
The Effect of Herbal Supplements on Blood Pressure: Systematic Review and Meta-Analysis



Abstract
:1. Introduction
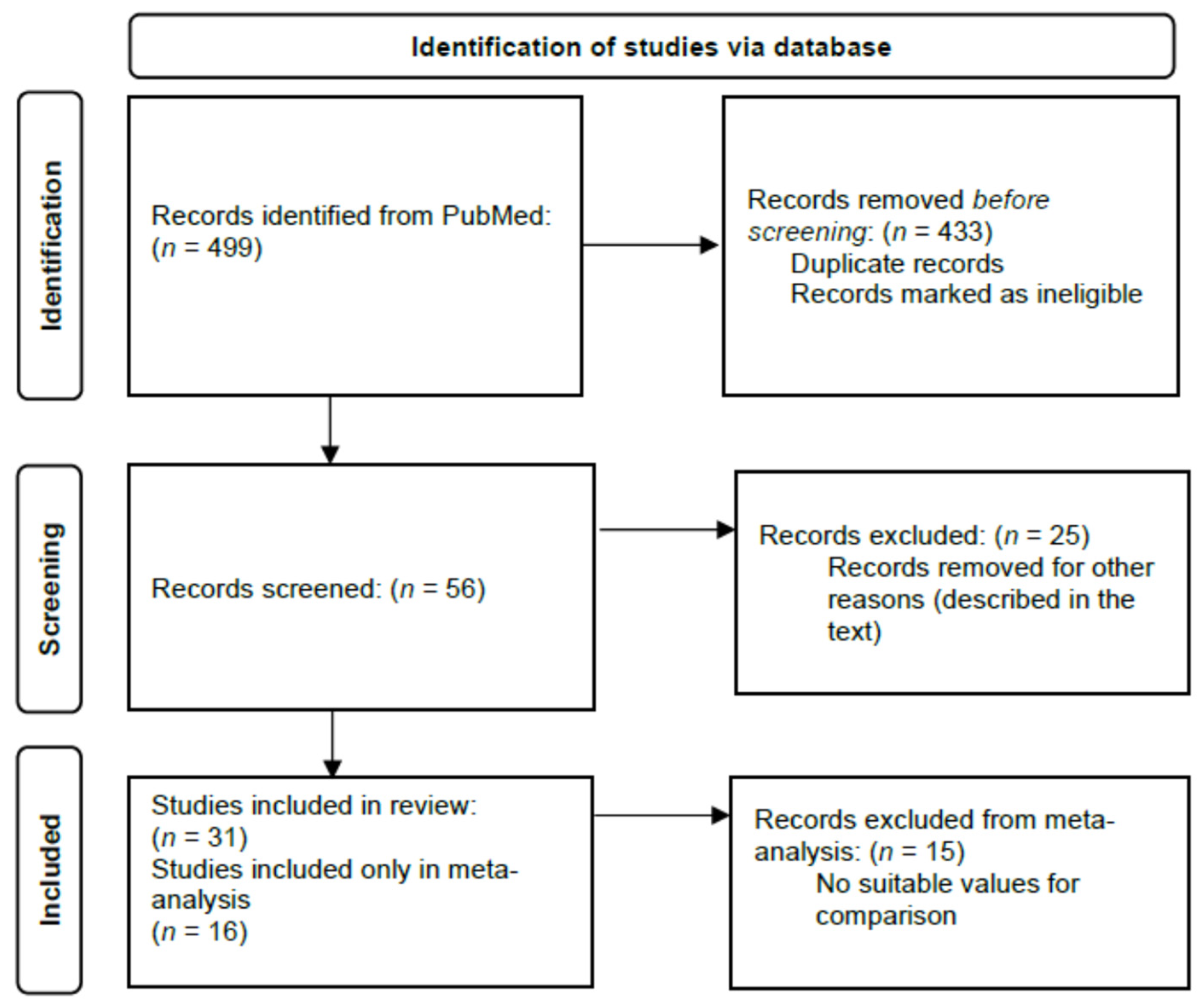
2. Materials and Methods
2.1. Data Source and Searching Strategy
2.2. Statistical Analysis
3. Results
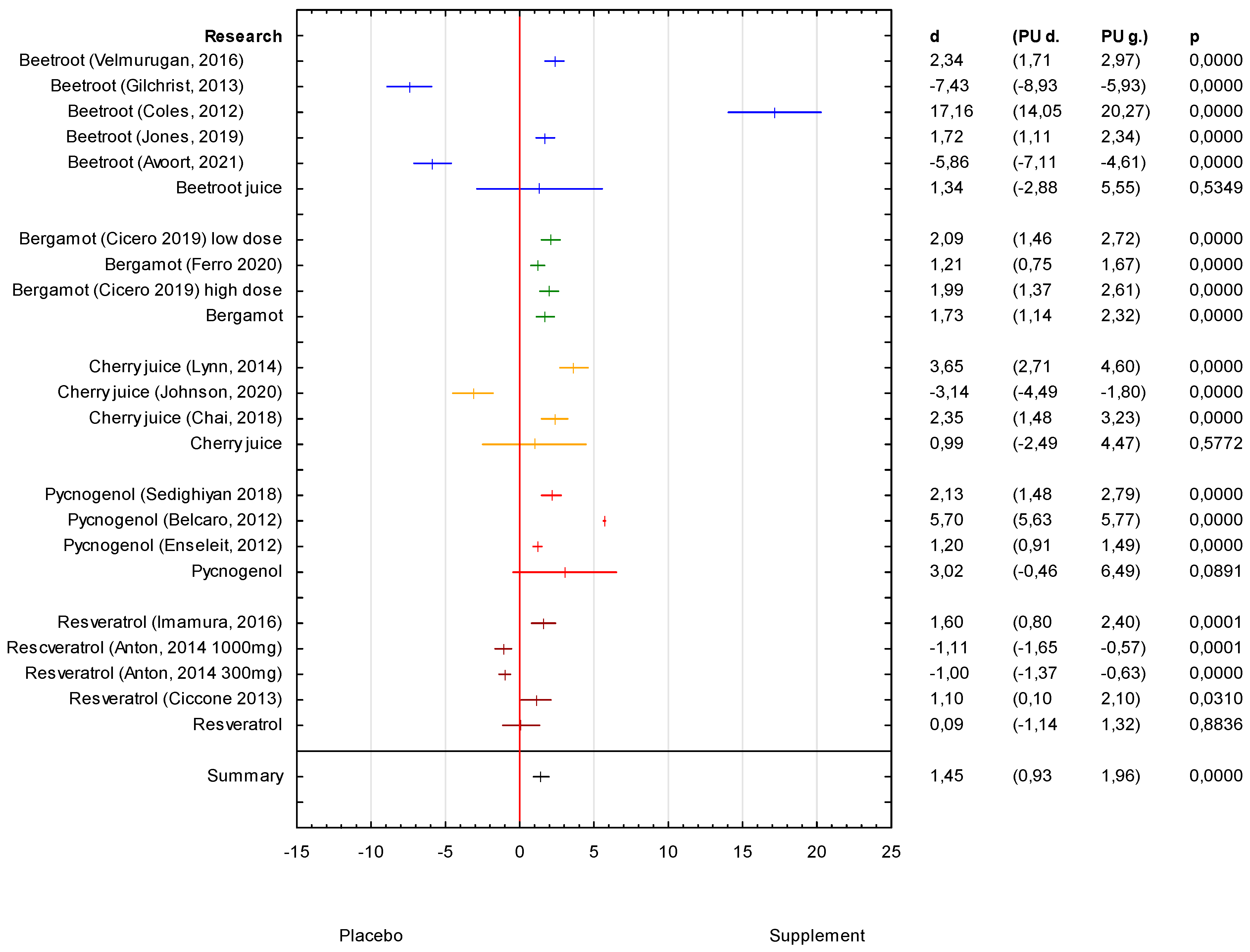
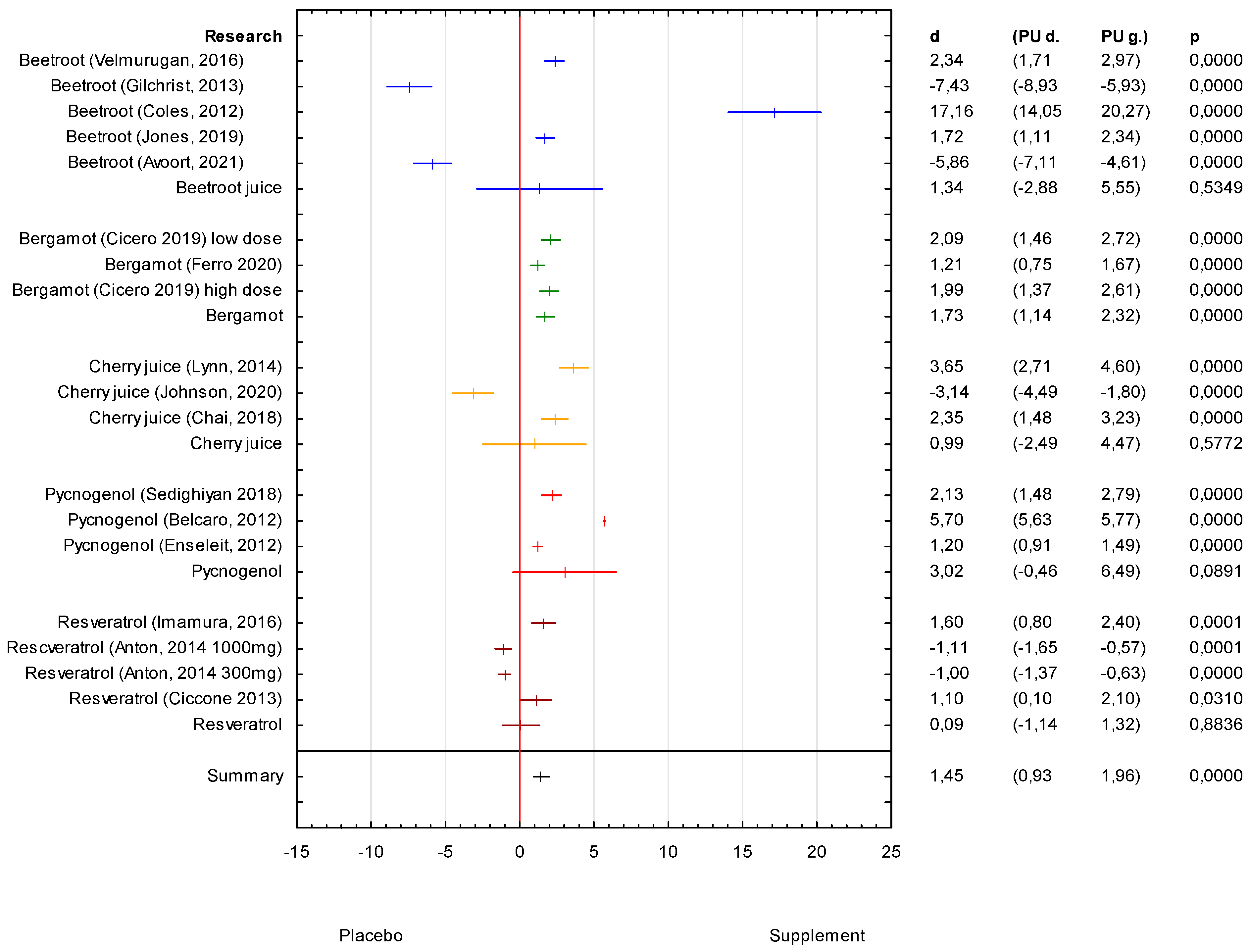
3.1. Analysis of the Supplements SBP Effectiveness
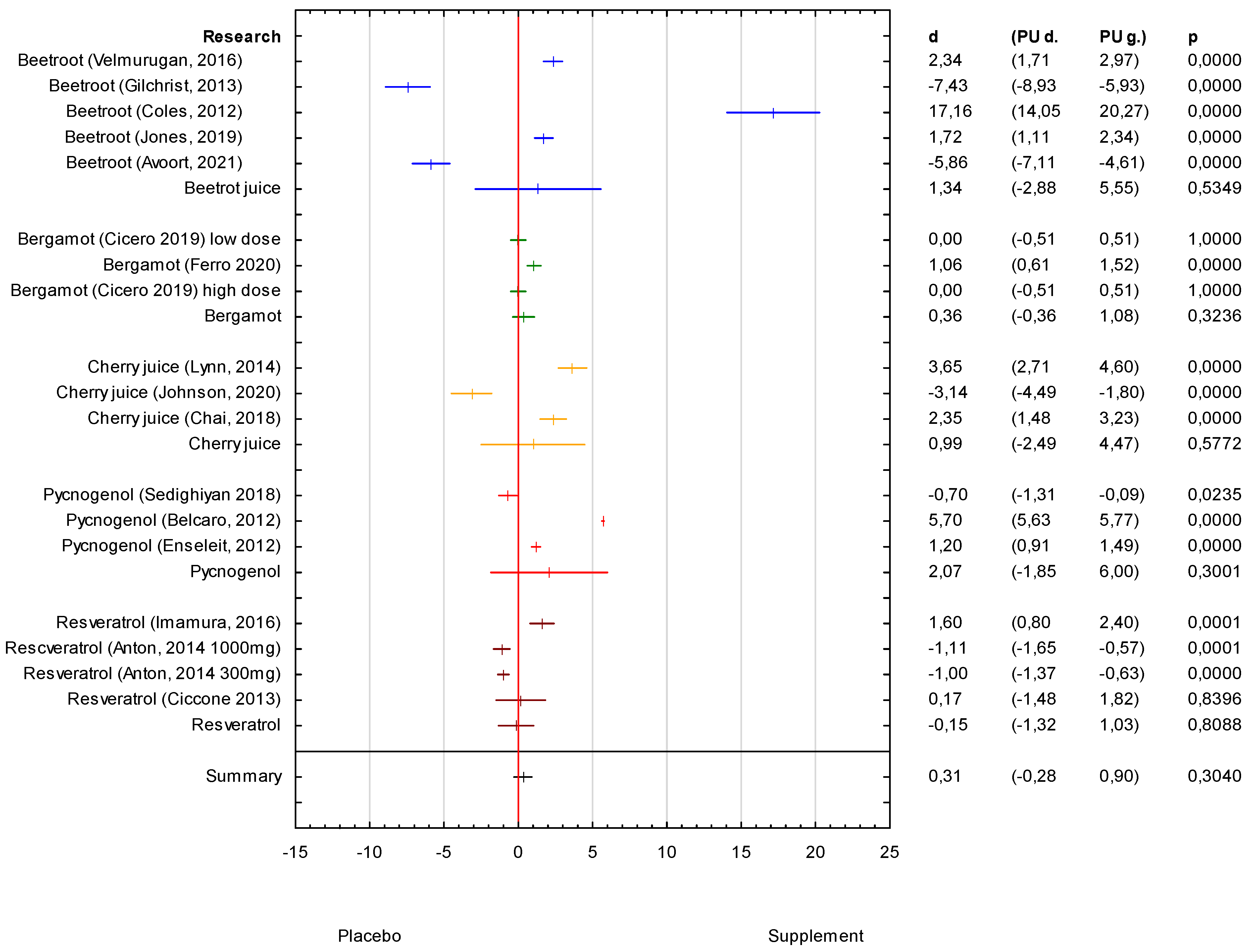
3.2. Analysis of the Supplements DBP Effectiveness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [PubMed] [Green Version]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar]
- AlJohani, S.; Salam, M.; BaniMustafa, A.; Zaidi, A.R.Z.; Aljohani, A.A.; Almutairi, A.; AlJohani, M.A.; AlSheef, M. Dietary Habits of Students Enrolled in Faculties of Health Sciences: A Cross-sectional Study. Cureus 2019, 11, e6012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Heart Association (AHA). Understanding Blood Pressure Readings. 2022. Available online: https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings (accessed on 10 June 2022).
- Visseren, F.L.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Rev. Esp. Cardiol 2022, 75, 429. [Google Scholar]
- World Health Organization. High Blood Pressure: A Public Health Problem. Available online: http://www.emro.who.int/media/world-health-day/public-health-problem-factsheet-2013.html (accessed on 10 June 2022).
- Ried, K.; Fakler, P.; Stocks, N.P. Effect of cocoa on blood pressure. Cochrane Database Syst. Rev. 2017, 4, Cd008893. [Google Scholar] [CrossRef] [PubMed]
- Hasani, H.; Arab, A.; Hadi, A.; Pourmasoumi, M.; Ghavami, A.; Miraghajani, M. Does ginger supplementation lower blood pressure? A systematic review and meta-analysis of clinical trials. Phytother. Res. 2019, 33, 1639–1647. [Google Scholar] [CrossRef]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Qi, D.; Nie, X.-L.; Zhang, J.-J. The effect of probiotics supplementation on blood pressure: A systemic review and meta-analysis. Lipids Health Dis. 2020, 19, 79. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Liu, C.; Kuang, X.; Deng, Q.; Zhao, F.; Li, D. Effects of Multivitamin and Multimineral Supplementation on Blood Pressure: A Meta-Analysis of 12 Randomized Controlled Trials. Nutrients 2018, 10, 1018. [Google Scholar] [CrossRef] [Green Version]
- Moradi, M.; Sohrabi, G.; Golbidi, M.; Yarmohammadi, S.; Hemati, N.; Campbell, M.S.; Moradi, S.; Kermani, M.A.H.; Farzaei, M.H. Effects of artichoke on blood pressure: A systematic review and meta-analysis. Complement. Ther. Med. 2021, 57, 102668. [Google Scholar] [CrossRef]
- Farzaei, M.H.; Rahimi, R.; Nikfar, S.; Abdollahi, M. Effect of resveratrol on cognitive and memory performance and mood: A meta-analysis of 225 patients. Pharmacol. Res. 2018, 128, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Xiao, M.; Zhao, J.; Li, Z.; Xing, B.; Li, X.; Kong, M.; Li, L.; Zhang, Q.; Liu, Y.; et al. An Overview of Plant Phenolic Compounds and Their Importance in Human Nutrition and Management of Type 2 Diabetes. Molecules 2016, 21, 1374. [Google Scholar] [CrossRef] [PubMed]
- Nardini, M. Phenolic Compounds in Food: Characterization and Health Benefits. Molecules 2022, 27, 783. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Viguiliouk, E.; Nishi, S.K.; Mejia, S.B.; Rahelić, D.; Kahleova, H.; Salas-Salvadó, J.; Kendall, C.W.C.; Sievenpiper, J.L. DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutrients 2019, 11, 338. [Google Scholar] [CrossRef] [Green Version]
- Hung, H.-C.; Joshipura, K.; Jiang, R.; Hu, F.B.; Hunter, D.; Smith-Warner, S.A.; Colditz, G.; Rosner, B.; Spiegelman, D.; Willett, W.C. Fruit and Vegetable Intake and Risk of Major Chronic Disease. J. Natl. Cancer Inst. 2004, 96, 1577–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nöthlings, U.; Schulze, M.B.; Weikert, C.; Boeing, H.; van der Schouw, Y.; Bamia, C.; Benetou, V.; Lagiou, P.; Krogh, V.; Beulens, J.W.J.; et al. Intake of Vegetables, Legumes, and Fruit, and Risk for All-Cause, Cardiovascular, and Cancer Mortality in a European Diabetic Population. J. Nutr. 2008, 138, 775–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kar, P.; Laight, D.; Rooprai, H.K.; Shaw, K.M.; Cummings, M. Effects of grape