
Kinetics of Biomarkers of Oxidative Stress in Septic Shock: A Pilot Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval of the Study Protocol
2.2. Patient Recruitment
2.3. Sample Collection
2.4. Laboratory Methods
2.5. Statistical Analysis
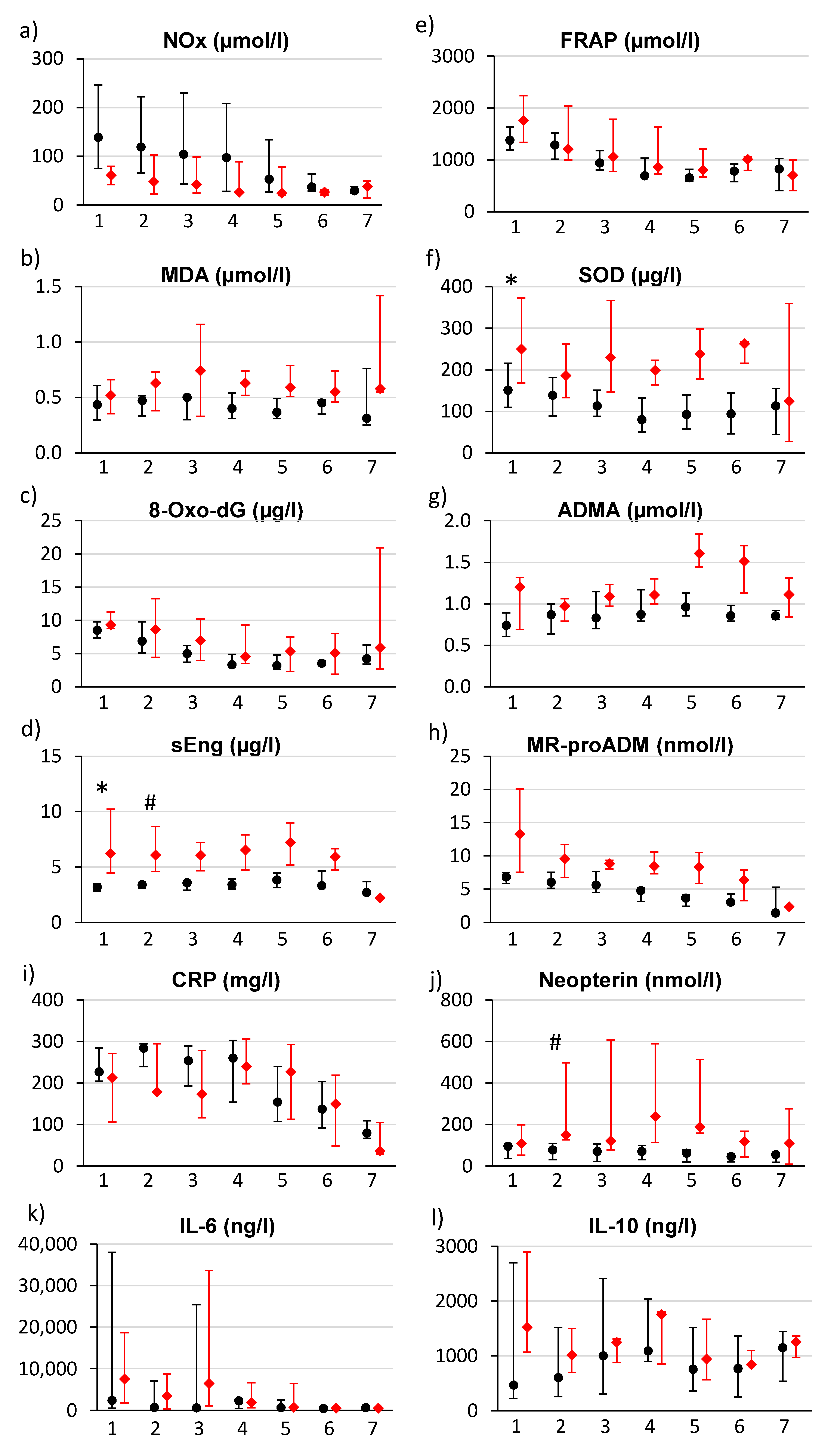
3. Results
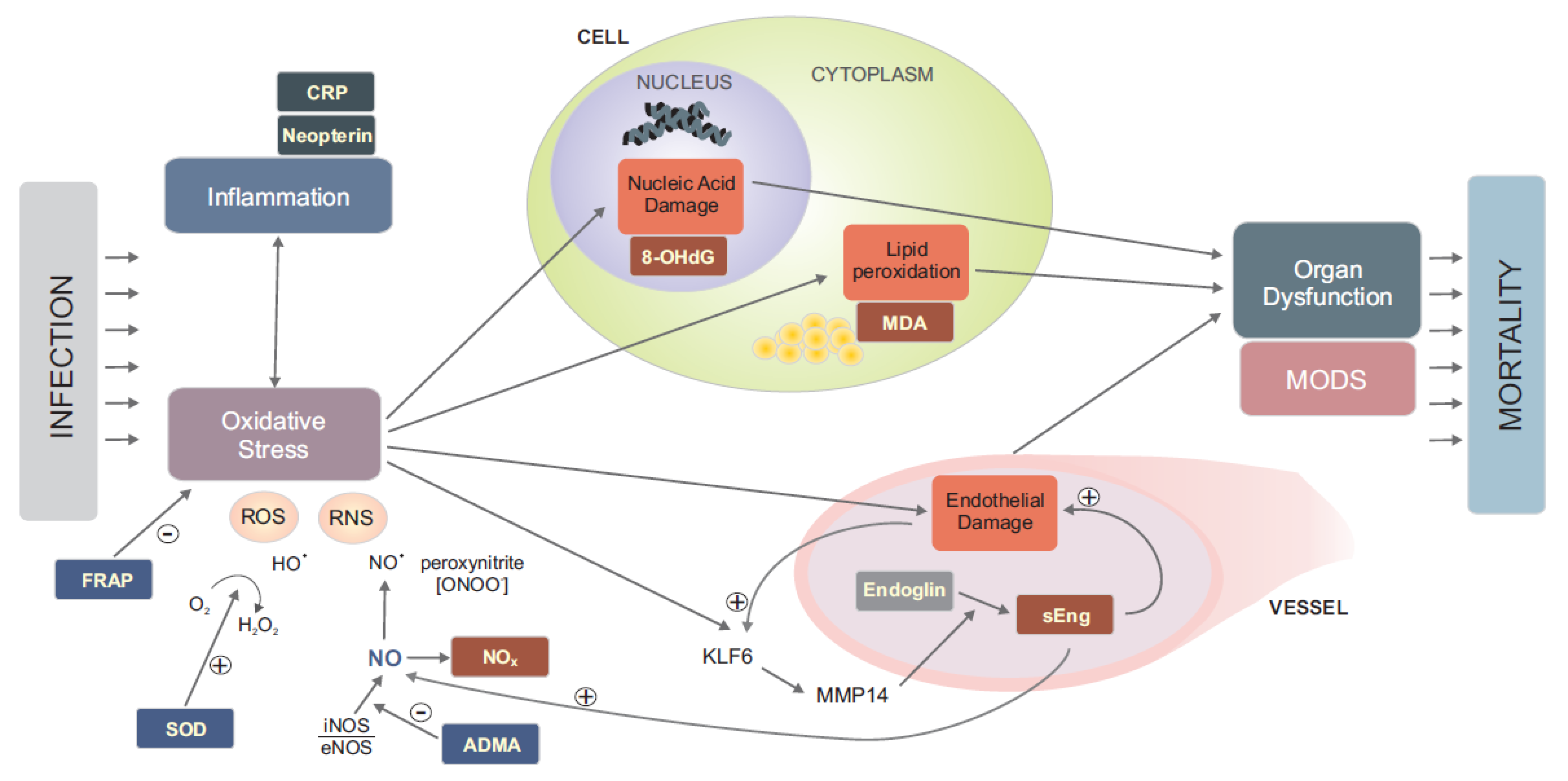
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Mantzarlis, K.; Tsolaki, V.; Zakynthinos, E. Role of Oxidative Stress and Mitochondrial Dysfunction in Sepsis and Potential Therapies. Oxid. Med. Cell. Longev. 2017, 2017, 5985209. [Google Scholar] [CrossRef] [PubMed]
- Prauchner, C.A. Oxidative Stress in Sepsis: Pathophysiological Implications Justifying Antioxidant Co-Therapy. Burns 2017, 43, 471–485. [Google Scholar] [CrossRef] [PubMed]
- Parenica, J.; Kala, P.; Mebazaa, A.; Littnerova, S.; Benesova, K.; Tomandl, J.; Goldbergová Pavkova, M.; Jarkovský, J.; Spinar, J.; Tomandlova, M.; et al. Activation of the Nitric Oxide Pathway and Acute Myocardial Infarction Complicated by Acute Kidney Injury. Cardiorenal Med. 2020, 10, 85–96. [Google Scholar] [CrossRef]
- Tomandlova, M.; Parenica, J.; Lokaj, P.; Ondrus, T.; Kala, P.; Miklikova, M.; Helanova, K.; Helan, M.; Malaska, J.; Benesova, K.; et al. Prognostic Value of Oxidative Stress in Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Prospective Cohort Study. Free Radic. Biol. Med. 2021, 174, 66–72. [Google Scholar] [CrossRef]
- Frijhoff, J.; Winyard, P.G.; Zarkovic, N.; Davies, S.S.; Stocker, R.; Cheng, D.; Knight, A.R.; Taylor, E.L.; Oettrich, J.; Ruskovska, T.; et al. Clinical Relevance of Biomarkers of Oxidative Stress. Antioxid. Redox Signal. 2015, 23, 1144–1170. [Google Scholar] [CrossRef] [Green Version]
- Ayala, J.C.; Grismaldo, A.; Sequeda-Castañeda, L.G.; Aristizábal-Pachón, A.F.; Morales, L. Oxidative Stress in ICU Patients: ROS as Mortality Long-Term Predictor. Antioxidants 2021, 10, 1912. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Khoschsorur, G.A.; Winklhofer-Roob, B.M.; Rabl, H.; Auer, T.; Peng, Z.; Schaur, R.J. Evaluation of a Sensitive HPLC Method for the Determination of Malondialdehyde, and Application of the Method to Different Biological Materials. Chromatographia 2000, 52, 181–184. [Google Scholar] [CrossRef]
