
Oxidative Stress Markers and Antioxidant Enzymes in Children and Adolescents with Depressive Disorder and Impact of Omega-3 Fatty Acids in Randomised Clinical Trial



 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biochemical Parameters
2.2. Statistical Analysis
3. Results
3.1. Baseline Data
3.2. Effect of FA Supplementation in Patients Suffering from Depressive Disorder
3.3. The Correlations between Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laher, I. (Ed.) Systems Biology of Free Radicals and Antioxidants, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Ďuračková, Z. Some current insights into oxidative stress. Physiol. Res. 2010, 59, 459–469. [Google Scholar] [CrossRef]
- Ďuračková, Z. Free radicals and antioxidants for non-experts. In Systems Biology of Free Radicals and Antioxidants, 1st ed.; Laher, I., Ed.; Springer: Berlin/Heidelberg, Germany, 2014; Volume 1, pp. 3–38. [Google Scholar]
- Delmastro, M.M.; Piganelli, J.D. Oxidative stress and redox modulation potential in type 1 diabetes. Clin. Dev. Immunol. 2011, 2011, 1–15. [Google Scholar] [CrossRef]
- Gospodaryov, D.V.; Lushchak, V. Oxidative stress: Cause and consequence of diseases. In Oxidative Stress and Diseases, 1st ed.; Lushchak, V., Ed.; InTech: Rijeka, Croatia, 2012; Volume 1, pp. 13–38. [Google Scholar]
- Sivoňová, M.; Žitňanová, I.; Hlinčíková, L.; Škodáček, I.; Trebatická, J.; Ďuračková, Z. Oxidative stress in university students during examinations. Stress 2004, 7, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Chovanová, Z.; Muchová, J.; Sivoňová, M.; Dvořáková, M.; Žitňanová, I.; Waczulíková, I.; Trebatická, J.; Škodáček, I.; Ďuračková, Z. Effect of polyphenolic extract, Pycnogenol, on the level of 8-oxoguanine in children suffering from attention deficit/hyperactivity disorder. Free Radic. Res. 2006, 40, 1003–1010. [Google Scholar] [CrossRef]
- Dvořáková, M.; Sivoňová, M.; Trebatická, J.; Škodáček, I.; Waczuliková, I.; Muchová, J.; Ďuračková, Z. The effect of polyphenolic extract from pine bark, Pycnogenol on the level of glutathione in children suffering from attention deficit hyperactivity disorder (ADHD). Redox Rep. 2006, 1, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Salim, S. Oxidative stress and the central nervous system. J. Pharmacol. Exp. Ther. 2017, 360, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Vaváková, M.; Ďuračková, Z.; Trebatická, J. Markers of oxidative stress and neuroprogression in depression disorder. Oxidative Med. Cell. Longev. 