seed extract in Type 2 diabetic subjects at high cardiovascular risk: A double blind randomized placebo controlled trial examining metabolic markers, vascular tone, inflammation, oxidative stress and insulin sensitivity. Diabet. Med. 2009, 26, 526–531. [Google Scholar] [CrossRef]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary Approaches to Stop Hypertension (DASH) Diet and Blood Pressure Reduction in Adults with and without Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- Nahas, R. Complementary and alternative medicine approaches to blood pressure reduction: An evidence-based review. Can. Fam. Physician 2008, 54, 1529–1533. [Google Scholar]
- Brook, R.D.; Appel, L.J.; Rubenfire, M.; Ogedegbe, G.; Bisognano, J.D.; Elliott, W.J.; Fuchs, F.D.; Hughes, J.W.; Lackland, D.T.; Staffileno, B.A.; et al. Beyond medications and diet: Alternative approaches to lowering blood pressure: A scientific statement from the american heart association. Hypertension 2013, 61, 1360–1383. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Naska, A.; Kasdagli, M.; Torres, D.; Lopes, C.; Carvalho, C.; Moreira, P.; Malavolti, M.; Orsini, N.; Whelton, P.K.; et al. Potassium Intake and Blood Pressure: A Dose-Response Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2020, 9, e015719. [Google Scholar] [CrossRef] [PubMed]
- Asbaghi, O.; Naeini, F.; Ashtary-Larky, D.; Kaviani, M.; Kelishadi, M.R.; Eslampour, E.; Moradi, S.; Mirzadeh, E.; Clark, C.C.; Naeini, A.A. Effects of chromium supplementation on blood pressure, body mass index, liver function enzymes and malondialdehyde in patients with type 2 diabetes: A systematic review and dose-response meta-analysis of randomized controlled trials. Complement. Ther. Med. 2021, 60, 102755. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Lara, J.; Siervo, M. Medium-term effects of dietary nitrate supplementation on systolic and diastolic blood pressure in adults: A systematic review and meta-analysis. J. Hypertens. 2017, 35, 1353–1359. [Google Scholar] [CrossRef]
- Weaver, S.R.; Rendeiro, C.; McGettrick, H.M.; Philp, A.; Lucas, S.J.E. Fine wine or sour grapes? A systematic review and meta-analysis of the impact of red wine polyphenols on vascular health. Eur. J. Nutr. 2021, 60, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Nyambuya, T.; Nkambule, B.; Mazibuko-Mbeje, S.; Mxinwa, V.; Mokgalaboni, K.; Orlando, P.; Silvestri, S.; Louw, J.; Tiano, L.; Dludla, P. A Meta-Analysis of the Impact of Resveratrol Supplementation on Markers of Renal Function and Blood Pressure in Type 2 Diabetic Patients on Hypoglycemic Therapy. Molecules 2020, 25, 5645. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Qasem, R.J. The estrogenic activity of resveratrol: A comprehensive review of in vitro and in vivo evidence and the potential for endocrine disruption. Crit. Rev. Toxicol. 2020, 50, 439–462. [Google Scholar] [CrossRef]
- Shaito, A.; Posadino, A.M.; Younes, N.; Hasan, H.; Halabi, S.; Alhababi, D.; Al-Mohannadi, A.; Abdel-Rahman, W.M.; Eid, A.H.; Nasrallah, G.K.; et al. Potential Adverse Effects of Resveratrol: A Literature Review. Int. J. Mol. Sci. 2020, 21, 2084. [Google Scholar] [CrossRef] [Green Version]
- Fogacci, F.; Tocci, G.; Presta, V.; Fratter, A.; Borghi, C.; Cicero, A.F.G. Effect of resveratrol on blood pressure: A systematic review and meta-analysis of randomized, controlled, clinical trials. Crit. Rev. Food Sci. Nutr. 2019, 59, 1605–1618. [Google Scholar] [CrossRef]
- Zamani, H.; de Joode, M.; Hossein, I.J.; Henckens, N.F.T.; Guggeis, M.A.; Berends, J.E.; de Kok, T.M.C.M.; van Breda, S.G.J. The benefits and risks of beetroot juice consumption: A systematic review. Crit. Rev. Food Sci. Nutr. 2020, 61, 788–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakubcik, E.M.; Rutherfurd-Markwick, K.; Chabert, M.; Wong, M.; Ali, A. Pharmacokinetics of Nitrate and Nitrite Following Beetroot Juice Drink Consumption. Nutrients 2021, 13, 281. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Paula, G.H.; Lacchini, R.; Tanus-Santos, J.E. Endothelial nitric oxide synthase: From biochemistry and gene structure to clinical implications of NOS3 polymorphisms. Gene 2016, 575, 584–599. [Google Scholar] [CrossRef] [PubMed]
