
Pharmacotherapies and Aortic Heme Oxygenase-1 Expression in Patients with Abdominal Aortic Aneurysm

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Primary Outcome Variable
2.2. Abdominal Aortic Wall Acquisition and Patient Data
2.3. Pharmacological Therapies
2.4. RNA Isolation, cDNA Synthesis, and Quantitative Real-Time PCR (qPCR)
2.5. Protein Isolation and Western Blot
2.6. Statistical Analyses
3. Results
3.1. Demographic Characteristics of Analyzed AAA Patients
3.2. Effects of AAA Risk Factors on Aortic HO-1 mRNA and Protein Expressions
3.3. Hierarchy of Treatments Affecting HO-1 Expression
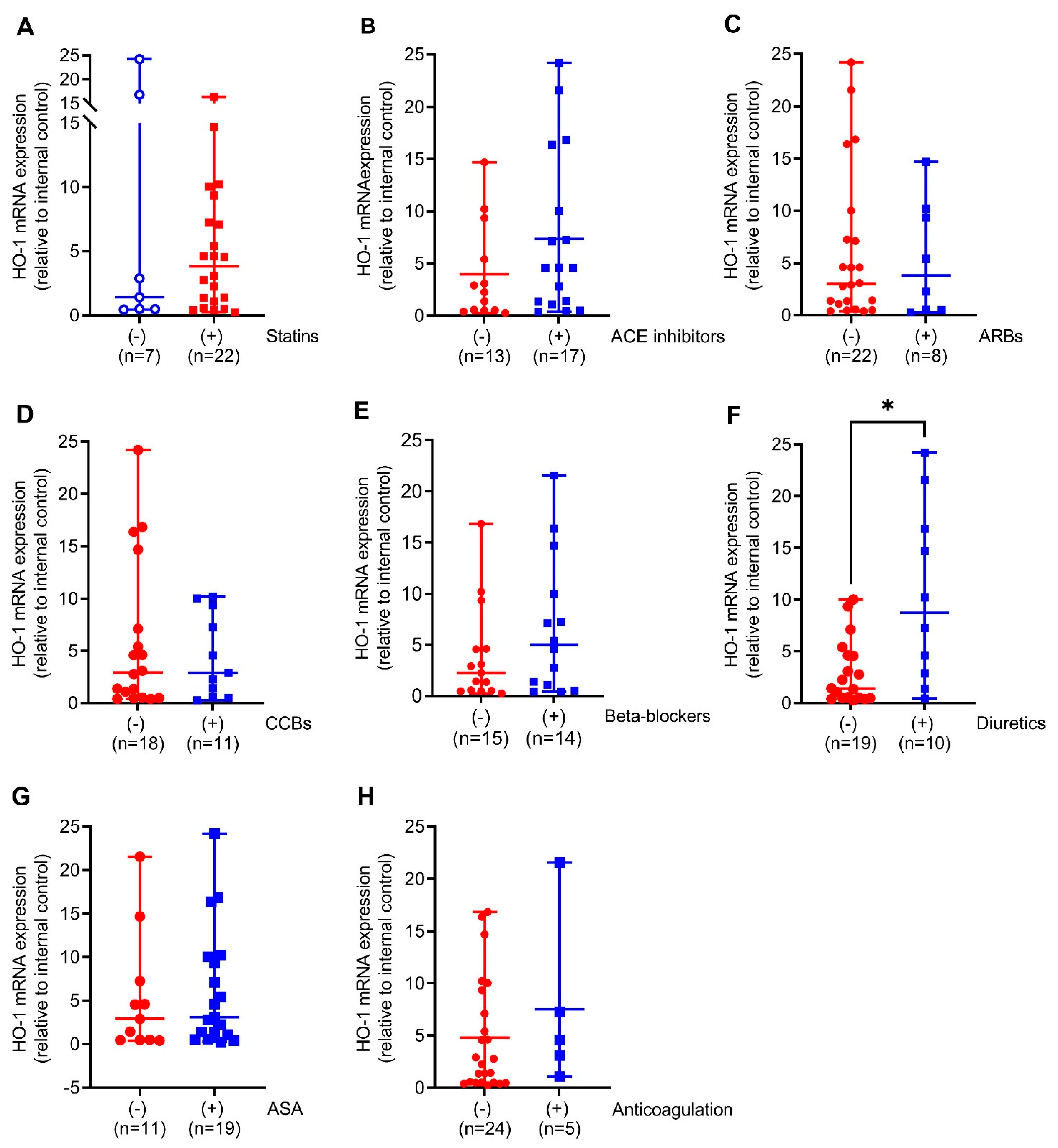
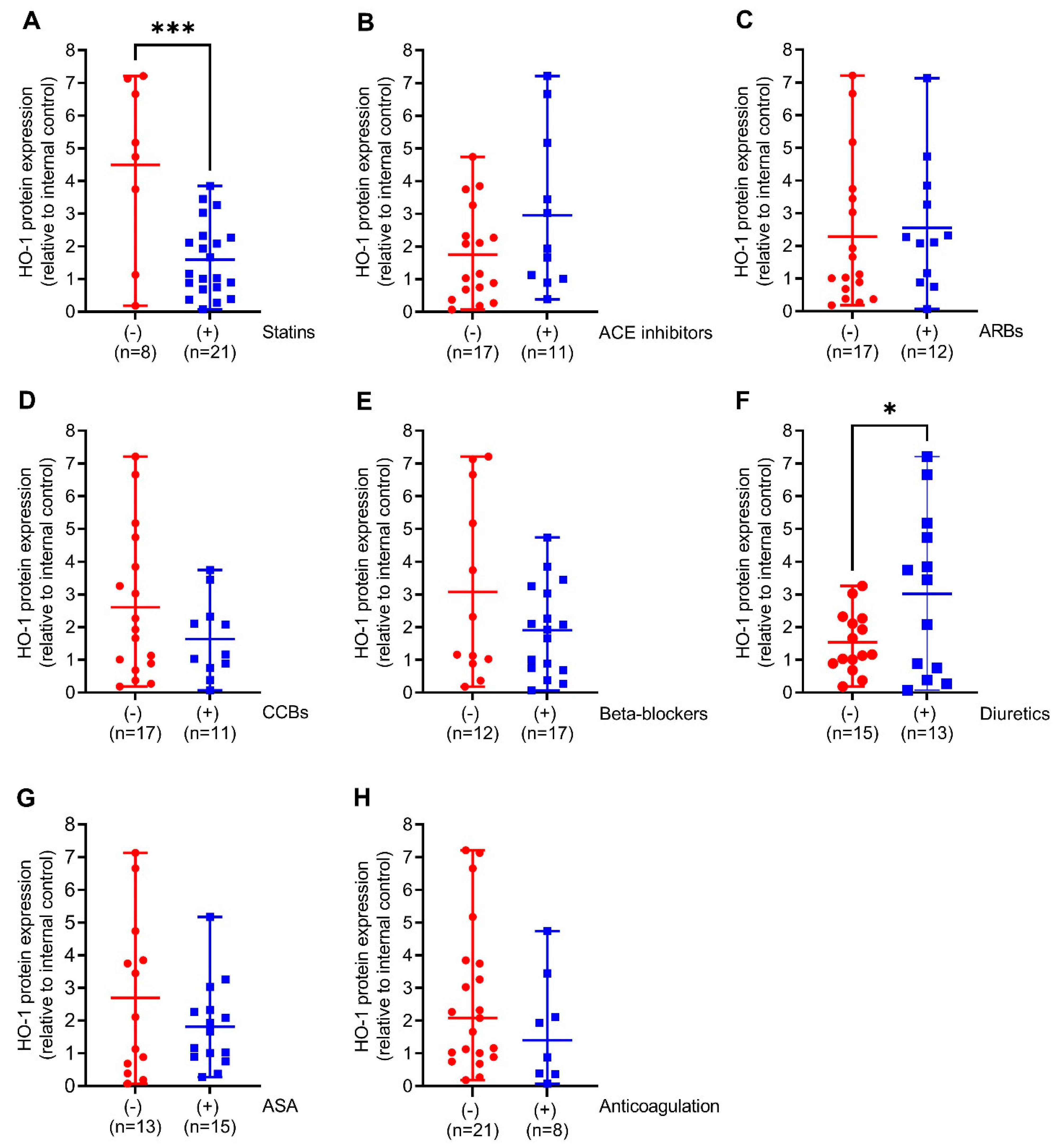
3.4. Regulation of HO-1 mRNA and Protein Expressions in Response to Cardiometabolic Standard Therapies
3.5. Regulation of Aortic HO-1 Expression towards Combinations of Antihypertensive Treatments
3.6. Linkage of HO-1 Expression with AAA Diameter and Thickness of the Intraluminal Thrombus
4. Discussion
5. Limitations of the Present Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steinmetz, E.F.; Buckley, C.; Shames, M.L.; Ennis, T.L.; Vanvickle-Chavez, S.J.; Mao, D.; Goeddel, L.A.; Hawkins, C.J.; Thompson, R.W. Treatment with simvastatin suppresses the development of experimental abdominal aortic aneurysms in normal and hypercholesterolemic mice. Ann. Surg. 2005, 241, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Koole, D.; Zandvoort, H.J.; Schoneveld, A.; Vink, A.; Vos, J.A.; van den Hoogen, L.L.; de Vries, J.P.; Pasterkamp, G.; Moll, F.L.; van Herwaarden, J.A. Intraluminal abdominal aortic aneurysm thrombus is associated with disruption of wall integrity. J. Vasc. Surg. 2013, 57, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.M.; Rateri, D.L.; Daugherty, A. Abdominal aortic aneurysm: Novel mechanisms and therapies. Curr. Opin. Cardiol. 2015, 30, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Lindeman, J.H.; Matsumura, J.S. Pharmacologic Management of Aneurysms. Circ. Res. 2019, 124, 631–646. [Google Scholar] [CrossRef]
- Miyake, T.; Morishita, R. Pharmacological treatment of abdominal aortic aneurysm. Cardiovasc. Res. 2009, 83, 436–443. [Google Scholar] [CrossRef]
