
Myeloperoxidase and Advanced Oxidation Protein Products in the Cerebrospinal Fluid in Women and Men with Parkinson’s Disease

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Information
2.3. Biofluid Collection, ELISA Analysis and Albumin Index
2.4. Statistics and Ethics
3. Results
3.1. Demographic and Clinical Parameters
3.2. Myeloperoxidase and Advanced Oxidation Protein Products in the CSF and Serum
3.2.1. Cohort of Patients and Controls’
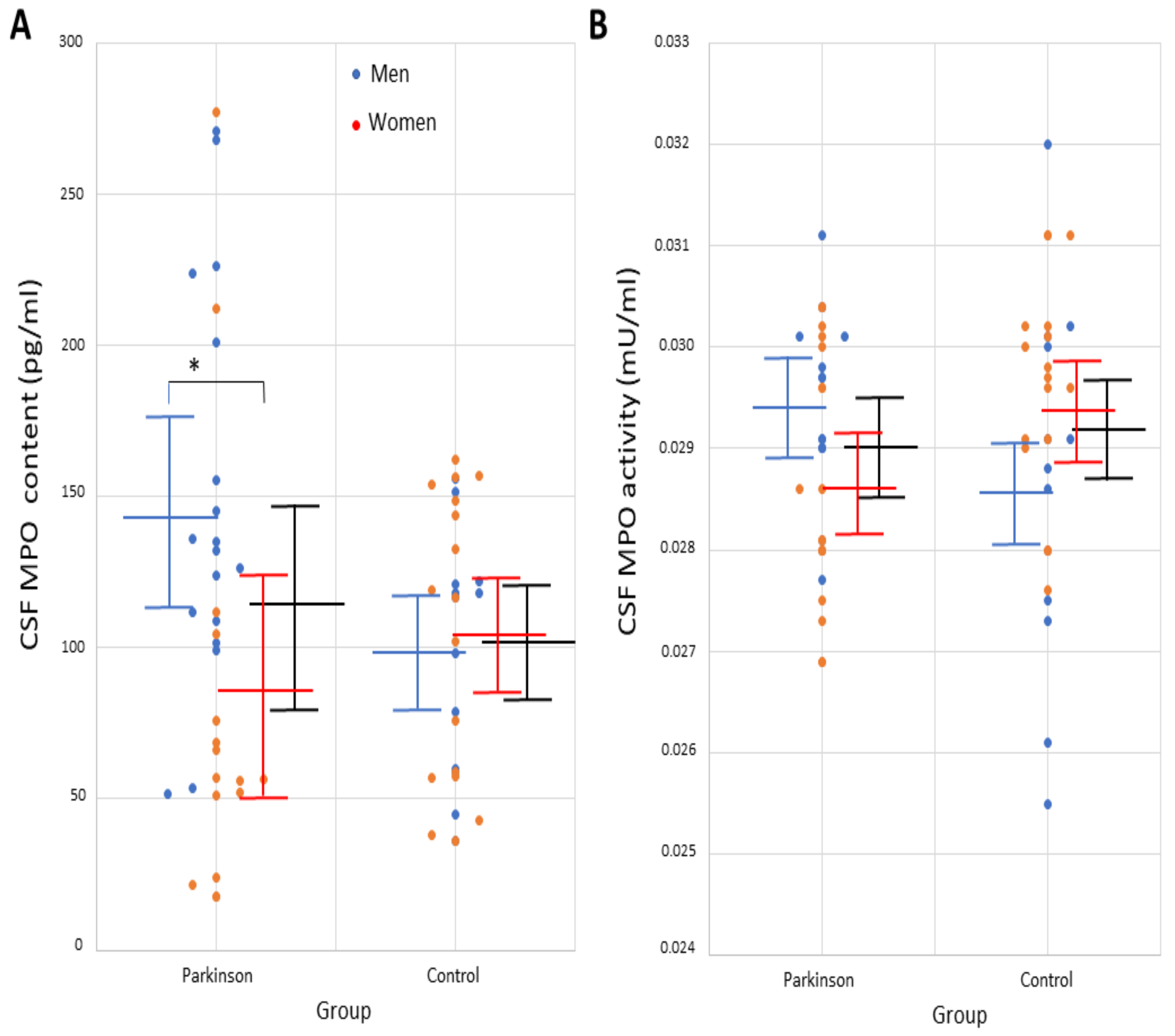
3.2.2. Study of Sex-Based Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harrison, J.E.; Schultz, J. Studies on the chlorinating activity of myeloperoxidase. J. Biol. Chem. 1976, 251, 1371–1374. [Google Scholar] [CrossRef]
- Dunford, H.B. Myeloperoxidase and eosinophil peroxidase: Phagocytosis and microbial killing. In Heme Peroxidases; Dunford, H.B., Ed.; Wiley: New York, NY, USA, 1999; pp. 349–385. [Google Scholar]
- Bafort, F.; Parisi, O.; Perraudin, J.P.; Jijakli, M.H. Mode of action of lactoperoxidase as related to its antimicrobial activity: A review. Enzym. Res. 2014, 2014, 517164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, M.J.; Hawkins, C.L.; Pattison, D.I.; Rees, M.D. Mammalian heme peroxidases: From molecular mechanisms to health implications. Antioxid. Redox Signal. 2008, 10, 1199–1234. [Google Scholar] [CrossRef] [PubMed]
- Vlasova, I.I. Peroxidase Activity of Human Hemoproteins: Keeping the Fire under Control. Molecules 2018, 23, 2561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galzigna, L.; de Iuliis, A.; Zanatta, L. Enzymatic dopamine peroxidation in substantia nigra of human brain. Clin. Chim. Acta 2000, 300, 131–138. [Google Scholar] [CrossRef]
- De Iuliis, A.; Burlina, A.P.; Boschetto, R.; Zambenedetti, P.; Arslan, P.; Galzigna, L. Increased dopamine peroxidation in postmortem Parkinsonian brain. Biochim. Biophys. Acta 2002, 1573, 63–67. [Google Scholar] [CrossRef]
- Everse, J.; Coates, P.W. The cytotoxic activity of lactoperoxidase: Enhancement and inhibition by neuroactive compounds. Free Radic. Biol. Med. 2004, 37, 839–849. [Google Scholar] [CrossRef]
- Everse, J.; Coates, P.W. Neurodegeneration and peroxidases. Neurobiol. Aging 2009, 30, 1011–1025. [Google Scholar] [CrossRef]
- Choi, D.K.; Pennathur, S.; Perier, C.; Tieu, K.; Teismann, P.; Wu, D.C.; Jackson-Lewis, V.; Vila, M.; Vonsattel, J.P.; Heinecke, J.W.; et al. Ablation of the inflammatory enzyme myeloperoxidase mitigates features of Parkinson’s disease in mice. J. Neurosci. 2005, 25, 6594–6600. [Google Scholar] [CrossRef]
- Everse, J.; Liu, C.J.; Coates, P.W. Physical and catalytic properties of a peroxidase derived from cytochrome C. Biochim. Biophys. Acta 2011, 1812, 1138–1145. [Google Scholar] [CrossRef]
- Teismann, P. Myeloperoxidase in the neurodegenerative process of Parkinson’s disease. Dtsch. Med. Wochenschr. 2014, 139, 99–102. [Google Scholar] [PubMed]
