
Assessment of Lipid Peroxidation in Alzheimer’s Disease Differential Diagnosis and Prognosis


Abstract
:
1. Introduction
2. Materials and Methods
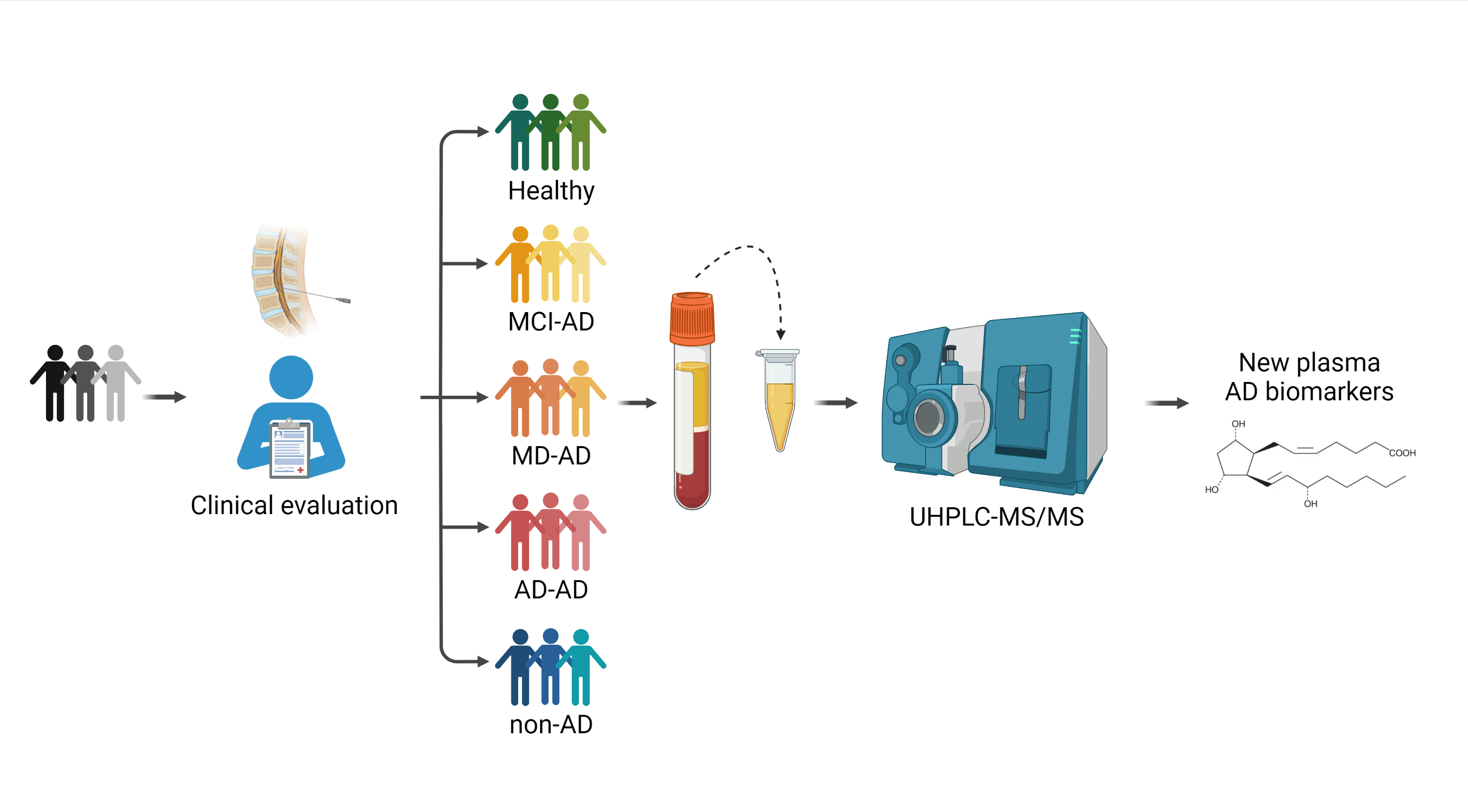
2.1. Participants
2.2. Lipid Peroxidation Compounds Determination and Samples Analysis
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Lipid Peroxidation Compounds
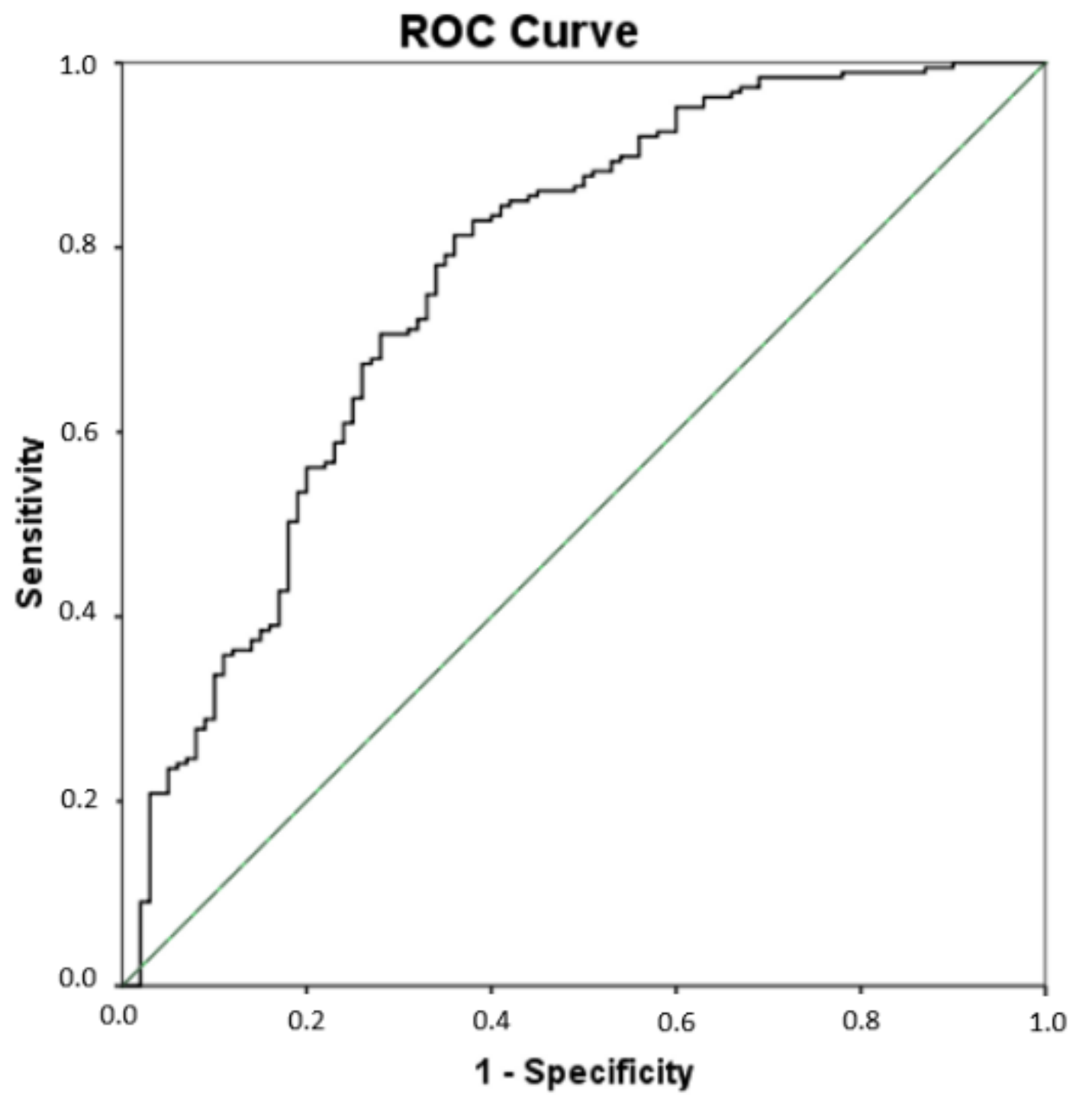
3.3. Multivariate Analysis
3.4. Alzheimer’s Disease Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Durmugier, J.; Sabia, S. Epidemiology of Alzheimer’s disease: Latest trends. Rev. Prat. 2020, 70, 149–151. [Google Scholar]
- World Health Organization. Global Action Plan on the Public Health Response to Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 13 October 2021).
- Guzman-Martinez, L.; Maccioni, R.B.; Farías, G.A.; Fuentes, P.; Navarrete, L.P. Biomarkers for Alzheimer’s Disease. Curr. Alzheimer Res. 2019, 16, 518–528. [Google Scholar] [CrossRef] [Green Version]
- Weller, J.; Budson, A. Current understanding of Alzheimer’s disease diagnosis and treatment. F1000Research 2018, 7, 1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultana, R.; Perluigi, M.; Butterfield, D.A. Lipid peroxidation triggers neurodegeneration: A redox proteomics view into the Alzheimer disease brain. Free Radic. Biol. Med. 2013, 62, 157–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, E.; Morel, A.; Saso, L.; Saluk, J. Isoprostanes and Neuroprostanes as Biomarkers of Oxidative Stress in Neurodegenerative Diseases. Oxid. Med. Cell. Longev. 2014, 2014, 572491. [Google Scholar] [CrossRef]
- Reich, E.E.; Markesbery, W.R.; Roberts, L.J.; Swift, L.L.; Morrow, J.D.; Montine, T.J. Brain Regional Quantification of F-Ring and D-/E-Ring Isoprostanes and Neuroprostanes in Alzheimer’s Disease. Am. J. Pathol. 2001, 158, 293–297. [Google Scholar] [CrossRef]
- Sidorova, Y.; Domanskyi, A. Detecting Oxidative Stress Biomarkers in Neurodegenerative Disease Models and Patients. Methods Protoc. 2020, 3, 66. [Google Scholar] [CrossRef]
- Rojas-Gutierrez, E.; Muñoz-Arenas, G.; Treviño, S.; Espinosa, B.; Chavez, R.; Rojas, K.; Flores, G.; Díaz, A.; Guevara, J. Alzheimer’s disease and metabolic syndrome: A link from oxidative stress and inflammation to neurodegeneration. Synapse 2017, 71, e21990. [Google Scholar] [CrossRef]
- Tramutola, A.; Lanzillotta, C.; Perluigi, M.; Butterfield, D.A. Oxidative stress, protein modification and Alzheimer disease. Brain Res. Bull. 2017, 133, 88–96. [Google Scholar] [CrossRef]
- Umeno, A.; Biju, V.; Yoshida, Y. In vivo ROS production and use of oxidative stress-derived biomarkers to detect the onset of diseases such as Alzheimer’s disease, Parkinson’s disease, and diabetes. Free Radic. Res. 2017, 51, 413–427. [Google Scholar] [CrossRef]