- Suzuki, S.; Shishido, T.; Ishino, M.; Katoh, S.; Sasaki, T.; Nishiyama, S.; Miyashita, T.; Miyamoto, T.; Nitobe, J.; Watanabe, T.; et al. 8-Hydroxy-2’-Deoxyguanosine Is a Prognostic Mediator for Cardiac Event. Eur. J. Clin. Investig. 2011, 41, 759–766. [Google Scholar] [CrossRef]
- Benzie, I.F.; Strain, J.J. The Ferric Reducing Ability of Plasma (FRAP) as a Measure of “Antioxidant Power”: The FRAP Assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gieseg, S.P.; Baxter-Parker, G.; Lindsay, A. Neopterin, Inflammation, and Oxidative Stress: What Could We Be Missing? Antioxidants 2018, 7, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murr, C.; Widner, B.; Wirleitner, B.; Fuchs, D. Neopterin as a Marker for Immune System Activation. Curr. Drug Metab. 2002, 3, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Annane, D.; Sanquer, S.; Sébille, V.; Faye, A.; Djuranovic, D.; Raphaël, J.C.; Gajdos, P.; Bellissant, E. Compartmentalised Inducible Nitric-Oxide Synthase Activity in Septic Shock. Lancet 2000, 355, 1143–1148. [Google Scholar] [CrossRef]
- Martin, G.; Asensi, V.; Montes, A.H.; Collazos, J.; Alvarez, V.; Pérez-Is, L.; Carton, J.A.; Taboada, F.; Valle-Garay, E. Endothelial (NOS3 E298D) and Inducible (NOS2 Exon 22) Nitric Oxide Synthase Polymorphisms, as Well as Plasma NOx, Influence Sepsis Development. Nitric Oxide Biol. Chem. 2014, 42, 79–86. [Google Scholar] [CrossRef]
- Ho, J.T.; Chapman, M.J.; O’Connor, S.; Lam, S.; Edwards, J.; Ludbrook, G.; Lewis, J.G.; Torpy, D.J. Characteristics of Plasma NOx Levels in Severe Sepsis: High Interindividual Variability and Correlation with Illness Severity, but Lack of Correlation with Cortisol Levels. Clin. Endocrinol. 2010, 73, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Lupp, C.; Baasner, S.; Ince, C.; Nocken, F.; Stover, J.F.; Westphal, M. Differentiated control of deranged nitric oxide metabolism: A therapeutic option in sepsis? Crit. Care. 2013, 17, 311. [Google Scholar] [CrossRef] [Green Version]
