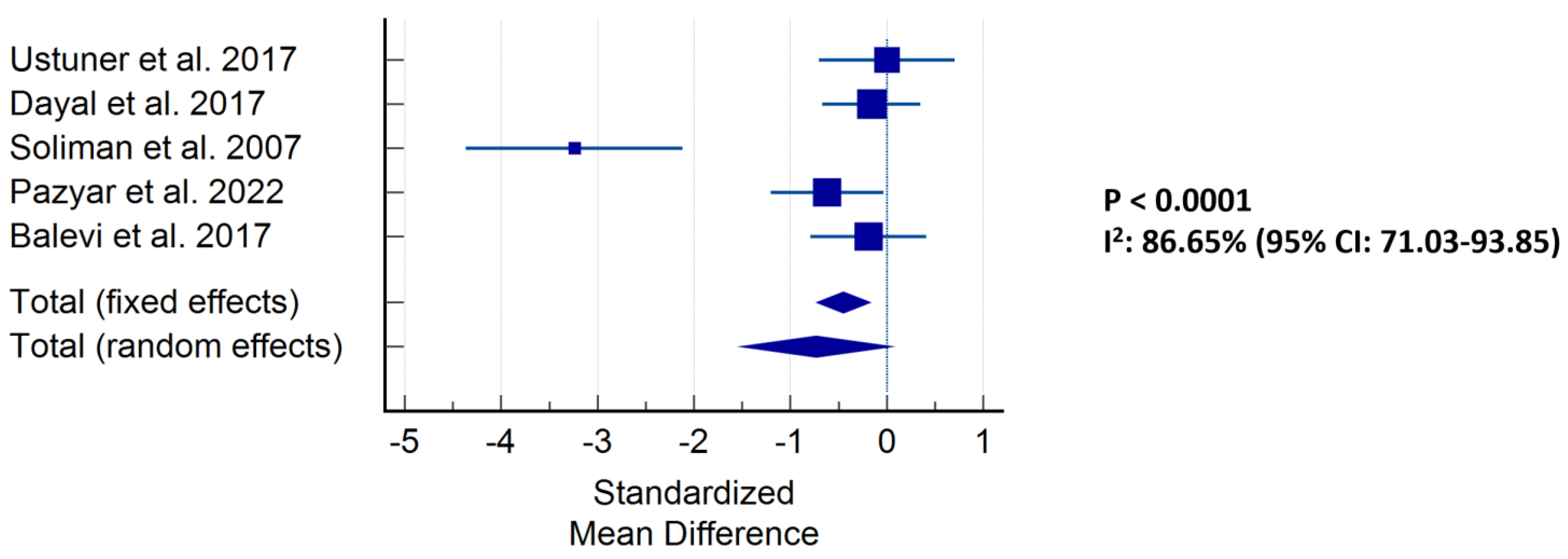
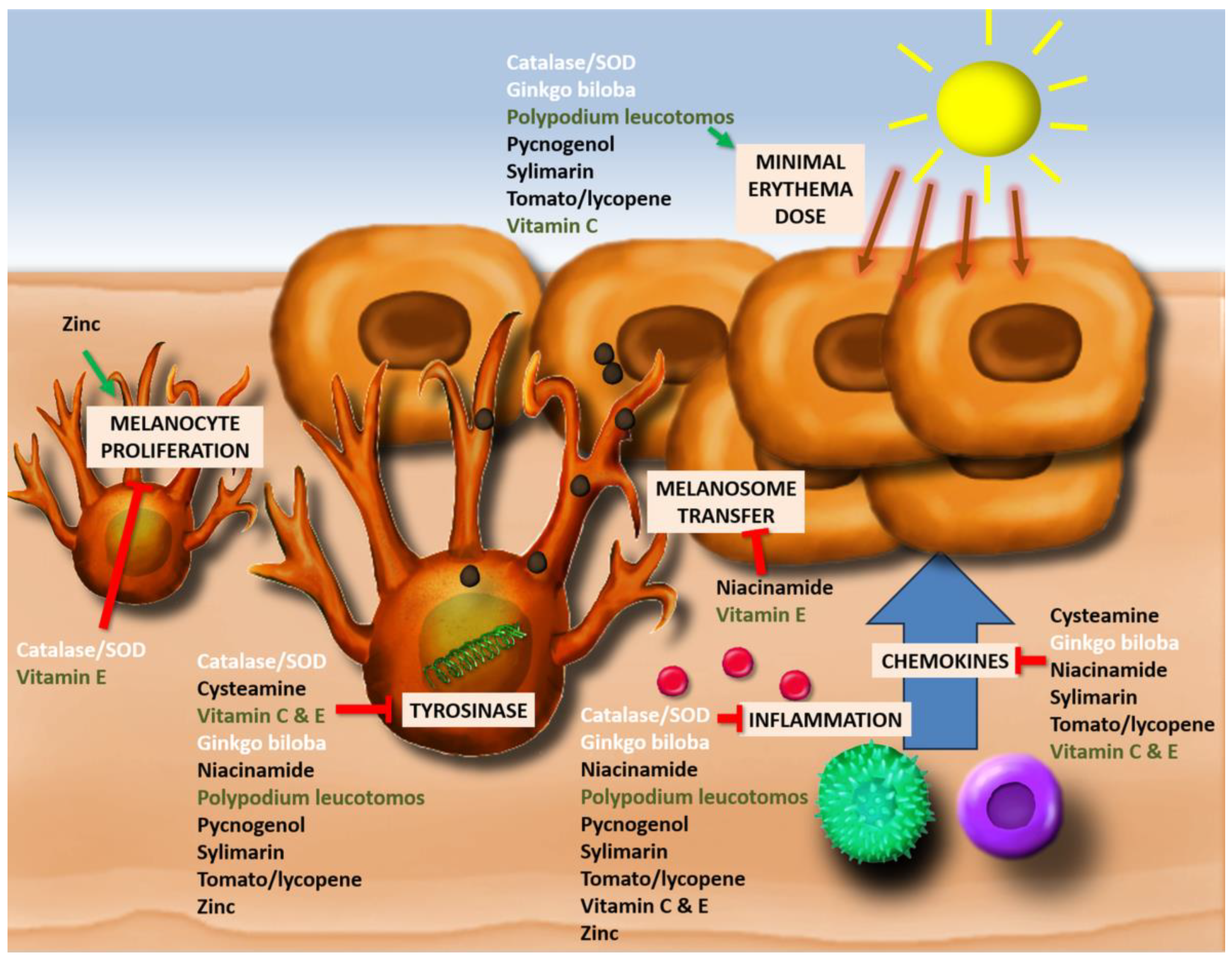
3.3. Effects of Antioxidants (Figure 3, Supplementary Table S2)
| Antioxidant | (P = Placebo/Nothing; O = Other Treatment) | (T)opical/(O)ral | Author | Study Design | (B)etween/(W)ithin | # Pts | Duration | Outcome | |
|---|---|---|---|---|---|---|---|---|---|
| Vitamin C | |||||||||
| 4% liquiritin mixed in 5% ascorbic acid | (P) 4% liquiritin | T | Akram et al., 2013 [86] | RCT | W | 41/41 | 6 m | ↑ | I: improvement in MASI: n = 36 (88%) C: improvement in MASI: n = 25 (61%) |
| 20% TCA Peel with 5% Ascorbic Acid | (P) 20% TCA peeling | T | Dayal et al., 2017 [53] | Unblinded, prosp., rand. | / | 30/30 | 12 w | ↑ | I: Baseline MASI: 23.55 ± 4.62; 12 wk: 9.50 +/− 5.31 C: Baseline MASI:23.6 ± 4.08; 12 wk: 15.10 +/− 4.44 |
| Vitamin C iontophoresis | (P) Distilled water iontophoresis | T | Huh et al., 2003 [87] | RCT | W | 21 | 12 w | ↑ | Significant difference between the ¢L value of the vitamin C- and placebo-treated sites (p = 0.03). |
| Intradermal tranexamic acid + top. ascorbic acid | (P) Intradermal tranexamic acid + placebo | T | Pazyar et al., 2022 [54] | Split-face comparative | W | 24 | 12 w | ↑ | I: Decrease in MASI: 2 points (baseline: 4.61 (SD 1.54); FU: 2.61 (SD 1.14) C: Decrease in MASI: 1.29 points (baseline: 4.49 (SD 1.48); FU: 3.20 (SD 1.21) Significantly lower final MASI in the intervention group. |
| TCA peel and ascorbic acid | (P) TCA peel | T | Soliman et al., 2007 [51] | Prop. trial (randomized?) | W | 15/15 | 16 w | ↑ | I: Baseline MASI: 13.753 ± 4.101; FU: 7.73 ± 4.203; average decrease: 6.023 C: Baseline MASI: 15.413 ± 2.881; FU: 12.32 ± 3.381 average decrease: 3.093 |
| Microneedling with vit C + Q-switched Nd:YAG | (P) Q-switched Nd:YAG | T | Ustuner et al., 2017 [52] | RCT | W | 16 | 6 m | ↑ | I: MASI at baseline: 7.04 ± 4.55; final: 2.49 ± 2.30 C: MASI at baseline: 6.13 ± 4.94; final: 4.52 ± 3.49 |
| Medlite C6 q-1064 laser+ vit C, E and ferulic acid | Medlite C6 q-1064 laser | T | Y et al., 2023 [88] | Ranomized split-face | W | 61 | 14 w | ↑ | I: difference in MASI score: t = 17.25 C: difference in MASI score: t = 9.78 |
| Salicylic acid peeling + vitamin C mesotherapy | (P) Salicylic acid peeling | T | Balevi et al., 2017 [55] | Single-blinded RCT | B | 23/21 | 2 m | ↗ | I: baseline MASI:16.68 ± 11.57; FU: 5.32 ± 2.68; Decrease: 11.36 C: baseline MASI: 15.81 ± 10.51; FU: 13.97 ± 10.86; Decrease: 1.84. N.S. |
| 1064-nm Q-switched Nd:YAG + ultrasonic vitamin C | (P) 1064-nm Q-switched Nd:YAG | T | Lee et al., 2015 [89] | Split-face prosp. | W | 8 | 4 sess + 3 m | ↗ | I: VAS after the first treatment: 3.00 ± 0.53; final VAS: 1.37 ± 0.52 C: VAS after the first treatment: 3.75 ± 0.89; final VAS: 1.50 ± 0.53 Significant > VAS reduction with vit. C at different time points, not at the final FU |
| Vitamin C + microneedling | (O) PRP + microneedling | T | Abdel-Rahman et al., 2021 [90] | Prosp. split-face | W | 10 | 6 sess + 1 m | ↑ | I: Baseline MASI: 11.75 ± 2.75; FU: 2.78 ± 0.67; MASI reduction: 76.29% C: Baseline MASI: 12.06 ± 2.39; FU: 5.86 ± 1.06; MASI reduction: 46.13% |
| Vitamin C iontophoresis | (O) glycolic acid 70% peel | T | Sobhi et al., 2012 [50] | Prosp., single blinded (?) | W | 14 | 6 sess | ↑ | I: Baseline MASI: 8.3143 ± 2.815; FU: 4.778 ± 2.793; decrease: 3.535 C: Baseline MASI: 7.9714 ± 2.536; FU: 6.2143 ± 2.725; decrease: 1.757 |
| Vitamin C after microneedling | (O) tranexamic acid after microneedling | T | El Attar. et al., 2022 [48] | Prosp., rand., uncont. | W | 20 | 12 w | ↘ | I: baseline hemi-MASI: 0.90–21.60; FU: 0.60–18.0; decrease: 45.94% C: baseline hemi-MASI: 0.90–21.60; FU: 0.0–16.20; decrease: 53.76%. |
| Transdermal injections of vitamin C | (O) transdermal tranexamic acid | D | Zhao et al., 2020 [49] | RCT | W | 17 | 2 m | ↘ | I: 6.94 ± 4.28; FU: 3.32 ± 3.30; Difference: 3.62 ± 2.79 C: 7.03 ± 3.84; FU: 2.97 ± 2.62; Difference: 4.06 ± 2.62 |
| Vitamin C iontophoresis | (O) Multivitamin ionotophoresis | T | Choi et al., 2010 [91] | Split-face | W | 20 | 12 | = | Both groups reported equal improvement in subjective self-assessment and colorimetry |
| Vitamin C + microneedling | (O) Tranexamic acid + microneedling | T | Raza et al., 2020 [92] | Split-face prosp. | W | 30 | 6 w | = | I: 13% excellent response, 43% good response, 30% fair improvement C: 16% excellent response, 40% good, 26% mild improvement |
| 3% vitamin C derivative | (O) Plant extracts, including orchid | T | Tadokoro et al., 2010 [93] | Split-face, prosp. study | W | 18 | 8 w | = | Both formulations significantly increased the average color value (lightness) of the pigmented spots (p < 0.01) |
| 20% vitamin C solution + microneedling | (O) Tranexamic acid + microneedling | T | Tahoun et al., 2020 [94] | Split-face prosp. | W | 30 | 16 w | = | I: MASI baseline: 6.34 ± 3.78; FU: 3.04 ± 2.64 C: MASI: baseline: 5.98 ± 3.58); FU: 3.64 ± 2.62 |
| 5% ascorbic acid | (O) 4% hydroquinone | T | Espinal-Perez et al., 2004 [95] | RCT, split-face | W | 16 | 16 w | ↓ | I: Patients’ assessment: excellent: n = 2, good: n = 8, moderate: n = 4, mild: n = 2 C: Patients’ assessment: excellent: n = 8, good: n = 7, moderate: n = 1, mild: n = 0 |
| Niacinamide | |||||||||
| Niacinamide formulated into cationic liposomes | (P) Control solution | T | Lee et al., 2022 [56] | Prospective, split-face | W | 21 | 4 w | ↑ | I: 1.38–2.08-fold improvement compared to the control solution (p < 0.05) |
| Niacinamide 4% | (P) Placebo | T | Campuzano et al., 2019 [96] | RCT | B | 10/10 | 8 w | ↗ | I: Baseline MASI: 15.4 ± 6.7; FU: 10.4 ± 5.1 C: Baseline MASI: 9.1 ± 1.4; FU: 7.1 ± 1.2. |
| Niacinamide + sunscreen | (P) Placebo + sunscreen | T | Hakozaki et al., 2002 [57] | RCT, split-face | W | 18 | 8 w | ↗ | 4–6 weeks: niacinamide + sunscreen showed significant increase in Lvalue (skin lightness) vs. placebo. No significance at 8 weeks (p = 0.059) |
| Niacinamide + sunscreen | (P) Placebo + sunscreen | T | Goh et al., 2012 [97] | RCT | B | 30/30 | 84 d | = | MASI scores showed a significant reduction in patients treated with the study cream (6.0 to 4.6) and vehicle cream (6.6 to 4.7) (N.S.). |
| Niacinamide 4% | (O) Hydroquinone 4% | T | Navarrete et al., 2011 [59] | RCT, split-face | W | 27 | 8 w | ↘ | I: Baseline MASI: 3.7 (95% CI, 2.9–4.4); FU: 1.4 (95% CI, 3.3–4.7) C: Baseline MASI: 4 (5% CI, 90.9–1.8); FU: 1.2 (95% IC, 0.8–1.6) |
| Niacinamide | (O) Kigman, intrad. tranexamic acid | T | Giasante et al., 2020 [58] | RCT | B | 10/10 | 8 w | = | Triple combination, topical niacinamide, and intradermal tranexamic acid have similar responses. |
| Cysteamine | |||||||||
| Cysteamine 5% | (P) Placebo | T | Farshi et al., 2017 [60] | RCT | B | 20/20 | 4 m | ↑ | I: MASI baseline: 18.1 ± 8.1; FU: 8.03 ± 5.2 C: MASI baseline: 13.2 ± 7.4; FU: 12.2 ± 7.4 |
| Cysteamine 5% | (P) Placebo | T | Mansouri et al., 2014 [61] | RCT | B | 25/25 | 4 m | ↑ | I: MASI baseline: 17.2 ± 8.1; MASI follow-up: 7.2 ± 5.5 C: MASI baseline: 13 ± 8.1; MASI follow-up: 11.6 ± 7.9 |