- Lubos, E.; Handy, D.E.; Loscalzo, J. Role of oxidative stress and nitric oxide in atherothrombosis. Front. Biosci. 2008, 13, 5323–5344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghi, C.; Cicero, A.F.G. Nutraceuticals with a clinically detectable blood pressure-lowering effect: A review of available randomized clinical trials and their meta-analyses. Br. J. Clin. Pharmacol. 2017, 83, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Kapil, V.; Khambata, R.S.; Robertson, A.; Caulfield, M.J.; Ahluwalia, A. Dietary nitrate provides sustained blood pressure lowering in hypertensive patients: A randomized, phase 2, double-blind, placebo-controlled study. Hypertension 2015, 65, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Imenshahidi, M.; Hosseinzadeh, H. Berberis Vulgaris and Berberine: An Update Review. Phytother Res. 2016, 30, 1745–1764. [Google Scholar] [CrossRef]
- Lazavi, F.; Mirmiran, P.; Sohrab, G.; Nikpayam, O.; Angoorani, P.; Hedayati, M. The barberry juice effects on metabolic factors and oxidative stress in patients with type 2 diabetes: A randomized clinical trial. Complement. Ther. Clin. Pract. 2018, 31, 170–174. [Google Scholar] [CrossRef]
- Carresi, C.; Gliozzi, M.; Musolino, V.; Scicchitano, M.; Scarano, F.; Bosco, F.; Nucera, S.; Maiuolo, J.; Macrì, R.; Ruga, S.; et al. The Effect of Natural Antioxidants in the Development of Metabolic Syndrome: Focus on Bergamot Polyphenolic Fraction. Nutrients 2020, 12, 1504. [Google Scholar]
- Perna, S.; Spadaccini, D.; Botteri, L.; Girometta, C.; Riva, A.; Allegrini, P.; Petrangolini, G.; Infantino, V.; Rondanelli, M. Efficacy of bergamot: From anti-inflammatory and anti-oxidative mechanisms to clinical applications as preventive agent for cardiovascular morbidity, skin diseases, and mood alterations. Food Sci. Nutr. 2019, 7, 369–384. [Google Scholar]
- Chai, S.C.; Davis, K.; Zhang, Z.; Zha, L.; Kirschner, K.F. Effects of Tart Cherry Juice on Biomarkers of Inflammation and Oxidative Stress in Older Adults. Nutrients 2019, 11, 228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malekahmadi, M.; Moradi Moghaddam, O.; Firouzi, S.; Daryabeygi-Khotbehsara, R.; Islam, S.M.S.; Norouzy, A.; Soltani, S. Effects of pycnogenol on cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2019, 150, 104472. [Google Scholar] [CrossRef] [PubMed]
- Pourmasoumi, M.; Hadi, A.; Mohammadi, H.; Rouhani, M.H. Effect of pycnogenol supplementation on blood pressure: A systematic review and meta-analysis of clinical trials. Phytotherapy Res. 2020, 34, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Tocci, G.; Sahebkar, A.; Presta, V.; Banach, M.; Cicero, A.F.G. Effect of Pycnogenol on Blood Pressure: Findings From a PRISMA Compliant Systematic Review and Meta-Analysis of Randomized, Double-Blind, Placebo-Controlled, Clinical Studies. Angiology 2010, 71, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gallegos, J.L.; Haskell-Ramsay, C.; Lodge, J.K. Effects of chronic consumption of specific fruit (berries, citrus and cherries) on CVD risk factors: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Nutr. 2021, 60, 615–639. [Google Scholar] [CrossRef] [PubMed]
- Bahadoran, Z.; Mirmiran, P.; Kabir, A.; Azizi, F.; Ghasemi, A. The Nitrate-Independent Blood Pressure–Lowering Effect of Beetroot Juice: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Velmurugan, S.; Gan, J.M.; Rathod, K.S.; Khambata, R.S.; Ghosh, S.M.; Hartley, A.; Van Eijl, S.; Sagi-Kiss, V.; Chowdhury, T.A.; Curtis, M.; et al. Dietary nitrate improves vascular function in patients with hypercholesterolemia: A randomized, double-blind, placebo-controlled study. Am. J. Clin. Nutr. 2016, 103, 25–38. [Google Scholar] [CrossRef] [Green Version]
- Hadi, A.; Arab, A.; Ghaedi, E.; Rafie, N.; Miraghajani, M.; Kafeshani, M. Barberry (Berberis vulgaris L.) is a safe approach for management of lipid parameters: A systematic review and meta-analysis of randomized controlled trials. Complement Ther. Med. 2019, 43, 117–124. [Google Scholar] [CrossRef]
- Asgary, S.; Karimi, R.; Momtaz, S.; Naseri, R.; Farzaei, M.H. Effect of resveratrol on metabolic syndrome components: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2019, 20, 173–186. [Google Scholar] [CrossRef]
