
Serum Zinc and Selenium Concentrations in Patients with Hypertrophy and Remodelling of the Left Ventricle Secondary to Arterial Hypertension

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tinggi, U. Selenium: Its role as antioxidant in human health. Environ. Health Prev. Med. 2008, 13, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Wang, N.; Tan, H.Y.; Li, S.; Xu, Y.; Guo, W.; Feng, Y. Supplementation of Micronutrient Selenium in Metabolic Diseases: Its Role as an Antioxidant. Oxidative Med. Cell. Longev. 2017, 2017, 7478523. [Google Scholar] [CrossRef]
- Chung, H.; Bird, A.J. Zinc Signals in Biology. In Zinc Signaling; Fukada, T., Kambe, T., Eds.; Springer: Singapore, 2019. [Google Scholar] [CrossRef]
- Marreiro, D.D.N.; Cruz, K.J.C.; Morais, J.B.S.; Beserra, J.B.; Severo, J.S.; De Oliveira, A.R.S. Zinc and Oxidative Stress: Current Mechanismsm. Antioxidants 2017, 6, 24. [Google Scholar] [CrossRef]
- Kuruppu, D.; Hendrie, H.C.; Yang, L.; Gao, S. Selenium levels and hypertension: A systematic review of the literature. Public Health Nutr. 2014, 17, 1342–1352. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Sun, S.; Feng, H.; Hou, J. Keshan Disease. In Endemic Disease in China; Sun, D., Ed.; Public Health in China; Springer: Singapore, 2019; Volume 2. [Google Scholar] [CrossRef]
- Yao, J.; Hu, P.; Zhang, D. Associations between Copper and Zinc and Risk of Hypertension in US Adults. Biol. Trace Elem. Res. 2018, 186, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, J.; Akbaraly, N.T.; Hininger, I.; Roussel, A.M.; Berr, C. Factors associated with longitudinal plasma selenium decline in the elderly: The EVA study. J. Nutr. Biochem. 2007, 18, 482–487. [Google Scholar] [CrossRef] [Green Version]
- Vinceti, M.; Chawla, R.; Filippini, T.; Dutt, C.; Cilloni, S.; Loomba, R.; Bargellini, A.; Orsini, N.; Dhillon, K.S.; Whelton, P. Blood pressure levels and hypertension prevalence in a high selenium environment: Results from a cross-sectional study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Grotto, D.; Carneiro, M.F.H.; De Castro, M.M.; Garcia, S.C.; Junior, F.B. Long-Term Excessive Selenium Supplementation Induces Hypertension in Rats. Biol. Trace Elem. Res. 2018, 182, 70–77. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Laukkanen, J.A. Serum zinc concentrations and incident hypertension: New findings from a population-based cohort study. J. Hypertens. 2016, 34, 1055–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Wang, W.; Liu, H.; Li, S.; Zhang, D. The association of serum zinc and copper with hypertension: A meta-analysis. J. Trace Elem. Med. Biol. 2019, 53, 41–48. [Google Scholar] [CrossRef]
