
Factors Involved in Endothelial Dysfunction Related to Angiogenic Disbalance and Oxidative Stress, in Women at High Risk of Term Pre-Eclampsia

 , , and
, , and
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Demographic and Clinical Characteristics of the Participants
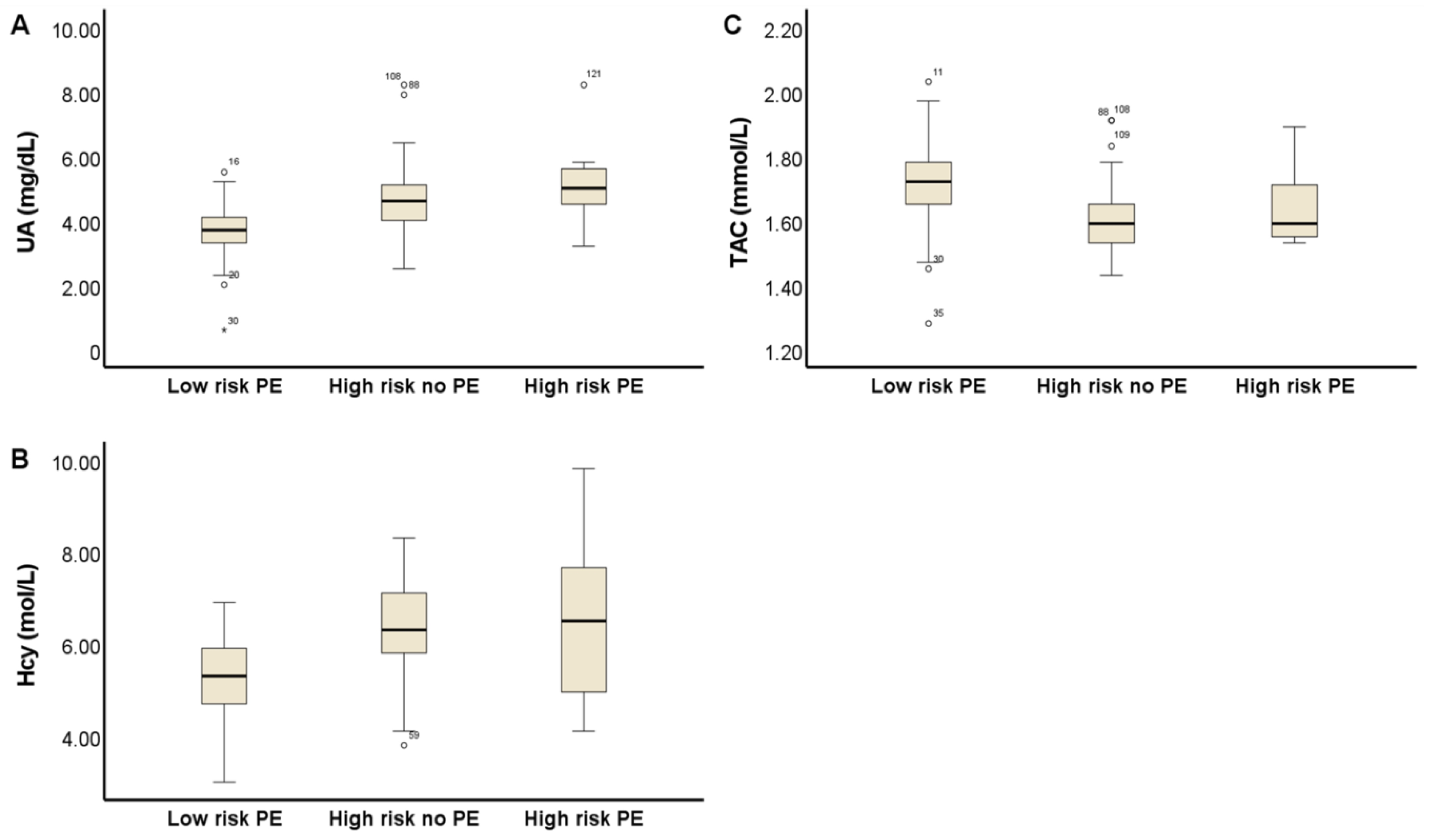
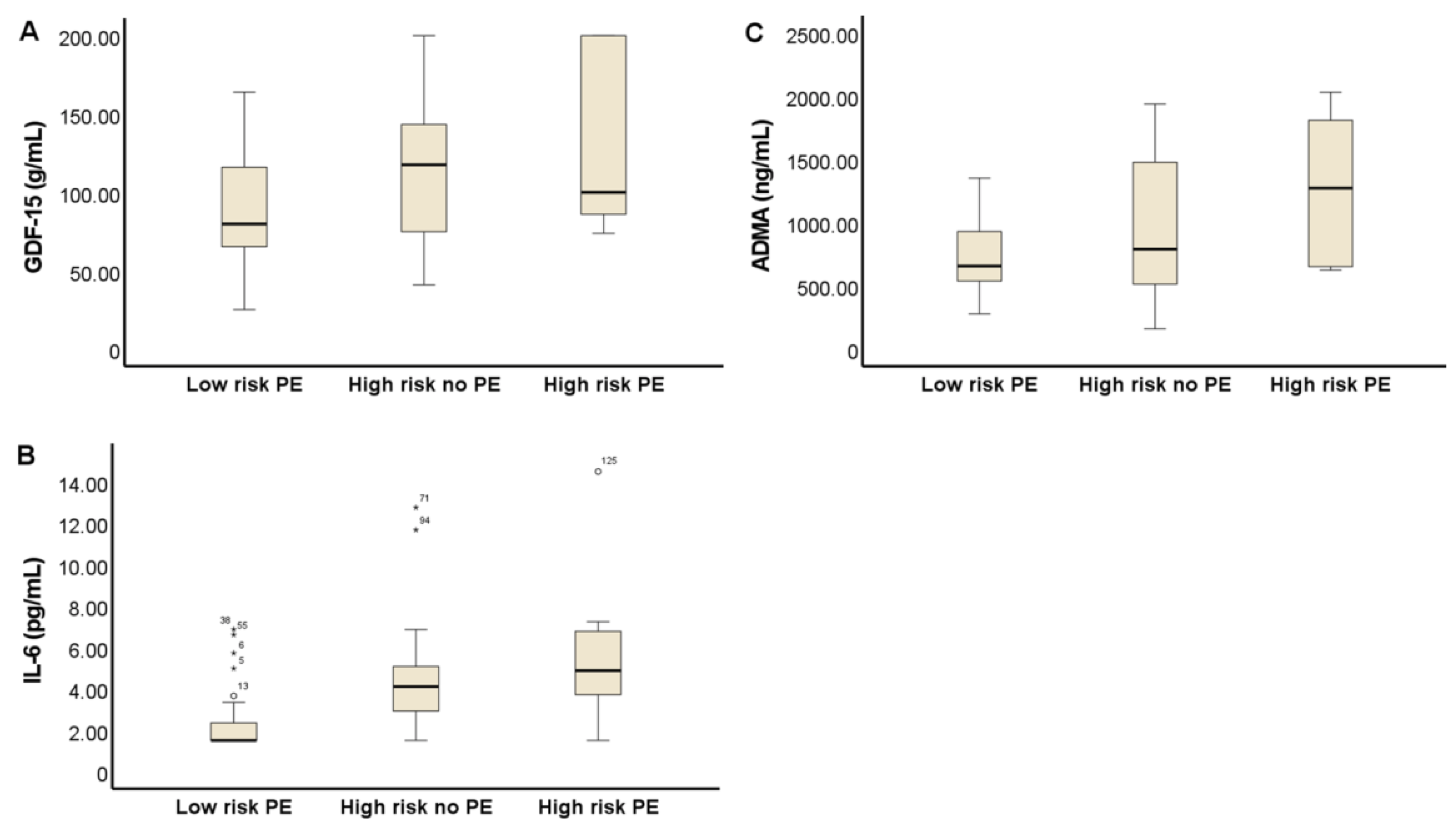
3.2. Biomarkers Related to Vascular Dysfunction Associated with PE and CVD
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Staff, A.C. The two-stage placental model of preeclampsia: An update. J. Reprod. Immunol. 2019, 134–135, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Stanhewicz, A.E. Residual vascular dysfunction in women with a history of preeclampsia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, R1062–R1071. [Google Scholar] [CrossRef] [PubMed]
- Orabona, R.; Sciatti, E.; Vizzardi, E.; Bonadei, I.; Prefumo, F.; Valcamonico, A.; Metra, M.; Frusca, T. Maternal endothelial function and vascular stiffness after HELLP syndrome: A case–control study. Ultrasound Obstet. Gynecol. 2017, 50, 596–602. [Google Scholar] [CrossRef] [Green Version]
- Moe, K.; Sugulle, M.; Dechend, R.; Angel, K.; Staff, A.C. Functional and structural vascular biomarkers in women 1 year after a hypertensive disorder of pregnancy. Pregnancy Hypertens. 2020, 21, 23–29. [Google Scholar] [CrossRef]
- Weissgerber, T.L.; Milic, N.M.; Milin-Lazovic, J.S.; Garovic, V.D. Impaired Flow-Mediated Dilation Before, During, and After Preeclampsia: A Systematic Review and Meta-Analysis. Hypertension 2016, 67, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Wright, D.; Wright, A.; Nicolaides, K.H. The competing risk approach for prediction of preeclampsia. Am. J. Obstet. Gynecol. 2020, 223, 12–23.e7. [Google Scholar] [CrossRef] [PubMed]
- Döbert, M.; Wright, A.; Varouxaki, A.N.; Mu, A.C.; Syngelaki, A.; Rehal, A.; Delgado, J.L.; Akolekar, R.; Muscettola, G.; Janga, D.; et al. STATIN trial: Predictive performance of competing-risk model in screening for pre-eclampsia at 35–37 weeks’ gestation. Ultrasound Obstet. Gynecol. 2021, 59, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Ciobanu, A.; Wright, A.; Panaitescu, A.; Syngelaki, A.; Wright, D.; Nicolaides, K.H. Prediction of imminent preeclampsia at 35–37 weeks gestation. Am. J. Obstet. Gynecol. 2019, 220, 584.e1–584.e11. [Google Scholar] [CrossRef]