2015, 2015, 898393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraguas, D.; Díaz-Caneja, C.M.; Ayora, M.; Hernández-Álvarez, F.; Rodríguez-Quiroga, A.; Recio, S.; Leza, J.C.; Arango, C. Oxidative stress and inflammation in first-episode psychosis: A systematic review and meta-analysis. Schizophr. Bull. 2019, 45, 742–751. [Google Scholar] [CrossRef]
- Ozdemir, O.; Selvi, Y.; Ozkol, H.; Tuluce, Y.; Besiroglu, L.; Aydin, A. Comparison of superoxide dismutase, glutathione peroxidase and adenosine deaminase activities between respiratory and nocturnal subtypes of patients with panic disorder. Neuropsychobiology 2012, 66, 244–251. [Google Scholar] [CrossRef]
- Siwek, M.; Sowa-Kućma, M.; Dudek, D.; Styczeń, K.; Szewczyk, B.; Kotarska, K.; Misztakk, P.; Pilc, A.; Wolak, M.; Nowak, G. Oxidative stress markers in affective disorders. Pharmacol. Rep. 2013, 65, 1558–1571. [Google Scholar] [CrossRef] [Green Version]
- Black, C.N.; Bot, M.; Scheffer, P.G.; Cuijpers, P.; Penninx, B.W. Is depression associated with increased oxidative stress? A systematic review and meta-analysis. Psychoneuroendocrinology 2015, 51, 164–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozcan, M.E.; Gulec, M.; Ozerol, E.; Polat, R.; Akyol, O. Antioxidant enzyme activities and oxidative stress in affective disorders. Int. Clin. Psychopharmacol. 2004, 19, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Black, C.N.; Bot, M.; Scheffer, P.G.; Penninx, B.W. Oxidative stress in major depressive and anxiety disorders, and the association with antidepressant use; results from a large adult cohort. Psychol. Med. 2017, 47, 936–948. [Google Scholar] [CrossRef] [Green Version]
- Greaney, J.L.; Saunders, E.F.H.; Santhanam, L.; Alexander, L.M. Oxidative stress contributes to microvascular endothelial dysfunction in men and women with major depressive disorder. Circ. Res. 2019, 15, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Freed, R.D.; Hollenhorst, C.N.; Weiduschat, N.; Mao, X.; Kang, G.; Shungu, D.C.; Gabbay, V. A pilot study of cortical glutathione in youth with depression. Psychiatry Res. Neuroimaging 2017, 270, 54–60. [Google Scholar] [CrossRef]
- Magalhães, P.V.; Jansen, K.; Pinheiro, R.T.; Colpo, G.D.; da Motta, L.L.; Klamt, F.; da Silva, R.A.; Kapczinski, F. Peripheral oxidative damage in early-stage mood disorders: A nested population-based case-control study. Int. J. Neuropsychopharmacol. 2012, 15, 1043–1050. [Google Scholar] [CrossRef] [Green Version]