- Hu, X.F.; Eccles, K.M.; Chan, H.M. High selenium exposure lowers the odds ratios for hypertension, stroke, and myocardial infarction associated with mercury exposure among Inuit in Canada. Environ. Int. 2017, 102, 200–206. [Google Scholar] [CrossRef]
- Burchfield, J.S.; Xie, M.; Hill, J.A. Pathological ventricular remodeling: Mechanisms: Part 1 of 2. Circulation 2013, 128, 388–400. [Google Scholar] [CrossRef] [Green Version]
- González, A.; Ravassa, S.; López, B.; Moreno, M.U.; Beaumont, J.; San José, G.; Querejeta, R.; Bayés-Genís, A.; Díez, J. Myocardial Remodeling in Hypertension. Toward a New View of Hypertensive Heart Disease. Hypertension 2018, 72, 549–558. [Google Scholar] [CrossRef]
- Nadruz, W. Myocardial remodeling in hypertension. J. Hum. Hypertens. 2015, 29, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.D.; Edvardsen, T.; Lai, S.; Castillo, E.; Pan, L.; Jerosch-Herold, M.; Sinha, S.; Kronmal, R.; Arnett, D.; Crouse, J.R., III; et al. Left ventricular concentric remodeling is associated with decreased global and regional systolic function: The Multi-Ethnic Study of Atherosclerosis. Circulation 2005, 112, 984–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronow, W.S. Hypertension and left ventricular hypertrophy. Ann. Transl. Med. 2017, 5, 310. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, M.; Oktay, A.A.; Stewart, M.H.; Milani, R.V.; Ventura, H.O.; Lavie, C.J. Left ventricular hypertrophy and hypertension. Prog. Cardiovasc. Dis. 2019, 63, 10–21. [Google Scholar] [CrossRef]
- Tomek, J.; Bub, G. Hypertension-induced remodelling: On the interactions of cardiac risk factors. J. Physiol. 2017, 595, 4027–4036. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, R.; Gonzalez, J.; Paoletto, F. The role of oxidative stress in the pathophysiology of hypertension. Hypertens. Res. 2011, 34, 431–440. [Google Scholar] [CrossRef] [Green Version]
- Rababa’h, A.M.; Guillory, A.N.; Mustafa, R.; Hijjawi, T. Oxidative Stress and Cardiac Remodeling: An Updated Edge. Curr. Cardiol. Rev. 2018, 14, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Li, J.M.; Gall, N.P.; Grieve, D.J.; Chen, M.; Shah, A.M. Activation of NADPH oxidase during progression of cardiac hypertrophy to failure. Hypertension 2002, 40, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Vara, D.; Pula, G. Reactive oxygen species: Physiological roles in the regulation of vascular cells. Curr. Mol. Med. 2014, 14, 1103–1125. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, E.; Lai, Z.F.; Yamashita, T.; Tanaka, T.; Kataoka, K.; Tokutomi, Y.; Ito, T.; Ogawa, H.; Kim-Mitsuyama, S. Enhancement of cardiac oxidative stress by tachycardia and its critical role in cardiac hypertrophy and fibrosis. J. Hypertens. 2006, 24, 2057–2069. [Google Scholar] [CrossRef]