- Gaschler, M.M.; Stockwell, B.R. Lipid peroxidation in cell death. Biochem. Biophys. Res. Commun. 2017, 482, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Angelova, P.R.; Esteras, N.; Abramov, A.Y. Mitochondria and lipid peroxidation in the mechanism of neurodegeneration: Finding ways for prevention. Med. Res. Rev. 2021, 41, 770–784. [Google Scholar] [CrossRef] [PubMed]
- Peña-Bautista, C.; Álvarez, L.; Durand, T.; Vigor, C.; Cuevas, A.; Baquero, M.; Vento, M.; Hervás, D.; Cháfer-Pericás, C. Clinical Utility of Plasma Lipid Peroxidation Biomarkers in Alzheimer’s Disease Differential Diagnosis. Antioxidants 2020, 9, 649. [Google Scholar] [CrossRef]
- Shichiri, M. The role of lipid peroxidation in neurological disorders. J. Clin. Biochem. Nutr. 2014, 54, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Czerska, M.; Zieliński, M.; Gromadzińska, J. Isoprostanes—A novel major group of oxidative stress markers. Int. J. Occup. Med. Environ. Health 2015, 29, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Kao, Y.-C.; Ho, P.-C.; Tu, Y.-K.; Jou, I.-M.; Tsai, K.-J. Lipids and Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 1505. [Google Scholar] [CrossRef] [PubMed]
- Bradley-Whitman, M.A.; Lovell, M.A. Biomarkers of lipid peroxidation in Alzheimer disease (AD): An update. Arch. Toxicol. 2015, 89, 1035–1044. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.; Zhukareva, V.; Sung, S.; Clark, C.M.; Rokach, J.; Lee, V.M.-Y.; Trojanowski, J.Q.; Pratico, D. Enhanced brain levels of 8,12-iso-iPF2 -VI differentiate AD from frontotemporal dementia. Neurology 2003, 61, 475–478. [Google Scholar] [CrossRef]
- Ashton, N.J.; Hye, A.; Rajkumar, A.P.; Leuzy, A.; Snowden, S.; Suárez-Calvet, M.; Karikari, T.K.; Schöll, M.; La Joie, R.; Rabinovici, G.D.; et al. An update on blood-based biomarkers for non-Alzheimer neurodegenerative disorders. Nat. Rev. Neurol. 2020, 16, 265–284. [Google Scholar] [CrossRef]
- Kim, W.S.; Jary, E.; Pickford, R.; He, Y.; Ahmed, R.M.; Piguet, O.; Hodges, J.R.; Halliday, G.M. Lipidomics Analysis of Behavioral Variant Frontotemporal Dementia: A Scope for Biomarker Development. Front. Neurol. 2018, 9, 104. [Google Scholar] [CrossRef] [Green Version]
- Phan, K.; He, Y.; Pickford, R.; Bhatia, S.; Katzeff, J.S.; Hodges, J.R.; Piguet, O.; Halliday, G.M.; Kim, W.S. Uncovering pathophysiological changes in frontotemporal dementia using serum lipids. Sci. Rep. 2020, 10, 3640. [Google Scholar] [CrossRef]
- Nasaruddin, M.L.; Pan, X.; McGuinness, B.; Passmore, P.; Kehoe, P.G.; Hölscher, C.; Graham, S.F.; Green, B.D. Evidence That Parietal Lobe Fatty Acids May Be More Profoundly Affected in Moderate Alzheimer’s Disease (AD) Pathology Than in Severe AD Pathology. Metabolites 2018, 8, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galasko, D.; Bennett, D.; Sano, M.; Ernesto, C.; Thomas, R.; Grundman, M.; Ferris, S. An inventory to assess activities of daily living for clinical trials in Alzheimer’s disease. The Alzheimer’s Disease Cooperative Study. Alzheimer Dis. Assoc. Disord. 