- Scola, G.; McNamara, R.K.; Croarkin, P.E.; Leffler, J.M.; Cullen, K.R.; Geske, J.R.; Biernacka, J.M.; Frye, M.A.; DelBello, M.P.; Andreazza, A.C. Lipid peroxidation biomarkers in adolescents with or at high-risk for bipolar disorder. J. Affect. Disord. 2016, 192, 176–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cháfer-Pericás, C. Lipid peroxidation in neurodegeneration. Antioxidants 2021, 10, 484. [Google Scholar] [CrossRef]
- Lotrich, F.E.; Sears, B.; McNamara, R.K. Elevated ratio of arachidonic acid to long-chain omega-3 fatty acids predict depression development following interferon-alpha treatment: Relationship with interleukin-6. Brain Behav. Immun. 2013, 31, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tassoni, D.; Kaur, G.; Weisinger, R.S.; Sinclair, A.J. The role of eicosanoids in the brain. Asia Pac. J. Clin. Nutr. 2008, 17 (Suppl. 1), 220–228. [Google Scholar]
- Trebatická, J.; Hradečná, Z.; Surovcová, A.; Katrenčíková, B.; Gushina, I.; Waczulíková, I.; Sušienková, K.; Garaiova, I.; Šuba, J.; Ďuračková, Z. Omega-3 fatty-acids modulate symptoms of depressive disorder, serum levels of omega-3 fatty acids and omega-6/omega-3 ratio in children. A randomized, double-blind and controlled trial. Psychiatry Res. 2020, 287, 112911. [Google Scholar] [CrossRef] [PubMed]
- Katrenčíková, B.; Vaváková, M.; Waczulíková, I.; Oravec, S.; Garaiova, I.; Nagyová, Z.; Hlaváčová, N.; Ďuračková, Z.; Trebatická, J. Lipid profile, lipoprotein subfractions, and fluidity of membranes in children and adolescents with depressive disorder: Effect of omega-3 fatty acids in a double-blind randomized controlled study. Biomolecules 2020, 10, 1427. [Google Scholar] [CrossRef] [PubMed]
- Paduchová, Z.; Katrenčíková, B.; Vaváková, M.; Laubertová, L.; Nagyová, Z.; Garaiová, I.; Ďuračková, Z.; Trebatická, J. The effect of omega-3 fatty acids on thromboxane, brain-derived neurotrophic factor, homocysteine, and vitamin d in depressive children and adolescents: Randomized controlled trial. Nutrients 2021, 13, 1095. [Google Scholar] [CrossRef]
- Drabkin, D.L.; Austin, J.H. Spectrophotometric studies I. Spectrophotometric constants for common hemoglobin derivatives in human, dog and rabbit blood. J. Biol. Chem. 1932, 98, 719–733. [Google Scholar] [CrossRef]