- García-Moreno, J.M.; de Pablos, A.M.; García-Sánchez, M.I.; Méndez-Lucena, C.; Damas-Hermoso, F.; Rus, M.; Chacón, J.; Fernández, E. May serum levels of advanced oxidized protein products serve as a prognostic marker of disease duration in patients with idiopathic Parkinson’s disease? Antioxid. Redox Signal. 2013, 18, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Espejo, E.; Bis-Humbert, C. Excess amounts of 3-iodo-l-tyrosine induce Parkinson-like features in experimental approaches of Parkinsonism. Neurotoxicology 2018, 67, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Everse, J.; Coates, P.W. Role of peroxidases in Parkinson disease: A hypothesis. Free Radic. Biol. Med. 2005, 38, 1296–1310. [Google Scholar] [CrossRef] [PubMed]
- Hazen, S.L.; D’Avignon, A.; Anderson, M.M.; Hsu, F.F.; Heinecke, J.W. Human neutrophils employ the myeloperoxidase-hydrogen peroxide-chloride system to oxidize alpha-amino acids to a family of reactive aldehydes. Mechanistic studies identifying labile intermediates along the reaction pathway. J. Biol. Chem. 1998, 273, 4997–5005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnhold, J.; Flemmig, J. Human myeloperoxidase in innate and acquired immunity. Arch. Biochem. Biophys. 2010, 500, 92–106. [Google Scholar] [CrossRef]
- Klebanoff, S.J.; Kettle, A.J.; Rosen, H.; Winterbourn, C.C.; Nauseef, W.M. Myeloperoxidase: A front-line defender against phagocytosed microorganisms. J. Leukoc. Biol. 2013, 93, 185–198. [Google Scholar] [CrossRef] [Green Version]
- Yap, Y.W.; Whiteman, M.; Cheung, N.S. Chlorinative stress: An under-appreciated mediator of neurodegeneration? Cell Signal. 2007, 19, 219–228. [Google Scholar] [CrossRef]
- Ray, R.S.; Katyal, A. Myeloperoxidase: Bridging the gap in neurodegeneration. Neurosci. Biobehav. Rev. 2016, 68, 611–620. [Google Scholar] [CrossRef]
- Jeitner, T.M.; Kalogiannis, M.; Krasnikov, B.F.; Gomlin, I.; Peltier, M.R.; Moran, G.R. Linking Inflammation and Parkinson Disease: Hypochlorous Acid Generates Parkinsonian Poisons. Toxicol. Sci. 2016, 151, 388–402. [Google Scholar] [CrossRef] [Green Version]
- Maki, R.A.; Holzer, M.; Motamedchaboki, K.; Malle, E.; Masliah, E.; Marsche, G.; Reynolds, W.F. Human myeloperoxidase (hMPO) is expressed in neurons in the substantia nigra in Parkinson’s disease and in the hMPO-α-synuclein-A53T mouse model, correlating with increased nitration and aggregation of α-synuclein and exacerbation of motor impairment. Free Radic. Biol. Med. 2019, 141, 115–140. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.C.; Kim, S.R.; Jin, B.K. Paroxetine prevents loss of nigrostriatal dopaminergic neurons by inhibiting brain inflammation and oxidative stress in an experimental model of Parkinson’s disease. J. Immunol. 2010, 185, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, E.C.; Hunot, S. Neuroinflammation in Parkinson’s disease: A target for neuroprotection? Lancet Neurol. 2009, 8, 382–397. [Google Scholar] [CrossRef]
- Soubhye, J.; Aldib, I.; Delporte, C.; Prévost, M.; Dufrasne, F.; Antwerpen, P.V. Myeloperoxidase as a Target for the Treatment of Inflammatory Syndromes: Mechanisms and Structure Activity Relationships of Inhibitors. Curr. Med. Chem. 2016, 23, 3975–4008. [Google Scholar] [CrossRef]