1997, 11 (Suppl. 2), S33–S39. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.P.; Berg, L.; Danziger, W.; Coben, L.A.; Martin, R.L. A New Clinical Scale for the Staging of Dementia. Br. J. Psychiatry 1982, 140, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, R.I.; Kurosaki, T.T.; Harrah, C.H.; Chance, J.M.; Filos, S. Measurement of Functional Activities in Older Adults in the Community. J. Gerontol. 1982, 37, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary Clinical Validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Cudaback, E.; Jorstad, N.L.; Yang, Y.; Montine, T.J.; Keene, C.D. Therapeutic implications of the prostaglandin pathway in Alzheimer’s disease. Biochem. Pharmacol. 2014, 88, 565–572. [Google Scholar] [CrossRef] [Green Version]
- Tuppo, E.; Forman, L.; Spur, B.; Chan-Ting, R.; Chopra, A.; Cavalieri, T. Sign of lipid peroxidation as measured in the urine of patients with probable Alzheimer’s disease. Brain Res. Bull. 2001, 54, 565–568. [Google Scholar] [CrossRef]
- García-Blanco, A.; Peña-Bautista, C.; Oger, C.; Vigor, C.; Galano, J.-M.; Durand, T.; Martín-Ibáñez, N.; Baquero, M.; Vento, M.; Cháfer-Pericás, C. Reliable determination of new lipid peroxidation compounds as potential early Alzheimer Disease biomarkers. Talanta 2018, 184, 193–201. [Google Scholar] [CrossRef]
- Greco, A.; Minghetti, L.; Levi, G. Isoprostanes, Novel Markers of Oxidative Injury, Help Understanding the Pathogenesis of Neurodegenerative Diseases. Neurochem. Res. 2000, 25, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Minghetti, L.; Greco, A.; Cardone, F.; Puopolo, M.; Ladogana, A.; Almonti, S.; Cunningham, C.; Perry, V.H.; Pocchiari, M.; Levi, G. Increased Brain Synthesis of Prostaglandin E 2 and F 2 -Isoprostane in Human and Experimental Transmissible Spongiform Encephalopathies. J. Neuropathol. Exp. Neurol. 2000, 59, 866–871. [Google Scholar] [CrossRef] [Green Version]
- Farooqui, A.A.; Horrocks, L.A.; Farooqui, T. Interactions between neural membrane glycerophospholipid and sphingolipid mediators: A recipe for neural cell survival or suicide. J. Neurosci. Res. 2007, 85, 1834–1850. [Google Scholar] [CrossRef] [PubMed]
- Milne, G.L.; Gao, B.; Terry, E.S.; Zackert, W.E.; Sanchez, S.C. Measurement of F2- isoprostanes and isofurans using gas chromatography–mass spectrometry. Free Radic. Biol. Med. 2013, 59, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Montine, T.J.; Markesbery, W.R.; Zackert, W.; Sanchez, S.C.; Roberts, L.J.; Morrow, J.D. The Magnitude of Brain Lipid Peroxidation Correlates with the Extent of Degeneration but Not with Density of Neuritic Plaques or Neurofibrillary Tangles or with APOE Genotype in Alzheimer’s Disease Patients. Am. J. Pathol. 1999, 155, 863–868. [Google Scholar] [CrossRef]