| Cysteamine 5% | (O) tranexamic acid mesotherapy | T | Karrabi et al., 2022 [65] | Single-blind, rand. | B | 27/27 | 2 m | = | I: mMASI baseline: 11.68 ± 2.70; FU: 6.32 ± 2.11 C: mMASI baseline: 10.43 ± 2.69; FU: 5.52 ± 2.55 |
| Cysteamine 5% | (O) 4% hydroquinone | T | Lima et al., 2020 [62] | quasi-rand., evaluator-blinded | B | 20/20 | 120 d | = | I: median (IQR): mMASI baseline: 9 (6–12); After: 5 (4–8) C: median (IQR): mMASI baseline: 6 (3–8); After: 2 (1–3) Mean reduction mMASI was 38% for CYS and 53% for HQ (p = 0.017). |
| Cysteamine 5% | (O) Hydroquinone 4% + vit C 3% | T | Sepaskhah et al., 2022 [63] | single-blind, RCT | B | 31/34 | 4 m | = | I: decrease in mMASI from 6.69 ± 2.96 to 4.47 ± 2.16 C: decrease in mMASI from 6.26 ± 3.25 to 3.87 ± 2.00 in the HC group. |
| Cysteamine 5% | (O) Hydroquinone | T | Nguyen et al., 2021 [64] | Rand., double blinded trial | B | 5/9 | 16 w | ↘ | I: reduction in mMASI: 1.52 ± 0.69 (21.3%) C: reduction in mMASI: 2.96 ± 1.15 (32%). N.S. |
| Silymarin | |||||||||
| Silymarin | (P) No treatment or placebo | T | Altaei et al., 2012 [98] | RCT | B | 32/32 | 4 w | ↑ | I: (0.1%) MASIstart: 17.1 ± 3.12; FU: 0; (0.2%); MASIstart: 16.5 ± 2.8; FU: 0 C: baseline MASI: 16.8 ± 3.2; FU: 17 ± 3.4 |
| Silymarin | (O) Low Fluence 1064 Nd:YAG | T | Ibrahim et al., 2021 [68] | RCT | B | 25/25 | 3 m | ↗ | I: mMASI baseline: 9 (IQR: 5.4–12.1); mMASI FU: 2.3 (1.2–6.6) C: mMASI baseline: 7.3 (IQR: 4.8–10.3)); mMASI FU: 2.1 (1–4.7) |
| Silymarin | (O) Hydroquinone | T | Wattanakrai et al., 2022 [67] | RCT, split-face | W | 23 | 3 m | ↗ | I: Modified MASI reduction: 17.97% C: Modified MASI reduction: 7.11% |
| Silymarin | (O) Hydroquinone | T | Nofal et al., 2019 [66] | Prosp. clinical trial | B | 14/14/14 | 3 m | ↘ | I: (0.7%): baseline MASI: 18.56 ± 5.58; FU: 10.96 ± 4.48; difference: 39.21% (1.4%): baseline MASI: 21.75 ± 8.47; FU: 14.88 ± 7.79; difference: 33.84% C: baseline MASI: 16.64 ± 9.02; FU: 8.81 ± 5.68; difference: 46.75% |
| Polypodium leucotomos | |||||||||
| Polypodium leucotomos | (P) Placebo | O | Martin et al., 2012 [71] | RCT | B | 21 | 12 w | ↑ | I: significantly improved mean (MASI) scores (5.7 to 3.3; p < 0.05), while the placebo group did not (4.7 to 5.7; p > 0.05). |
| Polypodium leucotomos + 4% hydroquinone | (P) Placebo + hydroquinone 4% | O | Goh et al., 2018 [69] | RCT | B | 33 | 12 w | ↑ | I: baseline mMASI: 6.8; final: −54.9% C: baseline mMASI: 6; final: −44.4% |
| Polypodium leucotomos | (P) Placebo | O | Ahmed et al., 2013 [70] | RCT | B | 16/17 | 12 w | = | The MASI scores similarly showed improvement in both groups without significant intergroup differences (p = 0.62). |
| Azelaic acid | |||||||||
| Azelaic acid 20% + oral tran. acid + sunscr. | (O) Hydroq 4% + oral tran. acid + sunscr. | T | Akl et al., 2021 [72] | RCT | B | 25/25 | 4 m | ↗ | I: mMASI baseline: 17.06 (+/−1.51); mMASI FU: 5.58 (+/−1.28) C: mMASI baseline: 17.77 (+/−1.45); mMASI FU: 7.18 (+/−1.31) |
| 20% azelaic acid | (O) 10% tranexamic acid cream | T | Das et al., 2020 [73] | RCT, split-face | B | 16/16 | 12 w | = | Composite malar area pigment score (CMAPS) of tranexamic acid (1.73 ± 1.68) less than azelaic acid (2.08 ± 1.70). N.S. |
| 20% azelaic acid cream | 2.3% diclofenac gel | T | Arpornpattanapong et al. 2023 [76] | Single blind, split face | W | 20 | 12 | ↘ | The difference in mMASI between diclofenac and azelaic acid was insignificant (p = 067); patient satisfaction was significantly higher for diclofenac. |
| Azelaic acid 20% | (O) Hydroquinone 4% | T | Emad et al., 2013 [75] | Prosp, split-face | B | 33 | 20 w | ↘ | I: baseline mMASI: 7.88 ± 3.27; FU mMASI: 3.47 ± 2.88; reduction: 55% C: baseline mMASI; 7.8 ± 3.36; FU mMASI: 3.11 ± 2.91; reduction: 61% |
| Oral tranexamic acid + topical 20% Azelaic Acid | (O) Oral + topical 3% tranexamic acid | T | Malik et al., 2019 [74] | Rand, prosp | B | 50/50 | 6 m | ↘ | I: baseline MASI: 34 ± 13; FU: 10.62 ± 7.43 C: baseline MASI: 33.7 ± 12; FU: 6.06 ± 5.06 |
| Tomato/Lycopene | |||||||||
| Tomato extract + hydroquinone 4% | (P) Hydroquinone 4% | O | Afriliana et al., 2020 [77] | Double-blind, rand. | B | 31/31 | 12 w | ↑ | I: mMASI baseline: 5.25; after: 1.2; decrease: 3 C: mMASI baseline: 6.0; after: 4.2; decrease: 1.2 |
| Lycopene 30 mg + 4% hydroquinone | (P) Placebo + 4% hydroquinone | T | Avianggi et al., 2022 [99] | Double-blind RCT | B | 59 | 12 w | ↑ | The difference in MASI scores after therapy in the treatment group had a significant decrease compared to the control group. |
| Zinc | |||||||||
| 10% Zinc Sulfate Solution | (O) Hydroquinone 4% | T | Iraji et al., 2012 [79] | RCT, investig.-blinded | B | 36/36 | 6 m | ↓ | I: difference in MASI: 0.7 ± 0.7 C: difference in MASI: 2.7 ± 1.6. More significant reduction for HQ vs. zinc. |
| 10% Zinc Sulfate Solution | (O) Hydroquinone 4% | T | Yousefi et al., 2014 [80] | RCT | / | 40/42 | 2 m | ↓ | I: baseline MASI: 6.3 ± 2.1; FU MASI: 5.1 ± 2.0; decrease in MASI: 18.6% ± 20.8 C: baseline MASI: 6.4 ± 1.6; FU MASI: 3.9 ± 1.4; decrease in MASI: 43.5% ± 15.5 |
| Glutathione | |||||||||
| Tranex. acid mesoth. + vit C + glutathione | (P) Tranex. acid mesotherapy + vit C | T | Iarji et al., 2019 [100] | RCT | W | 30 | 12 w | ↑ | I: mMASI decrease: of 3.046 ± 1.25 (p-value < 0.001) C: mMASI decrease: 1.82 ± 0.88 (p-value < 0.001). |
| Glutathione + microneedling | (P) Microneedling | T | Mohamed et al., 2023 [83] | Split face, non-blinded | W | 29 | 3 m | ↑ | I: baseline hemi-mMASI: 4.21 ±2.08; FU hemi-mMASI: 1.96 ± 1.30 C: baseline hemi-mMASI: 4.06 ± 1.91; FU hemi-mMASI: 2.31 ± 1.45 |
| Other | |||||||||
| Mulberry extract oil | (P) Placebo | T | Alvin et al., 2011 [81] | RCT | B | 25/25 | 8 w | ↑ | I: Baseline MASI: 4.076 ± 0.24; FU: 2.884 (±0.25); mean difference: 1.19 C: mean difference MASI: 0.06 |
| Rucinol serum | (P) Placebo | T | Khemis et al., 2007 [84] | RCT, split-face | W | 32 | 12 w | ↑ | I: clinical pigmentation score at baseline: 7.5 +/− 1.9; follow-up: 6.2 +/− 2.3 C: clinical pigmentation score at baseline: 7.5 +/− 1.9; follow-up: 6.7 +/− 2.1. |
| 75 mg pycnogenol 2x/d | (P) Placebo | O | Lima et al., 2020 [82] | RCT | B | 22/22 | 60 d | ↑ | I: mMASIbaseline: 9.1 (4.1); FU: 4.6 (3.4); mMASI reduction: 4.4 (3.1) C: mMASIbaseline: 9.2 (4.2); mMASI FU: 6.4 (4.3); mMASI reduction: 2.7 (2.5) |
| Petroselinum Crispum (Parsley) | (O) hydroquinone 4% | T | Khosravan et al., 2017 [85] | RCT | B | 25/25 | 8 w | = | I: Baseline MASI: 6.66 ± 4.39; FU MASI: 4.92 ± 3.07 C: Baseline MASI: 6.68 ± 3.24; FU MASI: 5.06 ± 2.66. N.S. |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kamiński, K.; Kazimierczak, U.; Kolenda, T. Oxidative Stress in Melanogenesis and Melanoma Development. Contemp. Oncol. 2022, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Denat, L.; Kadekaro, A.L.; Marrot, L.; Leachman, S.; Abdel-Malek, Z.A. Melanocytes as Instigators and Victims of Oxidative Stress. J. Investig. Dermatol. 2014, 134, 1512–1518. [Google Scholar] [CrossRef]