- Idriss, N.K.; Blann, A.D.; Lip, G.Y. Hemoxygenase-1 in cardiovascular disease. J. Am. Coll. Cardiol. 2008, 52, 971–978. [Google Scholar] [CrossRef]
- Fredenburgh, L.E.; Merz, A.A.; Cheng, S. Haeme oxygenase signalling pathway: Implications for cardiovascular disease. Eur. Heart J. 2015, 36, 1512–1518. [Google Scholar] [CrossRef]
- Giebe, S.; Cockcroft, N.; Hewitt, K.; Brux, M.; Hofmann, A.; Morawietz, H.; Brunssen, C. Cigarette smoke extract counteracts atheroprotective effects of high laminar flow on endothelial function. Redox Biol. 2017, 12, 776–786. [Google Scholar] [CrossRef]
- Immenschuh, S.; Ramadori, G. Gene regulation of heme oxygenase-1 as a therapeutic target. Biochem. Pharm. 2000, 60, 1121–1128. [Google Scholar] [CrossRef]
- Wu, M.L.; Ho, Y.C.; Yet, S.F. A central role of heme oxygenase-1 in cardiovascular protection. Antioxid. Redox Signal. 2011, 15, 1835–1846. [Google Scholar] [CrossRef]
- Ho, Y.C.; Wu, M.L.; Gung, P.Y.; Chen, C.H.; Kuo, C.C.; Yet, S.F. Heme oxygenase-1 deficiency exacerbates angiotensin II-induced aortic aneurysm in mice. Oncotarget 2016, 7, 67760–67776. [Google Scholar] [CrossRef] [PubMed]
- Azuma, J.; Wong, R.J.; Morisawa, T.; Hsu, M.; Maegdefessel, L.; Zhao, H.; Kalish, F.; Kayama, Y.; Wallenstein, M.B.; Deng, A.C.; et al. Heme Oxygenase-1 Expression Affects Murine Abdominal Aortic Aneurysm Progression. PLoS ONE 2016, 11, e0149288. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, A.; Muglich, M.; Wolk, S.; Khorzom, Y.; Sabarstinski, P.; Kopaliani, I.; Egorov, D.; Horn, F.; Brunssen, C.; Giebe, S.; et al. Induction of Heme Oxygenase-1 Is Linked to the Severity of Disease in Human Abdominal Aortic Aneurysm. J. Am. Heart Assoc. 2021, 10, e022747. [Google Scholar] [CrossRef] [PubMed]
- Piechota-Polanczyk, A.; Jozkowicz, A.; Nowak, W.; Eilenberg, W.; Neumayer, C.; Malinski, T.; Huk, I.; Brostjan, C. The Abdominal Aortic Aneurysm and Intraluminal Thrombus: Current Concepts of Development and Treatment. Front. Cardiovasc. Med. 2015, 2, 19. [Google Scholar] [CrossRef]
- Vandesompele, J.; De Preter, K.; Pattyn, F.; Poppe, B.; Van Roy, N.; De Paepe, A.; Speleman, F. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 3, RESEARCH0034. [Google Scholar] [CrossRef]