- Montine, K.S.; Quinn, J.F.; Zhang, J.; Fessel, J.P.; Roberts, L.J.; Morrow, J.D.; Montine, T.J. Isoprostanes and related products of lipid peroxidation in neurodegenerative diseases. Chem. Phys. Lipids 2004, 128, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Snowden, S.G.; Ebshiana, A.A.; Hye, A.; An, Y.; Pletnikova, O.; O’Brien, R.; Troncoso, J.; Legido-Quigley, C.; Thambisetty, M. Association between fatty acid metabolism in the brain and Alzheimer disease neuropathology and cognitive performance: A nontargeted metabolomic study. PLoS Med. 2017, 14, e1002266. [Google Scholar] [CrossRef] [Green Version]
- Irizarry, M.C.; Hyman, B.T. Brain isoprostanes: A marker of lipid peroxidation and oxidative stress in AD. Neurology 2003, 61, 436–437. [Google Scholar] [CrossRef]
- Connolly, J.; Siderowf, A.; Clark, C.M.; Mu, D.; Pratico, D. F2 Isoprostane Levels in Plasma and Urine do not Support Increased Lipid Peroxidation in Cognitively Impaired Parkinson Disease Patients. Cogn. Behav. Neurol. 2008, 21, 83–86. [Google Scholar] [CrossRef]
- Fessel, J.P.; Hulette, C.; Powell, S.; Roberts, L.J.; Zhang, J. Isofurans, but not F2-isoprostanes, are increased in the substantia nigra of patients with Parkinson’s disease and with dementia with Lewy body disease. J. Neurochem. 2003, 85, 645–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galano, J.-M.; Mas, E.; Barden, A.; Mori, T.A.; Signorini, C.; De Felice, C.; Barrett, A.; Opere, C.; Pinot, E.; Schwedhelm, E.; et al. Isoprostanes and neuroprostanes: Total synthesis, biological activity and biomarkers of oxidative stress in humans. Prostaglandins Other Lipid Mediat. 2013, 107, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, O.S.; Galano, J.-M.; Pavlickova, T.; Revol-Cavalier, J.; Vigor, C.; Lee, J.C.-Y.; Oger, C.; Durand, T. Moving forward with isoprostanes, neuroprostanes and phytoprostanes: Where are we now? Essays Biochem. 2020, 64, 463–484. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.S.; Galano, J.M.; Durand, T.; Lee, J.C.-Y. Current development in non-enzymatic lipid peroxidation products, isoprostanoids and isofuranoids, in novel biological samples. Free Radic. Res. 2015, 49, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Montine, T.J.; Quinn, J.F.; Milatovic, D.; Silbert, L.C.; Dang, T.; Sanchez, S.; Terry, E.; Roberts, L.J.; Kaye, J.A.; Morrow, J.D. Peripheral F2-isoprostanes and F4-neuroprostanes are not increased in Alzheimer’s disease. Ann. Neurol. 2002, 52, 175–179. [Google Scholar] [CrossRef]
- Singh, M.; Nam, D.T.; Arseneault, M.; Ramassamy, C. Role of By-Products of Lipid Oxidation in Alzheimer’s Disease Brain: A Focus on Acrolein. J. Alzheimer’s Dis. 2010, 21, 741–756. [Google Scholar] [CrossRef]
- Song, W.-L.; Lawson, J.A.; Reilly, D.; Rokach, J.; Chang, C.-T.; Giasson, B.; FitzGerald, G.A. Neurofurans, Novel Indices of Oxidant Stress Derived from Docosahexaenoic Acid. J. Biol. Chem. 2008, 283, 6–16. [Google Scholar] [CrossRef] [Green Version]