- El–Saadani, M.; Esterbauer, H.; El-Sayed, M.; Goher, M.; Nassar, A.Y.; Jürgens, G. A spectrophotometric assay for lipid peroxides in serum lipoproteins using a commercially available reagent. J. Lipid Res. 1989, 30, 627–630. [Google Scholar] [CrossRef]
- Witko-Sarsat, V.; Friedlander, M.; Capeillere-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. AOPP as a novel marker of oxidative stress in uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef] [Green Version]
- Re, E.; Pellegrini, L.; Prottegente, A.; Pannala, A.; Yang, M.; Rice-Evans, C. Antioxidant activity applying an improved ABTS radical cation decolorization assay. Free Radic. Biol. Med. 1999, 9–10, 1231–1237. [Google Scholar] [CrossRef]
- Bergmeyer, H.U. (Ed.) Methods of Enzymatic Analysis; Volume III: Enzymes 1: Oxidoreductases, Transferases; Verlag Chemie: Weinheim, Germany; Deerfield Beach, FL, USA; Basel, Switzerland, 1983. [Google Scholar]
- Michel, T.M.; Pülschen, D.; Thome, J. The role of oxidative stress in depressive disorders. Curr. Pharm. Des. 2012, 18, 5890–5899. [Google Scholar] [CrossRef] [Green Version]
- Maes, M.; Landucci Bonifacio, K.; Morelli, N.R.; Vargas, H.O.; Barbosa, D.S.; Carvalho, A.F.; Nunes, S.O.V. Major differences in neurooxidative and neuronitrosative stress pathways between major depressive disorder and types I and II bipolar disorder. Mol. Neurobiol. 2019, 56, 141–156. [Google Scholar] [CrossRef]
- Ohmori, H.; Kanayama, N. Immunogenicity of an inflammation-associated product, tyrosine nitrated self-proteins. Autoimmun. Rev. 2005, 4, 224–229. [Google Scholar] [CrossRef]
- Fuentes, E.; Moore-Carrasco, R.; de Andrade Paes, A.M.; Trostchansky, A. Role of platelet activation and oxidative stress in the evolution of myocardial infarction. J. Cardiovasc. Pharmacol. Ther. 2019, 24, 509–520. [Google Scholar] [CrossRef]
- Stefanescu, C.; Ciobica, A. The relevance of oxidative stress status in first episode and recurrent depression. J. Affect. Disord. 2012, 143, 34–38. [Google Scholar] [CrossRef]
- Kodydková, J.; Vávrová, L.; Zeman, M.; Jirák, R.; Macásek, J.; Stanková, B.; Tvrzická, E.; Zák, A. Antioxidative enzymes and increased oxidative stress in depressive women. Clin. Biochem. 2009, 42, 1368–1374. [Google Scholar] [CrossRef]
- Khanzode, S.D.; Dakhale, G.N.; Khanzode, S.S.; Saoji, A.; Palasodkar, R. Oxidative damage and major depression: The potential antioxidant action of selective serotonin re-uptake inhibitors. Redox Rep. 2003, 8, 365–37039. [Google Scholar] [CrossRef] [PubMed]
