

Obesity Affects Maternal and Neonatal HDL Metabolism and Function

 ,
,  ,
,  , ,
, , 
 , ,
, ,  ,
,  and
and
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Cohorts
2.2. Biochemical Analyses
2.3. ApoB-Depletion of Serum
2.4. Cholesterol Efflux Capacity
2.5. Lecithin–Cholesteryl Acyltransferase (LCAT) Activity
2.6. Arylesterase (AE)—Activity of Paraoxonase1 (PON1)
2.7. Antioxidative Capacity of Apob-Depleted Serum
2.8. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
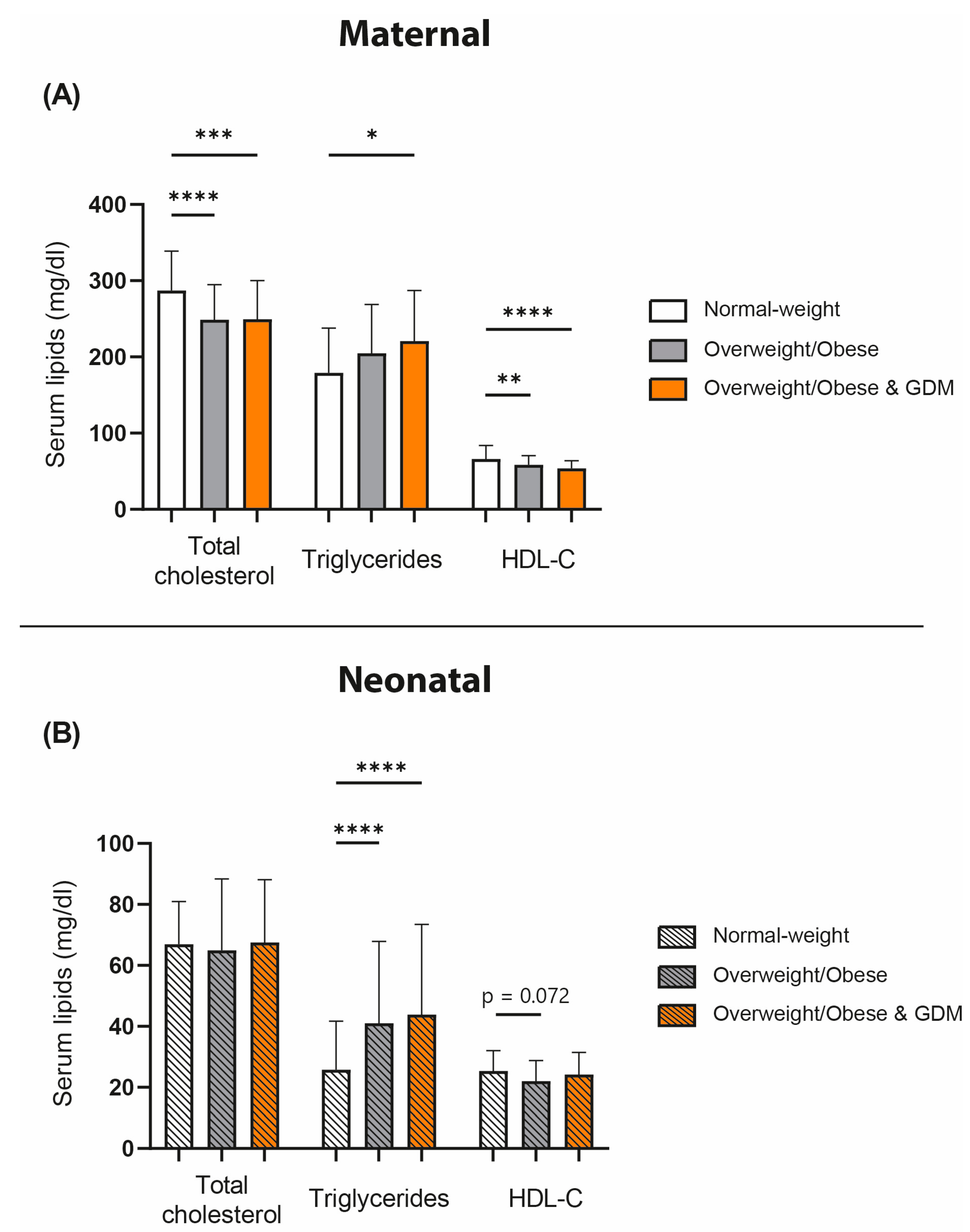
3.2. Serum Plasma Lipids of Normal-Weight, Overweight/Obese, and GDM Mothers and Their Neonates
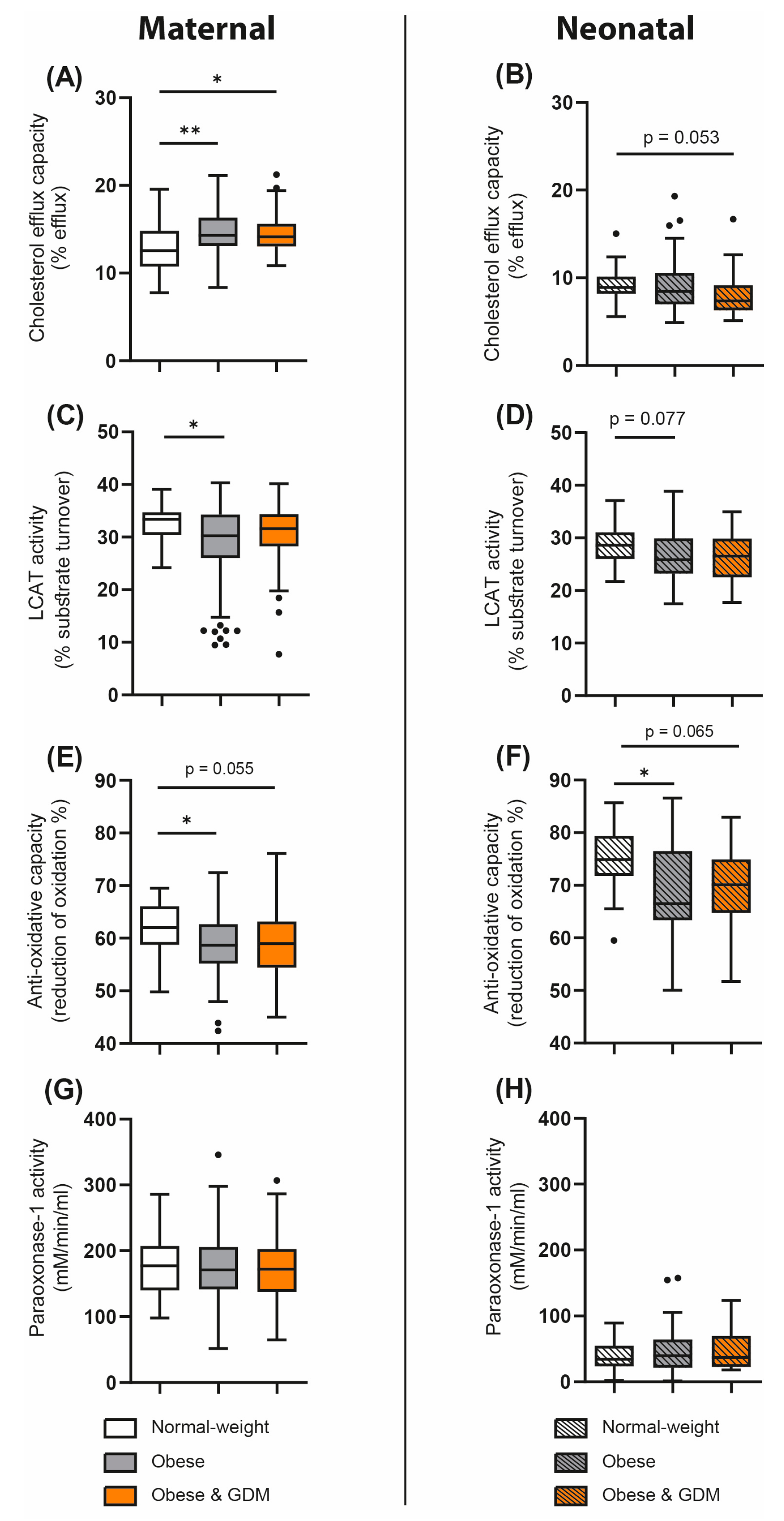
3.3. Obesity- and GDM-Associated Changes in Parameters of HDL Metabolism and Function
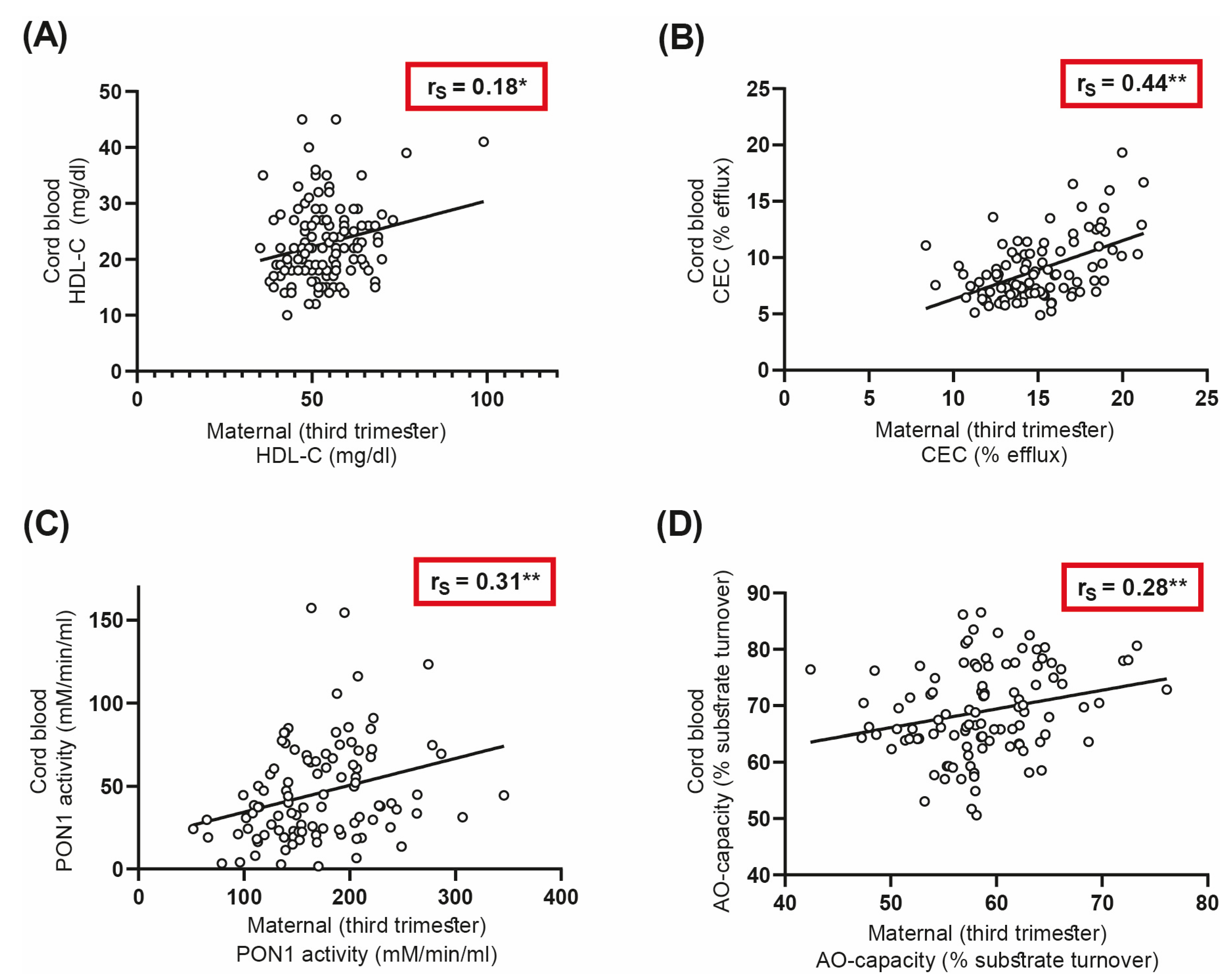
3.4. Correlations of Maternal and Neonatal HDL-Related Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vernini, J.M.; Moreli, J.B.; Magalhães, C.G.; Costa, R.A.A.; Rudge, M.V.C.; Calderon, I.M.P. Maternal and Fetal Outcomes in Pregnancies Complicated by Overweight and Obesity. Reprod. Health 2016, 13, 100. [Google Scholar] [CrossRef] [PubMed]
- Alfadhli, E.M. Maternal Obesity Influences Birth Weight More than Gestational Diabetes. BMC Pregnancy Childbirth 2021, 21, 111. [Google Scholar] [CrossRef] [PubMed]
- Leddy, M.A.; Power, M.L.; Schulkin, J. The Impact of Maternal Obesity on Maternal and Fetal Health. Rev. Obstet. Gynecol. 2008, 1, 170–178. [Google Scholar] [PubMed]
- Stadler, J.T.; van Poppel, M.N.M.; Christoffersen, C.; Hill, D.; Wadsack, C.; Simmons, D.; Desoye, G.; Marsche, G.; DALI Core Investigator Group. Gestational Hypertension and High-Density Lipoprotein Function: An Explorative Study in Overweight/Obese Women of the DALI Cohort. Antioxidants 2023, 12, 68. [Google Scholar] [CrossRef]
- Jenum, A.K.; Mørkrid, K.; Sletner, L.; Vange, S.; Torper, J.L.; Nakstad, B.; Voldner, N.; Rognerud-Jensen, O.H.; Berntsen, S.; Mosdøl, A.; et al. Impact of Ethnicity on Gestational Diabetes Identified with the WHO and the Modified International Association of Diabetes and Pregnancy Study Groups Criteria: A Population-Based Cohort Study. Eur. J. Endocrinol. 2012, 166, 317–324. [Google Scholar] [CrossRef]