- McDonald, S.D.; Malinowski, A.; Zhou, Q.; Yusuf, S.; Devereaux, P.J. Cardiovascular sequelae of preeclampsia/eclampsia: A systematic review and meta-analyses. Am. Heart J. 2008, 156, 918–930. [Google Scholar] [CrossRef]
- Bokslag, A.; Teunissen, P.W.; Franssen, C.; van Kesteren, F.; Kamp, O.; Ganzevoort, W.; Paulus, W.J.; de Groot, C.J. Effect of early-onset preeclampsia on cardiovascular risk in the fifth decade of life. Am. J. Obstet. Gynecol. 2017, 216, 523.e1–523.e7. [Google Scholar] [CrossRef] [Green Version]
- Thilaganathan, B.; Kalafat, E. Cardiovascular System in Preeclampsia and Beyond. Hypertension 2019, 73, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Turbeville, H.R.; Sasser, J.M. Preeclampsia beyond pregnancy: Long-term consequences for mother and child. Am. J. Physiol. Renal Physiol. 2020, 318, F1315–F1326. [Google Scholar] [CrossRef] [PubMed]
- Veerbeek, J.H.W.; Hermes, W.; Breimer, A.Y.; Van Rijn, B.B.; Koenen, S.V.; Mol, B.W.; Franx, A.; De Groot, C.J.; Koster, M.P. Cardiovascular disease risk factors after early-onset preeclampsia, late-onset preeclampsia, and pregnancy-induced hypertension. Hypertension 2015, 65, 600–606. [Google Scholar] [CrossRef] [Green Version]
- Bovee, E.M.; Gulati, M.; Maas, A.H. Novel Cardiovascular Biomarkers Associated with Increased Cardiovascular Risk in Women with Prior Preeclampsia/HELLP Syndrome: A Narrative Review. Eur. Cardiol. 2021, 16, e36. [Google Scholar] [CrossRef] [PubMed]
- Goulopoulou, S.; Davidge, S.T. Molecular mechanisms of maternal vascular dysfunction in preeclampsia. Trends Mol. Med. 2015, 21, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, I.A.; Jaleel, A.; Tamimi, W.; Al Kadri, H.M.F. Role of oxidative stress in the pathogenesis of preeclampsia. Arch. Gynecol. Obstet. 2010, 282, 469–474. [Google Scholar] [CrossRef]
- Aouache, R.; Biquard, L.; Vaiman, D.; Miralles, F. Oxidative Stress in Preeclampsia and Placental Diseases. Int. J. Mol. Sci. 2018, 19, 1496. [Google Scholar] [CrossRef] [Green Version]
- Khaliq, O.P.; Konoshita, T.; Moodley, J.; Naicker, T. The Role of Uric Acid in Preeclampsia: Is Uric Acid a Causative Factor or a Sign of Preeclampsia? Curr. Hypertens. Rep. 2018, 20, 80. [Google Scholar] [CrossRef]
- Ryu, A.; Cho, N.J.; Kim, Y.S.; Lee, E.Y. Predictive value of serum uric acid levels for adverse perinatal outcomes in preeclampsia. Medicine 2019, 98, e15462. [Google Scholar] [CrossRef]