- Roberts, L.J.; Milne, G.L. Isoprostanes. J. Lipid Res. 2009, 50, S219–S223. [Google Scholar] [CrossRef] [Green Version]
- VanRollins, M.; Woltjer, R.L.; Yin, H.; Morrow, J.D.; Montine, T.J. F2-Dihomo-isoprostanes arise from free radical attack on adrenic acid. J. Lipid Res. 2008, 49, 995–1005. [Google Scholar] [CrossRef] [Green Version]
- Medina, S.; De Miguel-Elízaga, I.; Oger, C.; Galano, J.-M.; Durand, T.; Martínez-Villanueva, M.; Castillo, M.L.G.-D.; Villegas-Martínez, I.; Ferreres, F.; Martínez-Hernández, P.; et al. Dihomo-isoprostanes—nonenzymatic metabolites of AdA—are higher in epileptic patients compared to healthy individuals by a new ultrahigh pressure liquid chromatography–triple quadrupole–tandem mass spectrometry method. Free Radic. Biol. Med. 2015, 79, 154–163. [Google Scholar] [CrossRef]
- De Felice, C.; Signorini, C.; Durand, T.; Oger, C.; Guy, A.; Bultel-Poncé, V.; Galano, J.-M.; Ciccoli, L.; Leoncini, S.; D’Esposito, M.; et al. F2-dihomo-isoprostanes as potential early biomarkers of lipid oxidative damage in Rett syndrome. J. Lipid Res. 2011, 52, 2287–2297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skinner, E.R.; Watt, C.; Besson, J.A.O.; Best, P.V. Differences in the fatty acid composition of the grey and white matter of different regions of the brains of patients with Alzheimer’s disease and control subjects. Brain 1993, 116, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, F.M.; Horrobin, D.F.; Skinner, E.R.; Besson, J.A.O.; Cooper, M.B. Abnormal content of n−6 and n−3 long-chain unsaturated fatty acids in the phosphoglycerides and cholesterol esters of parahippocampal cortex from Alzheimer’s disease patients and its relationship to acetyl CoA content. Int. J. Biochem. Cell Biol. 1998, 30, 197–207. [Google Scholar] [CrossRef]
- Proitsi, P.; Kim, M.; Whiley, L.; Pritchard, M.; Leung, R.; Soininen, H.; Kloszewska, I.; Mecocci, P.; Tsolaki, M.; Vellas, B.; et al. Plasma lipidomics analysis finds long chain cholesteryl esters to be associated with Alzheimer’s disease. Transl. Psychiatry 2015, 5, e494. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Clinical Evaluation | Classification of Participants | ||||
|---|---|---|---|---|---|
| Healthy | MCI-AD | MD-AD | AD-AD | Non-AD | |
| β-Amyloid-42 (pg·mL−1) | >725 | <725 | <725 | <725 | >725 |
| t-tau (pg·mL−1) | <485 | >485 | >485 | >485 | <485 |
| p-tau (pg·mL−1) | <56 | >56 | >56 | >56 | <56 |
| ADCS-ADL-MCI | >44 | <44 | <44 | <44 | <44 |
| CDR | 0 | ≤0.5 | ≤1 | ≥2 | ≤1 |
| FAQ | <9 | <9 | >9 | >9 | >9 |
| MMSE | ≥27 | ≤27 | ≤27 | ≤27 | ≤27 |
| RBANS.DM | ≥85 | ≤85 | ≤85 | ≤85 | ≤85 |
| Variable | Healthy (n = 80) | MCI-AD (n = 106) | MD-AD (n = 70) | AD-AD (n = 11) | Non-AD (n = 20) | p Value (Kruskal-Wallis Test) | |
|---|---|---|---|---|---|---|---|
| Demographic characteristics | |||||||
| Age (years, median (IQR)) | 63 (61–68) | 70 (67–74) | 71 (67–74) | 66 (70–73) | 65 (59–71) | <0.01 | |