- Opal, S.M.; van der Poll, T. Endothelial Barrier Dysfunction in Septic Shock. J. Intern. Med. 2015, 277, 277–293. [Google Scholar] [CrossRef] [Green Version]
- La Sala, L.; Pujadas, G.; De Nigris, V.; Canivell, S.; Novials, A.; Genovese, S.; Ceriello, A. Oscillating Glucose and Constant High Glucose Induce Endoglin Expression in Endothelial Cells: The Role of Oxidative Stress. Acta Diabetol. 2015, 52, 505–512. [Google Scholar] [CrossRef]
- Jezkova, K.; Rathouska, J.; Nemeckova, I.; Fikrova, P.; Dolezelova, E.; Varejckova, M.; Vitverova, B.; Tysonova, K.; Serwadczak, A.; Buczek, E.; et al. High Levels of Soluble Endoglin Induce a Proinflammatory and Oxidative-Stress Phenotype Associated with Preserved NO-Dependent Vasodilatation in Aortas from Mice Fed a High-Fat Diet. J. Vasc. Res. 2016, 53, 149–162. [Google Scholar] [CrossRef]
- Jerkic, M.; Letarte, M. Contribution of Oxidative Stress to Endothelial Dysfunction in Hereditary Hemorrhagic Telangiectasia. Front. Genet. 2015, 6, 34. [Google Scholar] [CrossRef] [Green Version]
- Aristorena, M.; Blanco, F.J.; de Las Casas-Engel, M.; Ojeda-Fernandez, L.; Gallardo-Vara, E.; Corbi, A.; Botella, L.M.; Bernabeu, C. Expression of Endoglin Isoforms in the Myeloid Lineage and Their Role during Aging and Macrophage Polarization. J. Cell Sci. 2014, 127, 2723–2735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Pan, C.C.; Bloodworth, J.C.; Nixon, A.B.; Theuer, C.; Hoyt, D.G.; Lee, N.Y. Antibody-Directed Coupling of Endoglin and MMP-14 Is a Key Mechanism for Endoglin Shedding and Deregulation of TGF-β Signaling. Oncogene 2014, 33, 3970–3979. [Google Scholar] [CrossRef] [PubMed]