- Ferrara, A. Increasing Prevalence of Gestational Diabetes Mellitus: A Public Health Perspective. Diabetes Care 2007, 30, S141–S146. [Google Scholar] [CrossRef]
- American Diabetes Association 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care 2017, 41, S13–S27. [Google Scholar] [CrossRef]
- Bellamy, L.; Casas, J.-P.; Hingorani, A.D.; Williams, D. Type 2 Diabetes Mellitus after Gestational Diabetes: A Systematic Review and Meta-Analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Vrachnis, N.; Augoulea, A.; Iliodromiti, Z.; Lambrinoudaki, I.; Sifakis, S.; Creatsas, G. Previous Gestational Diabetes Mellitus and Markers of Cardiovascular Risk. Int. J. Endocrinol. 2012, 2012, 458610. [Google Scholar] [CrossRef]
- Davis, C.L.; Gutt, M.; Llabre, M.M.; Marks, J.B.; O’Sullivan, M.J.; Potter, J.E.; Landel, J.L.; Kumar, M.; Schneiderman, N.; Gellman, M.; et al. History of Gestational Diabetes, Insulin Resistance and Coronary Risk. J. Diabetes Complicat. 1999, 13, 216–223. [Google Scholar] [CrossRef]
- Noctor, E.; Crowe, C.; Carmody, L.A.; Saunders, J.A.; Kirwan, B.; O’Dea, A.; Gillespie, P.; Glynn, L.G.; McGuire, B.E.; O’Neill, C.; et al. Abnormal Glucose Tolerance Post-Gestational Diabetes Mellitus as Defined by the International Association of Diabetes and Pregnancy Study Groups Criteria. Eur. J. Endocrinol. 2016, 175, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Shen, S.; Sun, L.; Yang, H.; Jin, B.; Cao, X. Metabolic Syndrome Risk after Gestational Diabetes: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e87863. [Google Scholar] [CrossRef] [PubMed]
- Kankowski, L.; Ardissino, M.; McCracken, C.; Lewandowski, A.J.; Leeson, P.; Neubauer, S.; Harvey, N.C.; Petersen, S.E.; Raisi-Estabragh, Z. The Impact of Maternal Obesity on Offspring Cardiovascular Health: A Systematic Literature Review. Front. Endocrinol. 2022, 13, 868441. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, R.M.; Allan, K.M.; Raja, E.A.; Bhattacharya, S.; McNeill, G.; Hannaford, P.C.; Sarwar, N.; Lee, A.J.; Bhattacharya, S.; Norman, J.E. Maternal Obesity during Pregnancy and Premature Mortality from Cardiovascular Event in Adult Offspring: Follow-up of 1,323,275 Person Years. BMJ 2013, 347, f4539. [Google Scholar] [CrossRef]