- Simon, J.D.; Peles, D.; Wakamatsu, K.; Ito, S. Current Challenges in Understanding Melanogenesis: Bridging Chemistry, Biological Control, Morphology, and Function. Pigment. Cell Melanoma Res. 2009, 22, 563–579. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Mosby, N.; Yang, J.; Xu, A.; Abdel-Malek, Z.; Kadekaro, A.L. Alpha-MSH Activates Immediate Defense Responses to UV-Induced Oxidative Stress in Human Melanocytes. Pigment. Cell Melanoma Res. 2009, 22, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-T.; Choi, B.; Tang, M. Melanocytes Are Deficient in Repair of Oxidative DNA Damage and UV-Induced Photoproducts. Proc. Natl. Acad. Sci. USA 2010, 107, 12180–12185. [Google Scholar] [CrossRef] [PubMed]
- Speeckaert, R.; Dugardin, J.; Lambert, J.; Lapeere, H.; Verhaeghe, E.; Speeckaert, M.M.; van Geel, N. Critical Appraisal of the Oxidative Stress Pathway in Vitiligo: A Systematic Review and Meta-Analysis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Sravani, P.V.; Babu, N.K.; Gopal, K.V.T.; Rao, G.R.R.; Rao, A.R.; Moorthy, B.; Rao, T.R. Determination of Oxidative Stress in Vitiligo by Measuring Superoxide Dismutase and Catalase Levels in Vitiliginous and Non-Vitiliginous Skin. Indian J. Dermatol. Venereol. Leprol. 2009, 75, 268–271. [Google Scholar] [CrossRef]
- Schallreuter, K.U.; Wood, J.M.; Berger, J. Low Catalase Levels in the Epidermis of Patients with Vitiligo. J. Investig. Dermatol. 1991, 97, 1081–1085. [Google Scholar] [CrossRef]
- Li, S.; Zhu, G.; Yang, Y.; Jian, Z.; Guo, S.; Dai, W.; Shi, Q.; Ge, R.; Ma, J.; Liu, L.; et al. Oxidative Stress Drives CD8+ T-Cell Skin Trafficking in Patients with Vitiligo through CXCL16 Upregulation by Activating the Unfolded Protein Response in Keratinocytes. J. Allergy Clin. Immunol. 2017, 140, 177–189. [Google Scholar] [CrossRef]
- Rahimi, H.; Mirnezami, M.; Yazdabadi, A.; Hajihashemi, A. Evaluation of Systemic Oxidative Stress in Patients with Melasma. J. Cosmet. Dermatol. 2023. [Google Scholar] [CrossRef]
- Choubey, V.; Sarkar, R.; Garg, V.; Kaushik, S.; Ghunawat, S.; Sonthalia, S. Role of Oxidative Stress in Melasma: A Prospective Study on Serum and Blood Markers of Oxidative Stress in Melasma Patients. Int. J. Dermatol. 2017, 56, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.E.; Harris, T.H.; Weninger, W.; Wherry, E.J.; Hunter, C.A.; Turka, L.A. A Mouse Model of Vitiligo with Focused Epidermal Depigmentation Requires IFN-γ for Autoreactive CD8+ T-Cell Accumulation in the Skin. J. Investig. Dermatol. 2012, 132, 1869–1876. [Google Scholar] [CrossRef]
- Lee, E.J.; Kim, J.Y.; Yeo, J.H.; Park, S.; Bae, Y.J.; Kwon, I.J.; Seong, S.H.; Lee, J.; Oh, S.H. ISG15-USP18 Dysregulation by Oxidative Stress Promotes IFN-γ Secretion from CD8+ T Cells in Vitiligo. J. Investig. Dermatol. 2023. [Google Scholar] [CrossRef]
- Sanclemente, G.; Garcia, J.; Zuleta, J.; Diehl, C.; Correa, C.; Falabella, R. A Double-Blind, Randomized Trial of 0.05% Betamethasone vs. Topical Catalase/Dismutase Superoxide in Vitiligo. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1359–1364. [Google Scholar] [CrossRef] [PubMed]
- Fontas, E.; Montaudié, H.; Passeron, T. Oral Gliadin-Protected Superoxide Dismutase in Addition to Phototherapy for Treating Non-Segmental Vitiligo: A 24-Week Prospective Randomized Placebo-Controlled Study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1725–1729. [Google Scholar] [CrossRef] [PubMed]
- Schallreuter, K.U.; Wood, J.M.; Lemke, K.R.; Levenig, C. Treatment of Vitiligo with a Topical Application of Pseudocatalase and Calcium in Combination with Short-Term UVB Exposure: A Case Study on 33 Patients. Dermatology 2009, 190, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, A.; Damiani, G.; Iacovelli, P.; Conic, R.R.Z.; Young Dermatologists Italian Network (YDIN); Gonzalez, S.; Morrone, A. NB-UVB plus Oral Polypodium Leucotomos Extract Display Higher Efficacy than NB-UVB Alone in Patients with Vitiligo. Dermatol. Ther. 2021, 34, e14776. [Google Scholar] [CrossRef]
- Reyes, E.; Jaén, P.; de las Heras, E.; de Eusebio, E.; Carrión, F.; Cuevas, J.; González, S.; Villarrubia, V.G.; Álvarez-Mon, M. Systemic Immunomodulatory Effects of Polypodium Leucotomos as an Adjuvant to PUVA Therapy in Generalized Vitiligo: A Pilot Study. J. Dermatol. Sci. 2006, 41, 213–216. [Google Scholar] [CrossRef]
- Middelkamp-Hup, M.; Bos, J.; Rius-Diaz, F.; Gonzalez, S.; Westerhof, W. Treatment of Vitiligo Vulgaris with Narrow-Band UVB and Oral Polypodium Leucotomos Extract: A Randomized Double-Blind Placebo-Controlled Study. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 942–950. [Google Scholar] [CrossRef]
- Salazar, G.Z.; Cedeño, M.B.; Román, V.P.; Pazmiño, R.U. Efecto del Polypodium leucotomos como adjuvante en la repigmentación inducida con UVB de banda estrecha en pacientes con vitíligo. Med. Cutanea Ibero-Lat.-Am. 2013, 41, 205–209. [Google Scholar]
- Dell’Anna, M.L.; Mastrofrancesco, A.; Sala, R.; Venturini, M.; Ottaviani, M.; Vidolin, A.P.; Leone, G.; Calzavara, P.G.; Westerhof, W.; Picardo, M. Antioxidants and Narrow band-UVB in the Treatment of Vitiligo: A Double-blind Placebo Controlled Trial. Clin. Exp. Dermatol. 2007, 32, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Colucci, R.; Dragoni, F.; Conti, R.; Pisaneschi, L.; Lazzeri, L.; Moretti, S. Evaluation of an Oral Supplement Containing Phyllanthus Emblica Fruit Extracts, Vitamin E, and Carotenoids in Vitiligo Treatment. Dermatol. Ther. 2015, 28, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Jayanth, D.P.; Pai, B.S.; Shenoi, S.D.; Balachandran, C. Efficacy of Antioxidants as an Adjunct to Photochemotherapy in Vitiligo: A Case Study of 30 Patients. Indian J. Dermatol. Venereol. Leprol. 2002, 68, 202–205. [Google Scholar] [PubMed]
- Iraji, F.; Haftbaradaran, E.; Davashi, S.; Zolfaghari-Baghbaderani, A.; Bokaii-Jazi, S. Comparing the Improvement of Unstable Vitiligo in Patients Treated by Topical PUVA-Therapy Alone, Topical PUVA-Therapy and Oral Vitamin D, and Topical PUVA-Therapy and Oral Vitamin D and Vitamin B12. J. Isfahan Med. Sch. 2017, 34, 1699–1705. [Google Scholar]
- Tjioe, M.; Gerritsen, M.J.P.; Juhlin, L.; van de Kerkhof, P.C.M. Treatment of Vitiligo Vulgaris with Narrow Band UVB (311 Nm) for One Year and the Effect of Addition of Folic Acid and Vitamin B12. Acta Derm. Venereol. 2002, 82, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Juhlin, L.; Olsson, M. Improvement of Vitiligo after Oral Treatment with Vitamin B12 and Folic Acid and the Importance of Sun Exposure. Acta Derm.-Venereol. 1997, 77, 460–462. [Google Scholar] [CrossRef]
- Don, P.; Iuga, A.; Dacko, A.; Hardick, K. Treatment of Vitiligo with Broadband Ultraviolet B and Vitamins. Int. J. Dermatol. 2006, 45, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Sendrasoa, F.A.; Ranaivo, I.M.; Sata, M.; Andrianarison, M.; Raharolahy, O.; Rakotoarisaona, M.F.; Razanakoto, N.H.; Ramarozatovo, L.S.; Rapelanoro Rabenja, F. Treatment Responses in Patients with Vitiligo to Very Potent Topical Corticosteroids Combined with Vitaminotherapy in Madagascar. Int. J. Dermatol. 2019, 58, 908–911. [Google Scholar] [CrossRef]