- Huh, S.H.; Chung, Y.C.; Piao, Y.; Jin, M.Y.; Son, H.J.; Yoon, N.S.; Hong, J.Y.; Pak, Y.K.; Kim, Y.S.; Hong, J.K.; et al. Ethyl pyruvate rescues nigrostriatal dopaminergic neurons by regulating glial activation in a mouse model of Parkinson’s disease. J. Immunol. 2011, 187, 960–969. [Google Scholar] [CrossRef] [Green Version]
- Santos-Galindo, M.; Acaz-Fonseca, E.; Bellini, M.J.; Garcia-Segura, L.M. Sex differences in the inflammatory response of primary astrocytes to lipopolysaccharide. Biol. Sex Differ. 2011, 2, 7. [Google Scholar] [CrossRef] [Green Version]
- Siani, F.; Greco, R.; Levandis, G.; Ghezzi, C.; Daviddi, F.; Demartini, C.; Vegeto, E.; Fuzzati-Armentero, M.T.; Blandini, F. Influence of Estrogen Modulation on Glia Activation in a Murine Model of Parkinson’s Disease. Front. Neurosci. 2017, 11, 306. [Google Scholar] [CrossRef] [Green Version]
- Cerri, S.; Mus, L.; Blandini, F. Parkinson’s Disease in Women and Men: What’s the Difference? J. Parkinsons Dis. 2019, 9, 501–515. [Google Scholar] [CrossRef] [Green Version]
- Kabutomori, O.; Yanagihara, T.; Iwatani, Y.; Kawarazaki, A.; Kabutomori, M. Sex difference in myeloperoxidase activity of neutrophils. Am. J. Hematol. 1999, 60, 312–313. [Google Scholar] [CrossRef]
- Nikulshin, S.; Tolstikova, I.; Bartule, A.; Kviluna, D.; Gravele, D.; Gardovska, D. Intracellular neutrophil myeloperoxidase level in pediatric patients: Significant age and gender variability. Int. J. Lab. Hematol. 2015, 37, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Witko-Sarsat, V.; Gausson, V.; Descamps-Latscha, B. Are advanced oxidation protein products potential uremic toxins? Kidney Int. Suppl. 2003, 84, S11–S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capeillère-Blandin, C.; Gausson, V.; Nguyen, A.T.; Descamps-Latscha, B.; Drüeke, T.; Witko-Sarsat, V. Respective role of uraemic toxins and myeloperoxidase in the uraemic state. Nephrol. Dial. Transplant. 2006, 21, 1555–1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Espejo, E. Is there a halo-enzymopathy in Parkinson’s disease? Neurologia 2019. [Google Scholar] [CrossRef]
- Miletić, J.; Drakulić, D.; Pejić, S.; Petković, M.; Ilić, T.V.; Miljković, M.; Stefanović, A.; Prostran, M.; Stojanov, M. Prooxidant-antioxidant balance, advanced oxidation protein products and lipid peroxidation in Serbian patients with Parkinson’s disease. Int. J. Neurosci. 2018, 128, 600–607. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, M.S.; Schumacher-Schuh, A.; Cardoso, A.M.; Bochi, G.V.; Baldissarelli, J.; Kegler, A.; Santana, D.; Chaves, C.M.; Schetinger, M.R.; Moresco, R.N.; et al. Iron and Oxidative Stress in Parkinson’s Disease: An Observational Study of Injury Biomarkers. PLoS ONE 2016, 11, e0146129. [Google Scholar] [CrossRef] [Green Version]
- Malle, E.; Furtmüller, P.G.; Sattler, W.; Obinger, C. Myeloperoxidase: A target for new drug development? Br. J. Pharmacol. 2007, 152, 838–854. [Google Scholar] [CrossRef] [Green Version]