- Ojeda-Fernández, L.; Recio-Poveda, L.; Aristorena, M.; Lastres, P.; Blanco, F.J.; Sanz-Rodríguez, F.; Gallardo-Vara, E.; de las Casas-Engel, M.; Corbí, Á.; Arthur, H.M.; et al. Mice Lacking Endoglin in Macrophages Show an Impaired Immune Response. PLoS Genet. 2016, 12, e1005935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemankova, L.; Varejckova, M.; Dolezalova, E.; Fikrova, P.; Jezkova, K.; Rathouska, J.; Cerveny, L.; Botella, L.M.; Bernabeu, C.; Nemeckova, I.; et al. Atorvastatin-Induced Endothelial Nitric Oxide Synthase Expression in Endothelial Cells Is Mediated by Endoglin. J. Physiol. Pharmacol. 2015, 66, 403–413. [Google Scholar] [PubMed]
- Carr, A.C.; Bozonet, S.; Pullar, J.; Spencer, E.; Rosengrave, P.; Shaw, G. Neutrophils Isolated from Septic Patients Exhibit Elevated Uptake of Vitamin C and Normal Intracellular Concentrations despite a Low Vitamin C Milieu. Antioxidants 2021, 10, 1607. [Google Scholar] [CrossRef]
- Kim, S.-M.; Kim, J.-Y.; Lee, S.; Park, J.-H. Adrenomedullin Protects against Hypoxia/Reoxygenation-Induced Cell Death by Suppression of Reactive Oxygen Species via Thiol Redox Systems. FEBS Lett. 2010, 584, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Yoshimoto, T.; Fukai, N.; Sato, R.; Sugiyama, T.; Ozawa, N.; Shichiri, M.; Hirata, Y. Antioxidant Effect of Adrenomedullin on Angiotensin II-Induced Reactive Oxygen Species Generation in Vascular Smooth Muscle Cells. Endocrinology 2004, 145, 3331–3337. [Google Scholar] [CrossRef]
- Vincent, J.L.; de Mendonça, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA Score to Assess the Incidence of Organ Dysfunction/Failure in Intensive Care Units: Results of a Multicenter, Prospective Study. Working Group on “Sepsis-Related Problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef]
- Moskowitz, A.; Andersen, L.W.; Cocchi, M.N.; Karlsson, M.; Patel, P.V.; Donnino, M.W. Thiamine as a Renal Protective Agent in Septic Shock. A Secondary Analysis of a Randomized, Double-Blind, Placebo-Controlled Trial. Ann. Am. Thorac. Soc. 2017, 14, 737–741. [Google Scholar] [CrossRef] [Green Version]