- Pertegal, M.; Fenoy, F.J.; Bonacasa, B.; Mendiola, J.; Delgado, J.L.; Hernández, M.; Salom, M.G.; Bosch, V.; Hernández, I. 2-methoxyestradiol plasma levels are associated with clinical severity indices and biomarkers of preeclampsia. Reprod. Sci. 2015, 22, 198–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corominas, A.I.; Medina, Y.; Balconi, S.; Casale, R.; Farina, M.; Martínez, N.; Damiano, A.E. Assessing the Role of Uric Acid as a Predictor of Preeclampsia. Front. Physiol. 2022, 12, 785219. [Google Scholar] [CrossRef]
- Kara, A.E.; Guney, G.; Tokmak, A.; Ozaksit, G. The role of inflammatory markers hs-CRP, sialic acid, and IL-6 in the pathogenesis of preeclampsia and intrauterine growth restriction. Eur. Cytokine Netw. 2019, 30, 29–33. [Google Scholar] [PubMed]
- Ma, Y.; Ye, Y.; Zhang, J.; Ruan, C.C.; Gao, P.J. Immune imbalance is associated with the development of preeclampsia. Medicine 2019, 98, e15080. [Google Scholar] [CrossRef]
- Szarka, A.; Rigó, J.; Lázár, L.; Beko, G.; Molvarec, A. Circulating cytokines, chemokines and adhesion molecules in normal pregnancy and preeclampsia determined by multiplex suspension array. BMC Immunol. 2010, 11, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dekker, G.A.; Van Geijn, H.P. Endothelial dysfunction in preeclampsia. Part II: Reducing the adverse consequences of endothelial cell dysfunction in preeclampsia; Therapeutic perspectives. J. Perinat. Med. 1996, 24, 119–139. [Google Scholar] [CrossRef] [PubMed]
- Dekker, G.A.; de Vries, J.I.P.; Doelitzsch, P.M.; Huijgens, P.C.; von Blomberg, B.M.E.; Jakobs, C.; Van Geijn, H.P. Underlying disorders associated with severe early-onset preeclampsia. Am. J. Obstet. Gynecol. 1995, 173, 1042–1048. [Google Scholar] [CrossRef]
- Dai, C.; Fei, Y.; Li, J.; Shi, Y.; Yang, X. A Novel Review of Homocysteine and Pregnancy Complications. Biomed. Res. Int. 2021, 2021, 6652231. [Google Scholar] [CrossRef]
- Makedos, G.; Papanicolaou, A.; Hitoglou, A.; Kalogiannidis, I.; Makedos, A.; Vrazioti, V.; Goutzioulis, M. Homocysteine, folic acid and B12 serum levels in pregnancy complicated with preeclampsia. Arch. Gynecol. Obstet. 2007, 275, 121–124. [Google Scholar] [CrossRef]
- Baksu, A.; Taskin, M.; Goker, N.; Baksu, B.; Uluocak, A. Plasma homocysteine in late pregnancies complicated with preeclampsia and in newborns. Am. J. Perinatol. 2006, 23, 31–35. [Google Scholar] [CrossRef]