- Jucaite, A.; Svenningsson, P.; Rinne, J.O.; Cselényi, Z.; Varnäs, K.; Johnström, P.; Amini, N.; Kirjavainen, A.; Helin, S.; Minkwitz, M.; et al. Effect of the myeloperoxidase inhibitor AZD3241 on microglia: A PET study in Parkinson’s disease. Brain 2015, 138 Pt 9, 2687–2700. [Google Scholar] [CrossRef] [Green Version]
- Gellhaar, S.; Sunnemark, D.; Eriksson, H.; Olson, L.; Galter, D. Myeloperoxidase-immunoreactive cells are significantly increased in brain areas affected by neurodegeneration in Parkinson’s and Alzheimer’s disease. Cell Tissue Res. 2017, 369, 445–454. [Google Scholar] [CrossRef]
- Mollenhauer, B.; Trautmann, E.; Otte, B.; Ng, J.; Spreer, A.; Lange, P.; Sixel-Döring, F.; Hakimi, M.; Vonsattel, J.P.; Nussbaum, R.; et al. α-Synuclein in human cerebrospinal fluid is principally derived from neurons of the central nervous system. J. Neural Transm. 2012, 119, 739–746. [Google Scholar] [CrossRef] [Green Version]
- Goldman, J.G.; Andrews, H.; Amara, A.; Naito, A.; Alcalay, R.N.; Shaw, L.M.; Taylor, P.; Xie, T.; Tuite, P.; Henchcliffe, C.; et al. Cerebrospinal fluid, plasma, and saliva in the BioFIND study: Relationships among biomarkers and Parkinson’s disease Features. Mov. Disord. 2018, 33, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Kang, U.J.; Goldman, J.G.; Alcalay, R.N.; Xie, T.; Tuite, P.; Henchcliffe, C.; Hogarth, P.; Amara, A.W.; Frank, S.; Rudolph, A.; et al. The BioFIND study: Characteristics of a clinically typical Parkinson’s disease biomarker cohort. Mov. Disord. 2016, 31, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Niñerola-Baizán, A.; Gallego, J.; Cot, A.; Aguiar, P.; Lomeña, F.; Pavía, J.; Ros, D. Optimization of the reconstruction parameters in [(123)I]FP-CIT SPECT. Phys. Med. Biol. 2018, 63, 085009. [Google Scholar] [CrossRef] [PubMed]
- Chahine, L.M.; Iranzo, A.; Fernández-Arcos, A.; Simuni, T.; Seedorff, N.; Caspell-Garcia, C.; Amara, A.W.; Comella, C.; Högl, B.; Hamilton, J.; et al. PPMI Sleep Working Group, Basic clinical features do not predict dopamine transporter binding in idiopathic REM behavior disorder. NPJ Parkinsons Dis. 2019, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Espejo, E.; Rodriguez de Fonseca, F.; Suárez, J.; Martín de Pablos, Á. Cerebrospinal fluid lactoperoxidase level is enhanced in idiopathic Parkinson’s disease, and correlates with levodopa equivalent daily dose. Brain Res. 2021, 1761, 147411. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Ferreira, J.J.; Lees, A.; Rocha, J.F.; Poewe, W.; Rascol, O.; Soares-da-Silva, P. Bi-Park 1 investigators. Opicapone as an adjunct to levodopa in patients with Parkinson’s disease and end-of-dose motor fluctuations: A randomised, double-blind, controlled trial. Lancet Neurol. 2016, 15, 154–165. [Google Scholar] [CrossRef]
- Verber, D.; Novak, D.; Borovič, M.; Dugonik, J.; Flisar, D. EQUIDopa: A responsive web application for the levodopa equivalent dose calculator. Comput. Methods Programs Biomed. 2020, 196, 105633. [Google Scholar] [CrossRef]
- Martin-de-Pablos, A.; Córdoba-Fernández, A.; Fernández-Espejo, E. Analysis of neurotrophic and antioxidant factors related to midbrain dopamine neuronal loss and brain inflammation in the cerebrospinal fluid of the elderly. Exp. Gerontol. 2018, 110, 54–60. [Google Scholar] [CrossRef]