- Kannel, W.B.; Dawber, T.R.; Friedman, G.D.; Glennon, W.E.; Mcnamara, P.M. Risk factors in coronary heart disease. An evaluation of several serum lipids as predictors of coronary heart disease: The framingham study. Ann. Intern. Med. 1964, 61, 888–899. [Google Scholar] [CrossRef]
- Castelli, W.P.; Garrison, R.J.; Wilson, P.W.F.; Abbott, R.D.; Kalousdian, S.; Kannel, W.B. Incidence of Coronary Heart Disease and Lipoprotein Cholesterol Levels: The Framingham Study. JAMA 1986, 256, 2835–2838. [Google Scholar] [CrossRef]
- Litvinov, D.; Mahini, H.; Garelnabi, M. Antioxidant and Anti-Inflammatory Role of Paraoxonase 1: Implication in Arteriosclerosis Diseases. N. Am. J. Med. Sci. 2012, 4, 523–532. [Google Scholar] [CrossRef]
- Rohatgi, A.; Khera, A.; Berry, J.D.; Givens, E.G.; Ayers, C.R.; Wedin, K.E.; Neeland, I.J.; Yuhanna, I.S.; Rader, D.R.; de Lemos, J.A.; et al. HDL Cholesterol Efflux Capacity and Incident Cardiovascular Events. New Engl. J. Med. 2014, 371, 2383–2393. [Google Scholar] [CrossRef]
- Boyce, G.; Button, E.; Soo, S.; Wellington, C. The Pleiotropic Vasoprotective Functions of High Density Lipoproteins (HDL). J. Biomed. Res. 2017, 32, 164. [Google Scholar] [CrossRef]
- Jomard, A.; Osto, E. High Density Lipoproteins: Metabolism, Function, and Therapeutic Potential. Front. Cardiovasc. Med. 2020, 7, 39. [Google Scholar] [CrossRef]
- Stadler, J.T.; Marsche, G. Obesity-Related Changes in High-Density Lipoprotein Metabolism and Function. Int. J. Mol. Sci. 2020, 21, 8985. [Google Scholar] [CrossRef] [PubMed]
- Stadler, J.T.; Lackner, S.; Mörkl, S.; Trakaki, A.; Scharnagl, H.; Borenich, A.; Wonisch, W.; Mangge, H.; Zelzer, S.; Meier-Allard, N.; et al. Obesity Affects HDL Metabolism, Composition and Subclass Distribution. Biomedicines 2021, 9, 242. [Google Scholar] [CrossRef] [PubMed]
- Rashid, S.; Genest, J. Effect of Obesity on High-Density Lipoprotein Metabolism. Obesity 2007, 15, 2875–2888. [Google Scholar] [CrossRef] [PubMed]
- Carroll, P.D.; Christensen, R.D. New and Underutilized Uses of Umbilical Cord Blood in Neonatal Care. Matern. Health Neonatol. Perinatol. 2015, 1, 16. [Google Scholar] [CrossRef]
- Hansen, A.P.; Haischer-Rollo, G.D.; Shapiro, J.B.; Aden, J.K.; Abadie, J.M.; Mu, T.S. The Novel Use of Umbilical Cord Blood to Obtain Complete Blood Counts for Critical Neonatal Assessment. Cureus 2022, 14, e28009. [Google Scholar] [CrossRef] [PubMed]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva Ad Hod, M.; Kitzmiler, J.L.; et al. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef]