- Pertegal, M.; Fenoy, F.J.; Hernández, M.; Mendiola, J.; Delgado, J.L.; Bonacasa, B.; Corno, A.; López, B.; Bosch, V.; Hernández, I. Fetal Val108/158Met catechol-O-methyltransferase (COMT) polymorphism and placental COMT activity are associated with the development of preeclampsia. Fertil. Steril. 2016, 105, 134–143.e3. [Google Scholar] [CrossRef] [Green Version]
- Mao, D.; Che, J.; Li, K.; Han, S.; Yue, Q.; Zhu, L.; Zhang, W.; Li, L. Association of homocysteine, asymmetric dimethylarginine, and nitric oxide with preeclampsia. Arch. Gynecol. Obstet. 2010, 282, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Dymara-Konopka, W.; Laskowska, M. The Role of Nitric Oxide, ADMA, and Homocysteine in The Etiopathogenesis of Preeclampsia-Review. Int. J. Mol. Sci. 2019, 20, 2757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holden, D.P.; Fickling, S.A.; Whitley, G.S.; Nussey, S.S. Plasma concentrations of asymmetric dimethylarginine, a natural inhibitor of nitric oxide synthase, in normal pregnancy and preeclampsia. Am. J. Obstet. Gynecol. 1998, 178, 551–556. [Google Scholar] [CrossRef]
- Laskowska, M.; Laskowska, K.; Oleszczuk, J. PP135. Maternal serum levels of endothelial nitric oxide synthase and ADMA, an endogenous ENOS inhibitor in pregnancies complicated by severe preeclampsia. Pregnancy Hypertens. 2012, 2, 312. [Google Scholar] [CrossRef]
- Lõpez-Alarcõn, M.; Montalvo-Velarde, I.; Vital-Reyes, V.S.; Hinojosa-Cruz, J.C.; Leaños-Miranda, A.; Martínez-Basila, A. Serial determinations of asymmetric dimethylarginine and homocysteine during pregnancy to predict pre-eclampsia: A longitudinal study. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 1586–1592. [Google Scholar] [CrossRef] [Green Version]
- Khosla, K.; Heimberger, S.; Nieman, K.M.; Tung, A.; Shahul, S.; Staff, A.C.; Rana, S. Long-Term Cardiovascular Disease Risk in Women after Hypertensive Disorders of Pregnancy: Recent Advances in Hypertension. Hypertension 2021, 78, 927–935. [Google Scholar] [CrossRef]
- Rana, S.; Lemoine, E.; Granger, J.; Karumanchi, S.A. Preeclampsia: Pathophysiology, Challenges, and Perspectives. Circ. Res. 2019, 124, 1094–1112. [Google Scholar] [CrossRef]