- Parsad, D.; Pandhi, R.; Juneja, A. Effectiveness of Oral Ginkgo Biloba in Treating Limited, Slowly Spreading Vitiligo. Clin. Exp. Dermatol. 2003, 28, 285–287. [Google Scholar] [CrossRef]
- Abu Raghif, A.; Ali, N.; Farhood, I.; Sahib, H.; Hameed, M. Evaluation of a Standardized Extract of Ginkgo Biloba in Vitiligo Remedy. Asian J. Pharm. Clin. Res. 2013, 6, 127–130. [Google Scholar]
- Szczurko, O.; Shear, N.; Taddio, A.; Boon, H. Ginkgo Biloba for the Treatment of Vitilgo Vulgaris: An Open Label Pilot Clinical Trial. BMC Complement. Altern. Med. 2011, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, L.; Wu, Y.; Gao, X.-H.; Chen, H.-D. Triple-Combination Treatment with Oral α-Lipoic Acid, Betamethasone Injection, and NB-UVB for Non-Segmental Progressive Vitiligo. J. Cosmet. Laser Ther. 2016, 18, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Tsiskarishvili, N.I.; Katsitadze, A.; Tsiskarishvili, N.V.; Tsiskarishvili, T.; Chitanava, L. Efficacy of combined use of antioxidative and phototherapy i the treatment of vitiligo. Georgian Med. News 2016, 52–57. [Google Scholar]
- Jalalmanesh, S.; Mansouri, P.; Rajabi, M.; Monji, F. Therapeutic Effects of Turmeric Topical Cream in Vitiligo: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. J. Cosmet. Dermatol. 2022, 21, 4454–4461. [Google Scholar] [CrossRef]
- Schallreuter, K.U.; Krüger, C.; Würfel, B.A.; Panske, A.; Wood, J.M. From Basic Research to the Bedside: Efficacy of Topical Treatment with Pseudocatalase PC-KUS in 71 Children with Vitiligo. Int. J. Dermatol. 2008, 47, 743–753. [Google Scholar] [CrossRef]
- Schallreuter, K.U.; Moore, J.; Behrens-Williams, S.; Panske, A.; Harari, M. Rapid Initiation of Repigmentation in Vitiligo with Dead Sea Climatotherapy in Combination with Pseudocatalase (PC-KUS). Int. J. Dermatol. 2002, 41, 482–487. [Google Scholar] [CrossRef]
- Soliman, M.; Samy, N.; Rafei, M.; Hegazy, M. Excimer Light Monotherapy vs Combined Excimer Light and Topical Antioxidants in the Treatment of Vitiligo. Lasers Surg. Med. 2014, 46, 17. [Google Scholar] [CrossRef]
- Yuksel, E.P.; Aydin, F.; Senturk, N.; Canturk, T.; Turanli, A.Y. Comparison of the Efficacy of Narrow Band Ultraviolet B and Narrow Band Ultraviolet B plus Topical Catalase-Superoxide Dismutase Treatment in Vitiligo Patients. Eur. J. Dermatol. 2009, 19, 341–344. [Google Scholar] [CrossRef]
- Alshiyab, D.M.; Al-qarqaz, F.A.; Muhaidat, J.M.; Alkhader, Y.S.; Al-sheyab, R.F.; Jafaar, S.I. Comparison of the Efficacy of Tacrolimus 0.1% Ointment and Tacrolimus 0.1% plus Topical Pseudocatalase/Superoxide Dismutase Gel in Children with Limited Vitiligo: A Randomized Controlled Trial. J. Dermatol. Treat. 2022, 33, 146–149. [Google Scholar] [CrossRef]
- Bakis-Petsoglou, S.; Le Guay, J.L.; Wittal, R. A Randomized, Double-blinded, Placebo-controlled Trial of Pseudocatalase Cream and Narrowband Ultraviolet B in the Treatment of Vitiligo. Br. J. Dermatol. 2009, 161, 910–917. [Google Scholar] [CrossRef]
- Naini, F.F.; Shooshtari, A.V.; Ebrahimi, B.; Molaei, R. The Effect of Pseudocatalase/Superoxide Dismutase in the Treatment of Vitiligo: A Pilot Study. J. Res. Pharm. Pract. 2012, 1, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Kostović, K.; Pastar, Z.; Pasić, A.; Ceović, R. Treatment of Vitiligo with Narrow-Band UVB and Topical Gel Containing Catalase and Superoxide Dismutase. Acta Dermatovenerol. Croat. 2007, 15, 10–14. [Google Scholar] [PubMed]
- Patel, D.C.; Evans, A.V.; Hawk, J.L.M. Topical Pseudocatalase Mousse and Narrowband UVB Phototherapy Is Not Effective for Vitiligo: An Open, Single-centre Study. Clin. Exp. Dermatol. 2002, 27, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Schallreuter, K.U.; Panske, A.; Chiuchiarelli, G. Ineffective Topical Treatment of Vitiligo with Cucumis Melo Extracts. Int. J. Dermatol. 2011, 50, 374–375. [Google Scholar] [CrossRef]
- Mohammad, A. Vitiligo Repigmentation with Anapsos (Polypodium leucotomos). Int. J. Dermatol. 1989, 28, 479. [Google Scholar]
- Elgoweini, M.; Din, N.N.E. Response of Vitiligo to Narrowband Ultraviolet B and Oral Antioxidants. J. Clin. Pharmacol. 2009, 49, 852–855. [Google Scholar] [CrossRef]
- Sun, Y.; Guan, X.; Wang, H.; Zhang, J.; Gu, H.; Lu, H.; Yao, Z.; Chen, X.; Zeng, F.; Wu, Y.; et al. Randomized Clinical Trial of Combined Therapy with Oral α-Lipoic Acid and NB-UVB for Nonsegmental Stable Vitiligo. Dermatol. Ther. 2021, 34, e14610. [Google Scholar] [CrossRef]
- El Attar, Y.; Doghaim, N.; El Far, N.; El hedody, S.; Hawwam, S.A. Efficacy and Safety of Tranexamic Acid versus Vitamin c after Microneedling in Treatment of Melasma: Clinical and Dermoscopic Study. J. Cosmet. Dermatol. 2022, 21, 2817–2825. [Google Scholar] [CrossRef]
- Zhao, H.; Li, M.; Zhang, X.; Li, L.; Yan, Y.; Wang, B. Comparing the Efficacy of Myjet-Assisted Tranexamic Acid and Vitamin C in Treating Melasma: A Split-Face Controlled Trial. J. Cosmet. Dermatol. 2020, 19, 47–54. [Google Scholar] [CrossRef]
- Sobhi, R.M.; Sobhi, A.M. A Single-Blinded Comparative Study between the Use of Glycolic Acid 70% Peel and the Use of Topical Nanosome Vitamin C Iontophoresis in the Treatment of Melasma. J. Cosmet. Dermatol. 2012, 11, 65–71. [Google Scholar] [CrossRef]
- Soliman, M.M.; Ramadan, S.A.-R.; Bassiouny, D.A.; Abdelmalek, M. MSc Combined Trichloroacetic Acid Peel and Topical Ascorbic Acid versus Trichloroacetic Acid Peel Alone in the Treatment of Melasma: A Comparative Study. J. Cosmet. Dermatol. 2007, 6, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Ustuner, P.; Balevi, A.; Ozdemir, M. A Split-Face, Investigator-Blinded Comparative Study on the Efficacy and Safety of Q-Switched Nd:YAG Laser plus Microneedling with Vitamin C versus Q-Switched Nd:YAG Laser for the Treatment of Recalcitrant Melasma. J. Cosmet. Laser Ther. 2017, 19, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Dayal, S. Clinical Efficacy and Safety on Combining 20% Trichloroacetic Acid Peel with Topical 5% Ascorbic Acid for Melasma. J. Clin. Diagn. Res. 2017, 11, WC08–WC11. [Google Scholar] [CrossRef] [PubMed]
- Pazyar, N.; Molavi, S.N.; Hosseinpour, P.; Hadibarhaghtalab, M.; Parvar, S.Y.; Dezfuly, M.B. Efficacy of Intradermal Injection of Tranexamic Acid and Ascorbic Acid versus Tranexamic Acid and Placebo in the Treatment of Melasma: A Split-Face Comparative Trial. Health Sci. Rep. 2022, 5, e537. [Google Scholar] [CrossRef] [PubMed]
- Balevi, A.; Ustuner, P.; Özdemir, M. Salicylic Acid Peeling Combined with Vitamin C Mesotherapy versus Salicylic Acid Peeling Alone in the Treatment of Mixed Type Melasma: A Comparative Study. J. Cosmet. Laser Ther. 2017, 19, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Kim, S.J.; Lee, J.B.; Yoo, H.S. Clinical Evaluation of the Brightening Effect of Chitosan-Based Cationic Liposomes. J. Cosmet. Dermatol. 2022, 21, 6822–6829. [Google Scholar] [CrossRef] [PubMed]
- Hakozaki, T.; Minwalla, L.; Zhuang, J.; Chhoa, M.; Matsubara, A.; Miyamoto, K.; Greatens, A.; Hillebrand, G.G.; Bissett, D.L.; Boissy, R.E. The Effect of Niacinamide on Reducing Cutaneous Pigmentation and Suppression of Melanosome Transfer. Br. J. Dermatol. 2002, 147, 20–31. [Google Scholar] [CrossRef]