- Jelsma, J.G.M.; van Poppel, M.N.M.; Galjaard, S.; Desoye, G.; Corcoy, R.; Devlieger, R.; van Assche, A.; Timmerman, D.; Jans, G.; Harreiter, J.; et al. DALI: Vitamin D and Lifestyle Intervention for Gestational Diabetes Mellitus (GDM) Prevention: An European Multicentre, Randomised Trial—Study Protocol. BMC Pregnancy Childbirth 2013, 13, 1. [Google Scholar] [CrossRef]
- Simmons, D.; Jelsma, J.G.M.; Galjaard, S.; Devlieger, R.; Van Assche, A.; Jans, G.; Corcoy, R.; Adelantado, J.M.; Dunne, F.; Desoye, G.; et al. Results from a European Multicenter Randomized Trial of Physical Activity and/or Healthy Eating to Reduce the Risk of Gestational Diabetes Mellitus: The DALI Lifestyle Pilot. Diabetes Care 2015, 38, 1650–1656. [Google Scholar] [CrossRef] [PubMed]
- Trakaki, A.; Sturm, G.J.; Pregartner, G.; Scharnagl, H.; Eichmann, T.O.; Trieb, M.; Knuplez, E.; Holzer, M.; Stadler, J.T.; Heinemann, A.; et al. Allergic Rhinitis Is Associated with Complex Alterations in High-Density Lipoprotein Composition and Function. Biochim. Biophys Acta Mol. Cell Biol. Lipids 2019, 1864, 1280–1292. [Google Scholar] [CrossRef]
- Calabresi, L.; Franceschini, G. Lecithin:Cholesterol Acyltransferase, High-Density Lipoproteins, and Atheroprotection in Humans. Trends Cardiovasc. Med. 2010, 20, 50–53. [Google Scholar] [CrossRef]
- Glomset, J.A. The Plasma Lecithins:Cholesterol Acyltransferase Reaction. J. Lipid Res. 1968, 9, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Hewing, B.; Moore, K.J.; Fisher, E.A. HDL and Cardiovascular Risk. Circ. Res. 2012, 111, 1117–1120. [Google Scholar] [CrossRef] [PubMed]
- Pascot, A.; Lemieux, I.; Prud’homme, D.; Tremblay, A.; Nadeau, A.; Couillard, C.; Bergeron, J.; Lamarche, B.; Després, J.-P. Reduced HDL Particle Size as an Additional Feature of the Atherogenic Dyslipidemia of Abdominal Obesity. J. Lipid Res. 2001, 42, 2007–2014. [Google Scholar] [CrossRef]
- Williams, P.T.; Vranizan, K.M.; Austin, M.A.; Krauss, R.M. Associations of Age, Adiposity, Alcohol Intake, Menstrual Status, and Estrogen Therapy with High-Density Lipoprotein Subclasses. Arterioscler. Thromb. J. Vasc. Biol. 1993, 13, 1654–1661. [Google Scholar] [CrossRef] [PubMed]