- Akbari, M.; Tamtaji, O.R.; Lankarani, K.B.; Tabrizi, R.; Dadgostar, E.; Kolahdooz, F.; Jamilian, M.; Mirzaei, H.; Asemi, Z. The Effects of Resveratrol Supplementation on Endothelial Function and Blood Pressures Among Patients with Metabolic Syndrome and Related Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. High Blood Press. Cardiovasc. Prev. 2019, 26, 305–319. [Google Scholar] [CrossRef]
- Pollack, R.M.; Barzilai, N.; Anghel, V.; Kulkarni, A.; Golden, A.; Broin, P.; Sinclair, D.; Bonkowski, M.; Coleville, A.J.; Powell, D.; et al. Resveratrol Improves Vascular Function and Mitochondrial Number but Not Glucose Metabolism in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Dyck, G.J.B.; Raj, P.; Zieroth, S.; Dyck, J.R.B.; Ezekowitz, J.A. The Effects of Resveratrol in Patients with Cardiovascular Disease and Heart Failure: A Narrative Review. Int. J. Mol. Sci. 2019, 20, 904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedman, B. Placebo-controlled trials and the logic of clinical purpose. IRB Ethics Hum. Res. 1990, 12, 1–6. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Name of the Supplement | Author Year | Sample | Supplement Administration Protocol | Duration | Form of Supplement | Significant Results |
|---|---|---|---|---|---|---|
| Resveratrol | Anton, 2014 | 32 overweight adults over 65 y | 300 mg/day or 1000 mg/day or placebo | 1 month | Product was provided by Reserveage Organics and contained naturally-derived resveratrol from grapes and wild Japanese knotweed (Polygonum cuspidatum). Microcrystalline cellulose was used for the placebo. | Daily resveratrol supplementation is generally well-tolerated in overweight, older adults. |
| Imamura, 2016 | 50 patients with T2DM | 100 mg/day or placebo | 12 weeks | Resveratrol was obtained from the BHN Corporation (Tokyo) as resveratrol-ε, which is derived from grape stems. Supplement of a 100-mg resveratrol (total resveratrol: oligo-stilbene 27.97 mg/100 mg/day) or placebo tablet. | Resveratrol supplementation decreased: systolic BP (−5.5 mmHg), d-ROMs (−25.6 ± 41.8 U.CARR), CAVI (−0.4 ± 0.7), BW (−0.8 ± 2.1 kg,), and body mass index (−0.5 kg/m2). Resveratrol supplementation improved arterial stiffness and reduced oxidative stress in patients with T2DM. | |
| Ciccone, 2013 | 50 eligible healthy volunteers aged 20–50 years | 500 mg/day or placebo | 1 month | Supplement Transmax (resveratrol, 500 mg, Biotivia Bioceuticals LLC). | Resveratrol supplementation significantly reduced triglyceride and C-reactive protein (CRP) concentrations and increased Total Antioxidant Status (TAS) values. | |
| Cherry juice | Chai, 2018 | 37 healthy adults, aged 65–80 years | 480 mL of tart cherry juice or control drink per day | 12 weeks | A total of 68 mL of Montmorency tart cherry concentrate (King Orchards, MI, USA) was diluted with 412 mL water. The control drink had the colour and taste as close as possible to the tart cherry juice, and it was prepared by mixing unsweetened black cherry-flavoured Kool-Aid (Kraft Foods, United States) with water. Drinks were consumed twice a day (in the morning and evening) in a dose of 240 mL per time. | Tart cherry juice decreased the levels of LDL and systolic BP. |
| Lynn, 2014 | 47 healthy adults, aged 30–50 years | 250 mL of tart cherry juice or control drink per day | 6 weeks | A total of 250 mL of tart cherry juice (30 mL concentrate—Cherry Active) diluted in water or the same volume of control drink-lemonade (Sprite) was consumed per day. | Tart cherry juice had no effect on arterial stiffness, c-reactive protein, and risk markers for cardiovascular disease. Some antioxidant effects can be observed among healthy adults. | |
| Johnson, 2020 | 19 participants with metabolic syndrome, aged 20–60 years | 480 mL of tart cherry juice or control drink per day | 12 weeks | The tart cherry juice consisted of Montmorency tart cherry juice and concentrate (Indian Summer, Inc., Traverse City, MI, USA). The tart cherry juice and the placebo-control drink were consumed twice a day (240 mL each, in the morning and in the evening). | Tart cherry juice decreased the levels of LDL and total cholesterol. There were no significant effects on hemodynamic or arterial stiffness parameters. | |