- Giasante, E. Melasma Treatment: Comparative Study between Triple Combination vs. Topical Niacinamide and Triple Combination vs Tranexamic Intradermal Acid. J. Dermatol. Nurses’ Assoc. 2020, 12. [Google Scholar]
- Navarrete-Solís, J.; Castanedo-Cázares, J.P.; Torres-Álvarez, B.; Oros-Ovalle, C.; Fuentes-Ahumada, C.; González, F.J.; Martínez-Ramírez, J.D.; Moncada, B. A Double-Blind, Randomized Clinical Trial of Niacinamide 4% versus Hydroquinone 4% in the Treatment of Melasma. Dermatol. Res. Pract. 2011, 2011, 379173. [Google Scholar] [CrossRef]
- Farshi, S.; Mansouri, P.; Kasraee, B. Efficacy of Cysteamine Cream in the Treatment of Epidermal Melasma, Evaluating by Dermacatch as a New Measurement Method: A Randomized Double Blind Placebo Controlled Study. J. Dermatol. Treat. 2018, 29, 182–189. [Google Scholar] [CrossRef]
- Mansouri, P.; Farshi, S.; Hashemi, Z.; Kasraee, B. Evaluation of the Efficacy of Cysteamine 5% Cream in the Treatment of Epidermal Melasma: A Randomized Double-Blind Placebo-Controlled Trial. Br. J. Dermatol. 2015, 173, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Lima, P.B.; Dias, J.A.F.; Cassiano, D.; Esposito, A.C.C.; Bagatin, E.; Miot, L.D.B.; Miot, H.A. A Comparative Study of Topical 5% Cysteamine versus 4% Hydroquinone in the Treatment of Facial Melasma in Women. Int. J. Dermatol. 2020, 59, 1531–1536. [Google Scholar] [CrossRef] [PubMed]
- Sepaskhah, M.; Karimi, F.; Bagheri, Z.; Kasraee, B. Comparison of the Efficacy of Cysteamine 5% Cream and Hydroquinone 4%/Ascorbic Acid 3% Combination Cream in the Treatment of Epidermal Melasma. J. Cosmet. Dermatol. 2022, 21, 2871–2878. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.; Remyn, L.; Chung, Y.; Honigman, A.; Wutami, I.; Mane, S.; Wong, C.; Rogrigues, M. Evaluation of the Efficacy of Cysteamine Cream Compared to Hydroquinone in the Treatment of Melasma: A Randomised, Double-Blinded, Tria. Australas. J. Dermatol. 2021, 62, e41–e46. [Google Scholar] [CrossRef] [PubMed]
- Karrabi, M.; Mansournia, M.A.; Sharestanaki, E.; Abdollahnejad, Y.; Sahebkar, M. Clinical Evaluation of Efficacy and Tolerability of Cysteamine 5% Cream in Comparison with Tranexamic Acid Mesotherapy in Subjects with Melasma: A Single-Blind, Randomized Clinical Trial Study. Arch. Dermatol. Res. 2021, 313, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Nofal, A.; Ibrahim, A.-S.M.; Nofal, E.; Gamal, N.; Osman, S. Topical Silymarin versus Hydroquinone in the Treatment of Melasma: A Comparative Study. J. Cosmet. Dermatol. 2019, 18, 263–270. [Google Scholar] [CrossRef]
- Wattanakrai, P.; Nimmannitya, K. A Randomized, Double-Blind, Split-Face Study of Topical Silymarin vs 2% Hydroquinone Cream in Melasmas. J. Drugs Dermatol. 2022, 21, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.M.A.; Farag, A.S.; Ali, M.S.; El-Gendy, W.M.A.F. Efficacy and Safety of Topical Silymarin Versus Low Fluence 1064-Nm Q Switched Nd:YAG Laser in the Treatment of Melasma: A Comparative Randomized Trial. Lasers Surg. Med. 2021, 53, 1341–1347. [Google Scholar] [CrossRef]
- Goh, C.-L.; Chuah, S.Y.; Tien, S.; Thng, G.; Vitale, M.A.; Delgado-Rubin, A. Double-Blind, Placebo-Controlled Trial to Evaluate the Effectiveness of Polypodium Leucotomos Extract in the Treatment of Melasma in Asian Skin. J. Clin. Aesthet. Dermatol. 2018, 11, 14–19. [Google Scholar]
- Ahmed, A.M.; Lopez, I.; Perese, F.; Vasquez, R.; Hynan, L.S.; Chong, B.; Pandya, A.G. A Randomized, Double-Blinded, Placebo-Controlled Trial of Oral Polypodium Leucotomos Extract as an Adjunct to Sunscreen in the Treatment of Melasma. JAMA Dermatol. 2013, 149, 981–983. [Google Scholar] [CrossRef]
- Martin, L.K.; Caperton, C.; Woolery-Lloyd, H.; Avashia, N. A Randomized Double-Blind Placebo Controlled Study Evaluating the Effectiveness and Tolerability of Oral Polypodium Leucotomos in Patients with Melasma. J. Am. Acad. Dermatol. 2012, 66, AB21. [Google Scholar] [CrossRef]
- Akl, E.M. Liposomal Azelaic Acid 20% Cream vs Hydroquinone 4% Cream as Adjuvant to Oral Tranexamic Acid in Melasma: A Comparative Study. J. Dermatol. Treat. 2022, 33, 2008–2013. [Google Scholar] [CrossRef] [PubMed]
- Das, N.; Rahaman, S.; Mondal, N.; Patra, A.; Sil, A.; Ghosh, A. Comparison of the Efficacy, Tolerability and Safety of 10% Tranexemic Acid Cream versus 20% Azelaic Acid Cream in Melasma: A Split Face, Double-Blind Randomised Controlled Trial. J. Dermatol. Nurses’ Assoc. 2020, 12, 2. [Google Scholar]
- Malik, F.; Hanif, M.; Mustafa, G. Combination of Oral Tranexamic Acid with Topical 3% Tranexamic Acid versus Oral Tranexamic Acid with Topical 20% Azelaic Acid in the Treatment of Melasma. J. Coll. Physicians Surg. Pak. 2019, 29, 502–504. [Google Scholar] [CrossRef]
- Emad, M.; Moezzi, J.; Dastgheib, L. Therapeutic Efficacy of a Cream Based Azelaic Acid 20% versus Hydroquinone 4% in Patients with Melasma. Iran J. Dermatol. 2013, 16, 13–16. [Google Scholar]
- Arpornpattanapong, J.; Vejjabhinanta, V.; Tanasombatkul, K.; Phinyo, P. The Effectiveness and Safety of Using 2.3% Diclofenac Gel and 20% Azelaic Acid Cream for Melasma: A Single-Blind, Split-Face Study. J. Dermatol. Treat. 2023, 34, AB233. [Google Scholar] [CrossRef]
- Afriliana, L.; Budipradigda, L.; Djamiatun, K. The Effect of Tomato Extract Supplementation to Interleukin-17 Serum Level in Women with Melasma. Int. J. Pharm. Res. 2020, 12, 3660–3666. [Google Scholar] [CrossRef]
- Bavarsad, N.; Mapar, M.A.; Safaezadeh, M.; Latifi, S.M. A Double-Blind, Placebo-Controlled Randomized Trial of Skin-Lightening Cream Containing Lycopene and Wheat Bran Extract on Melasma. J. Cosmet. Dermatol. 2021, 20, 1795–1800. [Google Scholar] [CrossRef]
- Iraji, F.; Tagmirriahi, N.; Gavidnia, K. Comparison between the Efficacy of 10% Zinc Sulfate Solution with 4% Hydroquinone Cream on Improvement of Melasma. Adv. Biomed. Res. 2012, 1, 39. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, A.; Khani Khoozani, Z.; Zakerzadeh Forooshani, S.; Omrani, N.; Moini, A.M.; Eskandari, Y. Is Topical Zinc Effective in the Treatment of Melasma? A Double-Blind Randomized Comparative Study. Dermatol. Surg. 2014, 40, 33–37. [Google Scholar] [CrossRef]
- Alvin, G.; Catambay, N.; Vergara, A.; Jamora, M.J. A Comparative Study of the Safety and Efficacy of 75% Mulberry (Morus Alba) Extract Oil versus Placebo as a Topical Treatment for Melasma: A Randomized, Single-Blind, Placebo-Controlled Trial. J. Drugs Dermatol. 2011, 10, 1025–1031. [Google Scholar] [PubMed]
- Lima, P.B.; Dias, J.A.F.; Esposito, A.C.C.; Miot, L.D.B.; Miot, H.A. French Maritime Pine Bark Extract (Pycnogenol) in Association with Triple Combination Cream for the Treatment of Facial Melasma in Women: A Double-Blind, Randomized, Placebo-Controlled Trial. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 502–508. [Google Scholar] [CrossRef]
- Mohamed, M.; Beshay, Y.M.A.; Assaf, H.M. Microneedling with Glutathione versus Microneedling Alone in Treatment of Facial Melasma: Split-Face Comparative Study. J. Cosmet. Dermatol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Khemis, A.; Kaiafa, A.; Queille-Roussel, C.; Duteil, L.; Ortonne, J.P. Evaluation of Efficacy and Safety of Rucinol Serum in Patients with Melasma: A Randomized Controlled Trial. Br. J. Dermatol. 2007, 156, 997–1004. [Google Scholar] [CrossRef]