- Wiener, C.; Rassier, G.T.; Kaster, M.P.; Jansen, K.; Pinheiro, R.T.; Klamt, F.; Magalhães, P.V.; Kapczinski, F.; Ghisleni, G.; da Silva, R.A. Gender-based differences in oxidative stress parameters do not underlie the differences in mood disorders susceptibility between sexes. Eur. Psychiatry 2014, 29, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Teyssier, J.R.; Ragot, S.; Chauvet-Gélinier, J.C.; Trojak, B.; Bonin, B. Expression of oxidative stress-response genes is not activated in the prefrontal cortex of patients with depressive disorder. Psychiatry Res. 2011, 186, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Frijhoff, J.; Winyard, P.G.; Zarkovic, N.; Davies, S.S.; Stocker, R.; Cheng, D.; Knight, A.R.; Taylor, E.L.; Oettrich, J.; Ruskovska, T.; et al. Clinical relevance of biomarkers of oxidative stress. Antioxid. Redox Signal. 2015, 23, 1144–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciuculete, D.M.; Voisin, S.; Kular, L.; Jonsson, J.; Rask-Andersen, M.; Mwinyi, J.; Schiöth, H.B. meQTL and ncRNA functional analyses of 102 GWAS-SNPs associated with depression implicate HACE1 and SHANK2 genes. Clin. Epigenet. 2020, 12, 99. [Google Scholar] [CrossRef]
- da Cruz Jung, I.E.; da Cruz, I.B.M.; Barbisan, F.; Trott, A.; Houenou, L.J.; Turra, B.O.; Duarte, T.; de Souza Praia, R.; Maia-Ribeiro, E.A.; da Costa Escobar Piccoli, J.; et al. Superoxide imbalance triggered by Val16Ala-SOD2 polymorphism increases the risk of depression and self-reported psychological stress in free-living elderly people. Mol. Genet. Genom. Med. 2020, 8, e1080. [Google Scholar] [CrossRef] [PubMed]
- Ait Tayeb, A.E.K.; Becquemont, L.; El-Asmar, K.; Mahmoudi, K.; Colle, R.; Trabado, S.; Gressier, F.; Feve, B.; Corruble, E.; Verstuyft, C. SOD2 genetic polymorphism (rs4880) has no impact on 6-month response to antidepressant treatment and inflammatory biomarkers in depressed patients. Basic Clin. Pharmacol. Toxicol. 2020, 126, 289–295. [Google Scholar] [CrossRef]
- Bortolasci, C.C.; Vargas, H.O.; Souza-Nogueira, A.; Barbosa, D.S.; Moreira, E.G.; Nunes, S.O.; Berk, M.; Dodd, S.; Maes, M. Lowered plasma paraoxonase (PON)1 activity is a trait marker of major depression and PON1 Q192R gene polymorphism–smoking interactions differentially predict the odds of major depression and bipolar disorder. J. Affect. Disord. 2014, 159, 23–30. [Google Scholar] [CrossRef]