| Bergamot | Cicero, 2019 | 90 overweight participants with dyslipidaemia; aged 20–75 years | pill with bergamot extract (120-mg flavonoids/pill) or placebo pill; two pills per day | 8 weeks | Before the treatment period, there was the diet standardization and physical activity period (2 weeks). A patient from the high-dose group was given two boxes with active treatment-Colber (from Esserre Pharma srl, Rome, Italy) containing bergamot extract (120 mg flavonoids/pill). A patient from the low-dose group was given one box with an active treatment and one with placebo. The patient from the placebo group was given two boxes with placebo pills. Each patient had 170 pills and took one tablet from each of two boxes at bedtime. | Improvement in TG, LDL; total cholesterol, C-reactive protein, and tumour necrosis factor-α decreased; improved lipid and glucose metabolism, adipokines pattern, and systemic inflammation in overweight subjects with dyslipidaemia. |
| Ferro, 2020 | 102 patients with liver steatosis; aged 30–75 years | 300 mg/day or placebo | 12 weeks | Participants received a nutraceutical from Bergamot and wild cardoon or placebo. | Liver fat content reduction, especially in participants over 50 years. | |
| Pycnogenol | Belcaro, 2013 | 130 participants with metabolic syndrome, aged 45–55 years | 150 mg/day or placebo | 6 months | The 50-mg tablets with Pycnogenol, from GEFA (Chateaugiron, France), were taken three times a day (total 150 mg of Pycnogenol per day) | Pycnogenol supplementation decreased levels of TG, fasting glucose, and plasma free radicals and increased the HDL cholesterol level. Pycnogenol decreased waist circumference and blood pressure. |
| Enseleit, 2012 | 23 patients with coronary artery disease, aged 49–73 years | 200 mg/day | 8 weeks | - | Pycnogenol supplementation improved endothelial function in patients with coronary artery disease by reducing oxidative stress. | |
| Sedighiyan, 2018 | 38 obese women, aged 18–45 years | 150 mg/day or placebo | 2 months | Women received a weight loss diet and tablets (the PBE group) with 150 mg pine bark extract, from Source Naturals (CA, USA) and the placebo group received one placebo tablet (containing starch powder) per day for 2 months with a meal. | Pine bark extract had positive effects on TG, fasting blood sugar, HDL, and BP. It had a protective effect on metabolic syndrome in obesity. | |
| Beetroot juice | Avoort, 2021 | 77 (pre)hypertensive adults, mean age 65 y | 250–300 g of nitrate-rich vegetables consumption (containing ∼350–400 mg nitrate/∼6–6.5 mmol nitrate) vs. 70 mL BRJ drink (400 mg nitrate) vs. control (usual dietary behaviour) | 12 weeks | Personalized dietary intervention vs. concentrated red beetroot juice (Beet-it Sport®, 70 mL; James White Drinks Ltd.) vs. usual diet. | A prolonged dietary intervention with high-nitrate vegetable intake lowered SBP in (pre)hypertensive middle-aged and older adults. DBP did not change in any of the groups. |
| Gilchrist, 2013 | 27 adults with type 2 diabetes, mean age 67 y | 250 mL BRJ (7.5 mmol of nitrate) daily or 250 mL nitrate-depleted BRJ (0.002 mmol of nitrate) | 2 weeks | BRJ sold as a beverage. They used their own procedure for the production of placebo juice, using a column containing a nitrate-specific anion-exchange resin (Purolite A520e). | Supplementation with 7.5 mmol of nitrate per day did not lower BP or improve endothelial function in individuals with type 2 diabetes. | |
| Jones, 2019 | 20 healthy older adults, mean age 63 y | 70 mL NO3− rich BRJ (400 mg of NO3−) a day vs. placebo | 28 days (±7) | BRJ drink (Beet-It Sport Shot 400). Prune juice was used for the placebo. | BRJ ingestion potentially improved BP. A decrease in SBP (−6 mmHg) and DBP (−4 mmHg) was significant (p = 0.04; p = 0.01, respectively). BP remained unchanged in the placebo group. | |
| Coles, 2012 | 30 healthy adults, mean age 42 y | 500 g of beetroot and apple juice (BJ) containing 15 mmol nitrate/L or a placebo juice | 24 h (measurements every hour after consumption) | Beetroot and apple juice (72% beetroots and 28% apples) vs. placebo (apple) juice; both supplied by Sunraysia Natural Beverage Company, Melbourne, VIC. | Trend of a lower SBP at 6 h after drinking BJ relative to placebo. Only men demonstrated a significant reduction in SBP (4–5 mmHg) at 6 h after BJ consumption. | |