- Khosravan, S.; Alami, A.; Mohammadzadeh-Moghadam, H.; Ramezani, V. The Effect of Topical Use of Petroselinum Crispum (Parsley) Versus That of Hydroquinone Cream on Reduction of Epidermal Melasma: A Randomized Clinical Trial. Holist. Nurs. Pract. 2017, 31, 16–20. [Google Scholar] [CrossRef]
- Akram, S.; Sattar, F.; Tahir, R.; Mujtaba, G. Efficacy of Topical 4% Liquiritin Compared with Topical 4% Liquiritin Mixed in 5% Ascorbic Acid in the Treatment of Melasma. J. Pak. Assoc. Dermatol. 2013, 23, 149–152. [Google Scholar]
- Huh, C.-H.; Seo, K.-I.; Park, J.-Y.; Lim, J.-G.; Eun, H.-C.; Park, K.-C. A Randomized, Double-Blind, Placebo-Controlled Trial of Vitamin C Iontophoresis in Melasma. Dermatology 2003, 206, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y. Efficacy and Safety Analysis of Medlite C6 Q-1064 Laser Combined with a Topical Antioxidant Serum Containing Vitamin C, Vitamin E, and Ferulic Acid in the Treatment of Melasma. J. Investig. Dermatol. 2023, 143, S223. [Google Scholar]
- Lee, M.-C.; Chang, C.-S.; Huang, Y.-L.; Chang, S.-L.; Chang, C.-H.; Lin, Y.-F.; Hu, S. Treatment of Melasma with Mixed Parameters of 1,064-Nm Q-Switched Nd:YAG Laser Toning and an Enhanced Effect of Ultrasonic Application of Vitamin C: A Split-Face Study. Lasers Med. Sci. 2015, 30, 159–163. [Google Scholar] [CrossRef]
- Abdel-Rahman, A.T.; Abdel-Hakeem, F.G.; Ragaie, M.H. Clinical, Dermoscopic, and Histopathologic Evaluation of Vitamin C versus PRP, with Microneedling in the Treatment of Mixed Melasma: A Split-Face, Comparative Study. Dermatol. Ther. 2022, 35, e15239. [Google Scholar] [CrossRef]
- Choi, Y.K.; Rho, Y.K.; Yoo, K.H.; Lim, Y.Y.; Li, K.; Kim, B.J.; Seo, S.J.; Kim, M.N.; Hong, C.K.; Kim, D.-S. Effects of Vitamin C vs. Multivitamin on Melanogenesis: Comparative Study in Vitro and in Vivo. Int. J. Dermatol. 2010, 49, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Raza, M.H.; Iftikhar, N.; Anwar, A.; Mashhood, A.A.; Tariq, S.; Hamid, M.A.B. Split-Face Comparative Analysis of Micro-Needling with Tranexamic Acid vs Vitamin C Serum in Melasma. J. Ayub Med. Coll. Abbottabad 2022, 34, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Tadokoro, T.; Bonté, F.; Archambault, J.C.; Cauchard, J.H.; Neveu, M.; Ozawa, K.; Noguchi, F.; Ikeda, A.; Nagamatsu, M.; Shinn, S. Whitening Efficacy of Plant Extracts Including Orchid Extracts on Japanese Female Skin with Melasma and Lentigo Senilis. J. Dermatol. 2010, 37, 522–530. [Google Scholar] [CrossRef]
- Tahoun, A.I.; Mostafa, W.Z.; Amer, M.A. Dermoscopic Evaluation of Tranexamic Acid versus Vitamin C, with Microneedling in the Treatment of Melasma: A Comparative, Split-Face, Single-Blinded Study. J. Dermatol. Treat. 2022, 33, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Espinal-Perez, L.E.; Moncada, B.; Castanedo-Cazares, J.P. A Double-Blind Randomized Trial of 5% Ascorbic Acid vs. 4% Hydroquinone in Melasma. Int. J. Dermatol. 2004, 43, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Campuzano-García, A.E.; Torres-Alvarez, B.; Hernández-Blanco, D.; Fuentes-Ahumada, C.; Cortés-García, J.D.; Castanedo-Cázares, J.P. DNA Methyltransferases in Malar Melasma and Their Modification by Sunscreen in Combination with 4% Niacinamide, 0.05% Retinoic Acid, or Placebo. Biomed. Res. Int. 2019, 2019, 9068314. [Google Scholar] [CrossRef] [PubMed]
- Goh, C.-L.; Thng, S.; Kumar, S.; Tan, W.P. A Double Blind Randomized Controlled Trial to Evaluate the Efficacy of a Niacinamide Containing Cream in the Treatment of Melasma. J. Dermatol. 2012, 39 (Suppl. 1), 219–220. [Google Scholar]
- Altaei, T. The Treatment of Melasma by Silymarin Cream. BMC Dermatol. 2012, 12, 18. [Google Scholar] [CrossRef]
- Avianggi, H.D.; Indar, R.; Adriani, D.; Riyanto, P.; Muslimin, M.; Afriliana, L.; Kabulrachman, K. The Effectiveness of Tomato Extract on Superoxide Dismutase (SOD) and Severity Degree of Patients with Melasma. Ital. J. Dermatol. Venerol. 2022, 157, 262–269. [Google Scholar] [CrossRef]
- Iraji, F.; Nasimi, M.; Asilian, A.; Faghihi, G.; Mozafarpoor, S.; Hafezi, H. Efficacy of Mesotherapy with Tranexamic Acid and Ascorbic Acid with and without Glutathione in Treatment of Melasma: A Split Face Comparative Trial. J. Cosmet. Dermatol. 2019, 18, 1416–1421. [Google Scholar] [CrossRef]
- Zattra, E.; Coleman, C.; Arad, S.; Helms, E.; Levine, D.; Bord, E.; Guillaume, A.; El-Hajahmad, M.; Zwart, E.; van Steeg, H.; et al. Polypodium Leucotomos Extract Decreases UV-Induced Cox-2 Expression and Inflammation, Enhances DNA Repair, and Decreases Mutagenesis in Hairless Mice. Am. J. Pathol. 2009, 175, 1952–1961. [Google Scholar] [CrossRef]
- Portillo, M.; Mataix, M.; Alonso-Juarranz, M.; Lorrio, S.; Villalba, M.; Rodríguez-Luna, A.; González, S. The Aqueous Extract of Polypodium Leucotomos (Fernblock®) Regulates Opsin 3 and Prevents Photooxidation of Melanin Precursors on Skin Cells Exposed to Blue Light Emitted from Digital Devices. Antioxidants 2021, 10, 400. [Google Scholar] [CrossRef] [PubMed]
- Schalka, R.; Vitale-Villarejo, M.A.; Agelune, C.M.; Bombarda, P.C.P. Benefícios do uso de um composto contendo extrato de polypodium loucotomos na redução da pigmentação e do eritema decorrentes da radiação ultravioleta. Surg. Cosmet. Dermatol. 2014, 6, 344–348. [Google Scholar]
- Cefali, L.C.; Ataide, J.A.; Fernandes, A.R.; Sanchez-Lopez, E.; de O. Sousa, I.M.; Figueiredo, M.C.; Ruiz, A.L.T.G.; Foglio, M.A.; Mazzola, P.G.; Souto, E.B. Evaluation of In Vitro Solar Protection Factor (SPF), Antioxidant Activity, and Cell Viability of Mixed Vegetable Extracts from Dirmophandra mollis Benth, Ginkgo biloba L., Ruta graveolens L., and Vitis vinífera L. Plants 2019, 8, 453. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, J.; Yang, B.; Zheng, Y.; Yao, M.; Sun, M.; Xu, L.; Lin, C.; Chang, D.; Tian, F. Ginkgo Biloba Extract Inhibits Astrocytic Lipocalin-2 Expression and Alleviates Neuroinflammatory Injury via the JAK2/STAT3 Pathway After Ischemic Brain Stroke. Front. Pharmacol. 2018, 9, 518. [Google Scholar] [CrossRef]
- Mousavi, S.N.; Hosseinikia, M.; Yousefi Rad, E.; Saboori, S. Beneficial Effects of Ginkgo Biloba Leaf Extract on Inflammatory Markers: A Systematic Review and Meta-Analysis of the Clinical Trials. Phytother. Res. 2022, 36, 3459–3469. [Google Scholar] [CrossRef] [PubMed]
- Ku, B.; Kim, D.; Choi, E.-M. Anti-Melanogenic Effect of the Aqueous Ethanol Extract of Ginkgo Biloba Leaf in B16F10 Cells. Toxicol. Environ. Health Sci. 2020, 12, 287–295. [Google Scholar] [CrossRef]
- Klomsakul, P.; Aiumsubtub, A.; Chalopagorn, P. Evaluation of Antioxidant Activities and Tyrosinase Inhibitory Effects of Ginkgo biloba Tea Extract. Sci. World J. 2022, 2022, e4806889. [Google Scholar] [CrossRef] [PubMed]
- Telang, P.S. Vitamin C in Dermatology. Indian Dermatol. Online J. 2013, 4, 143–146. [Google Scholar] [CrossRef]