- Scifres, C.M.; Catov, J.M.; Simhan, H.N. The Impact of Maternal Obesity and Gestational Weight Gain on Early and Mid-Pregnancy Lipid Profiles: Maternal Obesity, Weight Gain, and Serum Lipids. Obesity 2014, 22, 932–938. [Google Scholar] [CrossRef]
- Martin, C.L.; Vladutiu, C.J.; Zikry, T.M.; Grace, M.R.; Siega-Riz, A.M. Maternal Lipid Levels during Pregnancy and Child Weight Status at Three Years of Age. Pediatr. Obes. 2019, 14, e12485. [Google Scholar] [CrossRef]
- Mocarzel, C.C.; Velarde, G.C.; Antunes, R.d.A.; Sá, R.A.M.d.; Kurjak, A. Maternal Obesity Influences the Endocrine Cord Blood Profile of Their Offspring. J. Perinat. Med. 2020, 48, 242–248. [Google Scholar] [CrossRef]
- Sheikhahmadi, S.; Kazemian, M.; Afjeh, S. abolfazl Association of Umbilical Cord Lipid Profile with Gestational Age and Birth Weight in Newborns in Mahdieh Hospital in 2017. Sci. J. Kurd. Univ. Med. Sci. 2018, 23, 88–95. [Google Scholar] [CrossRef]
- Melchior, J.T.; Swertfeger, D.K.; Morris, J.; Street, S.E.; Warshak, C.R.; Welge, J.A.; Remaley, A.T.; Catov, J.M.; Davidson, W.S.; Woollett, L.A. Pregnancy Is Accompanied by Larger High Density Lipoprotein Particles and Compositionally Distinct Subspecies. J. Lipid Res. 2021, 62, 100107. [Google Scholar] [CrossRef]
- Talbot, C.P.J.; Plat, J.; Joris, P.J.; Konings, M.; Kusters, Y.H.A.M.; Schalkwijk, C.G.; Ritsch, A.; Mensink, R.P. HDL Cholesterol Efflux Capacity and Cholesteryl Ester Transfer Are Associated with Body Mass, but Are Not Changed by Diet-Induced Weight Loss: A Randomized Trial in Abdominally Obese Men. Atherosclerosis 2018, 274, 23–28. [Google Scholar] [CrossRef]
- Marsche, G.; Zelzer, S.; Meinitzer, A.; Kern, S.; Meissl, S.; Pregartner, G.; Weghuber, D.; Almer, G.; Mangge, H. Adiponectin Predicts High-Density Lipoprotein Cholesterol Efflux Capacity in Adults Irrespective of Body Mass Index and Fat Distribution. None 2017, 102, 4117–4123. [Google Scholar] [CrossRef]