| Gender (female (%)) | 44 (55%) | 61 (57.5%) | 46 (65.7%) | 7 (63.6%) | 11 (55%) | 0.70 | |
| Level of education n (%) | Basic Secondary University | 22 (27.5%) 21 (26.3%) 37 (46.3%) | 59 (55.7%) 23 (21.7%) 24 (22.6%) | 41 (58.6%) 16 (22.9%) 13 (18.6%) | 9 (81.8%) 1 (9.1%) 1 (9.1%) | 14 (70%) 3 (15%) 3 (15%) | <0.01 |
| Clinical characteristics | |||||||
| β-Amyloid-42 (pg·mL−1, median (IQR)) | 1201 (942.75–1439.75) | 597 (471.05–709.07) | 574 (444.75–648.50) | 636 (601.76–708.88) | 982 (858–1647) | <0.01 | |
| t-tau (pg·mL−1, median (IQR)) | 224 (173.25–304) | 583 (432.50–773.50) | 621 (448.50–945.50) | 699 (473–936) | 289 (205–376) | <0.01 | |
| p-tau (pg·mL−1, median (IQR)) | 36 (28–47.25) | 90 (70.50–109.50) | 88.50 (73–144) | 95 (73–122) | 40 (32–61) | <0.01 | |
| ADCS-ADL-MCI (median (IQR)) | 47 (43–50.75) | 41 (31–46) | 36 (24–42) | 29.50 (3–34.50) | 29 (22.50–40.75) | <0.01 | |
| CDR (median (IQR)) | 0 (0–0) | 0.5 (0.5–0.5) | 1 (0.5–1) | 2 (2–3) | 1 (0.5–1) | <0.01 | |
| FAQ (median (IQR)) | 0 (0–2) | 4 (1–7) | 13 (10–17.25) | 21 (14–25) | 11.50 (8–21) | <0.01 | |
| MMSE (median (IQR)) | 29 (28–30) | 25 (22–27.25) | 20 (17.75–24) | 14 (12–19) | 23 (18–25) | <0.01 | |
| RBANS.DM (median (IQR)) | 100 (95–106) | 52 (40–75) | 40 (40–49) | 40 (40–44) | 58 (45–78) | <0.01 | |
| Variable (nmol·L−1) | Healthy (n = 80) Median (1st, 3rd Quartile) | MCI-AD (n = 106) Median (1st, 3rd Quartile) | MD-AD (n = 70) Median (1st, 3rd Quartile) | AD-AD (n = 11) Median (1st, 3rd Quartile) | Non-AD (n = 20) Median (1st, 3rd Quartile) | p Value (Kruskal-Wallis Test) | |
|---|---|---|---|---|---|---|---|
| PGs a | PGE2 | 0.27 (0.05–0.45) | 0.07 (0–0.35) | 0.12 (0.04–0.50) | 0.10 (0–0.20) | 0.10 (0.07–0.16) | 0.03 * |
| PGF2α | 0.55 (0.28–0.86) | 0.60 (0.10–0.85) | 0.63 (0.26–1.13) | 0.60 (0.30–0.80) | 0.88 (0.53–1.38) | 0.058 ^ | |
| 15-E2t-IsoP | 0.78 (0.27–1.56) | 0.31 (0.09–1.01) | 0.30 (0.07–1.08) | 0.25 (0–0.67) | 0.13 (0.05–0.29) | <0.01 * | |
| 15-F2t-IsoP | 0.03 (0.01–0.06) | 0.02 (0–0.05) | 0.03 (0–0.21) | 0.02 (0–0.03) | 0 (0–0.57) | 0.08 | |
| IsoPs a | 15(R)-15-F2t-IsoP | 0.31 (0.20–0.59) | 0.30 (0.16–0.53) | 0.35 (0.20–0.58) | 0.25 (0.06–0.45) | 0.48 (0.21–0.75) | 0.21 |
| 2,3-dinor-15-epi-15-F2t-IsoP | 0 (0–0.02) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.58 | |
| 15-keto-15-E2t-IsoP | 0.33 (0–0.92) | 0 (0–0.17) | 0.01 (0–0.25) | 0 (0–0.32) | 0.05 (0–0.38) | <0.01 * | |
| 15-keto-15-F2t-IsoP | 0.37 (0.17–0.67) | 0.25 (0.07–0.40) | 0.33 (0.15–0.56) | 0.27 (0.07–0.40) | 0.47 (0.30–0.78) | <0.01 * | |
| 5-F2t-IsoP | 1.38 (0.88–2.62) | 0.98 (0.33–1.69) | 1.25 (0.65–2.00) | 0.65 (0.35–1.45) | 1.98 (1.08–2.55) | <0.01 * | |
| Total IsoPs | 0.72 (0.31–1.39) | 0.39 (0.26–0.67) | 0.45 (0.30–0.68) | 0.27 (0.22–0.37) | 0.62 (0.44–0.79) | <0.01 * | |
| IsoFs a | Total IsoFs | 0.33 (0.08–0.46) | 0.14 (0.08–0.32) | 0.19 (0.09–0.36) | 0.08 (0.05–0.14) | 0.23 (0.19–0.40) | <0.01 * |