- Lewis, E.D.; Meydani, S.N.; Wu, D. Regulatory Role of Vitamin E in the Immune System and Inflammation. IUBMB Life 2019, 71, 487–494. [Google Scholar] [CrossRef]
- Hung, C.; Lin, Y.; Zhang, L.; Chang, C.; Fang, J. Topical Delivery of Silymarin Constituents via the Skin Route. Acta Pharmacol. Sin. 2010, 31, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Wohlrab, J.; Kreft, D. Niacinamide-Mechanisms of Action and Its Topical Use in Dermatology. Ski. Pharmacol. Physiol. 2014, 27, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Jiang, H.; Li, W.; Qiang, M.; Dong, T.; Li, H. Role of Vitamin C in Skin Diseases. Front. Physiol. 2018, 9, 819. [Google Scholar] [CrossRef]
- Li, N.; Wu, X.; Jia, W.; Zhang, M.C.; Tan, F.; Zhang, J. Effect of Ionization and Vehicle on Skin Absorption and Penetration of Azelaic Acid. Drug Dev. Ind. Pharm. 2012, 38, 985–994. [Google Scholar] [CrossRef]
- Hwang, S.-W.; Oh, D.-J.; Lee, D.; Kim, J.-W.; Park, S.-W. Clinical Efficacy of 25% L-Ascorbic Acid (C’ensil) in the Treatment of Melasma. J. Cutan. Med. Surg. 2009, 13, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Ismail, E.S.A.; Patsatsi, A.; Abd el-Maged, W.M.; Nada, E.E.-D.A. el-Aziz Efficacy of Microneedling with Topical Vitamin C in the Treatment of Melasma. J. Cosmet. Dermatol. 2019, 18, 1342–1347. [Google Scholar] [CrossRef]
- Kelm, R.C.; Zahr, A.S.; Kononov, T.; Ibrahim, O. Effective Lightening of Facial Melasma during the Summer with a Dual Regimen: A Prospective, Open-Label, Evaluator-Blinded Study. J. Cosmet. Dermatol. 2020, 19, 3251–3257. [Google Scholar] [CrossRef]
- Yoo, J.M.; Park, H.J.; Choi, S.W.; Kim, H.O. Vitamin C-iontophoresis in Melasma. Korean J. Dermatol. 2014, 39, 285–291. [Google Scholar]
- Campos, V.; Pitassi, L. Oral Administration of Pycnogenol Associated with Sunscreen Improve Clinical Symptoms of Melasma. J. Am. Acad. Dermatol. 2014, 70, AB19. [Google Scholar] [CrossRef]
- Ni, Z.; Mu, Y.; Gulati, O. Treatment of Melasma with Pycnogenol®. Phytother. Res. 2002, 16, 567–571. [Google Scholar] [CrossRef]
- Hsu, C.; Ahmadi, S.; Pourahmad, M.; Ali Mahdi, H. Cysteamine cream as a new skin depigmenting product. Pigment. Cell Melanoma Res. 2012, 25, 645–675. [Google Scholar] [CrossRef]
- Kar, H.K. Efficacy of Beta-Carotene Topical Application in Melasma: An Open Clinical Trial. Indian J. Dermatol. Venereol. Leprol. 2002, 68, 320–322. [Google Scholar] [PubMed]
- Park, H.S.; Choi, J.C.; Chun, D.K.; Lee, Y.S. The Efficacy of Peeling with Amino Acid Filaggrin Based Antioxidants(AFAs). Korean J. Dermatol. 2015, 41, 1487–1493. [Google Scholar]
- Sharquie, K.E.; Al-Mashhadani, S.A.; Salman, H.A. Topical 10% Zinc Sulfate Solution for Treatment of Melasma. Dermatol. Surg. 2008, 34, 1346–1349. [Google Scholar] [CrossRef]
- Song, M.; Mun, J.-H.; Ko, H.-C.; Kim, B.-S.; Kim, M.-B. Korean Red Ginseng Powder in the Treatment of Melasma: An Uncontrolled Observational Study. J. Ginseng Res. 2011, 35, 170–175. [Google Scholar] [CrossRef]
- Yamakoshi, J.; Sano, A.; Tokutake, S.; Saito, M.; Kikuchi, M.; Kubota, Y.; Kawachi, Y.; Otsuka, F. Oral Intake of Proanthocyanidin-Rich Extract from Grape Seeds Improves Chloasma. Phytother. Res. 2004, 18, 895–899. [Google Scholar] [CrossRef]
- Yokoyama, M.; Itoh, Y. Clinical Evaluation of the Use of Whitening Cream Containing Ellagic Acid for the Treatment of Skin Pigmentation Conditions. Ski. Res. 2001, 43, 286–291. [Google Scholar]
- Gonzalez, S.; Alcaraz, M.V.; Cuevas, J.; Perez, M.; Jaen, P.; Alvarez-Mon, M.; Villarrubia, V.G. An Extract of the Fern Polypodium Leucotomos (Difur) Modulates Th1/Th2 Cytokines Balance in Vitro and Appears to Exhibit Anti-Angiogenic Activities in Vivo: Pathogenic Relationships and Therapeutic Implications. Anticancer Res. 2000, 20, 1567–1575. [Google Scholar] [PubMed]
- Gustafson, C.B.; Yang, C.; Dickson, K.M.; Shao, H.; Van Booven, D.; Harbour, J.W.; Liu, Z.-J.; Wang, G. Epigenetic Reprogramming of Melanoma Cells by Vitamin C Treatment. Clin. Epigenetics 2015, 7, 51. [Google Scholar] [CrossRef]
- Gęgotek, A.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Activity of Ascorbic Acid. Antioxidants 2022, 11, 1993. [Google Scholar] [CrossRef]
- Kang, J.S.; Kim, H.N.; Jung, D.J.; Kim, J.E.; Mun, G.H.; Kim, Y.S.; Cho, D.; Shin, D.H.; Hwang, Y.-I.; Lee, W.J. Regulation of UVB-Induced IL-8 and MCP-1 Production in Skin Keratinocytes by Increasing Vitamin C Uptake via the Redistribution of SVCT-1 from the Cytosol to the Membrane. J. Investig. Dermatol. 2007, 127, 698–706. [Google Scholar] [CrossRef]
- Eberlein-König, B.; Ring, J. Relevance of Vitamins C and E in Cutaneous Photoprotection. J. Cosmet. Dermatol. 2005, 4, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Kamei, Y.; Otsuka, Y.; Abe, K. Comparison of the Inhibitory Effects of Vitamin E Analogues on Melanogenesis in Mouse B16 Melanoma Cells. Cytotechnology 2009, 59, 183–190. [Google Scholar] [CrossRef]
- Endo, K.; Osawa, S.; Mizutani, T.; Miyaguchi, Y.; Okano, Y.; Masaki, H. A Potential of α-Tocopherol Fatty Acid Ester as an Anti-Pigmentation Agent. J. Jpn. Cosmet. Sci. Soc. 2020, 44, 283–288. [Google Scholar] [CrossRef]
- Asbaghi, O.; Sadeghian, M.; Nazarian, B.; Sarreshtedari, M.; Mozaffari-Khosravi, H.; Maleki, V.; Alizadeh, M.; Shokri, A.; Sadeghi, O. The Effect of Vitamin E Supplementation on Selected Inflammatory Biomarkers in Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Sci. Rep. 2020, 10, 17234. [Google Scholar] [CrossRef] [PubMed]
- Nazrun, A.S.; Norazlina, M.; Norliza, M.; Nirwana, S.I. The Anti-Inflammatory Role of Vitamin E in Prevention of Osteoporosis. Adv. Pharmacol. Sci. 2012, 2012, 142702. [Google Scholar] [CrossRef]
- Cook-Mills, J.M.; McCary, C.A. Isoforms of vitamin e differentially regulate inflammation. Endocr. Metab. Immune Disord. Drug Targets 2010, 10, 348–366. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Koga, T.; Martin, K.R.; Meydani, M. Effect of Vitamin E on Human Aortic Endothelial Cell Production of Chemokines and Adhesion to Monocytes. Atherosclerosis 1999, 147, 297–307. [Google Scholar] [CrossRef]
- Werninghaus, K.; Meydani, M.; Bhawan, J.; Margolis, R.; Blumberg, J.B.; Gilchrest, B.A. Evaluation of the Photoprotective Effect of Oral Vitamin E Supplementation. Arch. Dermatol. 1994, 130, 1257–1261. [Google Scholar] [CrossRef]
- Mireles-Rocha, H.; Galindo, I.; Huerta, M.; Trujillo-Hernández, B.; Elizalde, A.; Cortés-Franco, R. UVB Photoprotection with Antioxidants: Effects of Oral Therapy with d-Alpha-Tocopherol and Ascorbic Acid on the Minimal Erythema Dose. Acta Derm. Venereol. 2002, 82, 21–24. [Google Scholar] [CrossRef]
- Kim, H.-Y.; Sah, S.K.; Choi, S.S.; Kim, T.-Y. Inhibitory Effects of Extracellular Superoxide Dismutase on Ultraviolet B-Induced Melanogenesis in Murine Skin and Melanocytes. Life Sci. 2018, 210, 201–208. [Google Scholar] [CrossRef]
- Yasui, K.; Baba, A. Therapeutic Potential of Superoxide Dismutase (SOD) for Resolution of Inflammation. Inflamm. Res. 2006, 55, 359–363. [Google Scholar] [CrossRef]