- Rose, A.H.; Hoffmann, P.R. Selenoproteins and cardiovascular stress. Thromb. Haemost. 2015, 113, 494–504. [Google Scholar] [CrossRef]
- Romuk, E.; Jacheć, W.; Kozielska-Nowalany, E.; Birkner, E.; Zemła-Woszek, A.; Wojciechowska, C. Superoxide dismutase activity as a predictor of adverse outcomes in patients with nonischemic dilated cardiomyopathy. Cell Stress Chaperones 2019, 24, 661–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, F.W.; Hashimoto, A.S.; Lee, B.C.; Rose, A.H.; Shohet, R.V.; Hoffmann, P.R. Specific antioxidant selenoproteins are induced in the heart during hypertrophy. Arch. Biochem. Biophys. 2011, 512, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Joseph, J. Selenium and cardiometabolic health: Inconclusive yet intriguing evidence. Am. J. Med. Sci. 2013, 346, 216–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rees, K.; Hartley, L.; Day, C.; Flowers, N.; Clarke, A.; Stranges, S. Selenium supplementation for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2013, 1, CD009671. [Google Scholar] [CrossRef] [Green Version]
- Gać, P.; Urbanik, D.; Pawlas, N.; Poręba, M.; Martynowicz, H.; Prokopowicz, A.; Januszewska, L.; Markiewicz-Górka, I.; Jaremków, A.; Mazur, G.; et al. Total antioxidant status reduction conditioned by a serum selenium concentration decrease as a mechanism of the ultrasonographically measured brachial artery dilatation impairment in patients with arterial hypertension. Environ. Toxicol. Pharmacol. 2020, 75, 103332. [Google Scholar] [CrossRef]
- Mirdamadi, A.; Rafiei, R.; Kahazaipour, G.; Fouladi, L. Selenium Level in Patients with Heart Failure versus Normal Individuals. Int. J. Prev. Med. 2019, 10, 210. [Google Scholar] [CrossRef] [PubMed]
- Frączek-Jucha, M.; Kabat, M.; Szlósarczyk, B.; Czubek, U.; Nessler, J.; Gackowski, A. Selenium deficiency and the dynamics of changes of thyroid profile in patients with acute myocardial infarction and chronic heart failure. Kardiol. Pol. 2019, 77, 674–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghaemian, A.; Salehifar, E.; Shiraj, H.; Babaee, Z. A Comparison of Selenium Concentrations between Congestive Heart Failure Patients and Healthy Volunteers. J. Tehran Heart Cent. 2012, 7, 53–57. [Google Scholar]