- Moreira, E.G.; Boll, K.M.; Correia, D.G.; Soares, J.F.; Rigobello, C.; Maes, M. Why should psychiatrists and neuroscientists worry about Paraoxonase 1? Curr. Neuropharmacol. 2019, 17, 1004–1020. [Google Scholar] [CrossRef]
- Mosca, A.; Del Casale, A.; Borro, M.; Gentile, G.; Pomes, L.M.; Padovano, A.; Fiaschè, F.; Pinzone, V.; Rapinesi, C.; Zoppi, T.; et al. PON1 polymorphisms can predict generalized anxiety and depressed mood in patients with multiple chemical sensitivity. Pers. Med. 2021, 18, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Pawełczyk, T.; Grancow-Grabka, M.; Trafalska, E.; Szemraj, J.; Pawełczyk, A. Oxidative stress reduction related to the efficacy of n-3 polyunsaturated fatty acids in first episode schizophrenia: Secondary outcome analysis of the OFFER randomized trial. Prostaglandins Leukot. Essent. Fatty Acids 2017, 121, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhong, S.; Liao, X.; Chen, J.; He, T.; Lai, S.; Jia, Y. A meta-analysis of oxidative stress markers in depression. PLoS ONE 2015, 10, e0138904. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Galano, J.M.; Leung, H.H.; Balas, L.; Oger, C.; Durand, T.; Lee, J.C. Nonenzymatic oxygenated metabolite of docosahexaenoic acid, 4(RS)-4-F4t -neuroprostane, acts as a bioactive lipid molecule in neuronal cells. FEBS Lett. 2020, 594, 1797–1808. [Google Scholar] [CrossRef]
- Singh, S.; Arora, R.R.; Singh, M.; Khosla, S. Eicosapentaenoic acid versus docosahexaenoic acid as options for vascular risk prevention: A fish story. Am. J. Ther. 2016, 23, e905–e910. [Google Scholar] [CrossRef]
- Moylan, S.; Berk, M.; Dean, O.M.; Samuni, Y.; Williams, L.J.; O’Neil, A.; Hayley, A.C.; Pasco, J.A.; Anderson, G.; Jacka, F.N.; et al. Oxidative & nitrosative stress in depression: Why so much stress? Neurosci. Biobehav. Rev. 2014, 45, 46–62. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Healthy Controls | Patients | p |
|---|---|---|---|
| (n = 20) | (n = 58) | ||
| 8-IsoP-U (ng/mmol Cr) | 104.8 ± 18.2 | 132.4 ± 41.9 | 0.009a |
| LP (nmol/mL) | 46.3 (32.6; 31.6) | 38.5 (27.7; 57.9) | 0.279 b |
| AOPP (µmol/L) | 40.5 (31.2; 46.6) | 73.8 (44.1; 87.1) | <0.0001b |
| NT (nmol/L) | 21.7 (11.4; 36.6) | 34.0 (20.6; 56.6) | 0.026b |
| TEAC (mmol/L) | 3.71 (3.41; 4.16) | 3.85 (3.05; 4.21) | 0.367 b |
| SOD (U/mg Hb) | 9.81 ± 5.68 | 9.74 ± 2.09 | 0.206 a |
| GPx (µkat/mg Hb) | 0.69 (0.54; 0.75) | 0.56 (0.34; 0.71) | 0.015b |
| CAT (µkat/g Hb) | 4.47 ± 0.81 | 4.23 ± 1.20 | 0.421 a |