- Du, X.-M.; Kim, M.-J.; Hou, L.; Le Goff, W.; Chapman, M.J.; Van Eck, M.; Curtiss, L.K.; Burnett, J.R.; Cartland, S.P.; Quinn, C.M.; et al. HDL Particle Size Is a Critical Determinant of ABCA1-Mediated Macrophage Cellular Cholesterol Export. Circ. Res. 2015, 116, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Sasahara, T.; Yamashita, T.; Sviridov, D.; Fidge, N.; Nestel, P. Altered Properties of High Density Lipoprotein Subfractions in Obese Subjects. J. Lipid Res. 1997, 38, 600–611. [Google Scholar] [CrossRef]
- Fournier, N.; Francone, O.; Rothblat, G.; Goudouneche, D.; Cambillau, M.; Kellner-Weibel, G.; Robinet, P.; Royer, L.; Moatti, N.; Simon, A.; et al. Enhanced Efflux of Cholesterol from ABCA1-Expressing Macrophages to Serum from Type IV Hypertriglyceridemic Subjects. Atherosclerosis 2003, 171, 287–293. [Google Scholar] [CrossRef]
- Attia, N.; Ramaharo, A.; Paul, J.-L.; Cambillau, M.; Beaune, P.; Grynberg, A.; Simon, A.; Fournier, N. Enhanced Removal of Cholesterol from Macrophage Foam Cells to Serum from Type IV Hypertriglyceridemic Subjects. Atherosclerosis 2008, 198, 49–56. [Google Scholar] [CrossRef]
- Weibel, G.L.; Drazul-Schrader, D.; Shivers, D.K.; Wade, A.N.; Rothblat, G.H.; Reilly, M.P.; de la Llera-Moya, M. Importance of Evaluating Cell Cholesterol Influx With Efflux in Determining the Impact of Human Serum on Cholesterol Metabolism and Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 17–25. [Google Scholar] [CrossRef]
- Koekemoer, A.L.; Codd, V.; Masca, N.G.D.; Nelson, C.P.; Musameh, M.D.; Kaess, B.M.; Hengstenberg, C.; Rader, D.J.; Samani, N.J. Large-Scale Analysis of Determinants, Stability, and Heritability of High-Density Lipoprotein Cholesterol Efflux Capacity. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1956–1962. [Google Scholar] [CrossRef]
- Dobiásová, M.; Frohlich, J. Understanding the Mechanism of LCAT Reaction May Help to Explain the High Predictive Value of LDL/HDL Cholesterol Ratio. Physiol. Res. 1998, 47, 387–397. [Google Scholar] [PubMed]
- Gillett, M.P.; Silva, T.B. Relationship between Plasma Lecithin:Cholesterol Acyltransferase Activity and Plasma Triglyceride Concentration in Non-Pregnant and Pregnant Brazilian Women. Scand. J. Clin. Lab. Invest. Suppl. 1978, 150, 118–123. [Google Scholar] [CrossRef]
- Zeng, Z.; Liu, F.; Li, S. Metabolic Adaptations in Pregnancy: A Review. ANM 2017, 70, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Wonisch, W.; Falk, A.; Sundl, I.; Winklhofer-Roob, B.M.; Lindschinger, M. Oxidative Stress Increases Continuously with BMI and Age with Unfavourable Profiles in Males. Aging Male 2012, 15, 159–165. [Google Scholar] [CrossRef]