- Zabet, M.H.; Mohammadi, M.; Ramezani, M.; Khalili, H. Effect of High-Dose Ascorbic Acid on Vasopressor’s Requirement in Septic Shock. J. Res. Pharm. Pract. 2016, 5, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Chertoff, J. N-Acetylcysteine’s Role in Sepsis and Potential Benefit in Patients with Microcirculatory Derangements. J. Intensive Care Med. 2018, 33, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.; Zou, T.; Yang, X.; Zhang, Z.; Cao, P.; Han, J.; Duan, Y.; Ruan, B.-F.; Li, Q.-S. Discovery of Novel Pterostilbene Derivatives That Might Treat Sepsis by Attenuating Oxidative Stress and Inflammation through Modulation of MAPKs/NF-ΚB Signaling Pathways. Antioxidants 2021, 10, 1333. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Khangoora, V.; Rivera, R.; Hooper, M.H.; Catravas, J. Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study. Chest 2017, 151, 1229–1238. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 21) | Surviving (n = 12) | Deceased (n = 9) | p | |
|---|---|---|---|---|
| Basic characteristics | ||||
| Male | 15 (71.4%) | 8 (66.7%) | 7 (77.8%) | 0.659 |
| Female | 6 (28.6%) | 4 (33.3%) | 2 (22.2%) | 0.659 |
| Age (years) | 65 (26; 76) | 64 (33; 76) | 65 (26; 75) | 0.972 |
| BMI (kg/m2) | 29 (23; 51) | 30 (24; 51) | 29 (23; 36) | 0.602 |
| Systolic BP (mmHg) | 100 (40; 150) | 100 (40; 145) | 100 (70; 150) | 0.277 |
| Diastolic BP (mmHg) | 50 (30; 80) | 50 (30; 60) | 60 (50; 80) | 0.018 |
| Past medical history | ||||
| Smoking | 6 (28.6%) | 2 (16.7%) | 4 (44.4%) | 0.331 |
| Hypertension | 15 (71.4%) | 9 (75.0%) | 6 (66.7%) | 0.999 |
| Diabetes mellitus | 4 (19.0%) | 2 (16.7%) | 2 (22.2%) | 0.999 |
| Hyperlipoproteinaemia | 8 (38.1%) | 4 (33.3%) | 4 (44.4%) | 0.673 |
| Previous CAD | 2 (9.5%) | 1 (8.3%) | 1 (11.1%) | 0.999 |
| History of stroke/TIA | 3 (14.3%) | 2 (16.7%) | 1 (11.1%) | 0.999 |
| COPD | 2 (9.5%) | 0 (0.0%) | 2 (22.2%) | 0.171 |
| Atrial fibrillation | 3 (14.3%) | 2 (16.7%) | 1 (11.1%) | 0.999 |
| Medication at admission | ||||
| Antiplatelet drugs | 5 (23.8%) | 2 (16.7%) | 3 (33.3%) | 0.611 |
| Anticoagulants | 1 (4.8%) | 0 (0.0%) | 1 (11.1%) | 0.429 |