| Velmurugan, 2016 | 67 adults with untreated hypercholesterolemia, mean age 53 y | 250 mL nitrate-rich BRJ vs. placebo (nitrate-depleted BRJ) | 6 weeks | For BRJ, they used James Whites Drinks. The placebo juice was generated from the same batch of nitrate-replete juice by using a standard anion exchange resin, as described in the protocol. | Dietary nitrate ingestion lowered SBP (−4 mmHg) and improved vascular function (increase in the FMD response with a worsening in the placebo group) in hypercholesterolemic patients. |
| Name of the Supplement | Author Year | Sample | Supplement Administration Protocol | Placebo Group | Duration | Form of Supplement | Findings |
|---|---|---|---|---|---|---|---|
| Resveratrol | Pollack, 2017 | older glucose-intolerant adults aged 50–80 years (n = 30) | A resveratrol dose of 1500 mg twice daily was administered to the initial nine participants; however, because of gastrointestinal side effects, subsequent participants received 1000 mg twice daily. The study consisted of two randomly assigned 6-week treatment periods (resveratrol and placebo). Participants were instructed to begin the study drug on the evening following the baseline measurements and continue through the evening prior to metabolic testing at the end of each treatment period. Following a 3-week washout period, the participants crossed over to the other intervention for the second 6-week treatment period. | Older glucose-intolerant adults aged 50–80 years (n = 30) | 6 weeks | Resveratrol capsules (RevGenetics Corporation) | No changes in glucose tolerance, insulin sensitivity, weight, blood pressure, or lipid profile; however, resveratrol treatment may have beneficial effects on vascular function |
| Ligt, 2020 | 41 men and women (BMI: 27–35 kg/m2; aged 40–70 y | A total of 150 mg/d of resveratrol (n = 20) was administered in two doses of 75 mg per day—1 during lunch and 1 during dinner. | 21 persons | 6 months | Trans-resveratrol (resVida, 99.9%; provided by DSM Nutritional Products) capsules | No differences were found in intrahepatic lipid, body composition, blood pressure, energy metabolism, physical performance, or quality of life and sleep between treatment arms. | |
| Cherry juice | Desai, 2018 | 11 healthy, recreationally active participants; 30 ± 10 years | 260 mL of Montmorency tart cherry juice or placebo per day | 20 days | A total of 30 mL of Montmorency tart cherry concentrate (Cherry Active, Active Edge Ltd., Hanworth, UK) and 100 mL of water gave 130 mL of tart cherry juice, and the placebo drink was made with 30 mL of commercially available fruit-flavoured cordial (Cherries and Berries, Morrisons Bradford, UK) and 100 mL of water. The amount of 130 mL of drinks was consumed twice a day (in the morning and in the evening). | Consumption of Montmorency tart cherry juice in addition to exercising did not give an improvement on cardio-metabolic biomarkers. | |
| Beetroot juice | Asgary, 2016 | 24 hypertensive subjects aged 25–68 years old | 250 mL/day raw beet juice (RBJ) vs. 250 g/day cooked beet (CB) | NA | 2 weeks, followed by a 2-week washout period before entering the second phase of the study and receiving alternate treatment | Participants own preparation according to instruction | Both RBJ and CB were effective in improving BP, endothelial function, and systemic inflammation. BRJ had greater antihypertensive effects. More improvement was observed in endothelial function and systemic inflammation with RBJ compared with CB. |
| Avoort, 2020 | 30 recreationally active individuals, mean age 24 years | 250 g vegetables (ca.400 mg nitrate daily) at lunch vs. 70 mL of red beetroot juice/day | NA | BP measurement fasting and 2.5 h after lunch on day 1, 4, and 7. | Participant own preparation vs. BRJ drink (Beet-it Sport; James White Drinks Ltd.). | Fasting mean systolic and diastolic BP did not change, but the mean systolic and diastolic BP assessed 2.5 h after lunch were significantly reduced in both groups (SBP −5.1 mm Hg and DBP −5.3 mm Hg). | |