- Martín de Pablos, A.; García-Moreno, J.M.; Fernández, E. Does the Cerebrospinal Fluid Reflect Altered Redox State But Not Neurotrophic Support Loss in Parkinson’s Disease? Antioxid. Redox Signal. 2015, 23, 893–898. [Google Scholar] [CrossRef]
- Hernán, M.A.; Takkouche, B.; Caamaño-Isorna, F.; Gestal-Otero, J.J. A meta-analysis of coffee drinking, cigarette smoking, and the risk of Parkinson’s disease. Ann. Neurol. 2002, 52, 276–284. [Google Scholar] [CrossRef]
- O’Keefe, J.H.; Bhatti, S.K.; Patil, H.R.; DiNicolantonio, J.J.; Lucan, S.C.; Lavie, C.J. Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-cause mortality. J. Am. Coll. Cardiol. 2013, 62, 1043–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ragonese, P.; Salemi, G.; Morgante, L.; Aridon, P.; Epifanio, A.; Buffa, D.; Scoppa, F.; Savettieri, G. A case-control study on cigarette, alcohol, and coffee consumption preceding Parkinson’s disease. Neuroepidemiology 2003, 22, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Jeitner, T.M.; Kalogiannis, M.; Patrick, P.A.; Gomolin, I.; Palaia, T.; Ragolia, L.; Brand, D.; Delikatny, E.J. Inflaming the diseased brain: A role for tainted melanins. Biochim. Biophys. Acta 2015, 1852, 937–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahodwala, N.; Shah, K.; He, Y.; Wu, S.S.; Schmidt, P.; Cubillos, F.; Willis, A.W. Sex disparities in access to caregiving in Parkinson disease. Neurology 2018, 90, e48–e54. [Google Scholar] [CrossRef]
- Balzer-Geldsetzer, M.; Klotsche, J.; Dodel, R.; Riedel, O.; Landscape Consortium. Quality of life in a German cohort of Parkinson’s patients assessed with three different measures. J. Neurol. 2018, 265, 2713–2722. [Google Scholar] [CrossRef] [Green Version]
- Hanamsagar, R.; Alter, M.D.; Block, C.S.; Sullivan, H.; Bolton, J.L.; Bilbo, S.D. Generation of a microglial developmental index in mice and in humans reveals a sex difference in maturation and immune reactivity. Glia 2017, 65, 1504–1520. [Google Scholar] [CrossRef]
- Fernández-Espejo, E. Enhanced serum myeloperoxidase level correlates with clinical features of Parkinson’s disease. An. R. Acad. Nac. Med. 2022, 139, 44–54. Available online: https://analesranm.es/wp-content/uploads/2022/numero_139_01/pdfs/ar13901-org01.pdf (accessed on 10 May 2022). [CrossRef]
- Hampton, M.B.; Kettle, A.J.; Winterbourn, C.C. Inside the neutrophil phagosome: Oxidants, myeloperoxidase, and bacterial killing. Blood 1998, 92, 3007–3017. [Google Scholar] [CrossRef]
- Pullar, J.M.; Winterbourn, C.C.; Vissers, M.C. Loss of GSH and thiol enzymes in endothelial cells exposed to sublethal concentrations of hypochlorous acid. Am. J. Physiol. 1999, 277, H1505–H1512. [Google Scholar] [CrossRef]
- Kalousová, M.; Skrha, J.; Zima, T. Advanced glycation end-products and advanced oxidation protein products in patients with diabetes mellitus. Physiol. Res. 2002, 51, 597–604. Available online: http://www.biomed.cas.cz/physiolres/pdf/51/51_597.pdf (accessed on 15 June 2020).