| Patients—Om3 | Patients—Om6 | p between Om3 and Om6 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameters | Week 0 | Week 6 | p between 0 and 6 | Week 12 | p between 0 and 12 | Week 0 | Week 6 | p between 0 and 6 | Week 12 | p between 0 and 12 | Week 0 | Week 6 | Week 12 |
| n | 29 | 29 | 26 | 29 | 28 | 26 | 26 | ||||||
| 8-IsoP-U (ng/mmol Cr) | 133.8 ± 36.1 | 109.1 ± 44.1 | 0.005 | 89.9 ± 37.8 | <0.0001 | 123.2 ± 32.2 | 119.4 ± 40.1 | 0.509 | 113.6 ± 29.3 | 0.173 | 0.276 | 0.425 | 0.029 |
| LP (nmol/L) | 38.9 (28.3; 67.7) | 39.6 (26.5; 53.9) | 0.732 | 36.4 (22.6; 46.6) | 0.156 | 35.4 (27.2; 55.1) | 30.3 (26.6; 44.7) | 0.060 | 35.8 (24.6; 44.7) | 0.338 | 0.587 | 0.391 | 0.957 |
| AOPP (mmol/L) | 70.2 (59.8; 87.0) | 60.9 (38.7; 74.8) | <0.001 | 64.4 (47.4; 75.1) | 0.016 | 75.7 (44.5; 90.6) | 63.6 (39.7; 83.3) | 0.565 | 69.1 (47.7; 85.5) | 0.441 | 0.898 | 0.481 | 0.346 |
| NT (nmol/L) | 34.7 (24.0; 60.5) | 33.0 (21.0; 57.6) | 0.036 | 30.8 (15.7; 43.4) | 0.157 | 32.1 (18.7; 56.4) | 34.0 (18.6; 55.3) | 0.635 | 30.1 (16.9; 52.7) | 0.217 | 0.74 | 0.874 | 0.982 |
| TEAC (mmol/L) | 3.85 (3.05; 4.20) | 3.96 (3.64; 4.18) | 0.018 | 3.88 (3.51; 4.26) | 0.044 | 3.83 (3.40; 4.00) | 3.84 (3.65; 4.15) | 0.074 | 3.84 (3.51; 4.09) | 0.227 | 0.711 | 0.513 | 0.432 |
| SOD (U/mg Hb) | 9.77 ± 2.08 | 10.36 ± 2.21 | 0.022 | 10.68 ± 2.50 | 0.035 | 9.70 ± 2.10 | 10.11 ± 2.10 | 0.493 | 9.48 ± 1.90 | 0.764 | 0.901 | 0.664 | 0.06 |
| GPx (mkat/mg Hb) | 0.47 (0.32; 0.67) | 0.59 (0.38; 0.69) | 0.104 | 0.63 (0.37; 0.77) | 0.431 | 0.59 (0.37; 0.74) | 0.56 (0.40; 0.70) | 0.493 | 0.64 (0.40; 0.72) | 0.897 | 0.224 | 0.852 | 0.592 |
| CAT (mkat/g Hb) | 4.37 ± 1.42 | 4.32 ± 1.15 | 0.836 | 4.68 ± 1.47 | 0.478 | 4.10 ± 0.94 | 4.18 ± 1.5 | 0.756 | 4.06 ± 1.66 | 0.897 | 0.398 | 0.681 | 0.155 |
| All Patients at the Week 0 | n | r | p |
| CDI and 8-IsoP-U | 55 | 0.033 | 0.404 |
| CDI and LP | 52 | −0.135 | 0.169 |
| CDI and AOPP | 58 | −0.013 | 0.461 |
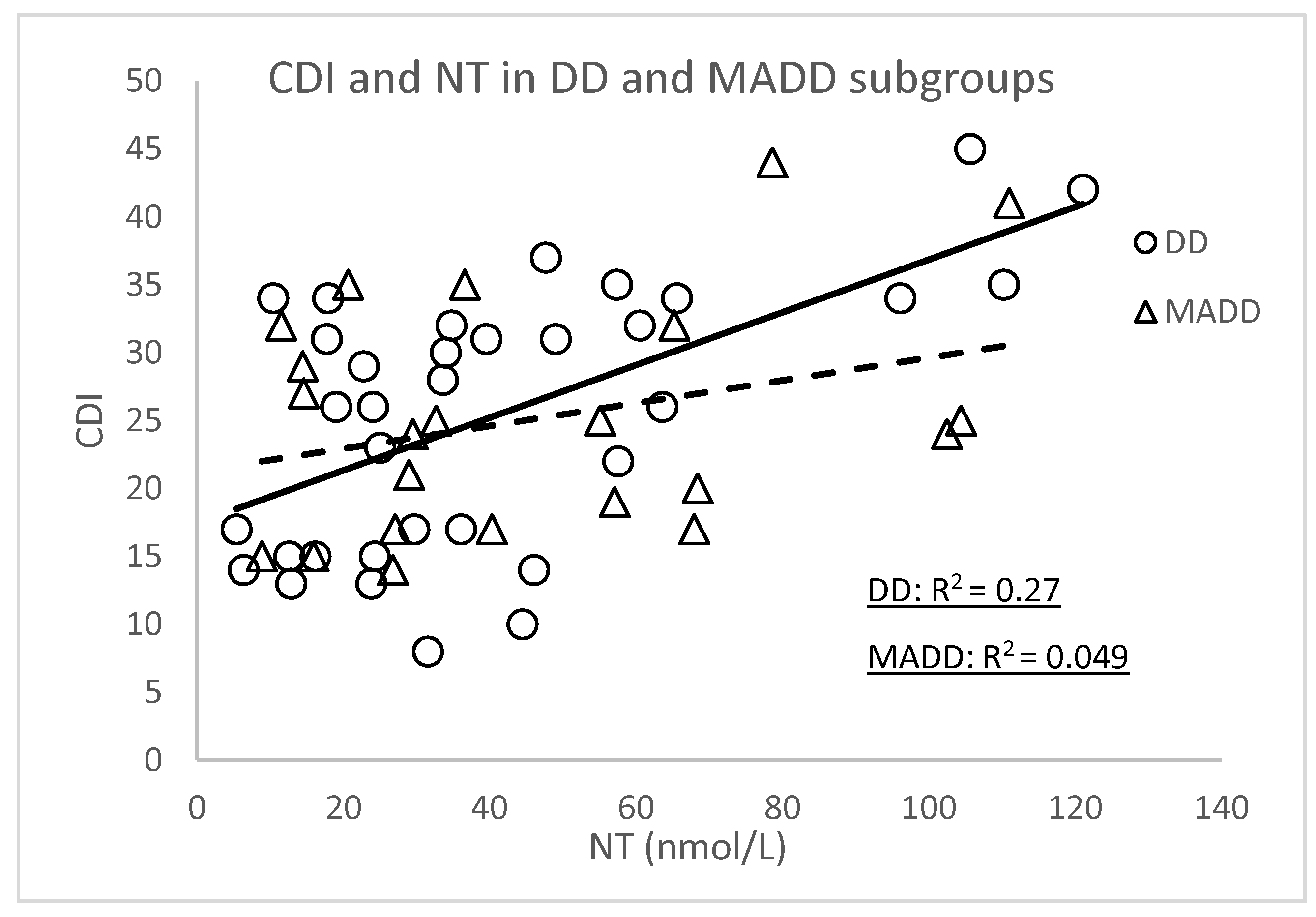
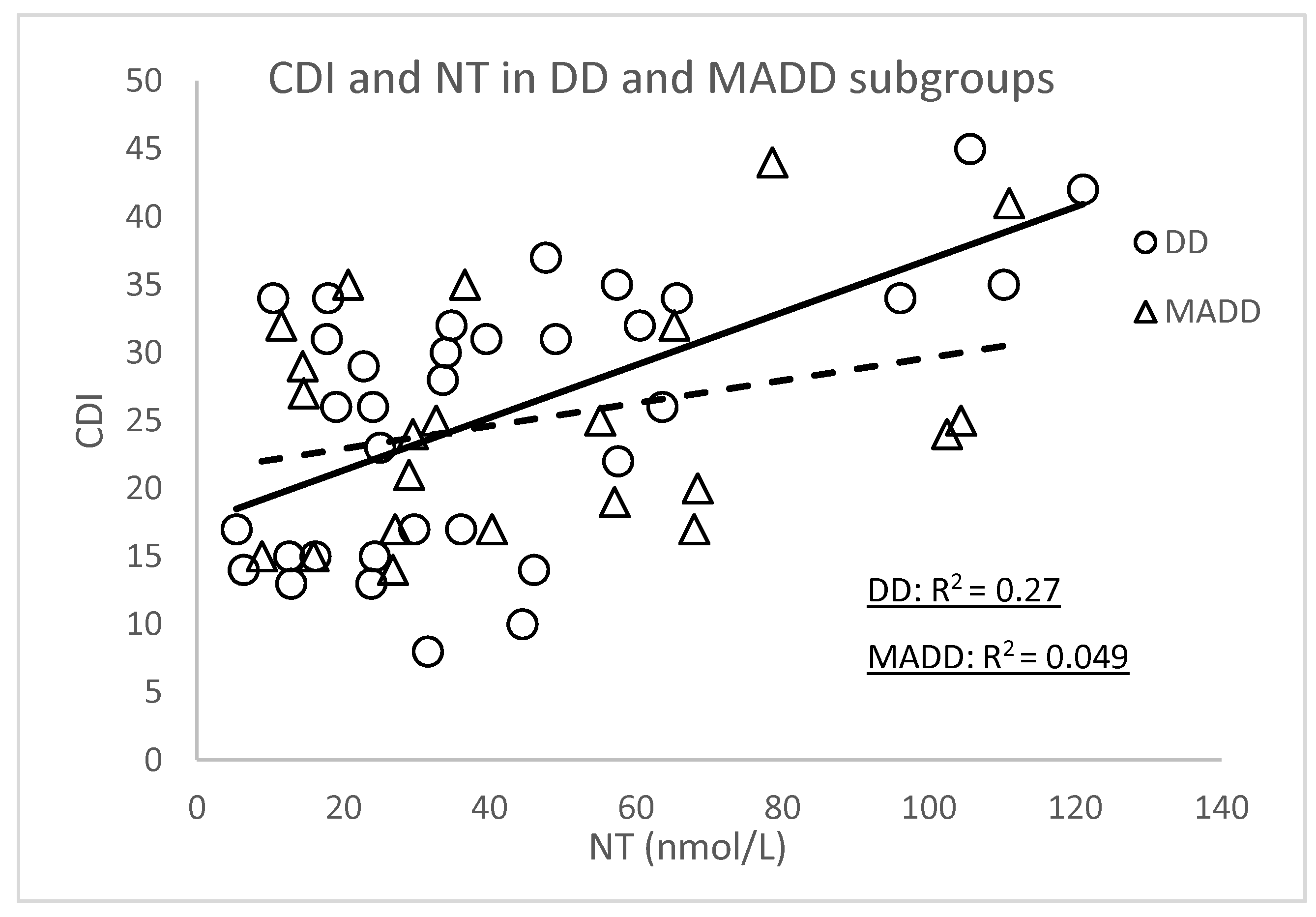
| CDI and NT | 56 | 0.407 | <0.001 |
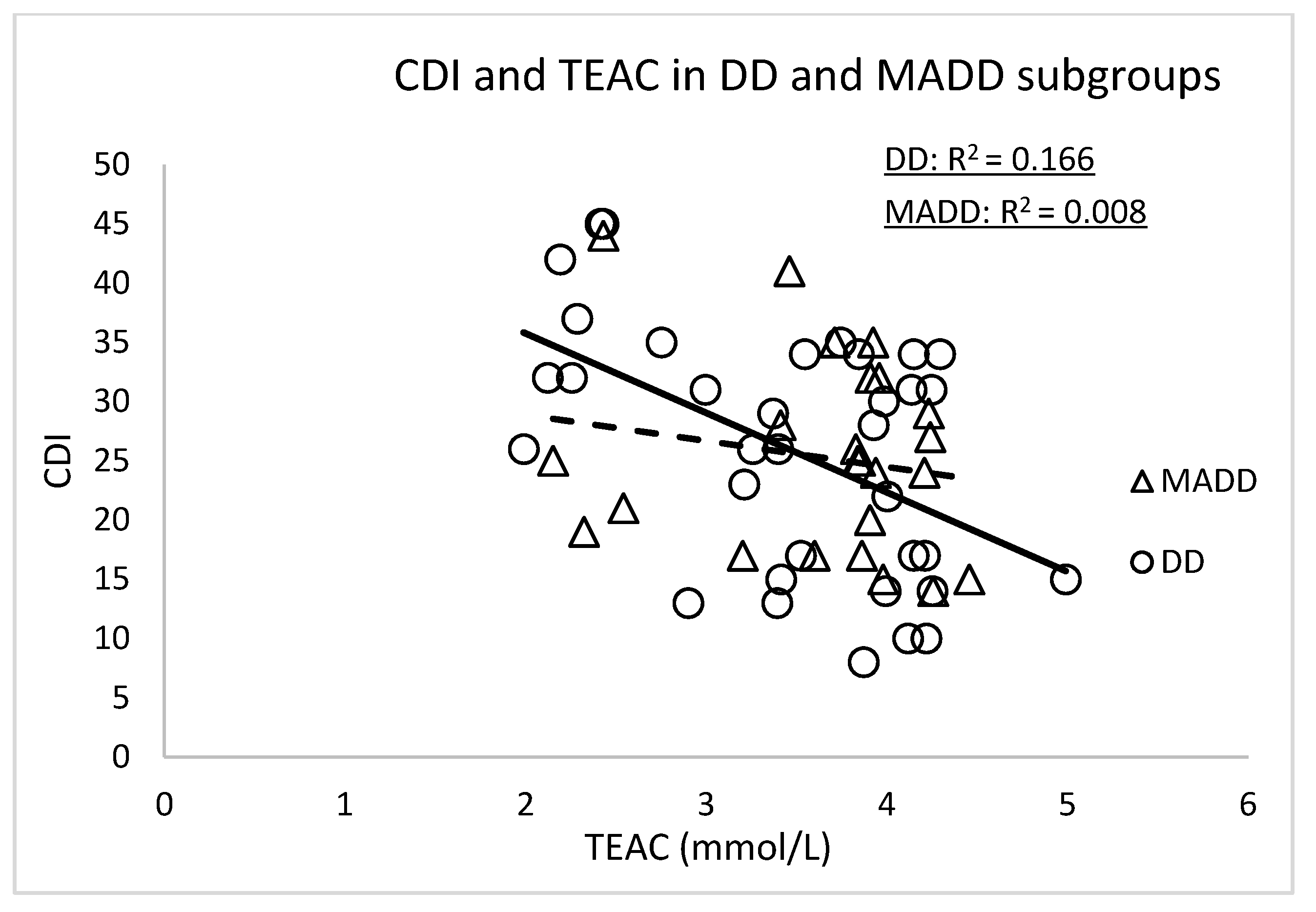
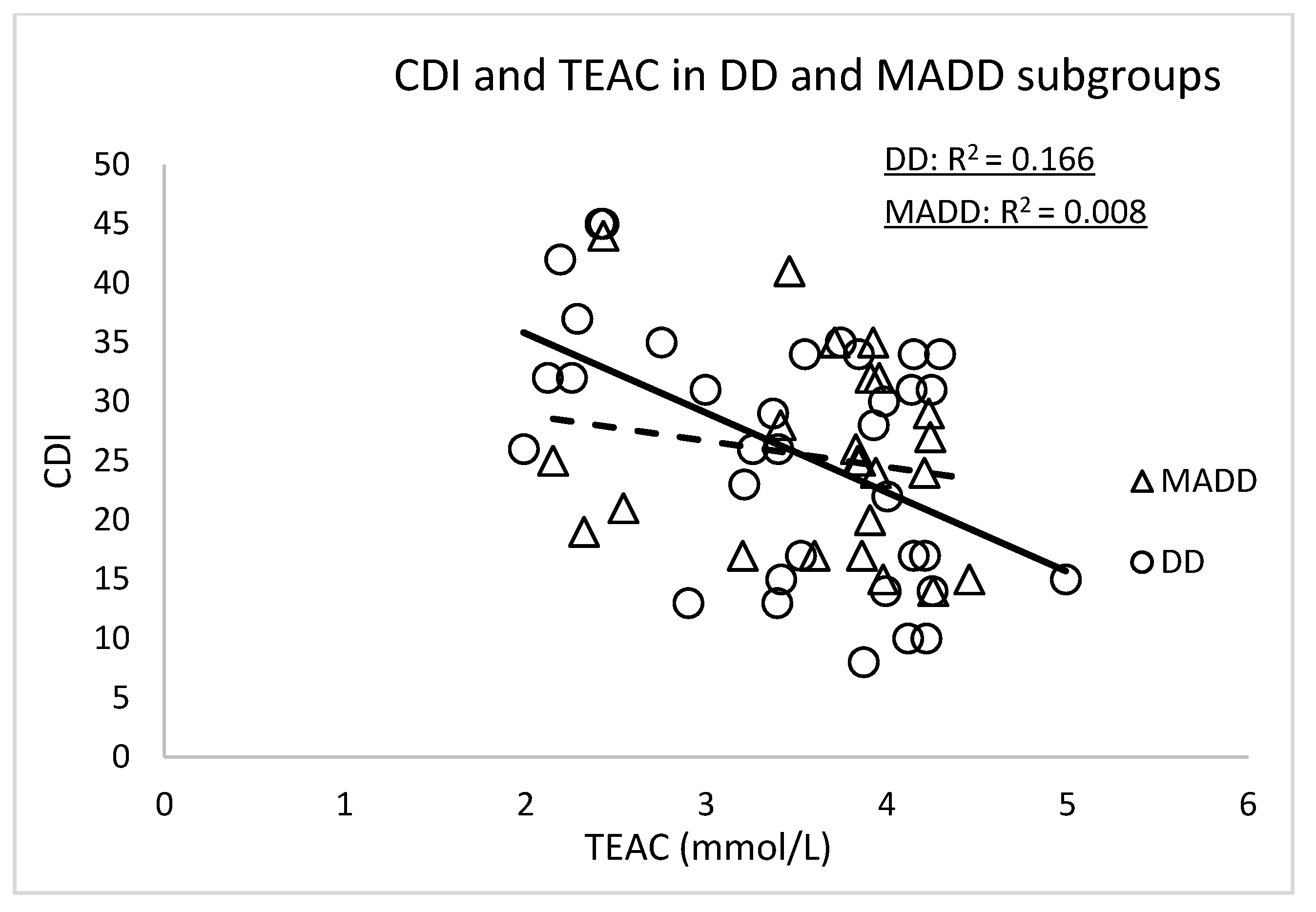
| CDI and TEAC | 59 | −0.343 | 0.004 |
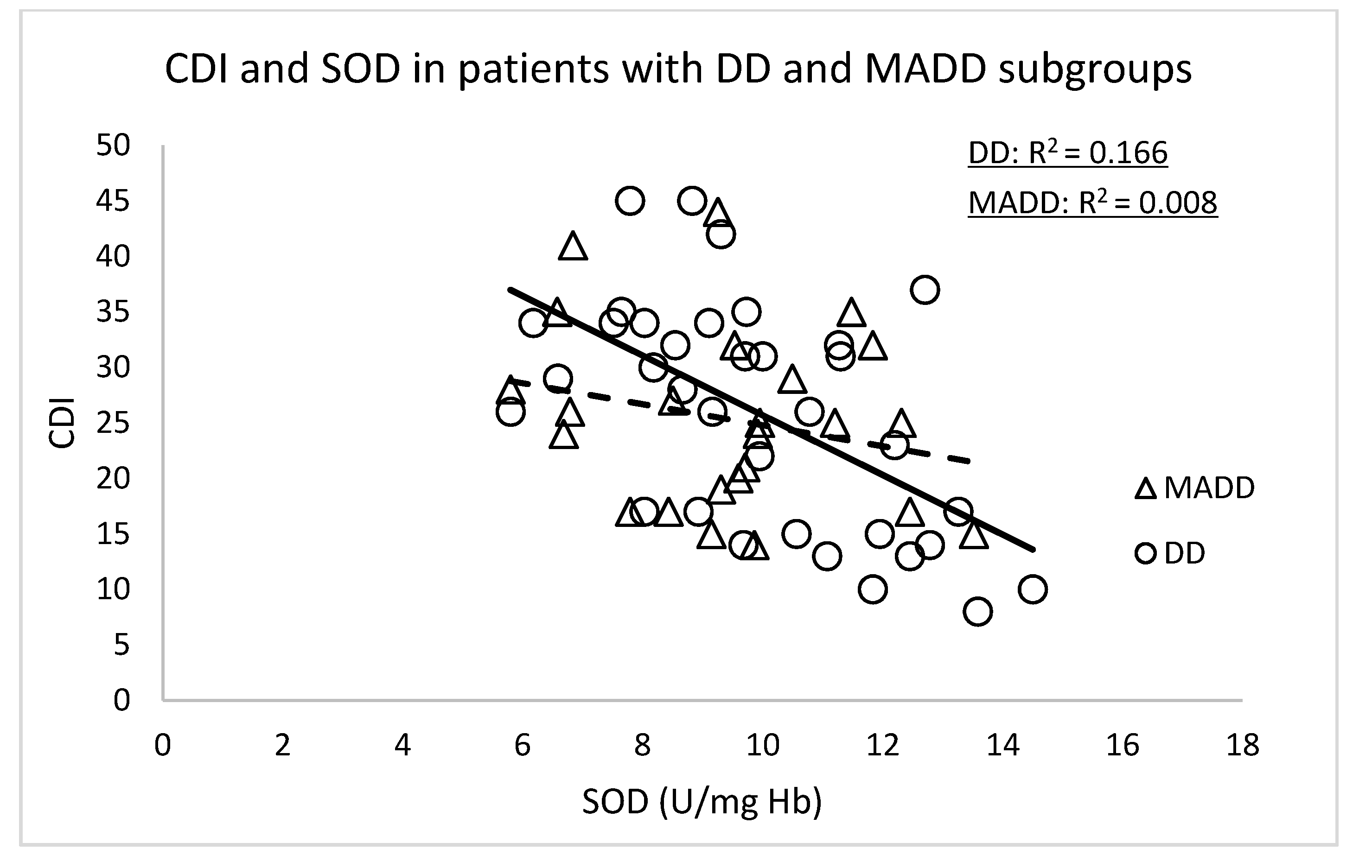
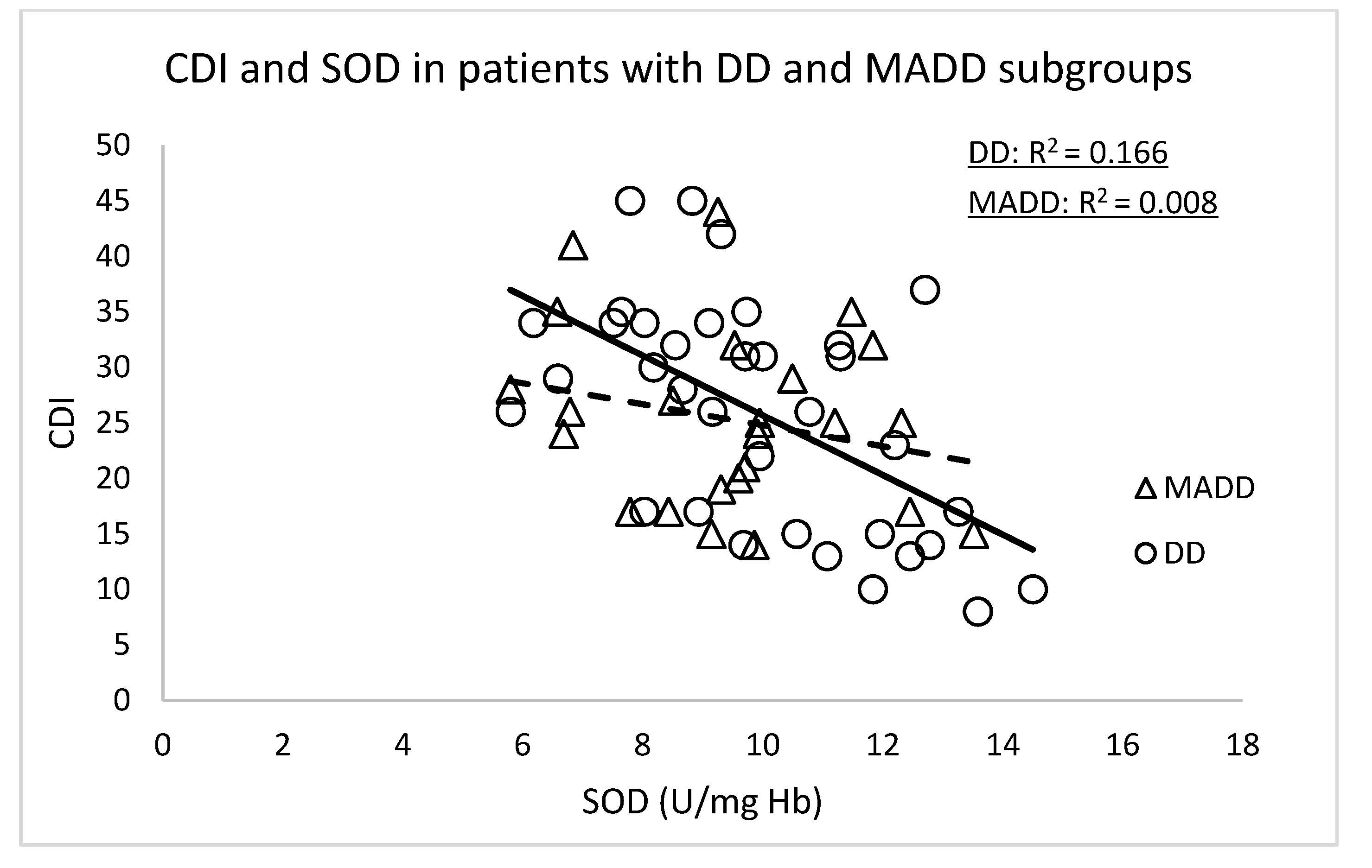
| CDI and SOD | 59 | −0.436 | <0.001 |
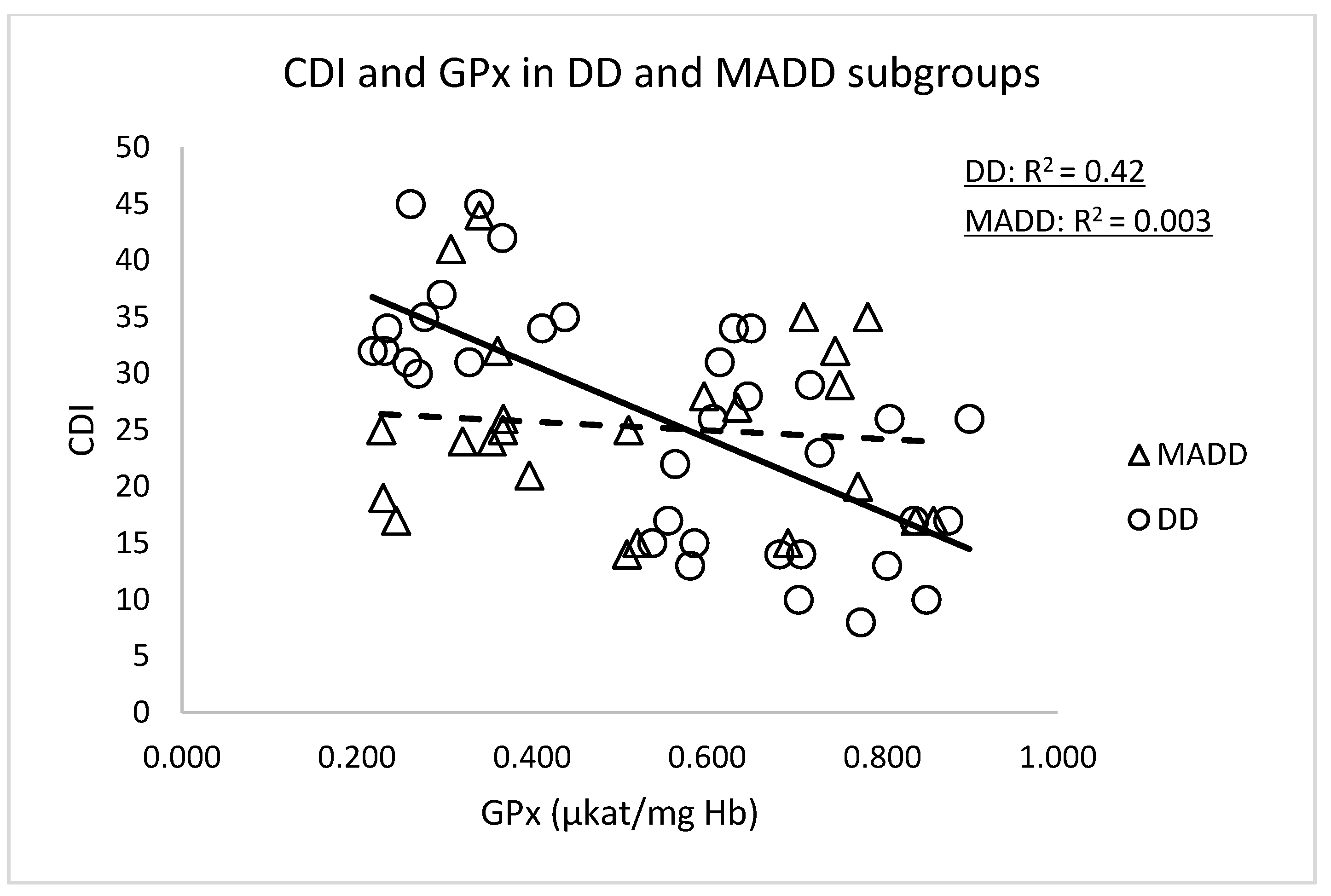
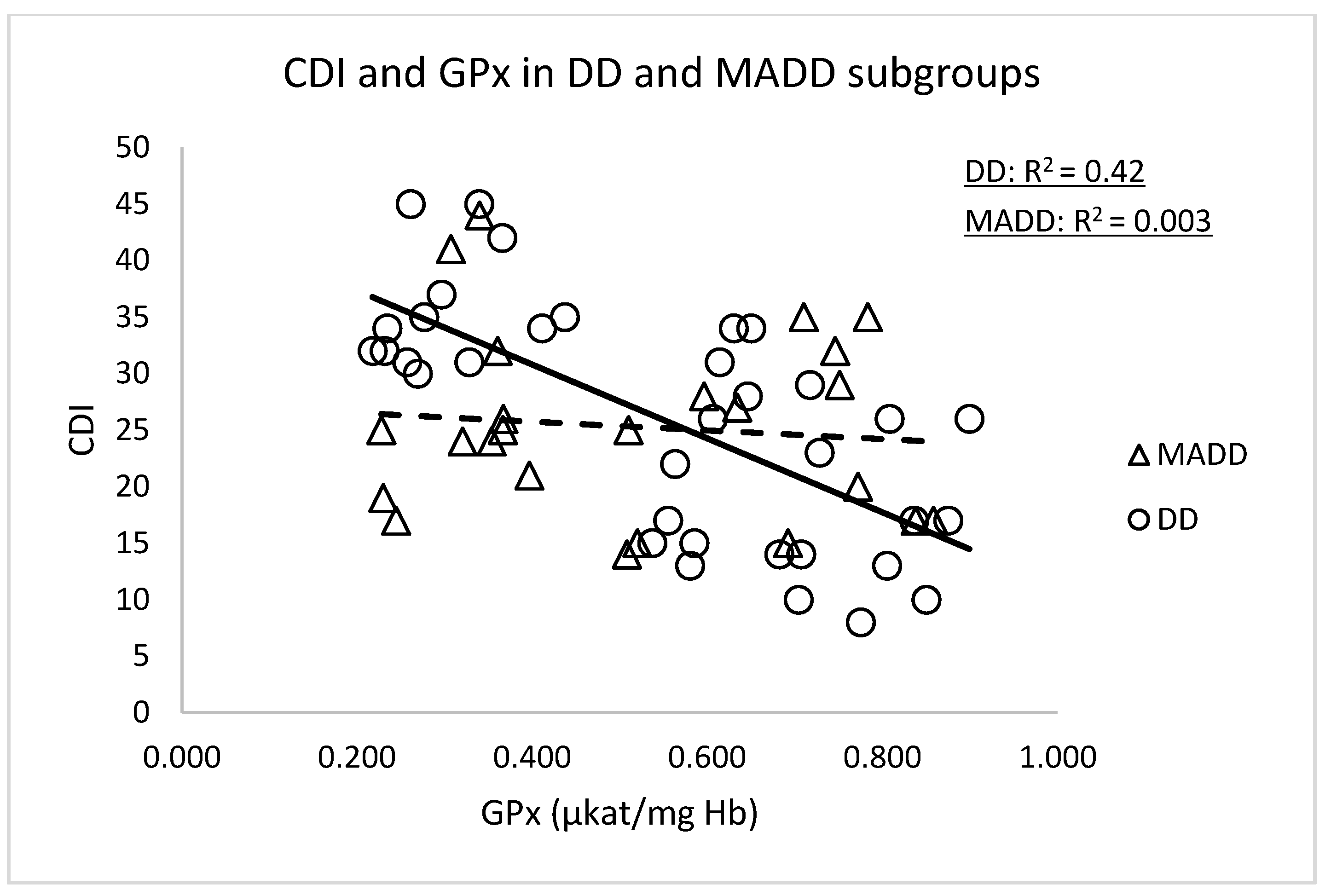