| Bondonno, 2015 | 27 treated hypertensive individuals | 2 × 70 mL concentrated nitrate-rich beetroot juice (70 mL with breakfast and 70 mL with dinner) vs. placebo | 2 × 70 mL of nitrate-depleted beetroot juice (70 mL with breakfast and 70 mL with dinner) | 1 week | Concentrated nitrate-rich beetroot-juice beverage (Beet it; James White Drinks Ltd.) vs. nitrate-depleted beetroot juice beverage (Beet it; James White Drinks Ltd.). | No differences in home BP and 24-h ambulatory BP were observed with the 1-wk intake of nitrate-rich beetroot juice in comparison with the placebo. | |
| Gallardo, 2021 | 9 healthy older subjects, mean age 70 y | 3.3 mL/kg of concentrated beetroot juice containing 0, 200, or 400 µmol/kg of nitrate. Pts received all doses, with a 1- to 2-week washout period between visits. | Placebo: 3.3 mL/kg BRJ devoid of NO3−(0) | 2 h | A commercial concentrated beetroot juice (BRJ) supplement (Beet It Sport, James White Drinks, Ipswich, UK); placebo was produced by extracting NO3− from BRJ using a highly selective anion exchange resin (i.e., Purolite a520e). | No significant changes were found in systolic, diastolic, or mean arterial blood pressure. | |
| Hobbs, 2012 | 18 normotensive individuals | Study 1. (n = 18) one intervention: 0 g BJ (500 g water) as a control; or 100 g BJ with 400 g water; or 250 g BJ with 250 g water or 500 g BRJStudy 2. (n = 14) one intervention: 200 g white bread (control, 0 g beetroot enrichment); or 200 g bread enriched with either white or red beetroot (comprising 50% of the total weight of dough before baking). | NA | 24 h | BRJ—James White Drinks Limited. The control drink and BJ drinks were all diluted with low-nitrate mineral water (The Buxton Mineral Water Company Limited). Bread products (Eccentricities Limited). | BJ consumption significantly, and in a near dose-dependent manner, lowered SBP and DBP over a period of 24 h, compared with the water control. Bread products enriched with 100 g of red or white beetroot lowered SBP and DBP over a period of 24 h, with no statistical differences between the varieties. | |
| Avoort, 2020 | 15 healthy men and women, mean age 24 y | 400 mg of nitrate at lunch, provided through nitrate-rich vegetables and dietary counselling, or 70 mL beetroot juice supplementation. | NA | 1 week, with 1-week washout | Dietary instruction for patients; (70 mL) of red beetroot juice (Beet-it Sport; James White Drinks Ltd.) | Fasting mean SBP and DBP did not change, but mean SBP and DBP assessed 2.5 h after lunch were significantly reduced throughout both intervention periods (p < 0.05), with no differences between beetroot juice and nitrate-rich vegetables. | |
| Jakubcik, 2021 | 11 healthy adults, 18–50 years old | 250 mL of BR containing one of the following: (i) high NO3−, low NO2− (HL; 572 mg NO3−, 32 mg NO2−); (ii) medium NO3−, medium NO2− (MM; 280 mg NO3−, 237 mg NO2−); (iii) low NO3−, medium NO2− (LM; 43 mg NO3−, 262 mg NO2−); (iv) placebo (PL; low NO3−, low NO2−: 8 mg NO3−, 5.8 mg NO2−). | placebo (PL; low NO3−, low NO2−: 8 mg NO3−, 5.8 mg NO2−) | 6 h | Prepared according to the protocol | There was no effect of NO3− or NO2− ingestion on SBP or DBP compared to PL. Mean arterial pressure decreased following the consumption of HL, MM, and LM; however, in comparison, LM showed its effect 2 h later. | |
| Kapil, 2015 | 68 hypertensive patients, 18–85 years old | 250 mL BRJ vs. 250 mL placebo | n = 34 | 4 weeks | 250 mL of beetroot juice, James White Drinks Ltd., Ipswich, UK; placebo 250 mL nitrate-depleted beetroot juice, James White Drinks Ltd., Ipswich, UK. | Mean reduction in clinic BP was 7.7/2.4 mmHg; 24 h ambulatory blood pressure was reduced by 7.7/5.2 mmHg, and home blood pressure was reduced by 8.1/3.8 mmHg. Endothelial function improved by ~20%, and arterial stiffness reduced by 0.59 m/s after dietary nitrate consumption with no change after placebo | |