- Ferretti, G.; Bacchetti, T.; Moroni, C.; Savino, S.; Liuzzi, A.; Balzola, F.; Bicchiega, V. Paraoxonase Activity in High-Density Lipoproteins: A Comparison between Healthy and Obese Females. J. Clin. Endocrinol. Metab. 2005, 90, 1728–1733. [Google Scholar] [CrossRef]
- Schulpis, K.H.; Barzeliotou, A.; Papadakis, M.; Rodolakis, A.; Antsaklis, A.; Papassotiriou, I.; Vlachos, G.D. Maternal Chronic Hepatitis B Virus Is Implicated with Low Neonatal Paraoxonase/Arylesterase Activities. Clin. Biochem. 2008, 41, 282–287. [Google Scholar] [CrossRef]
- Gugliucci, A.; Numaguchi, M.; Caccavello, R.; Kimura, S. Paraoxonase 1 Lactonase Activity and Distribution in the HDL Subclasses in the Cord Blood. Redox Rep. 2014, 19, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Sreckovic, I.; Birner-Gruenberger, R.; Obrist, B.; Stojakovic, T.; Scharnagl, H.; Holzer, M.; Scholler, M.; Philipose, S.; Marsche, G.; Lang, U.; et al. Distinct Composition of Human Fetal HDL Attenuates Its Anti-Oxidative Capacity. Biochim. Et Biophys. Acta (BBA)—Mol. Cell Biol. Lipids 2013, 1831, 737–746. [Google Scholar] [CrossRef]
- Herrera, E.; Desoye, G. Maternal and Fetal Lipid Metabolism under Normal and Gestational Diabetic Conditions. Horm. Mol. Biol. Clin. Investig. 2016, 26, 109–127. [Google Scholar] [CrossRef]
- Stadler, J.T.; Wadsack, C.; Marsche, G. Fetal High-Density Lipoproteins: Current Knowledge on Particle Metabolism, Composition and Function in Health and Disease. Biomedicines 2021, 9, 349. [Google Scholar] [CrossRef]
- Larqué, E.; Ruiz-Palacios, M.; Koletzko, B. Placental Regulation of Fetal Nutrient Supply. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Woollett, L.A. Review: Transport of Maternal Cholesterol to the Fetal Circulation. Placenta 2011, 32, S218–S221. [Google Scholar] [CrossRef] [PubMed]
- Challier, J.C.; Basu, S.; Bintein, T.; Minium, J.; Hotmire, K.; Catalano, P.M.; Hauguel-de Mouzon, S. Obesity in Pregnancy Stimulates Macrophage Accumulation and Inflammation in the Placenta. Placenta 2008, 29, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Dron, J.S.; Hegele, R.A. Genetics of Lipid and Lipoprotein Disorders and Traits. Curr. Genet. Med. Rep. 2016, 4, 130–141. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal Characteristics | Normal Weight N = 34 | Overweight/Obese N = 132 | P Normal Weight vs. Overweight/Obese | GDM N = 54 | P Overweight/Obese vs. GDM |