| ACE inhibitors | 2 (9.5%) | 0 (0.0%) | 2 (22.2%) | 0.171 |
| Beta-blockers | 7 (33.3%) | 5 (41.7%) | 2 (22.2%) | 0.642 |
| Statins | 4 (19.0%) | 2 (16.7%) | 2 (22.2%) | 0.999 |
| ARBs | 4 (19.0%) | 3 (25.0%) | 1 (11.1%) | 0.603 |
| Diuretics | 2 (9.5%) | 2 (16.7%) | 0 (0.0%) | 0.486 |
| Spironolactone | 2 (9.5%) | 2 (16.7%) | 0 (0.0%) | 0.486 |
| Ca-blockers | 2 (9.5%) | 1 (8.3%) | 1 (11.1%) | 0.999 |
| Oral antidiabetic drugs | 3 (14.3%) | 2 (16.7%) | 1 (11.1%) | 0.999 |
| Sepsis severity, organ dysfunction | ||||
| APACHE II | 28 (19; 42) | 28 (18; 37) | 30 (20; 46) | 0.465 |
| SOFA | 12 (7; 18) | 12 (10; 17) | 12 (7; 18) | 0.807 |
| Lactate (mmol/L) | 3.4 (0.9; 12.7) | 3.3 (0.9; 8.4) | 3.9 (1.3; 12.7) | 0.499 |
| Creatinin (µmol/L) | 153 (39; 570) | 146 (39; 391) | 196 (52; 570) | 0.508 |
| Trombocytes (109/L) | 131 (26; 231) | 112 (51; 231) | 150 (26; 190) | 0.761 |
| Source of sepsis | ||||
| Pneumonia | 8 (38.1%) | 4 (33.3%) | 4 (44.4%) | 0.673 |
| Abdominal infection | 7 (33.3%) | 6 (50.0%) | 1 (11.1%) | 0.159 |
| Urosepsis | 1 (4.8%) | 0 (0.0%) | 1 (11.1%) | 0.429 |
| CRBI | 1 (4.8%) | 0 (0.0%) | 1 (11.1%) | 0.429 |
| Meningitis | 2 (9.5%) | 1 (8.3%) | 1 (11.1%) | 1.000 |
| Multiple or unknown | 2 (9.5%) | 1 (8.3%) | 1 (11.1%) | 1.000 |
| Biomarker | Surviving (n = 12) | Deceased (n = 9) | p Value | Cut-off Value | AUC | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|
| NOx (µmol/L) | 139.0 (58.1; 267.0) | 61.0 (39.7; 161.5) | 0.073 | ≤80.5 | 0.810 | 0.833 | 0.714 |
| MDA (µmol/L) | 0.44 (0.26; 0.65) | 0.52 (0.33; 0.89) | 0.219 | ≥0.32 | 0.667 | 1.000 | 0.417 |
| 8-oxo-dG (µg/L) | 8.48 (5.63; 19.47) | 9.30 (8.06; 22.26) | 0.155 | ≥8.3 | 0.690 | 0.889 | 0.500 |
| sEng (µg/L) | 3.17 (2.70; 3.73) | 6.21 (3.95; 10.36) | 0.002 * | ≥3.63 | 0.976 | 1.000 | 0.857 |
| FRAP (µmol/L) | 1377 (925; 2130) | 1762 (923; 2601) | 0.422 | ≥2 211 | 0.611 | 0.333 | 1.000 |
| SOD (µg/L) | 150.5 (82.6; 364.9) | 249.9 (141.4; 939.0) | 0.039 * | ≥134.2 | 0.773 | 1.000 | 0.500 |