- De Lorgeril, M.; Salen, P.; Accominotti, M.; Cadau, M.; Steghens, J.P.; Boucher, F.; de Leiris, J. Dietary and blood antioxidants in patients with chronic heart failure, Insights into the potential importance of selenium in heart failure. Eur. J. Heart Fail. 2001, 3, 661–669. [Google Scholar] [CrossRef] [Green Version]
- da Cunha, S.; Albanesi Filho, F.M.; da Cunha Bastos, V.L.; Antelo, D.S.; Souza, M.M. Thiamin, selenium, and copper levels in patients with idiopathic dilated cardiomyopathy taking diuretics. Arq. Bras. Cardiol. 2002, 79, 460–465. [Google Scholar] [CrossRef]
- Mihailović, M.; Avramović, D.; Jovanović, I.; Pesut, O.J.; Matić, D.P.; Stojanov, V.J. Blood and plasma selenium levels and GSH-Px activities in patients with arterial hypertension and chronic heart disease. J. Environ. Pathol. Toxicol. Oncol. 1997, 17, 285–289. [Google Scholar]
- Oster, O.; Prellwitz, W.; Kasper, W.; Meinertz, T. Congestive cardiomyopathy and the selenium content of serum. Clin. Chim. Acta 1983, 128, 125–132. [Google Scholar] [CrossRef]
- Alehagen, U.; Johansson, P.; Björnstedt, M.; Rosén, A.; Dahlström, U. Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and coenzyme Q10 supplementation: A 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. Int. J. Cardiol. 2013, 167, 1860–1866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh, K.; Kikuchi, N.; Satoh, T.; Kurosawa, R.; Sunamura, S.; Siddique, M.A.H.; Omura, J.; Yaoita, N.; Shimokawa, H. Identification of Novel Therapeutic Targets for Pulmonary Arterial Hypertension. Int. J. Mol. Sci. 2018, 19, 4081. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, N.; Satoh, K.; Satoh, T.; Yaoita, N.; Siddique, M.A.H.; Omura, J.; Kurosawa, R.; Nogi, M.; Sunamura, S.; Miyata, S.; et al. Diagnostic and Prognostic Significance of Serum Levels of SeP (Selenoprotein P) in Patients with Pulmonary Hypertension. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 2553–2562. [Google Scholar] [CrossRef] [PubMed]
- Burk, R.F.; Hill, K.E. Selenoprotein P-expression, functions, and roles in mammals. Biochim. Biophys. Acta 2009, 1790, 1441–1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshihisa, A.; Abe, S.; Kiko, T.; Kimishima, Y.; Sato, Y.; Watanabe, S. Association of Serum Zinc Level with Prognosis in Patients With Heart Failure. J. Card. Fail. 2018, 24, 375–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexanian, I.; Parissis, J.; Farmakis, D.; Athanaselis, S.; Pappas, L.; Gavrielatos, G.; Mihas, C.; Paraskevaidis, I.; Sideris, A.; Kremastinos, D.; et al. Clinical and echocardiographic correlates of serum copper and zinc in acute and chronic heart failure. Clin. Res. Cardiol. 