| NeuroPs b | 4(RS)-4-F4t-NeuroP | 1.37 (0.95–3.68) | 1.10 (0–1.50) | 1.08 (0.58–1.40) | 0.97 (0–1.27) | 1.03 (0.61–1.46) | <0.01 * |
| 10-epi-10-F4t-NeuroP | 0.15 (0.06–0.22) | 0.13 (0.01–0.22) | 0.20 (0.05–0.32) | 0.11 (0.07–0.20) | 0.32 (0.25–0.41) | <0.01 * | |
| 14(RS)-14-F4t-NeuroP | 1.08 (0.13–1.89) | 0.53 (0–1.58) | 0.88 (0.25–1.30) | 0.15 (0–0.42) | 0.91 (0.60–1.43) | 0.01 * | |
| Total NeuroPs | 0.05 (0–0.56) | 0 (0–0.11) | 0 (0–0.05) | 0 (0–0.38) | 0.01 (0–0.06) | <0.01 * | |
| NeuroFs b | Total NeuroFs | 0.16 (0.06–0.32) | 0.15 (0.05–0.33) | 0.12 (0.05–0.25) | 0.09 (0–0.11) | 0.08 (0.04–0.15) | 0.02 * |
| Dihomo-IsoPs c | 1a,1b-dihomo-PGF2α | 0 (0–3.34) | 0 (0–0) | 0 (0–1.03) | 0 (0–0) | 1.18 (0–1.40) | <0.01 * |
| Ent-7(RS)-7-F2t-dihomo-IsoP | 0.03 (0–0.17) | 0.10 (0–0.22) | 0.15 (0.10–0.22) | 0.15 (0.05–0.22) | 0.12 (0.10–0.19) | <0.01 * | |
| 17-F2t-dihomo-IsoP | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.10 | |
| 17-epi-17-F2t-dihomo-IsoP | 0 (0–0) | 0 (0–0.02) | 0 (0–0.02) | 0 (0–0.02) | 0 (0–0) | 0.054 ^ | |
| Dihomo-IsoFs c | 17(RS)-10-epi-SC-Δ15-11-dihomo-IsoF | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.07 |
| 7(RS)-ST-Δ8-11-dihomo-IsoF | 0 (0–0.22) | 0 (0–0.17) | 0.02 (0–0.10) | 0.05 (0.02–0.12) | 0 (0–0.09) | 0.52 | |
| Lipids | Healthy vs. MCI-AD | Healthy vs. MD-AD | Healthy vs. AD-AD | Healthy vs. Non-AD | MCI-AD vs. MD-AD | MCI-AD vs. AD-AD | MCI-AD vs. Non-AD | MD-AD vs. AD-AD | MD-AD vs. Non-AD | |
|---|---|---|---|---|---|---|---|---|---|---|
| PGs a | PGE2 | <0.01 * | 0.38 | 0.06 | 0.23 | 0.05 * | 0.78 | 0.23 | 0.23 | 0.90 |
| PGF2α | 0.66 | 0.30 | 0.97 | <0.01 * | 0.16 | 0.79 | <0.01 * | 0.50 | 0.09 | |
| 15-E2t-IsoP | <0.01 * | <0.01 * | 0.01 * | <0.01 * | 0.99 | 0.37 | 0.09 | 0.52 | 0.09 | |
| 15-F2t-IsoP | 0.07 | 0.24 | 0.10 | 0.59 | 0.01 * | 0.89 | 0.95 | 0.18 | 0.26 | |
| IsoPs a | 15(R)-15-F2t-IsoP | 0.65 | 0.51 | 0.21 | 0.20 | 0.20 | 0.23 | 0.07 | 0.12 | 0.31 |
| 2,3-dinor-15-epi-15-F2t-IsoP | 0.48 | 0.19 | 0.40 | 0.22 | 0.46 | 0.61 | 0.40 | 0.91 | 0.73 | |
| 15-keto-15-E2t-IsoP | <0.01 * | <0.01 * | 0.03 * | 0.11 | 0.08 | 0.57 | 0.11 | 0.79 | 0.73 | |
| 15-keto-15-F2t-IsoP | <0.01 * | 0.42 | 0.19 | 0.18 | 0.02 * | 0.76 | <0.01 * | 0.35 | 0.05 * | |
| 5-F2t-IsoP | <0.01 * | 0.06 | 0.01 * | 0.31 | 0.16 | 0.47 | <0.01 * | 0.10 | 0.01 * | |
| Total IsoPs | <0.01 * | 0.01 * | <0.01 * | 0.49 | 0.33 | 0.02 * | 0.01 * | <0.01 * | 0.09 | |
| IsoFs a | Total IsoFs | <0.01 * | 0.051 ^ | <0.01 * | 0.63 | 0.21 | 0.01 * | 0.02 * | <0.01 * | 0.18 |
| NeuroPs b | 4(RS)-4-F4t-NeuroP | <0.01 * | <0.01 * | 0.02 * | 0.02 * | 0.95 | 0.38 | 0.98 | 0.35 | 0.92 |
| 10-epi-10-F4t-NeuroP | 0.72 | 0.18 | 0.55 | <0.01 * | 0.10 | 0.73 | <0.01 * | 0.34 | <0.01 * | |
| 14(RS)-14-F4t-NeuroP | 0.059 ^ | 0.26 | <0.01 * | 0.99 | 0.26 | 0.07 | 0.17 | <0.01 * | 0.49 | |
| Total NeuroPs | <0.01 * | <0.01 * | 0.15 | 0.28 | 0.73 | 0.98 | 0.34 | 0.98 | 0.12 | |