| CDI and GPx | 59 | −0.42 | <0.001 |
| CDI and CAT | 58 | −0.143 | 0.142 |
| All patients at the week 0 | n | r | p |
| omega-6/omega-3 and 8-IsoP-U | 56 | 0.392 | 0.004 |
| omega-6/omega-3 and LP | 52 | 0.026 | 0.429 |
| omega-6/omega-3 and AOPP | 55 | 0.043 | 0.379 |
| omega-6/omega-3 and NT | 52 | 0.385 | 0.005 |
| omega-6/omega-3 and TEAC | 55 | 0.052 | 0.352 |
| omega-6/omega-3 and SOD | 55 | −0.237 | 0.046 |
| omega-6/omega-3 and GPx | 55 | −0.176 | 0.198 |
| omega-6/omega-3 and CAT | 54 | 0.057 | 0.682 |
| Controls | n | r | p |
| omega-6/omega-3 and 8-IsoP-U | 17 | 0.559 | 0.020 |
| omega-6/omega-3 and LP | 19 | 0.035 | 0.445 |
| omega-6/omega-3 and AOPP | 20 | −0.023 | 0.461 |
| omega-6/omega-3 and NT | 20 | 0.144 | 0.273 |
| omega-6/omega-3 and TEAC | 20 | 0.277 | 0.242 |
| omega-6/omega-3 and SOD | 20 | −0.364 | 0.138 |
| omega-6/omega-3 and GPx | 18 | 0.042 | 0.963 |
| omega-6/omega-3 and CAT | 19 | 0.244 | 0.309 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katrenčíková, B.; Vaváková, M.; Paduchová, Z.; Nagyová, Z.; Garaiova, I.; Muchová, J.; Ďuračková, Z.; Trebatická, J. Oxidative Stress Markers and Antioxidant Enzymes in Children and Adolescents with Depressive Disorder and Impact of Omega-3 Fatty Acids in Randomised Clinical Trial. Antioxidants 2021, 10, 1256. https://doi.org/10.3390/antiox10081256
Katrenčíková B, Vaváková M, Paduchová Z, Nagyová Z, Garaiova I, Muchová J, Ďuračková Z, Trebatická J. Oxidative Stress Markers and Antioxidant Enzymes in Children and Adolescents with Depressive Disorder and Impact of Omega-3 Fatty Acids in Randomised Clinical Trial. Antioxidants. 2021; 10(8):1256. https://doi.org/10.3390/antiox10081256
Chicago/Turabian StyleKatrenčíková, Barbora, Magdaléna Vaváková, Zuzana Paduchová, Zuzana Nagyová, Iveta Garaiova, Jana Muchová, Zdenka Ďuračková, and Jana Trebatická. 2021. "Oxidative Stress Markers and Antioxidant Enzymes in Children and Adolescents with Depressive Disorder and Impact of Omega-3 Fatty Acids in Randomised Clinical Trial" Antioxidants 10, no. 8: 1256. https://doi.org/10.3390/antiox10081256
APA StyleKatrenčíková, B., Vaváková, M., Paduchová, Z., Nagyová, Z., Garaiova, I., Muchová, J., Ďuračková, Z., & Trebatická, J. (2021). Oxidative Stress Markers and Antioxidant Enzymes in Children and Adolescents with Depressive Disorder and Impact of Omega-3 Fatty Acids in Randomised Clinical Trial. Antioxidants, 10(8), 1256. https://doi.org/10.3390/antiox10081256