2014, 103, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Teng, T.; Bian, B.; Yao, W.; Yu, X.; Wang, Z.; Xu, Z.; Sun, Y. Zinc Levels in Left Ventricular Hypertrophy. Biol. Trace Elem. Res. 2017, 176, 48–55. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| age (years) # | 53.72 ± 12.74 |
| height (cm) # | 172.72 ± 10.88 |
| body mass (kg) # | 95.17 ± 18.03 |
| BMI (kg/m2) # | 31.79 ± 4.67 |
| smoking * | 20.5 (16) |
| pack-years of smoking # | 21.15 ± 8.15 |
| arterial hypertension * | 100.0 (78) |
| duration of arterial hypertension (years) # | 11.86 ± 9.32 |
| diuretics * | 51.3 (40) |
| β-blockers * | 51.3 (40) |
| ACE inhibitors * | 35.9 (28) |
| angiotensyn receptor blockers * | 42.3 (33) |
| calcium channel blockers * | 51.3 (40) |
| total cholesterol (mg/dl) # | 204.80 ± 44.40 |
| HDL cholesterol (mg/dl) # | 48.83 ± 13.33 |
| LDL cholesterol (mg/dl) # | 121.00 ± 35.88 |
| triglicerides (mg/dl) # | 197.66 ± 144.51 |
| glucose (mg/dl) # | 100.12 ± 21.88 |
| Se-S (μg/L) # | 89.84 ± 18.75 |
| Zn-S (mg/L) # | 0.86 ± 0.13 |
| LVEDd (mm) # | 50.67 ± 5.56 |
| LVESd (mm) # | 30.85 ± 3.83 |
| IVSDd (mm) # | 12.55 ± 2.11 |
| PWDd (mm) # | 10.54 ± 1.26 |
| EF (%) # | 67.13 ± 5.13 |
| LVMI (g/m2) # | 114.83 ± 36.44 |
| RWT # | 0.46 ± 0.06 |
| NG * | 28.2 (22) |
| LVH * | 71.8 (56) |
| CR * | 28.2 (22) |
| CH * | 29.5 (23) |
| EH * | 14.1 (11) |
| A | Subgroups Differing in Se-S | Subgroups Differing in Zn-S | ||||
|---|---|---|---|---|---|---|
| Low-Se (Se-S < 88.91 μg/L) | High-Se (Se-S ≥ 88.91 μg/L) | p | Low-Zn (Zn-S < 0.84 mg/L) | High-Zn (Zn-S ≥ 0.84 mg/L) | p | |
| NG * | 12.8 (5) | 43.6 (17) | 0.003 & | 16.2 (6) | 39.0 (16) | 0.025 & |
| LVH * | 87.2 (34) | 56.4 (22) | 0.003 & | 83.8 (31) | 60.9 (25) | 0.025 & |
| CR * | 30.8 (12) | 25.6 (10) | 0.609 | 32.4 (12) | 24.4 (10) | 0.431 |
| CH * | 35.9 (14) | 23.1 (9) | 0.215 | 32.4 (12) | 26.8 (11) | 0.587 |
| EH * | 20.5 (8) | 7.7 (3) | 0.104 | 18.9 (7) | 9.8 (4) | 0.248 |
| B | Se-S (μg/L) # | Zn-S (mg/L) # | ||||
| subgroups differing in left ventricular hypertrophy | NG | 100.24 ± 26.01 | 0.90 ± 0.12 | |||
| LVH | 85.76 ± 13.19 | 0.83 ± 0.13 | ||||
| p | 0.002 & | 0.032 & | ||||
| subgroups differing in the type of left ventricular geometry | NG | 100.24 ± 26.01 | 0.90 ± 0.12 | |||
| CR | 84.10 ± 12.89 | 0.83 ± 0.14 | ||||
| CH | 85.11 ± 12.41 | 0.85 ± 0.12 | ||||
| EH | 90.44 ± 15.44 | 0.80 ± 0.14 | ||||
| p | NG vs. CR: 0.004 & | NG vs. CR: 0.174 | ||||