| NeuroFs b | Total NeuroFs | 0.73 | 0.39 | <0.01 * | 0.04 * | 0.58 | <0.01 * | 0.054 ^ | 0.02 * | 0.14 |
| Dihomo-IsoPs c | 1a,1b-dihomo-PGF2α | <0.01 * | <0.01 * | <0.01 * | 0.78 | 0.26 | 0.14 | <0.01 * | 0.06 | <0.01 * |
| Ent-7(RS)-7-F2t-dihomo-IsoP | 0.01 * | <0.01 * | 0.08 | 0.02 * | 0.01 * | 0.57 | 0.51 | 0.60 | 0.35 | |
| 17-F2t-dihomo-IsoP | 0.56 | 0.04 * | 0.51 | 0.06 | 0.08 | 0.42 | 0.13 | 0.21 | 0.82 | |
| 17-epi-17-F2t-dihomo-IsoP | <0.01 * | <0.01 * | 0.26 | 0.48 | 0.65 | 0.82 | 0.36 | 0.68 | 0.27 | |
| Dihomo-IsoFs c | 17(RS)-10-epi-SC-Δ15-11-dihomo-IsoF | 0.64 | 0.059 ^ | 0.59 | 0.02 * | 0.09 | 0.51 | 0.04 * | 0.27 | 0.53 |
| 7(RS)-ST-Δ8-11-dihomo-IsoF | 0.89 | 0.83 | 0.38 | 0.21 | 0.92 | 0.22 | 0.28 | 0.19 | 0.24 | |
| Parameter | (95% CI) |
|---|---|
| Sensitivity (%) | 81.3 (75.1–86.2) |
| Specificity (%) | 64 (54.2–72.7) |
| Accuracy (%) | 75.3 (70–80) |
| Positive predictive value (%) | 81 (74.6–85.8) |
| Negative predictive value (%) | 64.6 (54.8–73.4) |
| Odds ratio | 7.72 (4.46–13.37) |
| Lipids | p Value (Kruskal-Wallis Test) | |
|---|---|---|
| PGs a | PGE2 | 0.11 |
| PGF2α | 0.36 | |
| 15-E2t-IsoP | 0.71 | |
| 15-F2t-IsoP | 0.03 * | |
| IsoPs a | 15(R)-15-F2t-IsoP | 0.17 |
| 2,3-dinor-15-epi-15-F2t-IsoP | 0.71 | |
| 15-keto-15-E2t-IsoP | 0.22 | |
| 15-keto-15-F2t-IsoP | 0.08 | |
| 5-F2t-IsoP | 0.19 | |
| Total IsoPs | 0.02 * | |
| IsoFs a | Total IsoFs | 0.01 * |
| NeuroPs b | 4(RS)-4-F4t-NeuroP | 0.65 |
| 10-epi-10-F4t-NeuroP | 0.23 | |
| 14(RS)-14-F4t-NeuroP | 0.03 * | |
| Total NeuroPs | 0.94 | |
| NeuroFs b | Total NeuroFs | 0.03 * |
| Dihomo-IsoPs c | 1a,1b-dihomo-PGF2α | 0.13 |
| Ent-7(RS)-7-F2t-dihomo-IsoP | 0.06 | |
| 17-F2t-dihomo-IsoP | 0.13 | |
| 17-epi-17-F2t-dihomo-IsoP | 0.86 | |
| Dihomo-IsoFs c | 17(RS)-10-epi-SC-Δ15-11-dihomo-IsoF | 0.15 |
| 7(RS)-ST-Δ8-11-dihomo-IsoF | 0.43 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferré-González, L.; Peña-Bautista, C.; Baquero, M.; Cháfer-Pericás, C. Assessment of Lipid Peroxidation in Alzheimer’s Disease Differential Diagnosis and Prognosis. Antioxidants 2022, 11, 551. https://doi.org/10.3390/antiox11030551
Ferré-González L, Peña-Bautista C, Baquero M, Cháfer-Pericás C. Assessment of Lipid Peroxidation in Alzheimer’s Disease Differential Diagnosis and Prognosis. Antioxidants. 2022; 11(3):551. https://doi.org/10.3390/antiox11030551
Chicago/Turabian StyleFerré-González, Laura, Carmen Peña-Bautista, Miguel Baquero, and Consuelo Cháfer-Pericás. 2022. "Assessment of Lipid Peroxidation in Alzheimer’s Disease Differential Diagnosis and Prognosis" Antioxidants 11, no. 3: 551. https://doi.org/10.3390/antiox11030551
APA StyleFerré-González, L., Peña-Bautista, C., Baquero, M., & Cháfer-Pericás, C. (2022). Assessment of Lipid Peroxidation in Alzheimer’s Disease Differential Diagnosis and Prognosis. Antioxidants, 11(3), 551. https://doi.org/10.3390/antiox11030551