- Perry, H.; Khalil, A.; Thilaganathan, B. Preeclampsia and the cardiovascular system: An update. Trends Cardiovasc. Med. 2018, 28, 505–513. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Low Risk | High Risk | p Value |
|---|---|---|---|
| (n = 57) | (n = 68) | ||
| Age, years | 32.6 ± 5.7 | 32.8 ± 6.4 | 0.76 |
| Weight, kg | 73.5 (67.5–79.2) | 76.25 (70–84.9) | 0.152 |
| Height, cm | 163 (160–166.5) | 160 (157–164.5) | 0.044 |
| Body mass index, kg/m2 | 28.1 ± 3.2 | 30.1 ± 4.7 | 0.016 |
| Caucasian | 57 (100) | 66 (97.1) | 0.294 |
| Cigarette smoker | 10 (17.5) | 5 (7.4) | 0.071 |
| Nulliparous, | 29 (50.9) | 47 (69.1) | 0.029 |
| Family history of PE | 1 (1.8) | 8 (11.8) | 0.031 |
| Medical History | |||
| Lupus | 1 (1.8) | 0 | 0.456 |
| AAS | 1 (1.8) | 1 (1.5) | 0.706 |
| Diabetes mellitus | 0 | 1 (1.5) | 0.544 |
| Hypertension | 0 | 2 (2.9) | 0.294 |
| Obstetric History | |||
| In vitro fertilization | 6 (10.5) | 12 (17.6) | 0.192 |
| Gestational age, weeks | 35.1 (35–35.4) | 35.4 (35.3–35.7) | |
| MAP, mm Hg | 86.3 (79.1–89.9) | 95.5 (91.0–100.2) | p < 0.0001 |
| UtA-PI | 0.68 (0.6–0.81) | 0.69 (0.6–0.86) | 0.392 |
| UtA-PI (MoM) | 0.95 (0.83–1.13) | 0.99 (0.85–1.16) | 0.319 |
| Gestational diabetes | 1 (1.8) | 8 (11.8) | 0.031 |
| Risk of PE | 292 (102–876) | 9 (6–15) | p < 0.0001 |
| Pregnancy Outcomes | |||
| Labor | |||
| Spontaneous | 40 (70.2) | 30 (44.1) | 0.004 |
| Induced | 12 (21.1) | 34 (50) | 0.001 |
| No labor | 5 (8.7) | 4 (5.9) | 0.535 |
| Mode of delivery | |||
| Vaginal | 37 (64.9) | 30 (44.1) | 0.021 |
| Cesarean | 12 (21.1) | 21 (30.9) | 0.216 |
| Instrumental | 8 (14) | 17 (25) | 0.128 |
| GA at delivery (w) | 39.9 (39.3–40.6) | 39.8 (39.1–40.4) | 0.517 |
| Birth weight (g) | 3360 (3052–3577) | 3218 (2929–3537) | 0.311 |
| PE | 0 | 7 (10.3) | |
| PI | 0 | 7 (10.3) | |
| Laboratory Parameters | Low Risk PE | High Risk No PE | High Risk PE |
|---|---|---|---|
| (n = 57) | (n = 61) | (n = 7) | |
| Dyslipidemia | median (IQR) | median (IQR) | median (IQR) |
| Cholesterol, (mg/dL) | 248.7 (217.5–280.5) | 245 (205–276) | 253 (211–266) |
| Triglyicerides (mg/dL) | 246 (189.5–292) | 258 (226–303) | 248 (137–263) |
| HDL (mg/dL) | 76 (63.5–82.5) | 68 (58–78) | 59 (45–74) |
| LDL (mg/dL) | 127 (102–151) | 121 (90.5–147.25) | 124 (119–159) |
| Apo B (mg/dL) | 133 (115–153) | 126 (110–155) | 137 (118–161) |
| Apo A-I (mg/dL) | 224 (205–246.5) | 218 (203–232) | 200 (158–226) ꭊ |