| NG vs. CH: 0.006 & | NG vs. CH: 0.376 | |||||
| NG vs. EH: 0.140 | NG vs. EH: 0.037 & | |||||
| CR vs. CH: 0.849 | CR vs. CH: 0.916 | |||||
| CR vs. EH: 0.338 | CR vs. EH: 0.521 | |||||
| CH vs. EH: 0.416 | CH vs. EH: 0.428 | |||||
| Model for: Probability of Left Ventricle Hypertrophy | ||||||
|---|---|---|---|---|---|---|
| Intercept | Age (Years) | LDL Cholesterol (mg/dl) | Glucose (mg/dl) | Se-S (μg/L) | Zn-S (mg/L) | |
| regression coefficient | −0.92 | 0.07 | 0.04 | 0.03 | −0.03 | −0.22 |
| SEM of Rc | 0.40 | 0.02 | 0.02 | 0.01 | 0.01 | 0.10 |
| p value | <0.01 & | 0.04 & | 0.03 & | 0.04 & | 0.02 & | 0.01 & |
| odds ratio (for unit change) | 0.09 | 1.07 | 1.08 | 1.07 | 0.96 | 0.92 |
| confidence interval | ||||||
| −95% | 0.03 | 1.01 | 1.01 | 1.02 | 0.91 | 0.89 |
| +95% | 0.11 | 1.15 | 1.16 | 1.11 | 0.98 | 0.96 |
| LVH Prediction | ||
|---|---|---|
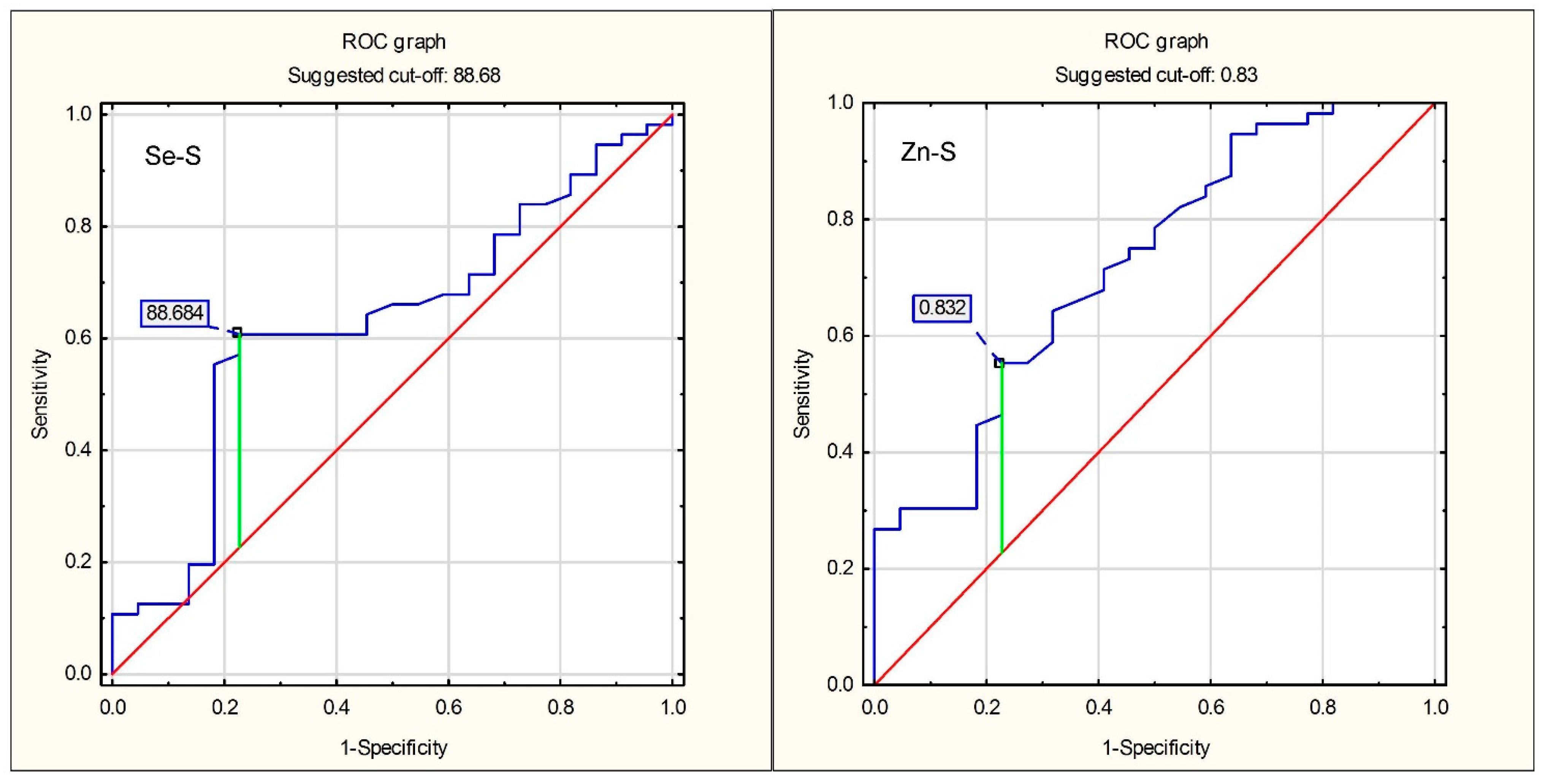
| Se-S < 88.68 μg/L | Zn-S < 0.83 mg/L | |
| sensitivity | 0.773 | 0.773 |
| specificity | 0.589 | 0.554 |
| accuracy | 0.641 | 0.615 |
| positive prediction value | 0.425 | 0.405 |
| negative predictive value | 0.868 | 0.861 |
| positive likelihood ratio | 1.881 | 1.731 |
| negative likelihood ratio | 0.386 | 0.411 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gać, P.; Czerwińska, K.; Poręba, M.; Prokopowicz, A.; Martynowicz, H.; Mazur, G.; Poręba, R. Serum Zinc and Selenium Concentrations in Patients with Hypertrophy and Remodelling of the Left Ventricle Secondary to Arterial Hypertension. Antioxidants 2021, 10, 1803. https://doi.org/10.3390/antiox10111803
Gać P, Czerwińska K, Poręba M, Prokopowicz A, Martynowicz H, Mazur G, Poręba R. Serum Zinc and Selenium Concentrations in Patients with Hypertrophy and Remodelling of the Left Ventricle Secondary to Arterial Hypertension. Antioxidants. 2021; 10(11):1803. https://doi.org/10.3390/antiox10111803
Chicago/Turabian StyleGać, Paweł, Karolina Czerwińska, Małgorzata Poręba, Adam Prokopowicz, Helena Martynowicz, Grzegorz Mazur, and Rafał Poręba. 2021. "Serum Zinc and Selenium Concentrations in Patients with Hypertrophy and Remodelling of the Left Ventricle Secondary to Arterial Hypertension" Antioxidants 10, no. 11: 1803. https://doi.org/10.3390/antiox10111803
APA StyleGać, P., Czerwińska, K., Poręba, M., Prokopowicz, A., Martynowicz, H., Mazur, G., & Poręba, R. (2021). Serum Zinc and Selenium Concentrations in Patients with Hypertrophy and Remodelling of the Left Ventricle Secondary to Arterial Hypertension. Antioxidants, 10(11), 1803. https://doi.org/10.3390/antiox10111803