|---|---|---|---|---|---|
| Maternal age, year | 29.9 ± 5.1 | 31.9 ± 5.2 | 0.13 | 31.1 ± 5.8 | 0.66 |
| BMI, kg/m2 | 21.5 ± 1.7 | 34.2 ± 4.6 | <0.001 | 34.1 ± 4.4 | 0.99 |
| Systolic blood pressure, mm Hg | 117 ± 11 | 120 ± 10 | 0.491 | 118 ± 10 | 0.472 |
| Diastolic blood pressure, mm Hg | 74 ± 9 | 78 ± 9 | 0.45 | 75 ± 7 | 0.104 |
| HOMA-IR | - | 3.3 (2.4–4.4) | - | 5.1 (3.0–6.6) | <0.001 |
| Neonatal characteristics | |||||
| Birth weight, g | 3177 ± 498 | 3495 ± 518 | 0.03 | 3768 ± 483 | 0.003 |
| Gestational age at birth, week | 38.6 ± 1.7 | 39.6 ± 1.4 | <0.001 | 39.8 ± 1.2 | 0.71 |
| Placenta weight, g | 591 ± 95 | 633 ± 138 | 0.24 | 686 ± 133 | 0.06 |
| Female sex, | 19 (56%) | 61 (46%) | 0.31 | 28 (51%) | 0.64 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stadler, J.T.; van Poppel, M.N.M.; Wadsack, C.; Holzer, M.; Pammer, A.; Simmons, D.; Hill, D.; Desoye, G.; Marsche, G.; DALI Core Investigator Group. Obesity Affects Maternal and Neonatal HDL Metabolism and Function. Antioxidants 2023, 12, 199. https://doi.org/10.3390/antiox12010199
Stadler JT, van Poppel MNM, Wadsack C, Holzer M, Pammer A, Simmons D, Hill D, Desoye G, Marsche G, DALI Core Investigator Group. Obesity Affects Maternal and Neonatal HDL Metabolism and Function. Antioxidants. 2023; 12(1):199. https://doi.org/10.3390/antiox12010199
Chicago/Turabian StyleStadler, Julia T., Mireille N. M. van Poppel, Christian Wadsack, Michael Holzer, Anja Pammer, David Simmons, David Hill, Gernot Desoye, Gunther Marsche, and DALI Core Investigator Group. 2023. "Obesity Affects Maternal and Neonatal HDL Metabolism and Function" Antioxidants 12, no. 1: 199. https://doi.org/10.3390/antiox12010199
APA StyleStadler, J. T., van Poppel, M. N. M., Wadsack, C., Holzer, M., Pammer, A., Simmons, D., Hill, D., Desoye, G., Marsche, G., & DALI Core Investigator Group. (2023). Obesity Affects Maternal and Neonatal HDL Metabolism and Function. Antioxidants, 12(1), 199. https://doi.org/10.3390/antiox12010199