| ADMA (µmol/L) | 0.74 (0.42; 1.09) | 1.20 (0.62; 1.83) | 0.040 * | ≥1.16 | 0.769 | 0.556 | 1.000 |
| MR-proADM (nmol/L) | 6.82 (4.34; 21.45) | 17.06 (7.52; 24.72) | 0.240 | ≥7.50 | 0.722 | 0.833 | 0.833 |
| CRP (mg/L) | 227.1 (112.6; 316.4) | 212.4 (83.4; 327.6) | 0.553 | ≤138.9 | 0.583 | 0.444 | 0.917 |
| Neopterin (nmol/L) | 94.9 (12.5; 155.1) | 109.2 (33.5; 531.6) | 0.305 | ≥122.0 | 0.646 | 0.500 | 0.833 |
| IL-6 (ng/L) | 2445 (398; 191,782) | 7617 (837; 64,783) | 0.651 | ≥1616 | 0.567 | 0.889 | 0.500 |
| IL-10 (ng/L) | 467 (192; 7356) | 1520 (397; 75,390) | 0.111 | ≥645 | 0.713 | 0.889 | 0.667 |
| SOFA | 12.0 (9.6; 16.5) | 12.0 (7.8; 17.6) | 0.807 | ≤10.5 | 0.537 | 0.333 | 0.833 |
| Lactate (mmol/L) | 3.25 (0.90; 7.85) | 3.90 (1.50; 10.62) | 0.499 | ≥3.35 | 0.593 | 0.667 | 0.583 |
| Creatinin (µmol/L) | 146.0 (57.7; 352.5) | 196.0 (58.8; 476.4) | 0.508 | ≥182.0 | 0.593 | 0.556 | 0.750 |
| Trombocytes (109/L) | 112.0 (61.7; 229.5) | 150.0 (31.6; 292.1) | 0.761 | ≥114.0 | 0.500 | 0.750 | 0.545 |
| Biomarker | Surviving (n = 12) | Deceased (n = 9) | p | Cut-Off Value | AUC | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|
| NOx (µmol/L) | 119.0 (44.7; 237.4) | 48.0 (22.9; 148.0) | 0.138 | ≤57.5 | 0.762 | 0.667 | 0.857 |
| MDA (µmol/L) | 0.47 (0.29; 0.64) | 0.63 (0.35; 1.15) | 0.167 | ≥0.59 | 0.702 | 0.571 | 0.917 |
| 8-oxo-dG (µg/L) | 6.86 (3.87; 13.27) | 8.60 (4.27; 20.92) | 0.591 | ≥8.4 | 0.583 | 0.571 | 0.750 |
| sEng (µg/L) | 3.41 (3.08; 3.60) | 6.06 (3.83; 9.92) | 0.010 * | ≥4.10 | 0.958 | 0.833 | 1.000 |
| FRAP (µmol/L) | 1288 (822; 1649) | 1209 (667; 2118) | 0.866 | ≥1848 | 0.470 | 0.286 | 1.000 |
| SOD (µg/L) | 138.6 (72.0; 331.7) | 186.0 (128.1; 457.3) | 0.120 | ≥118.8 | 0.726 | 1.000 | 0.417 |
| ADMA (µmol/L) | 0.87 (0.57; 1.33) | 0.97 (0.78; 1.45) | 0.340 | ≥0.72 | 0.643 | 1.000 | 0.417 |
| MR-proADM (nmol/L) | 6.01 (4.46; 13.19) | 9.54 (4.02; 15.89) | 0.309 | ≥6.64 | 0.694 | 0.833 | 0.667 |
| CRP (mg/L) | 284.2 (176.2; 307.1) | 178.8 (133.8; 389.0) | 0.237 | ≤191.9 | 0.673 | 0.571 | 0.917 |