| McDonagh, 2018 | 10 healthy, normotensive males, age 24 y | 55 mL of a concentrated beetroot juice drink (∼5.76 mmol) (BR); 456 mL of a non-concentrated beetroot juice drink (BL), and a solid beetroot flapjack (BF; 60 g). A drink containing soluble beetroot crystals (BC; ∼1.40 mmol NO3−) and a control drink (CON; 70 mL deionised water) were also ingested. | NA | 24 h | Concentrated beetroot drink (55 mL of Beet It Sport Stamina Shot, James White Drinks, Ltd., Ipswich, UK), a non-concentrated beetroot drink (456 mL of Beet It Organic Beetroot Juice, James White Drinks, Ltd., Ipswich, UK) and a beetroot flapjack (60 g of Beet It Pro Elite Sport Flapjack, James White Drinks, Ltd., Ipswich, UK). In addition, subjects consumed the recommended dose (5 g dissolved in 114 mL of water; 1.40 mmol NO3− and ∼0.07 mmol NO2− ) of Concentrated Organic Beetroot Crystals (SuperBeets Canister; Neogenis, now known as HumanN, Texas, US), and a control drink (70 mL deionised water) that contained negligible NO3− and NO2− contents. | BR, but not BF, BL, and BC, reduced systolic (∼5 mmHg) and mean arterial pressure (∼3–4 mmHg; p < 0.05), whereas BF reduced diastolic BP (∼4 mmHg; p < 0.05). | |
| Siervo, 2020 | 47 middle-aged and older participants, age: 50–70 y, with elevated blood pressure | (1) high-nitrate beetroot juice (∼400 mg nitrate) and folic acid (∼5 mg folic acid) (N + F), (2) high-nitrate beetroot juice and placebo (N + P), or (3) nitrate-depleted beetroot juice and placebo (P + P). | n = 15 | 60 days | N + F: 70 mL of concentrated beetroot juice (Beet It shots, James White Ltd.) and 1 capsule of folate (folic acid, 5 mg, Bio-Tech Pharmacal Inc.). N + P: 70 mL of concentrated beetroot juice as group 1 (Beet It, James White Ltd.) and 1 placebo capsule containing sucrose powder. P + P: 70 mL of nitrate-depleted beetroot juice (<1 mg inorganic nitrate, James White Ltd.) and a placebo capsule containing sucrose powder. | After 60 d, 24-h systolic BP dropped by −10.8 ± 9.8 mm Hg (p < 0.001), −6.1 ± 13.2 mm Hg (p = 0.03), and −0.3 ± 9.7 mm Hg (p = 0.83) in the N + P, N + F, and P + P groups, respectively. There was a significant decrease in 24-h diastolic BP in the N + P group (−5.4 ± 5.0 mm Hg, p = 0.004), whereas changes were not significant in the N + F (−1.8 ± 8.1 mm Hg, p = 0.32) and P + P (1.6 ± 8.3 mm Hg, p = 0.43) groups. | |
| Stanaway, 2019 | 13 younger (18–30 years) and 11 older (50–70 years) recreationally active adults | Pts consumed either 150 mL of nitrate-rich beetroot juice (BR; 10.5 mmol nitrate) or placebo (PL; 1 mmol nitrate). | The same as a study group | BP measurements before and 145 min after supplementation | Beetroot juice, extracted from fresh washed beetroots (beta vulgaris ‘Pablo’), was blended with other fruit juices to provide a standardized beetroot juice drink with a constant soluble solid concentration and nitrate concentration (10.5 mmol/150 mL). The placebo beetroot drink was produced using beetroot juice concentrate and standardized to the same constant soluble solids concentration but contained a low nitrate concentration (1 mmol/150 mL). | BR consumption significantly increased plasma nitrate and nitrite concentrations and reduced SBP (p < 0.001) in both age groups and reduced DBP (p = 0.013) in older adults. | |
| Barberry | Lazavi, 2018 | 46 diabetic patients; aged 30–70 years | 200 mL of barberry juice daily | Control group received no intervention | 8 weeks | The concentrated barberry juice was diluted with water. | The consumption of barberry juice decreased systolic and diastolic blood pressure, TG, fasting blood sugar, and total cholesterol. The risk of cardiovascular diseases might decrease in patients with diabetes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipert, A.; Szadkowska, I.; Matusiak-Wieczorek, E.; Kochan, E. The Effect of Herbal Supplements on Blood Pressure: Systematic Review and Meta-Analysis. Antioxidants 2022, 11, 1419. https://doi.org/10.3390/antiox11081419
Lipert A, Szadkowska I, Matusiak-Wieczorek E, Kochan E. The Effect of Herbal Supplements on Blood Pressure: Systematic Review and Meta-Analysis. Antioxidants. 2022; 11(8):1419. https://doi.org/10.3390/antiox11081419
Chicago/Turabian StyleLipert, Anna, Iwona Szadkowska, Ewelina Matusiak-Wieczorek, and Ewa Kochan. 2022. "The Effect of Herbal Supplements on Blood Pressure: Systematic Review and Meta-Analysis" Antioxidants 11, no. 8: 1419. https://doi.org/10.3390/antiox11081419
APA StyleLipert, A., Szadkowska, I., Matusiak-Wieczorek, E., & Kochan, E. (2022). The Effect of Herbal Supplements on Blood Pressure: Systematic Review and Meta-Analysis. Antioxidants, 11(8), 1419. https://doi.org/10.3390/antiox11081419