- Witko-Sarsat, V.; Friedlander, M.; Capeillère-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int. 1996, 49, 1304–1313. Available online: https://www.kidney-international.org/article/S0085-253859480-5/pdf (accessed on 11 March 2018). [CrossRef] [PubMed] [Green Version]
- Xiao, L.L.; Zhang, F.; Zhao, Y.L.; Zhang, L.J.; Xie, Z.Y.; Huang, K.Z.; Ouyang, X.X.; Wu, X.X.; Xu, X.W.; Li, L.J. Using advanced oxidation protein products and ischaemia-modified albumin to monitor oxidative stress levels in patients with drug-induced liver injury. Sci. Rep. 2020, 10, 18128. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | PD (n = 34) | Control (n = 30) | p |
|---|---|---|---|
| Age, years | 65 ± 12 | 57.4 ± 14 | NS |
| Gender, male n(%) | 18 (60) | 13(45) | NS |
| Body mass index, kg/m2 | 23.2 ± 3 | 24.6 ± 3 | NS |
| Education, years | 17.3 ± 1.6 | 17.4 ± 3.5 | NS |
| Albumin index | 6.9 ± 1.9 | 6.6 ± 1.6 | NS |
| Leukocyte count, cells/µL | 3.1 ± 0.7 | 2.7 ± 0.6 | NS |
| CSF MPO content, pg/mL | 114 ± 73 | 101 ± 43 | NS |
| CSF MPO activity, mU/mL | 0.0290 ± 0.001 | 0.0292 ± 0.001 | NS |
| Serum MPO content, pg/mL | 3770 ± 2871 | 1430 ± 683 | <0.0001 |
| Serum MPO activity, mU/mL | 44.1 ± 6 | 35.1 ± 7 | <0.0001 |
| CSF AOPP content, µM | 23.4 ± 29 (n = 16) | nd | |
| Serum AOPP content, µM | 535 ± 349 | nd | |
| Levodopa equivalent daily dose, mg | 686.2 ± 532 | ||
| Disease duration, years | 12.1 ± 7.8 | ||
| Age at PD onset, years | 51.2 ± 14 | ||
| Modified Hoehn–Yahr stage | 2.1 ± 0.7 | ||
| Modified Schwab–England | 77.8 ± 24 | ||
| MDS-UPDRS part III (on) | 25.6 ± 15 | ||
| Total MDS-UPDRS (I-III) (on) | 37.9 ± 26 | ||
| MDS-UPDRS part IV (all patients) | 1.2 ± 2.2 |
| MPO Content | MPO Activity | |||
|---|---|---|---|---|
| Parameter | Correlation, r | p | Correlation, r | p |
| Age, years | 0.298 | NS | −0.022 | NS |
| Body mass index | 0.102 | NS | −0.021 | NS |
| Education, years | 0.091 | NS | 0.076 | NS |
| Albumin index | 0.024 | NS | −0.129 | NS |
| Leukocyte count, cells/µL | 0.123 | NS | 0.202 | NS |
| Serum MPO concentration (pg/mL) | −0.091 | NS | −0.079 | NS |
| Serum MPO activity (mU/mL) | −0.121 | NS | 0.385 | NS |