- Takayanagi, S.; Suzuki, H.; Yokozawa, M.; Yamauchi, K. The Effect of Intake of GliSODin on Minimal Erythema Dose (MED), a Randomised, Double-Blind, Placebo-Controlled, Parallel-Group Study of Healthy Japanese. Pharmacometrics 2016, 90, 77–81. [Google Scholar]
- Kim, Y.; Lee, Y.; Lee, J.; Yi, Y. Inhibitory Effect of Ginkgo Biloba Extracts on Melanin Biosynthesis. J. Soc. Cosmet. Sci. Korea 2015, 41, 383–389. [Google Scholar] [CrossRef]
- Plonka, P.M.; Handjiski, B.; Michalczyk, D.; Popik, M.; Paus, R. Oral Zinc Sulphate Causes Murine Hair Hypopigmentation and Is a Potent Inhibitor of Eumelanogenesis in Vivo. Br. J. Dermatol. 2006, 155, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Rudolf, E.; Rudolf, K. Increases in Intracellular Zinc Enhance Proliferative Signaling as Well as Mitochondrial and Endolysosomal Activity in Human Melanocytes. Cell. Physiol. Biochem. 2017, 43, 1–16. [Google Scholar] [CrossRef]
- Prasad, A.S. Clinical, Immunological, Anti-Inflammatory and Antioxidant Roles of Zinc. Exp. Gerontol. 2008, 43, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Lei, T.C.; Virador, V.M.; Vieira, W.D.; Hearing, V.J. A Melanocyte–Keratinocyte Coculture Model to Assess Regulators of Pigmentation in Vitro. Anal. Biochem. 2002, 305, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Yiasemides, E.; Sivapirabu, G.; Halliday, G.M.; Park, J.; Damian, D.L. Oral Nicotinamide Protects against Ultraviolet Radiation-Induced Immunosuppression in Humans. Carcinogenesis 2009, 30, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.; Wang, H.; Zhao, L.; Bai, Y.; Xie, F.; He, J.; Lv, C. Niacin Downregulates Chemokine (c-c Motif) Ligand 2 (CCL2) Expression and Inhibits Fat Synthesis in Rat Liver Cells. Trop. J. Pharm. Res. 2020, 19, 977–982. [Google Scholar] [CrossRef]
- Snaidr, V.A.; Damian, D.L.; Halliday, G.M. Nicotinamide for Photoprotection and Skin Cancer Chemoprevention: A Review of Efficacy and Safety. Exp. Dermatol. 2019, 28, 15–22. [Google Scholar] [CrossRef]
- Atallah, C.; Viennet, C.; Robin, S.; Ibazizen, S.; Greige-Gerges, H.; Charcosset, C. Effect of Cysteamine Hydrochloride-Loaded Liposomes on Skin Depigmenting and Penetration. Eur. J. Pharm. Sci. 2022, 168, 106082. [Google Scholar] [CrossRef]
- Ahmad, F.; Mitchell, R.D.; Houben, T.; Palo, A.; Yadati, T.; Parnell, A.J.; Patel, K.; Shiri-Sverdlov, R.; Leake, D.S. Cysteamine Decreases Low-Density Lipoprotein Oxidation, Causes Regression of Atherosclerosis, and Improves Liver and Muscle Function in Low-Density Lipoprotein Receptor–Deficient Mice. J. Am. Heart Assoc. 2021, 10, e017524. [Google Scholar] [CrossRef]
- Choo, S.-J.; Ryoo, I.-J.; Kim, Y.-H.; Xu, G.-H.; Kim, W.-G.; Kim, K.-H.; Moon, S.-J.; Son, E.-D.; Bae, K.; Yoo, I.-D. Silymarin Inhibits Melanin Synthesis in Melanocyte Cells. J. Pharm. Pharmacol. 2009, 61, 663–667. [Google Scholar] [CrossRef]
- Tsaroucha, A.K.; Valsami, G.; Kostomitsopoulos, N.; Lambropoulou, M.; Anagnostopoulos, C.; Christodoulou, E.; Falidas, E.; Betsou, A.; Pitiakoudis, M.; Simopoulos, C.E. Silibinin Effect on Fas/FasL, HMGB1, and CD45 Expressions in a Rat Model Subjected to Liver Ischemia-Reperfusion Injury. J. Investig. Surg. 2018, 31, 491–502. [Google Scholar] [CrossRef]
- Lin, Z.-Y.; Chuang, W.-L. Influence of Silibinin on Differential Expressions of Total Cytokine Genes in Human Hepatocellular Carcinoma Cell Lines. Biomed. Prev. Nutr. 2011, 1, 91–94. [Google Scholar] [CrossRef]
- Trappoliere, M.; Caligiuri, A.; Schmid, M.; Bertolani, C.; Failli, P.; Vizzutti, F.; Novo, E.; di Manzano, C.; Marra, F.; Loguercio, C.; et al. Silybin, a Component of Sylimarin, Exerts Anti-Inflammatory and Anti-Fibrogenic Effects on Human Hepatic Stellate Cells. J. Hepatol. 2009, 50, 1102–1111. [Google Scholar] [CrossRef]
- Katiyar, S.K.; Meleth, S.; Sharma, S.D. Silymarin, a Flavonoid from Milk Thistle (Silybum marianum L.), Inhibits UV-Induced Oxidative Stress Through Targeting Infiltrating CD11b+ Cells in Mouse Skin. Photochem Photobiol 2008, 84, 266–271. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kang, K.S.; Yokozawa, T. The Anti-Melanogenic Effect of Pycnogenol by Its Anti-Oxidative Actions. Food Chem. Toxicol. 2008, 46, 2466–2471. [Google Scholar] [CrossRef]
- Verlaet, A.; van der Bolt, N.; Meijer, B.; Breynaert, A.; Naessens, T.; Konstanti, P.; Smidt, H.; Hermans, N.; Savelkoul, H.F.J.; Teodorowicz, M. Toll-Like Receptor-Dependent Immunomodulatory Activity of Pycnogenol®. Nutrients 2019, 11, 214. [Google Scholar] [CrossRef]
- Saliou, C.; Rimbach, G.; Moini, H.; McLaughlin, L.; Hosseini, S.; Lee, J.; Watson, R.R.; Packer, L. Solar Ultraviolet-Induced Erythema in Human Skin and Nuclear Factor-Kappa-B-Dependent Gene Expression in Keratinocytes Are Modulated by a French Maritime Pine Bark Extract. Free Radic. Biol. Med. 2001, 30, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Ambarwati, N.S.S.; Armandari, M.O.; Widayat, W.; Desmiaty, Y.; Elya, B.; Arifianti, A.E.; Ahmad, I. In Vitro Studies on the Cytotoxicity, Elastase, and Tyrosinase Inhibitory Activities of Tomato (Solanum lycopersicum Mill.) Extract. J. Adv. Pharm. Technol. Res. 2022, 13, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Khan, U.M.; Sevindik, M.; Zarrabi, A.; Nami, M.; Ozdemir, B.; Kaplan, D.N.; Selamoglu, Z.; Hasan, M.; Kumar, M.; Alshehri, M.M.; et al. Lycopene: Food Sources, Biological Activities, and Human Health Benefits. Oxidative Med. Cell. Longev. 2021, 2021, e2713511. [Google Scholar] [CrossRef] [PubMed]
- Gouranton, E.; Thabuis, C.; Riollet, C.; Malezet-Desmoulins, C.; El Yazidi, C.; Amiot, M.J.; Borel, P.; Landrier, J.F. Lycopene Inhibits Proinflammatory Cytokine and Chemokine Expression in Adipose Tissue. J. Nutr. Biochem. 2011, 22, 642–648. [Google Scholar] [CrossRef]
- Stahl, W.; Eichler, O.; Sies, H.; Heinrich, U.; Wiseman, S.; Tronnier, H. Dietary Tomato Paste Protects against Ultraviolet Light–Induced Erythema in Humans. J. Nutr. 2001, 131, 1449–1451. [Google Scholar] [CrossRef]
- Aust, O.; Stahl, W.; Sies, H.; Tronnier, H.; Heinrich, U. Supplementation with Tomato-Based Products Increases Lycopene, Phytofluene, and Phytoene Levels in Human Serum and Protects against UV-Light-Induced Erythema. Int. J. Vitam. Nutr. Res. 2005, 75, 54–60. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Speeckaert, R.; Bulat, V.; Speeckaert, M.M.; van Geel, N. The Impact of Antioxidants on Vitiligo and Melasma: A Scoping Review and Meta-Analysis. Antioxidants 2023, 12, 2082. https://doi.org/10.3390/antiox12122082
Speeckaert R, Bulat V, Speeckaert MM, van Geel N. The Impact of Antioxidants on Vitiligo and Melasma: A Scoping Review and Meta-Analysis. Antioxidants. 2023; 12(12):2082. https://doi.org/10.3390/antiox12122082
Chicago/Turabian StyleSpeeckaert, Reinhart, Vedrana Bulat, Marijn M. Speeckaert, and Nanja van Geel. 2023. "The Impact of Antioxidants on Vitiligo and Melasma: A Scoping Review and Meta-Analysis" Antioxidants 12, no. 12: 2082. https://doi.org/10.3390/antiox12122082
APA StyleSpeeckaert, R., Bulat, V., Speeckaert, M. M., & van Geel, N. (2023). The Impact of Antioxidants on Vitiligo and Melasma: A Scoping Review and Meta-Analysis. Antioxidants, 12(12), 2082. https://doi.org/10.3390/antiox12122082