| Neopterin (nmol/L) | 77.7 (13.1; 114.6) | 151.0 (50.0; 541.3) | 0.013 * | ≥122.5 | 0.875 | 0.833 | 1.000 |
| IL-6 (ng/L) | 733(193; 79,268) | 3515 (342; 140,294) | 0.432 | ≥916 | 0.619 | 0.714 | 0.583 |
| IL-10 (ng/L) | 606 (114; 2556) | 1011 (326; 6938) | 0.64 | ≥521 | 0.571 | 0.857 | 0.500 |
| SOFA | 12.0 (8.0; 15.9) | 13.0 (6.4; 19.2) | 0.887 | ≥17.5 | 0.639 | 0.222 | 1.000 |
| Lactate (mmol/L) | 2.45 (0.90; 7.08) | 1.80 (1.49; 8.77) | 0.703 | ≥1.35 | 0.440 | 1.000 | 0.333 |
| Creatinin (µmol/L) | 136.0 (53.9; 327.6) | 213.0 (76.6; 475.8) | 0.261 | ≥205.5 | 0.667 | 0.714 | 0.833 |
| Trombocytes (109/L) | 92.6 (44.1; 231.6) | 105.0 (23.2; 213.9) | 0.965 | ≤54.0 | 0.488 | 0.375 | 0.900 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helan, M.; Malaska, J.; Tomandl, J.; Jarkovsky, J.; Helanova, K.; Benesova, K.; Sitina, M.; Dastych, M.; Ondrus, T.; Pavkova Goldbergova, M.; et al. Kinetics of Biomarkers of Oxidative Stress in Septic Shock: A Pilot Study. Antioxidants 2022, 11, 640. https://doi.org/10.3390/antiox11040640
Helan M, Malaska J, Tomandl J, Jarkovsky J, Helanova K, Benesova K, Sitina M, Dastych M, Ondrus T, Pavkova Goldbergova M, et al. Kinetics of Biomarkers of Oxidative Stress in Septic Shock: A Pilot Study. Antioxidants. 2022; 11(4):640. https://doi.org/10.3390/antiox11040640
Chicago/Turabian StyleHelan, Martin, Jan Malaska, Josef Tomandl, Jiri Jarkovsky, Katerina Helanova, Klara Benesova, Michal Sitina, Milan Dastych, Tomas Ondrus, Monika Pavkova Goldbergova, and et al. 2022. "Kinetics of Biomarkers of Oxidative Stress in Septic Shock: A Pilot Study" Antioxidants 11, no. 4: 640. https://doi.org/10.3390/antiox11040640
APA StyleHelan, M., Malaska, J., Tomandl, J., Jarkovsky, J., Helanova, K., Benesova, K., Sitina, M., Dastych, M., Ondrus, T., Pavkova Goldbergova, M., Gal, R., Lokaj, P., Tomandlova, M., & Parenica, J. (2022). Kinetics of Biomarkers of Oxidative Stress in Septic Shock: A Pilot Study. Antioxidants, 11(4), 640. https://doi.org/10.3390/antiox11040640