- Lin, Q.; Weis, S.; Yang, G.; Weng, Y.-H.; Helston, R.; Rish, K.; Smith, A.; Bordner, J.; Polte, T.; Gaunitz, F.; et al. Heme Oxygenase-1 Protein Localizes to the Nucleus and Activates Transcription Factors Important in Oxidative Stress. J. Biol. Chem. 2007, 282, 20621–20633. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Hinkelmann, U.; Grosser, N.; Erdmann, K.; Schröder, H.; Immenschuh, S. Simvastatin-dependent up-regulation of heme oxygenase-1 via mRNA stabilization in human endothelial cells. Eur. J. Pharm. Sci. 2010, 41, 118–124. [Google Scholar] [CrossRef]
- Zhang, A.; Suzuki, T.; Adachi, S.; Naganuma, E.; Suzuki, N.; Hosoya, T.; Itoh, K.; Sporn, M.B.; Yamamoto, M. Distinct Regulations of HO-1 Gene Expression for Stress Response and Substrate Induction. Mol. Cell. Biol. 2021, 41, e0023621. [Google Scholar] [CrossRef]
- Schillinger, M.; Exner, M.; Mlekusch, W.; Domanovits, H.; Huber, K.; Mannhalter, C.; Wagner, O.; Minar, E. Heme oxygenase-1 gene promoter polymorphism is associated with abdominal aortic aneurysm. Thromb. Res. 2002, 106, 131–136. [Google Scholar] [CrossRef]
- Dennery, P.A. Signaling function of heme oxygenase proteins. Antioxid. Redox Signal. 2014, 20, 1743–1753. [Google Scholar] [CrossRef] [PubMed]
- Duarte, J.D.; Cooper-DeHoff, R.M. Mechanisms for blood pressure lowering and metabolic effects of thiazide and thiazide-like diuretics. Expert Rev. Cardiovasc. Ther. 2010, 8, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Pickkers, P.; Hughes, A.D.; Russel, F.G.M.; Thien, T.; Smits, P. Thiazide-Induced Vasodilation in Humans Is Mediated by Potassium Channel Activation. Hypertension 1998, 32, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, Y.; Man, R.Y.; Vanhoutte, P.M. Upregulation of heme oxygenase-1 potentiates EDH-type relaxations in the mesenteric artery of the spontaneously hypertensive rat. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H1471–H1483. [Google Scholar] [CrossRef] [PubMed]
- Zager, R.A.; Johnson, A.C.M.; Becker, K. Plasma and Urinary Heme Oxygenase-1 in AKI. J. Am. Soc. Nephrol. 2012, 23, 1048–1057. [Google Scholar] [CrossRef] [PubMed]