| ApoB/Apo A-I ratio | 0.61 (0.52–0.69) | 0.58 (0.50–0.71) | 0.78 (0.58–0.89) ꭊ |
| Lp A (mg/dL) | 13.5 (4.7–27.45) | 13 (7.6–32.2) | 17.1 (4.8–31.3) |
| Angiogenic | |||
| PlGF (pg/mL) | 354.7 (165.5–546.3) | 88.6 (56.3–130.7) * | 122.6 (77.74–489.9) |
| PlGF MoM | 1.05 (0.60–1.73) | 0.32 (0.23–0.56) * | 0.45 (0.33–1.11) |
| sFlt-1 (pg/mL) | 2090 (1489–2689) | 5027 (3723–6452) * | 4902 (1972–7259) |
| sFlt-1 (MoM) | 1.03 (0.71–1.36) | 2.10 (1.72–2.84) * | 2.06 (1.02–5.33) |
| sFlt-1/PLGF | 5.6 (3.6–14) | 58.1 (35.8–87.3) * | 23.5 (3.9–134.3) |
| Other Parameters | |||
| Proteinuria (mg/dL) | 10 (7.0–11.7) | 10 (8–14) | 93.5 (17.5–225) ꭊ |
| Platelets (×1000/mm3) | 217 (180–217) | 199 (163–249) | 249 (186–279) |
| Creatinin mg/dL | 0.52(0.45–0.56) | 0.5 (0.45–0.64) | 0.59 (0.42–0.95) |
| Coeff B | Std. Err | Coeff b | t | Sig. | |
|---|---|---|---|---|---|
| (Const.) | 74.312 | 4.229 | 17.571 | 0.000 | |
| AU | 2.066 | 0.705 | 0.254 | 2.929 | 0.004 |
| IL-6 | 1.114 | 0.365 | 0.265 | 3.052 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santoyo, J.M.; Noguera, J.A.; Avilés, F.; Delgado, J.L.; de Paco-Matallana, C.; Pérez, V.; Hernández, I. Factors Involved in Endothelial Dysfunction Related to Angiogenic Disbalance and Oxidative Stress, in Women at High Risk of Term Pre-Eclampsia. Antioxidants 2022, 11, 1409. https://doi.org/10.3390/antiox11071409
Santoyo JM, Noguera JA, Avilés F, Delgado JL, de Paco-Matallana C, Pérez V, Hernández I. Factors Involved in Endothelial Dysfunction Related to Angiogenic Disbalance and Oxidative Stress, in Women at High Risk of Term Pre-Eclampsia. Antioxidants. 2022; 11(7):1409. https://doi.org/10.3390/antiox11071409
Chicago/Turabian StyleSantoyo, Jean Michell, José Antonio Noguera, Francisco Avilés, Juan Luis Delgado, Catalina de Paco-Matallana, Virginia Pérez, and Isabel Hernández. 2022. "Factors Involved in Endothelial Dysfunction Related to Angiogenic Disbalance and Oxidative Stress, in Women at High Risk of Term Pre-Eclampsia" Antioxidants 11, no. 7: 1409. https://doi.org/10.3390/antiox11071409
APA StyleSantoyo, J. M., Noguera, J. A., Avilés, F., Delgado, J. L., de Paco-Matallana, C., Pérez, V., & Hernández, I. (2022). Factors Involved in Endothelial Dysfunction Related to Angiogenic Disbalance and Oxidative Stress, in Women at High Risk of Term Pre-Eclampsia. Antioxidants, 11(7), 1409. https://doi.org/10.3390/antiox11071409