| CSF MPO activity | 0.471 | 0.0049 | ||
| Levodopa equivalent daily dose, mg | 0.037 | NS | 0.244 | NS |
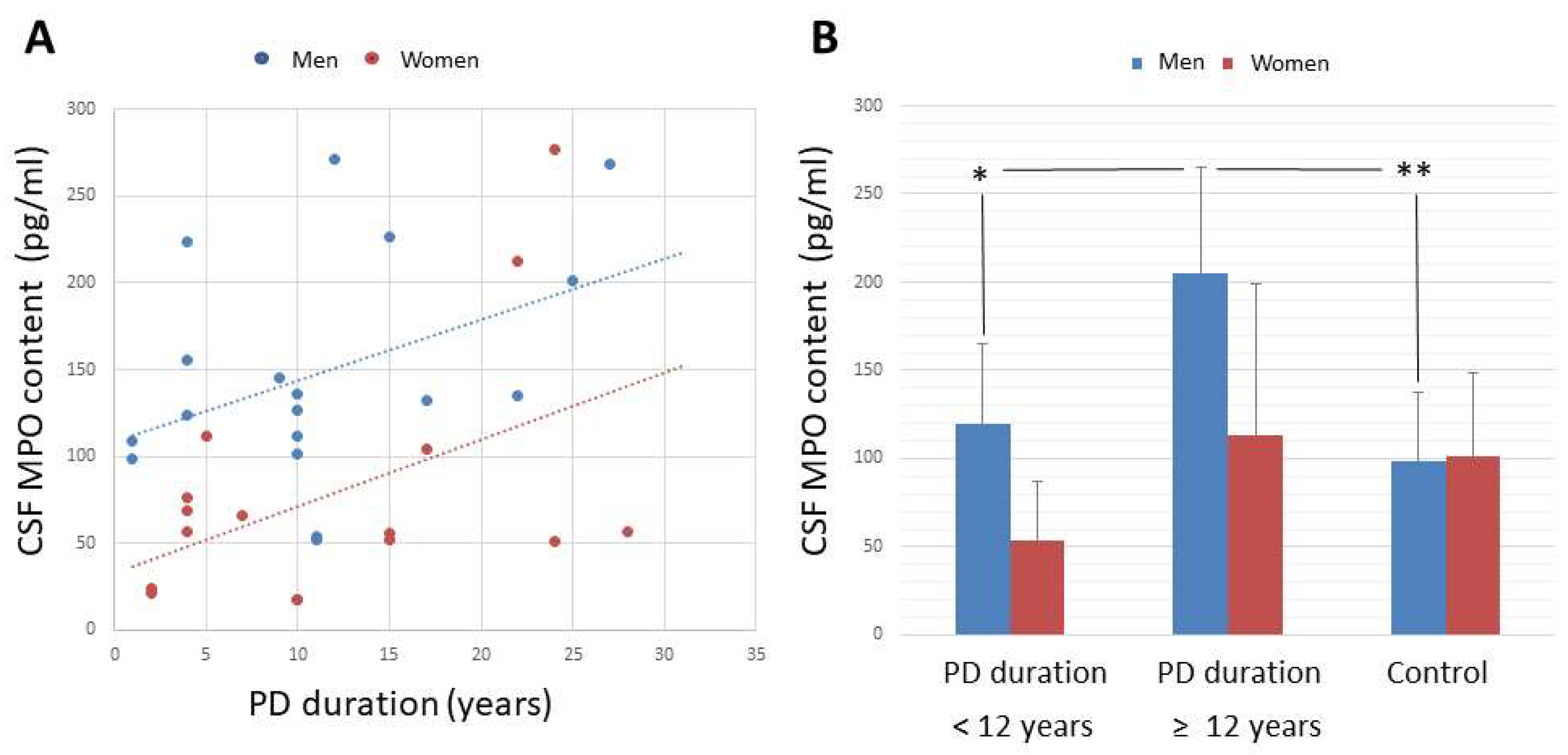
| Disease duration, years | 0.475 | 0.0045 | 0.070 | NS |
| Age-at-PD onset, years | −0.156 | NS | 0.034 | NS |
| Hoehn–Yahr stage | −0.121 | NS | 0.128 | NS |
| Modified Schwab–England | −0.175 | NS | 0.028 | NS |
| MDS-UPDRS part III (on) | −0.059 | NS | 0.045 | NS |
| Total MDS-UPDRS (I-III) (on) | 0.010 | NS | −0.096 | NS |
| MDS-UPDRS part IV (all patients) | 0.044 | NS | 0.093 | NS |
| Parameters | PD | Control | ||
|---|---|---|---|---|
| Men (n = 18) | Women (n = 16) | Men (n = 13) | Women (n = 17) | |
| Age, years | 63.2 ± 10 | 62.1 ± 12 | 56.9 ± 15 | 584 ± 12 |
| Body mass index, kg/m2 | 23.1 ± 7 | 23.3 ± 3 | 24.4 ± 5 | 24.9 ± 3 |
| Education, years | 17.3 ± 1.3 | 17.4 ± 1.7 | 17.5 ± 4 | 17.3 ± 3 |
| Albumin index | 6.8 ± 1.6 | 7.0 ± 2 | 6.7 ± 1.5 | 6.5 ± 1.8 |
| Leukocyte count, cells/µL | 3.1 ± 0.6 | 3.2 ± 0.8 | 2.8 ± 0.5 | 2.6 ± 0.7 |
| CSF MPO content, pg/mL | 148 ± 63 * | 81 ± 71 | 99 ± 41 | 103 ± 47 |
| CSF MPO activity, mU/mL | 0.0294 ± 0.001 | 0.0287 ± 0.001 | 0.0286 ± 0.001 | 0.0294 ± 0.001 |
| Serum MPO content, pg/mL | 3890 ± 3100 * | 3690 ± 1695 ** | 1242 ± 727 | 1650 ± 608 |
| Serum MPO activity, mU/mL | 44.3 ± 3 ** | 43.7 ± 4 ** | 35.1 ± 6 | 35 ± 6 |
| CSF AOPP content, µM | 16.7 ± 23 (n = 6) | 9.9 ± 19 (n = 10) | nd | nd |
| Serum AOPP content, µM | 588 ± 311 | 455 ± 391 | nd | nd |
| Levodopa equivalent daily dose, mg | 714 ± 664 | 650 ± 432 | ||
| Disease duration, years | 11 ± 8 | 12 ± 8 | ||
| Age at PD onset, years | 51.4 ± 13 | 53.7 ± 15 | ||
| Modified Hoehn–Yahr stage | 2.2 ± 0.7 | 2.1 ± 0.8 | ||
| Modified Schwab–England | 76.5 ± 23 | 68.8 ± 27 | ||
| MDS-UPDRS part III (on) | 29.4 ± 14 | 23.8 ± 17 | ||
| Total MDS-UPDRS (I-III) (on) | 44 ± 26 | 37.2 ± 30 | ||
| MDS-UPDRS part IV (all patients) | 1.4 ± 2.5 | 1.5 ± 2.2 | ||
| MPO Content | MPO Activity | |||
|---|---|---|---|---|
| Parameter | Men (n = 18) | Women (n = 16) | Men (n = 18) | Women (n = 16) |
| Age, years | 0.158 | 0.405 | −0.022 | −0.023 |
| Body mass index | 0.101 | 0.087 | −0.024 | −0.025 |