- Botros, F.T.; Schwartzman, M.L.; Stier, C.T., Jr.; Goodman, A.I.; Abraham, N.G. Increase in heme oxygenase-1 levels ameliorates renovascular hypertension. Kidney Int. 2005, 68, 2745–2755. [Google Scholar] [CrossRef]
- Tian, S.; Ge, X.; Wu, K.; Yang, H.; Liu, Y. Ramipril Protects the Endothelium from High Glucose–Induced Dysfunction through CaMKKβ/AMPK and Heme Oxygenase-1 Activation. J. Pharm. Exp. Ther. 2014, 350, 5–13. [Google Scholar] [CrossRef]
- Ishizaka, N.; Griendling, K.K. Heme oxygenase-1 is regulated by angiotensin II in rat vascular smooth muscle cells. Hypertension 1997, 29, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Morawietz, H.; Erbs, S.; Holtz, J.; Schubert, A.; Krekler, M.; Goettsch, W.; Kuss, O.; Adams, V.; Lenk, K.; Mohr, F.W.; et al. Endothelial Protection, AT1 blockade and Cholesterol-Dependent Oxidative Stress: The EPAS trial. Circulation 2006, 114, I296–I301. [Google Scholar] [CrossRef]
- Morawietz, H.; Rueckschloss, U.; Niemann, B.; Duerrschmidt, N.; Galle, J.; Hakim, K.; Zerkowski, H.R.; Sawamura, T.; Holtz, J. Angiotensin II induces LOX-1, the human endothelial receptor for oxidized low-density lipoprotein. Circulation 1999, 100, 899–902. [Google Scholar] [CrossRef] [Green Version]
- Golledge, J.; Pinchbeck, J.; Tomee, S.M.; Rowbotham, S.E.; Singh, T.P.; Moxon, J.V.; Jenkins, J.S.; Lindeman, J.H.; Dalman, R.L.; McDonnell, L.; et al. Efficacy of Telmisartan to Slow Growth of Small Abdominal Aortic Aneurysms: A Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-S.; Chang, C.-C.; Zhu, Y.; Shyy, J.Y.-J. Simvastatin Induces Heme Oxygenase-1. Circulation 2004, 110, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Sigala, F.; Efentakis, P.; Karageorgiadi, D.; Filis, K.; Zampas, P.; Iliodromitis, E.K.; Zografos, G.; Papapetropoulos, A.; Andreadou, I. Reciprocal regulation of eNOS, H2S and CO-synthesizing enzymes in human atheroma: Correlation with plaque stability and effects of simvastatin. Redox Biol. 2017, 12, 70–81. [Google Scholar] [CrossRef]
- Piechota-Polanczyk, A.; Kopacz, A.; Kloska, D.; Zagrapan, B.; Neumayer, C.; Grochot-Przeczek, A.; Huk, I.; Brostjan, C.; Dulak, J.; Jozkowicz, A. Simvastatin Treatment Upregulates HO-1 in Patients with Abdominal Aortic Aneurysm but Independently of Nrf2. Oxid. Med. Cell. Longev. 2018, 2018, 2028936. [Google Scholar] [CrossRef] [PubMed]
- True, A.L.; Olive, M.; Boehm, M.; San, H.; Westrick, R.J.; Raghavachari, N.; Xu, X.; Lynn, E.G.; Sack, M.N.; Munson, P.J.; et al. Heme oxygenase-1 deficiency accelerates formation of arterial thrombosis through oxidative damage to the endothelium, which is rescued by inhaled carbon monoxide. Circ. Res. 2007, 101, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Durante, W. Targeting Heme Oxygenase-1 in the Arterial Response to Injury and Disease. Antioxidants 2020, 9, 829. [Google Scholar] [CrossRef]
- Lindenblatt, N.; Bordel, R.; Schareck, W.; Menger, M.D.; Vollmar, B. Vascular heme oxygenase-1 induction suppresses microvascular thrombus formation in vivo. Arter. Thromb. Vasc. Biol. 2004, 24, 601–606. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| log HO-1 mRNA | ||||
|---|---|---|---|---|
| Treatment combination | Estimate | CI left | CI right | p-value |
| ARBs [0] | 1.024 | 0.410 | 2.559 | 0.960 |
| Diuretics [0] | 3.144 | 1.315 | 7.512 | 0.014 |
| ACE [0] | 1.192 | 0.536 | 2.651 | 0.670 |
| Diuretics [0] | 3.060 | 1.290 | 7.259 | 0.015 |
| ARBs [0] | 0.861 | 0.312 | 2.373 | 0.773 |
| CCBs [0] | 0.919 | 0.357 | 2.367 | 0.862 |
| CCBs [0] | 0.923 | 0.369 | 2.306 | 0.865 |
| ACE [0] | 1.339 | 0.564 | 3.178 | 0.511 |
| Beta-blockers [0] | 1.486 | 0.663 | 3.330 | 0.342 |
| Diuretics [0] | 2.844 | 1.189 | 6.800 | 0.024 |
| CCBs [0] | 1.862 | 0.785 | 4.420 | 0.166 |
| Beta-blockers [0] | 1.034 | 0.414 | 2.584 | 0.943 |
| ACE [0] | 1.183 | 0.523 | 2.678 | 0.689 |
| CCBs [0] | 0.944 | 0.399 | 2.229 | 0.896 |
| Diuretics [0] | 3.056 | 1.274 | 7.333 | 0.017 |
| log HO-1 Protein | ||||
|---|---|---|---|---|
| Treatment combination | Estimate | CI left | CI right | p-value |
| ARBs [0] | 1.695 | 0.617 | 4.657 | 0.314 |
| Diuretics [0] | 2.068 | 0.768 | 5.573 | 0.161 |
| ACE [0] | 1.617 | 0.608 | 4.300 | 0.344 |
| Diuretics [0] | 1.778 | 0.659 | 4.797 | 0.265 |
| CCBs [0] | 1.314 | 0.469 | 3.682 | 0.607 |
| ACE [0] | 1.879 | 0.680 | 5.187 | 0.233 |