| Education, years | 0.275 | −0.364 | 0.159 | −0.306 |
| Albumin index | 0.021 | 0.028 | −0.149 | −0.103 |
| Leukocyte count, cells/µL | 0.101 | 0.204 | 0.212 | 0.186 |
| CSF MPO activity | 0.470 * | 0.498 * | ||
| Serum MPO content | −0.387 | 0.216 | −0.174 | −0.109 |
| Serum MPO activity | 0.128 | 0.326 | 0.314 | −0.273 |
| Levodopa equivalent daily dose, mg | 0.016 | 0.076 | 0.230 | 0.331 |
| Disease duration, years | 0.469 * | 0.565 * | 0.404 | −0.276 |
| Age-at-PD onset, years | −0.135 | −0.024 | −0.256 | 0.329 |
| Hoehn–Yahr stage | −0.048 | −0.236 | 0.343 | 0.104 |
| Modified Schwab–England | −0.018 | −0.401 | 0.010 | −0.006 |
| MDS-UPDRS part III (on) | −0.019 | −0.307 | 0.324 | 0.013 |
| Total MDS-UPDRS (I-III) (on) | −0.017 | −0.183 | 0.292 | −0.120 |
| MDS-UPDRS part IV (all patients) | 0.216 | −0.012 | 0.320 | −0.080 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Espejo, E.; Rodríguez de Fonseca, F.; Gavito, A.L.; Córdoba-Fernández, A.; Chacón, J.; Martín de Pablos, Á. Myeloperoxidase and Advanced Oxidation Protein Products in the Cerebrospinal Fluid in Women and Men with Parkinson’s Disease. Antioxidants 2022, 11, 1088. https://doi.org/10.3390/antiox11061088
Fernández-Espejo E, Rodríguez de Fonseca F, Gavito AL, Córdoba-Fernández A, Chacón J, Martín de Pablos Á. Myeloperoxidase and Advanced Oxidation Protein Products in the Cerebrospinal Fluid in Women and Men with Parkinson’s Disease. Antioxidants. 2022; 11(6):1088. https://doi.org/10.3390/antiox11061088
Chicago/Turabian StyleFernández-Espejo, Emilio, Fernando Rodríguez de Fonseca, Ana Luisa Gavito, Antonio Córdoba-Fernández, José Chacón, and Ángel Martín de Pablos. 2022. "Myeloperoxidase and Advanced Oxidation Protein Products in the Cerebrospinal Fluid in Women and Men with Parkinson’s Disease" Antioxidants 11, no. 6: 1088. https://doi.org/10.3390/antiox11061088
APA StyleFernández-Espejo, E., Rodríguez de Fonseca, F., Gavito, A. L., Córdoba-Fernández, A., Chacón, J., & Martín de Pablos, Á. (2022). Myeloperoxidase and Advanced Oxidation Protein Products in the Cerebrospinal Fluid in Women and Men with Parkinson’s Disease. Antioxidants, 11(6), 1088. https://doi.org/10.3390/antiox11061088