| ARBs [0] | 1.545 | 0.503 | 4.747 | 0.454 |
| CCBs [0] | 0.950 | 0.316 | 2.858 | 0.928 |
| Beta-blockers [0] | 0.948 | 0.352 | 2.549 | 0.916 |
| Diuretics [0] | 1.933 | 0.697 | 5.359 | 0.215 |
| Beta-blockers [0] | 1.090 | 0.404 | 2.945 | 0.866 |
| CCBs [0] | 1.127 | 0.405 | 3.140 | 0.820 |
| ACE [0] | 1.708 | 0.611 | 4.775 | 0.316 |
| CCBs [0] | 1.237 | 0.440 | 3.477 | 0.690 |
| Diuretics [0] | 1.738 | 0.631 | 4.788 | 0.294 |
| log HO-1 mRNA | ||||
|---|---|---|---|---|
| Parameter | Estimate | CI left | CI right | p-value |
| Aortic diameter, mm | 1.015 | 0.976 | 1.054 | 0.467 |
| Thickness ILT, mm | 0.983 | 0.936 | 1.032 | 0.488 |
| log HO-1 protein | ||||
| Parameter | Estimate | CI left | CI right | p-value |
| Aortic diameter, mm | 0.981 | 0.943 | 1.020 | 0.333 |
| Thickness ILT, mm | 1.010 | 0.962 | 1.061 | 0.680 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmann, A.; Hamann, B.; Klimova, A.; Müglich, M.; Wolk, S.; Busch, A.; Frank, F.; Sabarstinski, P.; Kapalla, M.; Nees, J.A.; et al. Pharmacotherapies and Aortic Heme Oxygenase-1 Expression in Patients with Abdominal Aortic Aneurysm. Antioxidants 2022, 11, 1753. https://doi.org/10.3390/antiox11091753
Hofmann A, Hamann B, Klimova A, Müglich M, Wolk S, Busch A, Frank F, Sabarstinski P, Kapalla M, Nees JA, et al. Pharmacotherapies and Aortic Heme Oxygenase-1 Expression in Patients with Abdominal Aortic Aneurysm. Antioxidants. 2022; 11(9):1753. https://doi.org/10.3390/antiox11091753
Chicago/Turabian StyleHofmann, Anja, Bianca Hamann, Anna Klimova, Margarete Müglich, Steffen Wolk, Albert Busch, Frieda Frank, Pamela Sabarstinski, Marvin Kapalla, Josef Albin Nees, and et al. 2022. "Pharmacotherapies and Aortic Heme Oxygenase-1 Expression in Patients with Abdominal Aortic Aneurysm" Antioxidants 11, no. 9: 1753. https://doi.org/10.3390/antiox11091753
APA StyleHofmann, A., Hamann, B., Klimova, A., Müglich, M., Wolk, S., Busch, A., Frank, F., Sabarstinski, P., Kapalla, M., Nees, J. A., Brunssen, C., Poitz, D. M., Morawietz, H., & Reeps, C. (2022). Pharmacotherapies and Aortic Heme Oxygenase-1 Expression in Patients with Abdominal Aortic Aneurysm. Antioxidants, 11(9), 1753. https://doi.org/10.3390/antiox11091753